
Abstract
Background:
The eye may serve as source for diagnostic testing for early detection of Alzheimer’s disease (AD). Examination of amyloid-β (Aβ) and tau protein content in human vitreous and its correlation to neuro-cognition may improve ocular-based AD detection methods.
Objective:
To evaluate levels of Aβ and tau protein in human vitreous humor and investigate the clinical predictive role of these proteins as early diagnostic markers of AD.
Methods:
A prospective, single-center, multi-surgeon cohort study. Vitreous humor samples from 80 eyes were measured quantitatively for Aβ40-42, pTau, and tTau. Linear regression was used to test associations between AD biomarker levels, Mini-Mental State Exam (MMSE), and serum apolipoprotein E (APOE) allele status, with adjustment for age, sex, and education level of patients.
Results:
Lower MMSE scores were significantly associated with lower levels of vitreous Aβ40 (p = 0.015), Aβ42 (p = 0.0066), and tTau (p = 0.0085), and these biomarkers were not associated with any pre-existing eye conditions. Presence of the ɛ4 allele and the ɛ2 allele approached significance with reduced Aβ40 level (p = 0.053) and increased p-Tau level (p = 0.056), respectively.
Conclusion:
Patients with poor cognitive function have significantly lower vitreous humor levels of AD-related biomarkers Aβ40, Aβ42, and tTau. These biomarkers do not correlate with underlying eye conditions, suggesting their specificity in association with cognitive change. This is the first study to our knowledge to correlate cognition with AD-related proteins in the vitreous humor. Results suggest ocular proteins may have a role for early dementia detection in individuals at risk for AD.
INTRODUCTION
Alzheimer’s disease (AD) is a chronic neurodegenerative disease that represents the most common form of dementia, accounting for 60–70% of dementia cases worldwide [1, 2]. Abnormal aggregates of amyloid-β (Aβ) and tau protein are histological hallmarks of the disease, and deposition of Aβ plaques begins many years prior to the onset of clinical symptoms [3]. Early treatment is essential to preventing disease progression, but early disease detection is limited by a lack of low cost screening tests that can be applied broadly [4].
The outer layers of the eye, including the retina, share a common neuro-ectodermal embryological origin and vasculature with the brain [5, 6] and there are many similarities between the inner blood-brain barrier and the blood-retinal barrier. These anatomical similarities permit common manifestations of disease among the eye and brain, and as an optical system, the eye provides a direct window to display neuro-retinal disease [7]. Through non-invasive visualization, the eye can serve as a barometer of neural integrity and aid in the prediction, diagnosis, and prognosis of neurological disease such as stroke, multiple sclerosis, and Parkinson’s disease. A similar association exists between the eye and amyloid-based diseases. Many studies have shown associations between ocular pathology and AD [8–20]. AD related proteins have been isolated in the aqueous and vitreous humor [19, 21–26], and AD and brain Aβ burden has been shown to be associated with Aβ deposits in the lens and retina in animal models [27–32] and human studies [33–37]. Individuals with glaucoma, age-related macular degeneration, and diabetic retinopathy have been shown to be at increased risk of AD [38], and eye manifestations such as retinal nerve fiber layer attenuation or loss [8–20, 39–49] may offer a predictive value for AD detection.
With regard to early disease detection, emphasis has been placed on the diagnostic utility of protein markers in cerebrospinal fluid (CSF), and CSF levels of Aβ and tau correlate with cognitive function in individuals with AD [4, 50–58]. Sampling of ocular fluid for diagnostic testing is performed routinely for many conditions, such as CNS lymphoma, viral syndromes, bacterial and fungal infections, and amyloidosis, and we postulate that analysis of ocular fluid may have clinical utility in early AD detection. This study was initiated to quantify AD protein biomarkers in human vitreous humor of patients with eye disease and to determine whether levels of these proteins correlate with measured cognition levels. While prior studies have shown Aβ levels in ocular tissues of animal models and postmortem AD patients, this is the first study to our knowledge to correlate human cognitive status with AD-related protein levels in the eye in a non-AD cohort.
MATERIALS AND METHODS
Study Design
This was a single site multi-surgeon prospective cross-sectional cohort study. The study protocol was approved and overseen by the Boston Medical Center and Boston University Medical Campus Institutional Review Board; the study was performed in accord with the ethical standards of the Committee on Human Experimentation of our institution and the Declaration of Helsinki.
Patients were eligible for study participation if they were greater than 18 years of age, spoke English or Spanish, and were scheduled for vitrectomy surgery in at least one eye as part of standard care. Indications for surgery included various vitreoretinal disorders, such as rhegmatogenous retinal detachment, epiretinal membrane, macular hole, retained lens fragment, and vitreous hemorrhage or tractional retinal detachment due to diabetic retinopathy (DR). Written informed consent was obtained from patients who agreed to participate.
Demographic and MMSE Data Collection
Once enrolled, clinical and demographic data were obtained through a combination of a patient questionnaire and electronic medical record review. Information was collected on patient race, highest level of education, smoking history, baseline color vision, ocular history, medical history, family history of cognitive dysfunction, family history of ocular disease, athletic history, military history, history of head and/or neck injuries, and subjective cognitive complaints. Patients were not excluded on the basis of race or coexisting ocular or medical morbidities. A Mini-Mental State Examination (MMSE) was administered to all patients upon enrollment in the study and prior to their eye surgery.
Biospecimen Collection
At the start of the vitrectomy procedure, the surgical team aspirated 0.5–1.0 mL of undiluted vitreous fluid through the vitrectomy probe into an attached sterile 3 mL syringe. Once the undiluted vitreous specimen was collected, saline was immediately infused into