
Abstract
Background:
Little is known regarding the differential effects of the apolipoprotein E (APOE) ɛ4 on the regional topography of amyloid and tau in patients with both early-onset (EOAD) and late-onset Alzheimer’s disease (LOAD).
Objective:
To compare the distribution and association of tau, amyloid, and cortical thickness among groups classified by the presence of APOE ɛ4 allele and onset age.
Methods:
A total of 165 participants including 54 EOAD patients (29 ɛ4-; 25 ɛ4+), 45 LOAD patients (21 ɛ4-; 24 ɛ4+), and 66 age-matched controls underwent 3T MRI, 18F-THK5351 (THK) and 18F-flutemetamol (FLUTE) PET scans, APOE genotyping, and neuropsychological tests. Data for voxel-wise and standardized uptake values from PET scans were analyzed in the context of APOE and age at onset.
Results:
EOAD ɛ4- patients showed greater THK retention in the association cortices, whereas their EOAD ɛ4+ counterparts had more retention in medial temporal areas. THK topography of LOAD ɛ4+ was similar to EOAD ɛ4 + . THK correlated positively with FLUTE and conversely with mean cortical thickness, being lowest in EOAD ɛ4-, highest in LOAD ɛ4-, and modest in ɛ4+ groups. Even in the APOE ɛ4+ groups, THK tended to correlate with FLUTE and mean cortical thickness in the inferior parietal region in EOAD and in the medial temporal region in LOAD. LOAD ɛ4- manifested with prevalent small vessel disease markers and the lowest correlation between THK retention and cognition.
Conclusion:
Our observations suggest the differential effects of the APOE ɛ4 on the relationship between tau and amyloid in EOAD and LOAD.
INTRODUCTION
The ɛ4 allele of apolipoprotein E (APOE) is a known risk factor for late-onset Alzheimer’s disease (LOAD) [1–3]. APOE is present in lipoprotein particles in the human brain and plays critical roles in amyloid-β (Aβ) protein precursor synthesis, amyloid-β clearance, and tau phosphorylation [4–6]. Of the three (ɛ2, ɛ3, and ɛ4) gene variants that can ultimately alter APOE structure and function, APOE ɛ4 increases AD risk in a dose-dependent manner by 2- to 3-fold with one ɛ4 allele and 12-fold with two ɛ4 alleles [1, 7]. Typical characteristics of AD such as female predominance, vulnerability of medial temporal atrophy, and the amnestic phenotype of cognitive impairment are associated with APOE ɛ4 [2, 8].
Although APOE ɛ4 is primarily associated with LOAD, several studies have shown that it also increases the risk of early-onset AD (EOAD) [1, 10]. Distinct from LOAD, EOAD is clinically characterized by an early onset before 65 years old, parietal signs and symptoms, and rapid disease progression [11]. Due to these differences between EOAD and LOAD, it is assumed that APOE ɛ4 may have different effects on AD according to onset age [12]. Moreover, EOAD tends to develop in the absence of APOE ɛ4 [13] and atypical features of AD such as non-memory symptoms and faster progression have been found in the absence of APOE ɛ4 in EOAD patients [14].
Several individual studies have reported the different effects of APOE ɛ4 and age at onset in the brains of AD patients. While the medial temporal preference of atrophic patterns [15], tau and amyloid accumulation [16], and hypometabolism [17] were found in LOAD patients with APOE ɛ4, EOAD patients without APOE ɛ4 showed more severe and generalized brain atrophy and hypometabolism [12, 18]. It has also been reported in pathologic and tau positron emission tomography (PET) studies that spatial distribution of neurofibrillary tangles differs according to the age at onset and does not follow the Braak & Braak staging in EOAD patients [19–21]. However, little is known regarding the differential effect of APOE ɛ4 on the regional topography of amyloid and tau in patients with both early-onset and late-onset AD.
Concerns have been raised in regards to off-target binding of the first generation tau PET tracers [22, 23]. Evidence suggests that [18F]THK5351 binding to monoamine oxidase-B (MAO-B) markedly increases in vivo tau PET signal [23]. Other recent studies, however, have shown that THK family radiotracers discriminate well between AD dementia and healthy controls [24] and may be a suitable imaging marker to detect neurodegenerative changes caused by reactive astrogliosis as well as tau [25–28].
The present study sought to compare clinical characteristics and distribution of tau and amyloid among groups classified by the presence of the APOE ɛ4 allele and age at onset (EOAD and LOAD). Another aim was to investigate the combined effects of APOE genotype and age at onset on the relationship between tau and amyloid burden, brain atrophy, and cognitive function.
MATERIALS AND METHODS
Participants
We recruited a total number of 177 participants including 103 patients with AD, and 74 cognitively unimpaired (CU) subjects from October 2015 to September 2017. Participants underwent 18F-THK5351(THK) and 18F-flutemetamol (FLUTE) PET scans, 3.0-Tesla MRI, APOE genotyping, and detailed neuropsychological tests at the Memory Clinic at Gachon University Gil Medical Center (Republic of Korea). Of the 177 participants who had been screened for this study, 12 participants who failed to complete all imaging studies or had unsuitable data due to motion defects were excluded. Thus, a total 165 participants including 54 EAOD patients (25 APOE ɛ4+ and 29 APOE ɛ4-), 45 LOAD patients (24 APOE ɛ4+ and 21 APOE ɛ4-), and 66 CU participants were used in the analyses.
AD dementia patients had been diagnosed with probable AD according to the National Institute of Neurological and Communicative Disorders and Stroke and the AD and Related Disorders Association [29]. Diagnoses were confirmed by a neurologist (Y. Noh). The AD patients were categorized as EOAD (age at onset < 65) or LOAD (age at onset≥65). Patients with a history of neurological diseases or psychiatric disorders were not included. Patients with structural abnormalities in MRI such as cerebral, cerebellar, or brainstem infarction, intracranial hemorrhage, hydrocephalus, severe white matter hyperintensities, white matter hyperintensities associated with radiation, traumatic brain injury, tumors, multiple sclerosis, and vasculitis were excluded. Patients with dementia other than AD were also excluded after screening by laboratory tests including complete blood count, thyroid function, syphilis serology, folate levels, vitamin B12, and metabolic profile. Patients with vascular dementia and familial AD were also excluded.
The age group-matched CU participants were either healthy volunteers from the community or spouses of the patients. They did not exhibit subjective or objective cognitive decline with a Clinical Dementia Rating (CDR) score of 0 and z-scores within 1.5 standard deviations in age- and education-corrected norms on detailed neuropsychological tests. As well as AD patients, we excluded CU participants with structural abnormalities in MRI such as cerebral, cerebellar, or brainstem infarction, intracranial hemorrhage, hydrocephalus, severe white matter hyperintensity, white matter hyperintensity associated with radiation, traumatic brain injury, tumors, multiple sclerosis, or vasculitis. For comparison with the EOAD or LOAD groups, CU subjects were divided into each age-matched control groups comprising 33 young controls (YC, mean age = 57.6 years old) and 33 old controls (OC, mean age = 75.7 years old).
Written informed consent was obtained from all participants or their guardians and this study was approved by the Institutional Review Board of Gachon University Gil Medical Center.
Neuropsychological assessment
All participants had their cognitive function evaluated using the Mini-Mental State Examination (MMSE), CDR, CDR-sum of boxes (CDR-SOB), and detailed neuropsychological tests including attention, language, verbal and visual memory, visuospatial, praxis, and frontal/executive functioning. Elements of Gerstmann syndrome were evaluated in all participants. Detailed items of the comprehensive test battery [30, 31] have been described in our previous study [32].
Image acquisition and preprocessing
MR imaging acquisition and segmentation
All participants underwent brain MR imaging using a Verio 3.0-Tesla MRI scanner (Siemens with a Siemens matrix coil) to acquire 3D T1-MPRAGE (Repetition time: 1900 ms, echo time: 2.93 ms, flip angle: 8°, pixel bandwidth: 170 Hz/pixel, matrix size: 256×208, field of view: 256 mm, NEX: 1, total acquisition time: 4 min 10 s, voxel size: 0.5×0.5×1.0 mm3). We analyzed the images using FreeSurfer 6.0 (http://www.surfer.nmr.mgh.harvard.edu) to define regions-of-interest (ROIs) in the native-space of each participant and to support correction of gray matter (GM) atrophy and white matter spillover in the PET data. Other clinical MRI sequences including fluid attenuated inversion recovery (FLAIR), susceptibility weighted imaging (SWI), and T1- and T2-weighted imaging were also acquired. The FLAIR imaging parameters used were as follows: repetition time = 9000 ms, echo time = 122 ms, flip angle = 150°, pixel bandwidth = 287 Hz/pixel, matrix size = 256×224; the SWI imaging parameters used were: repetition time = 27 ms, echo time = 20 ms, flip angle = 15°, pixel bandwidth = 120 Hz/pixel, matrix size = 256×224; and the T1-weighted imaging parameters used were: repetition time = 500 ms, echo time = 9.2 ms, flip angle = 70°, pixel bandwidth = 391 Hz/pixel, matrix size = 256×224. T2-weighted imaging parameters used were as follows: repetition time = 9650 ms, echo time = 88 ms, flip angle = 120°, pixel bandwidth = 174 Hz/pixel, matrix size = 256×224.
Lacunes were defined as lesions of≥3 mm and≤15 mm in diameter with low signal on T1-weighted images, high signal on T2-weighted images, and a perilesional halo on 80 axial sections of FLAIR images. Microbleeds were defined as small lesions of≤10 mm in diameter, using criteria proposed by Greenberg et al. [33], on 20 axial sections of time constant T2-weighted gradient– recalled echo sequence MRIs. Images were analyzed using FreeSurfer 6.0 (http://www.surfer.nmr.mgh.harvard.edu).
PET imaging acquisition
All 18F-THK5351 and 18F-FLUTE PET scans were acquired using a Siemens Biograph 6 Truepoint PET/computed tomography (CT) scanner (Siemens, Knoxville, TN, USA) with a list-mode emission acquisition. THK5351 was synthesized and radiolabeled at Gachon University Neuroscience Research Institute and scans were acquired from 50 to 70 min after the intravenous injection of 185 MBq of 18F-THK5351. FLUTE was purchased from Carecamp Incorporated, and scans were acquired from 90 to 110 min after the intravenous injection of 185 MBq of 18F-FLUTE. Attenuation was corrected with a low-dose CT scan and data was reconstructed onto a 256×256×109 matrix with a voxel size of 1.3×1.3×1.5 mm3 using a 2D ordered subset expectation maximization algorithm with 8 iterations and 16 subsets.
PET quantification
[18F]THK5351 and [18F]FLUTE PET images were co-registered with the corresponding T1 images using FreeSurfer. Regional mean values of PET images were then extracted after region-based partial volume correction (PVC) using the PETSurfer tool in FreeSurfer [34, 35] and the weighted-average acquired for pre-defined ROIs. ROIs included the prefrontal (frontal pole, pars orbitalis, orbital frontal, pars triagularis, pars opercularis, rostral middle frontal, superior frontal, caudal middle frontal, and medial orbital frontal regions), orbitofrontal (orbital frontal and medial orbital frontal regions), sensorimotor (pre-central, post-central, and paracentral regions), anterior cingulate (accumbens-area, caudal anterior cingulate, and rostral anterior cingulate regions), superior parietal, inferior parietal (inferior parietal and supramarginal regions), precuneus, posterior cingulate, occipital cortex (precuneus, pericalcarine, and lateral occipital regions), superior temporal, middle temporal, inferior temporal, mesial temporal (hippocampus, amygdala, parahippocampal and entorhinal cortices), entorhinal cortices, parahippocampus, hippocampus, amygdala, fusiform gyrus, lingual gyrus, striatum, and cortical regions. The cortical retention ratio of FLUTE was calculated based on AD-associated regions including the prefrontal, superior parietal, lateral temporal, inferior parietal, occipital, anterior cingulate, mesial temporal precuneus, and posterior cingulate cortices [36]. Regional standardized uptake value ratios (SUVRs) were calculated using cerebellar GM as the reference region for THK images [37, 38] and the pons for FLUTE images [36]. SUVR images were also generated from the MRI co-registered PET images with voxel-based PVC [34, 35]. [18F]FLUTE images were also evaluated visually in the frontal, temporal, parietal cortices, striatum, and precuneus.
Statistical analysis
Demographic and clinical characteristics between groups classified by age at onset and APOE ɛ4 were performed using analysis of variance for continuous variables and a chi square test for nominal variables. Group comparisons of THK SUVR, FLUTE SUVR, and neuropsychological test results were performed between groups followed by pairwise comparisons for adjusted means (Bonferroni, p < 0.05). Region-wise multiple comparisons were corrected using the Benjamini-Hochberg false discovery rate method [39]. Pearson’s correlation analysis of THK SUVR and detailed neuropsychological tests were performed. All statistical analyses mentioned previously were conducted using PASW Statistics 23 software (SPSS Inc, Chicago, IL, USA) with a significance of p < 0.05 (two-way).
Voxel-wise group comparisons of GM-masked SUVR images were performed using 2 sample t-tests with a false discovery rate correction with adjustment for age (for different age group comparisons), sex, and years of education using SPM12 (Statistical Parametric Mapping; Wellcome Trust Centre for Neuroimaging, London, UK). The resulting t-score maps were displayed on the inflated FsAverage brain using MRtools (http://mrtools.mgh.harvard.edu/). Multiple regression analyses were performed to determine correlation of THK5351 retention with cortical FLUTE retention and mean cortical thickness. The analyses were performed with adjustments for age (for different age groups), sex, and years of education. Results were significant at p < 0.001, uncorrected for multiple comparisons.
To evaluate the intra-voxel correlation between THK5351 retention and FLUTE retention in each diagnostic group, voxel-wise partial correlation analysis was performed using the Biological Parametric Mapping (BPM) 3.1 toolbox with SPM5 [40]. The analyses were performed with adjustments for age and years of education. No predefined brain mask was applied, and the absolute p value threshold was used. The resulting t-score maps (uncorrected p < 0.01, cluster > 100) for partial correlation were overlaid on an inflated FsAverage brain.
To investigate inter-regional correlations of the two tracers, correlation matrices were calculated from partial correlation analysis with adjustment for age. Correlation analysis between regional THK5351 retention and FLUTE retention within 42 ROIs was performed. Spearman’s rho was computed after controlling for the effects of age, sex, and years of education. To visualize clear matrices, Spearman’s rho value at p < 0.01 was also presented.
RESULTS
Demographics and clinical characteristics
Demographic and clinical characteristics of the study participants are shown in Table 1. Mean ages in the EOAD ɛ4+ and LOAD ɛ4+ groups were 61.80±5.58 and 76.38±5.82 years, respectively. Years of education, disease duration, and global cognition were not significantly different among the patient groups.
Demographics and clinical characteristics of the study population
Data are presented as mean±standard deviation for continuous variables and number (%) for nominal variables. Group comparisons were performed between the four AD groups with analysis of variance for continuous variables and chi square test for nominal variables. aSignificant (F, p < 0.05) versus LOAD APOE ɛ4 +; bSignificant (F, p < 0.05) versus LOAD APOE ɛ4 –; cSignificant (F, p < 0.05) versus EOAD APOE ɛ4 +; dSignificant (F, p < 0.05) versus EOAD APOE ɛ4 –; eSignificant (F, p < 0.05) versus OC; fSignificant (χ2, p < 0.05) for group difference by chi square test. EOAD, early onset Alzheimer’s disease; YC, young control; LOAD, late onset Alzheimer’s disease; OC, old control; MMSE, Mini-Mental State Examination; CDR SOB, Clinical Dementia Rating– sum of boxes; WMH, white matter hyperintensity; PWMH, periventricular white matter hyperintensity; DWMH, deep white matter hyperintensity; CTh, cortical thickness; ICV, intracranial volume.
In imaging measures, however, LOAD ɛ4- patients showed the lowest amyloid positivity (90.5%, p < 0.05) and the highest total white matter hyperintensity volume among all groups (14490.38±11120.60 mm3, p < 0.05). EOAD ɛ4- patients showed the least mean cortical thickness (2.23±0.16 mm, p < 0.05) and LOAD ɛ4+ patients showed the smallest hippocampal volume (2719.38±422.11 mm3, p < 0.05 versus EOAD ɛ4-).
Cerebrovascular disease markers, such as periventricular (p < 0.05) or volumes of deep (p < 0.05) white matter hyperintensities were greater in the LOAD ɛ4- patients than LOAD ɛ4+, while remaining comparable between EOAD ɛ4+ and EOAD ɛ4-. The neuropsychological test results among the groups showed that the EOAD ɛ4- group had reduced scores for attention, visuoconstruction, and visual memory functions (Supplementary Table 1).
Regional SUVR of THK and FLUTE PET
Table 2 shows the regional SUVR values for THK PET in all groups. In the dementia groups, the EOAD ɛ4- group showed increased THK retention in the superior parietal (p < 0.001), inferior parietal (p < 0.001), and precuneus (p < 0.001) cortices compared to the LOAD ɛ4- and ɛ4+ groups. The LOAD ɛ4+ group showed greater THK retention in the medial temporal region (p < 0.001) than the EOAD ɛ4- and ɛ4+ groups.
Regional SUVR of [18F] THK5351 PET
Data are presented as mean±standard deviation. Analysis of covariance with pairwise group comparisons were performed after adjusting for year of education aSignificant (F, p < 0.05) versus LOAD APOE ɛ4 +; bSignificant (F, p < 0.05) versus LOAD APOE ɛ4 –; cSignificant (F, p < 0.05) versus EOAD APOE ɛ4 +; dSignificant (F, p < 0.05) versus EOAD APOE ɛ4 –; eSignificant (F, p < 0.05) versus OC. All significant ROIs survived region-wise FDR correction for multiple comparisons. SUVR, standardized uptake value ratio; PET, positron emission tomography; ROI, region of interest; EOAD, early-onset Alzheimer’s disease; YC, young control; LOAD, late-onset Alzheimer’s disease; OC, old control.
FLUTE retention was generally and significantly increased in the EOAD ɛ4- group when compared to the LOAD ɛ4- and ɛ4+ groups. Regional SUVR values for FLUTE PET are presented in Supplementary Table 2.
Voxel-wise THK retention in patient groups
Figure 1A shows group differences according to APOE ɛ4 status. EOAD ɛ4+ showed greater THK retention in the anterior cingulate and occipital cortex, while EOAD ɛ4- showed greater THK retention in the bilateral dorsolateral prefrontal, inferior parietal, and lateral temporal cortices. LOAD ɛ4+ showed increased THK retention in the medial temporal cortex, while LOAD ɛ4- showed increased THK retention in some regions of the dorsolateral prefrontal and parietal cortices. EOAD groups showed larger differences due to the APOE ɛ4 allele than the LOAD groups.
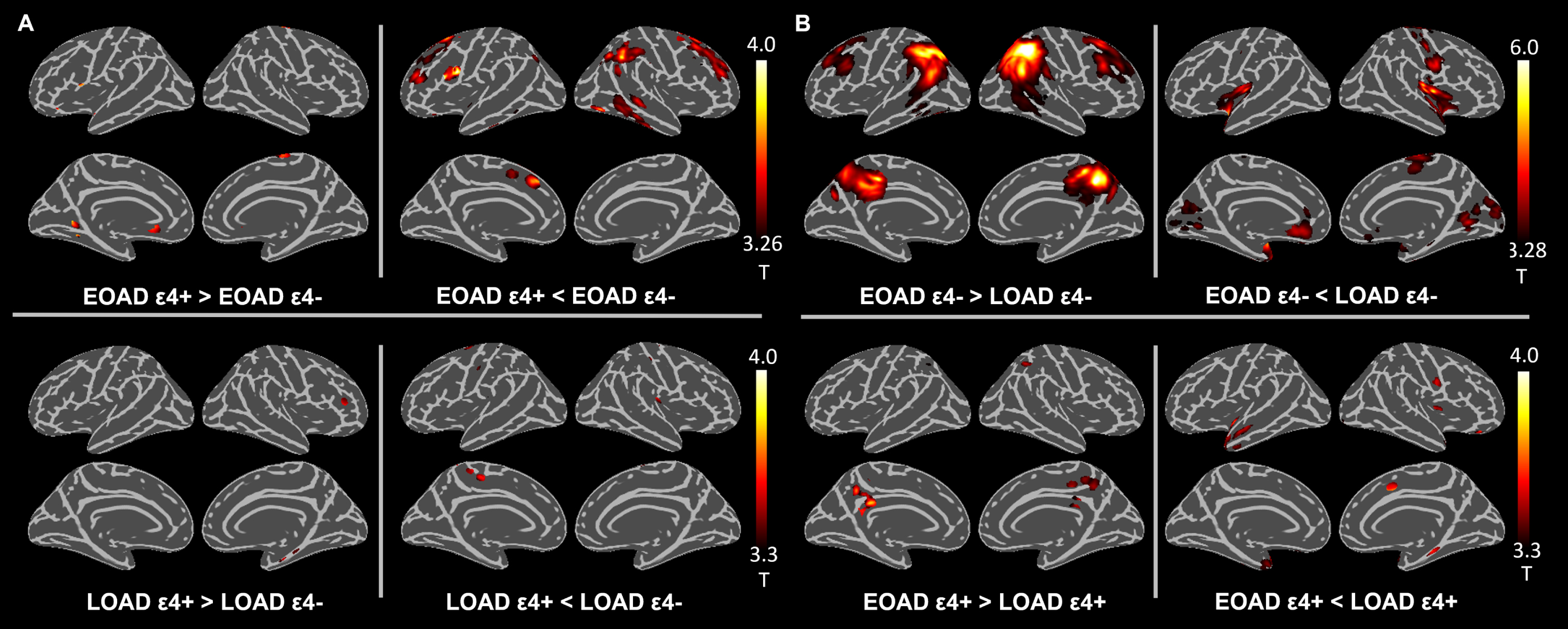
Differences in 18F-THK5351 retention according to APOE genotyping and onset age. Differences in 18F-THK5351 retention between groups according to: (A) APOE genotyping and (B) onset age are presented after adjustment for age (only for same-age group comparisons), sex, and educational years at uncorrected p < 0.001. EOAD, early-onset Alzheimer’s disease; APOE, apolipoprotein E; YC, young control; LOAD, late-onset Alzheimer’s disease; OC, old control.
Figure 1B shows group differences identified according to age at onset. EOAD ɛ4- showed more THK retention in the parietal, precuneus, and dorsolateral prefrontal cortices compared to LOAD ɛ4-, while LOAD ɛ4- showed more THK retention in the anterior cingulate, occipital, and medial temporal areas compared to EOAD ɛ4-. Comparisons between EOAD ɛ4+ and LOAD ɛ4+ showed greater retention in the medial parietal and lesser retention in the medial temporal and occipital cortices in EOAD ɛ4+, although the difference was small.
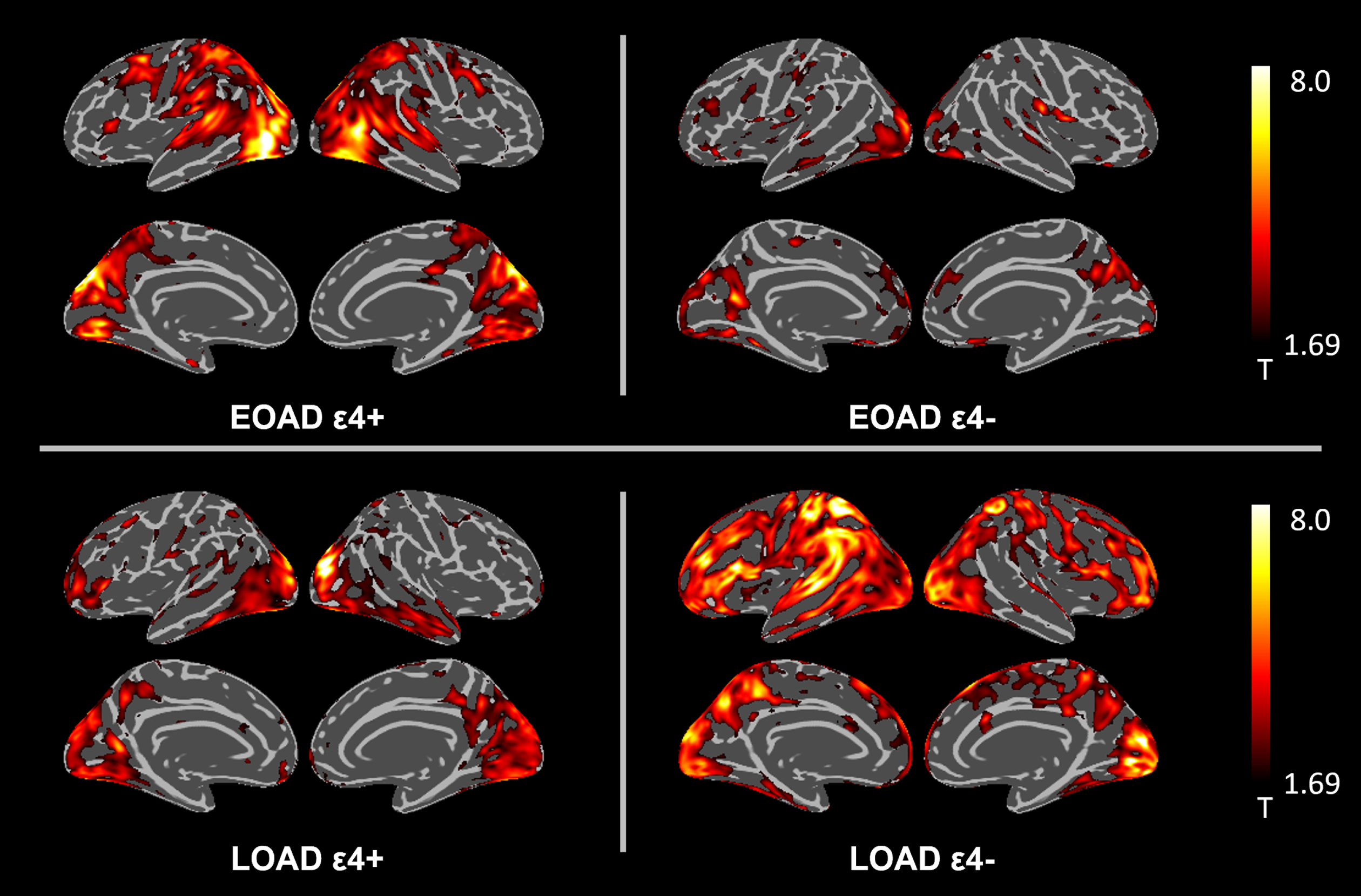
Voxel-wise THK retention comparing each patient group to their age-matched controls are presented in Supplementary Figure 1. The EOAD ɛ4- group showed the greatest retention in the association cortices such as dorsolateral prefrontal and parietal cortices. The EOAD ɛ4+ group showed THK retention in the lateral temporal and inferior parietal cortices and precuneus while the LOAD ɛ4+ group showed THK retention more distinctly in the medial temporal and inferior temporal regions, while the LOAD ɛ4- group showed the least THK retention.
Correlations between THK and FLUTE retention
Figure 2 shows correlations between intra-voxel THK and FLUTE retention in each group. EOAD ɛ4- showed sparse correlation between THK and FLUTE. Meanwhile, LOAD ɛ4- had significantly more generalized cortical regions where THK and FLUTE had significant positive correlations. APOE ɛ4 carrier groups appeared to be in between the findings for the EOAD ɛ4- and LOAD ɛ4- groups. Correlation matrix of results from partial correlations in each group showed similar results (Supplementary Figure 2).
Intra-voxel correlation between THK and FLUTE with BPM analysis. Intra-voxel correlation was performed after adjusting for age and educational years with significance defined as an uncorrected p < 0.01. FLUTE, flutemetamol; BPM, biological parametric mapping; EOAD, early-onset Alzheimer’s disease; LOAD, late-onset Alzheimer’s disease; ɛ4, apolipoprotein ɛ4; L, left; R, right.
Supplementary Figure 3 shows the scatter plots indicating global FLUTE retention in the x axis and global THK retention in the y axis. Scatter plots of global SUVRs in both THK and FLUTE in the EOAD ɛ4- and LOAD ɛ4- showed quite different distribution, whereas those in the EOAD ɛ4+ and LOAD ɛ4+ groups intermingled each other.
Association between THK and mean cortical thickness
Figure 3 shows the negative association between THK retention and mean cortical thickness. In the EOAD ɛ4- group, the thinner the cortex, the larger the area of greater THK retention. In the EOAD ɛ4+ group, the brain regions where THK retention was observed to increase as mean cortical thickness decreased were the precuneus, lateral temporal, and inferior parietal cortices. Contrary to EOAD ɛ4+, LOAD ɛ4+ showed greater THK retention in the medial and anterior temporal cortices according to cortical atrophy. LOAD ɛ4- showed the smallest number of regions correlating with cortical atrophy.
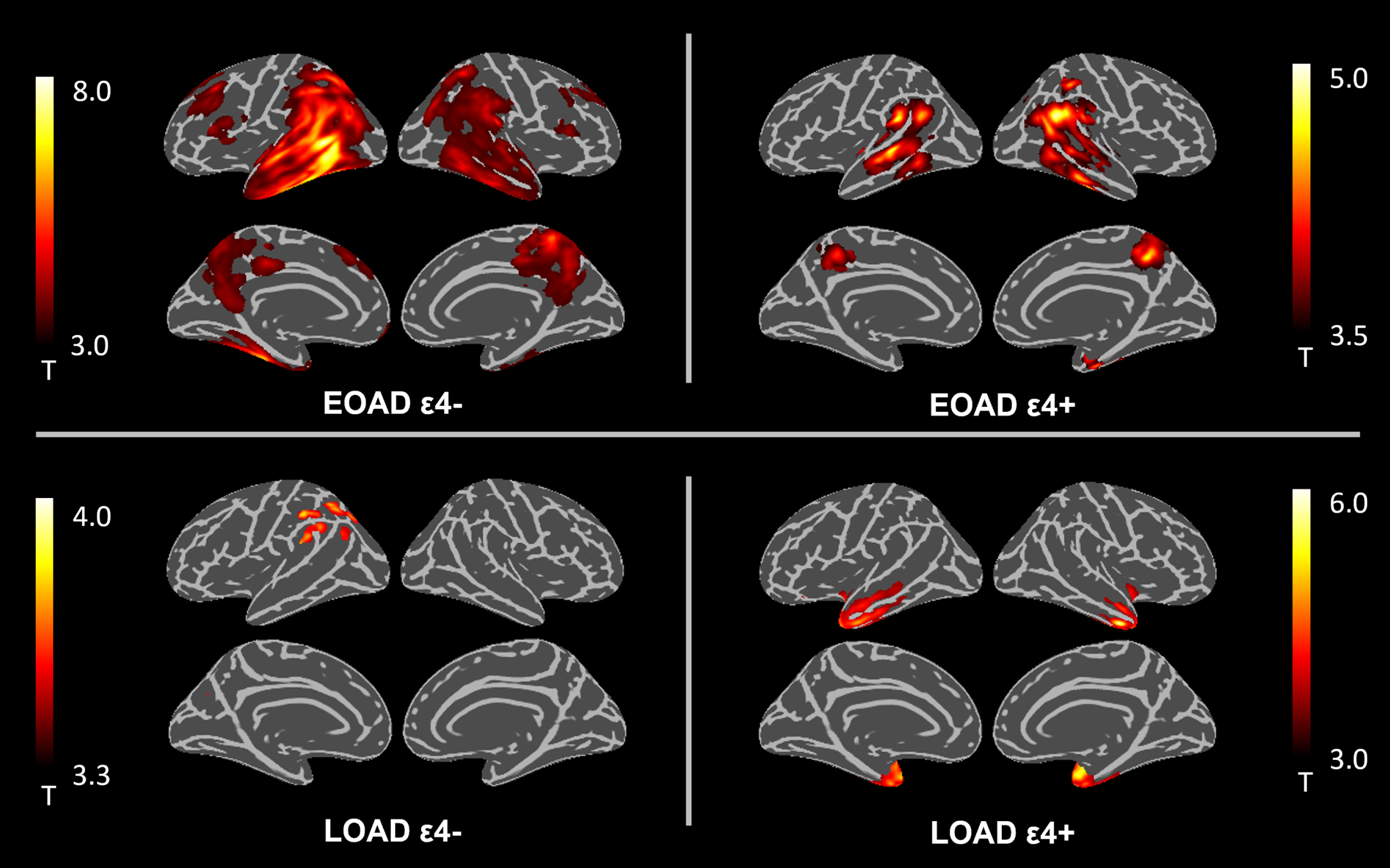
THK retention showing a significant negative correlation with mean cortical thickness. Correlations are adjusted for age, sex, and educational years at uncorrected p < 0.001. APOE, apolipoprotein E; FLUTE, flutemetamol; EOAD, early-onset Alzheimer’s disease; LOAD, late-onset Alzheimer’s disease.
Neuropsychological test results associated with THK
Correlations between neuropsychological test results in the four groups according to age at onset and APOE positivity are presented in Supplementary Tables 3–6. Cognitive function significantly correlated with cortical THK retention in all groups except for the LOAD ɛ4- group that showed almost no association. The EOAD ɛ4- group showed the most prominent association between THK and cognitive functions: BNT, RCFT copy test, and RCFT immediate recall were correlated with the parietal and temporal areas (Supplementary Table 3). SPM results of the association between THK and MMSE or CDR SOB are presented in Fig. 4. Association between THK and other cognitive test results are shown in Supplementary Figures 4 and 5 that replicated the greatest increased association between THK and cognitive function in the EOAD ɛ4- group. Frontal executive function such as COWAT animal and confrontational naming ability was associated with THK retention in large areas including the dorsolateral prefrontal, parietal, and temporal cortices in the EOAD ɛ4- group.
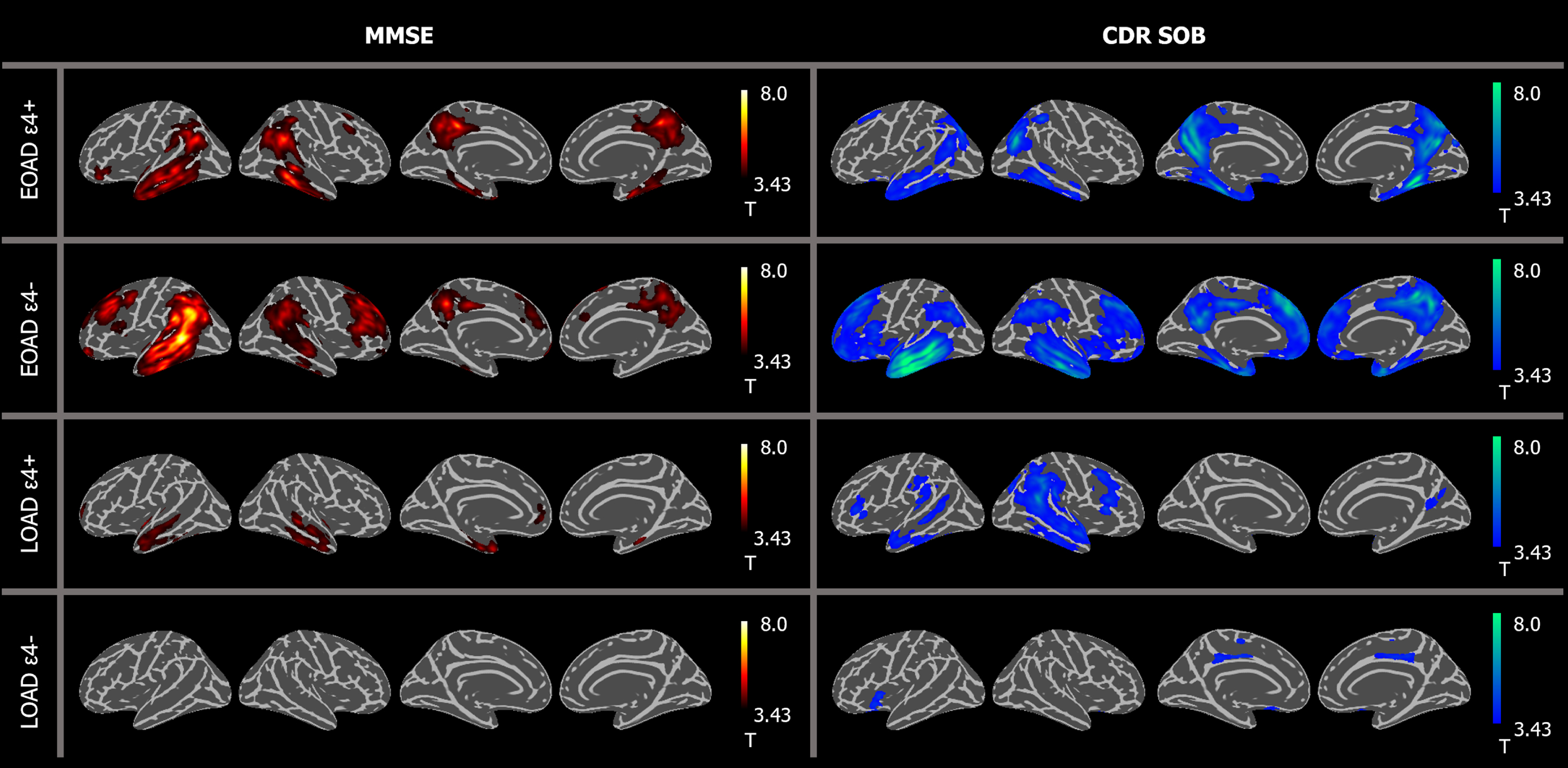
Relationship between THK retention and global cognition. The relationships between regional THK retention and MMSE or CDR SOB in each group are presented after adjusting for age and years of education at uncorrected p < 0.001. EOAD, early-onset Alzheimer’s disease; LOAD, late-onset Alzheimer’s disease; MMSE, Mini-Mental Status Examination; CDR SOB, Clinical Dementia Rating sum of boxes.
DISCUSSION
In this study, we investigated the differential effect of APOE ɛ4 positivity and age at onset on THK, FLUTE, MRI, and cognitive function. The EOAD ɛ4- group showed predominant atypical features of AD including extra-temporal THK retention correlated with dysexecutive function. In the EOAD ɛ4+ and LOAD ɛ4+ groups, the pattern of THK retention and its association with FLUTE and cortical thickness was comparable. The LOAD ɛ4- group showed a process combined with senile changes such as less amyloid burden, distinct memory decline, and increased white matter hyperintensities. These results suggest a differential effect of APOE ɛ4 positivity on the brains of AD patients in association with age at onset.
The major finding of this study is a differential effect of APOE ɛ4 on THK retention in association with age at onset. Among all groups, the EOAD ɛ4- group showed increased hippocampal-sparing THK retention in the precuneus and parietal cortices compared to the other three groups, while the LOAD ɛ4+ group showed more THK retention in the typical regions of AD including the medial temporal region. Previous studies have reported the different impact of onset age on tau PET uptake, with tau accumulating in diffuse cortices including the parietal regions in EOAD while this occurs distinctly in the temporal regions in LOAD [19–21]. The impact of APOE ɛ4 on the differential distribution of tau in AD has also been found. In LOAD with APOE ɛ4, 18F-AV-1451 burden was significantly observed in the temporal and entorhinal cortices and hippocampus [16, 41]. In the present study, we replicated these results with THK retention in the parietal cortex in LOAD ɛ4- and in the medial temporal cortex in the LOAD ɛ4+ group. In EOAD, we also found that the ɛ4- group showed higher THK retention in the diffuse neocortical regions while the ɛ4+ group showed relatively increased THK in the anterior cingulate and medial temporal cortices. This is in line with previous findings that EOAD exhibits atypical parietal predominant tau pathology and the absence of APOE ɛ4 being associated with diffuse volume loss and hypometabolism in EOAD [12, 18]. Even in APOE ɛ4 carriers, we found that EOAD ɛ4+ had greater THK retention in the parietal cortex and LOAD ɛ4+ had more in the medial temporal cortex. These results may also imply a differential effect of APOE ɛ4 on tau accumulation according to age at onset. Another finding is the differential association between tau and amyloid regarding APOE ɛ4 positivity and onset age. The association between THK and FLUTE was significant in more generalized cortical regions in increasing order: EOAD ɛ4-, LOAD ɛ4+, EOAD ɛ4+, and LOAD ɛ4-. It has been found that tau has more localized and symptom-reflective retention than the amyloid deposits that accumulate diffusely throughout association neocortices [21, 42]. Previous authors have theorized that APOE ɛ4 influences brain amyloid and tau deposition in complex mechanisms such as association between APOE and medial temporal tau independent of amyloid [41, 43], synergistic effects of APOE and amyloid on tau retention [44], and a moderating influence of APOE on the effect of medial temporal tau on cognitive function independent of amyloid pathology [45]. The present study is the first to compare the relationship between regional amyloid and tau PET uptake among the four groups stratified by age at onset and APOE ɛ4 positivity. In the EOAD groups, the EOAD ɛ4+ group showed greater correlation between tau and amyloid retention than the EOAD ɛ4- group. We can postulate that EOAD ɛ4+ patients might face more Aβ accumulation than EOAD ɛ4- patients [46] and accelerated tau retention by APOE ɛ4 [19, 44]. It is notable that the stronger association between tau and amyloid was found in LOAD ɛ4- than in LOAD ɛ4+ patients in this study. This reaffirms similar results in a recent study that found conversely greater Aβ burden and widespread extra-temporal tau retention in the LOAD ɛ4- group compared to LOAD ɛ4+ [16]. This discrepant effect of the APOE ɛ4 allele on the association of tau and Aβ in EOAD and LOAD might be contributing to a larger proportion of the hippocampal-sparing subtype of tau deposition in EOAD groups [11, 47] and the general and multi-faceted senile changes in relatively old LOAD groups [48].
Comparisons of cortical thickness and clinical information including cerebrovascular pathologies and cognitive function among groups also supported the differential effects of APOE ɛ4 and age at onset. The EOAD ɛ4- group showed the highest tau retention, cortical thinning, the association between THK retention and cortical thinning, and the association between THK retention and region-specific cognitive function. In contrast, the LOAD ɛ4- group showed the greatest increase in cerebrovascular small vessel disease markers by MRI, such as the volume of white matter hyperintensity and the number of lacunes, and the least association between THK retention and cortical thickness or cognitive function. It has been reported previously that medial temporal tau retention correlates with verbal memory dysfunction in LOAD patients, while the greater parieto-occipital tau binding in EOAD correlates more with visuospatial and executive function than in LOAD patients [8, 19] and these reflections of cognitive function are comparable in relation to cortical thickness but not with amyloid PET uptake [21, 50]. A lack of APOE ɛ4 has also been associated with more pronounced non-memory deficits in EOAD [14, 15], as we observed in this study. Additionally, as other important changes such as neuroinflammation, cholinergic dysfunction, cerebrovascular pathologic events, and the effect of possible other cognitive reservoirs can also occur during AD pathology especially in older groups, the LOAD ɛ4- group in this study might be characterized by complex senile mechanisms [51].
Taken together, our findings suggest a spectrum of hypothetical relationships among APOE ɛ4, onset age, tau, and amyloid shown in the four groups: EOAD ɛ4-, EOAD ɛ4+, LOAD ɛ4+, and LOAD ɛ4 + . In EOAD ɛ4-, tau and amyloid may develop independently and tau may accumulate with a neocortical predilection. In the APOE ɛ4+ groups, THK tended to correlate with FLUTE and mean cortical thickness in the inferior parietal region in EOAD and in the medial temporal region in LOAD. In the LOAD ɛ4+ group, APOE may affect amyloid accumulation strongly, with the APOE effect overriding the relationship between amyloid and tau resulting in the most typical characteristics of AD. Lastly, in LOAD ɛ4-, more complicated processes including tau and amyloid may develop synergistically according to senile changes.
We wish to note several limitations to our findings. First, we should acknowledge that THK5351 PET images are confounded by MAO-B availability across the entire brain, so caution is warranted for interpretation [52]. Another limitation of our study is its cross-sectional nature, which means we cannot establish a temporal relationship. As we treated APOE ɛ4 positivity and age group as binary variables, we were unable to observe any dose-response effects. Furthermore, we lack environmental factors or lifestyle choices, such as physical activity, nutrition, and cognitive engagement, that may differ between EOAD and LOAD and may depend on APOE ɛ4 status. Because the pathology and interactions may vary depending on the onset age and APOE ɛ4, longitudinal follow-up studies that investigate these modifiable factors will be necessary. To support our hypotheses, further studies with longitudinal follow-up, pathologic data, and careful consideration of confounding factors, as well as the use of tau PET radiotracers with minimal off-target binding affinity, arenecessary.
Conclusion
Our observations suggest that there are differential effects of the APOE ɛ4 allele on the relationship between tau and Aβ in EOAD and LOAD. In EOAD ɛ4- patients, most of whom exhibit hippocampal-sparing type AD, prominent tau may develop independent of amyloid. EOAD ɛ4+ and LOAD ɛ4+ lies in between APOE ɛ4- patients. In LOAD ɛ4- patients, a more combined process including vascular or other degenerative pathologies. Although APOE ɛ4 allele is known to manifest typical AD symptoms, the effect of APOE on the relationship between tau, amyloid, and cortical thickness may be different in EOAD and LOAD. Further studies are warranted to ascertain the complicated interactions between genotype and other demographic and pathological factors in AD.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This study was supported by a grant from the Korea Healthcare Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare of the Republic of Korea (grant No: HI14C1135), a grant from the Brain Research Program of the National Research Foundation (NRF), funded by the Korean government (MSIT) (No. 2018M3C7A1056889) and a grant from the Basic Science Research Program through the National Research Foundation of Korea (NRF) that is funded by the Ministry of Education (2021R1A6A1A03038996).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.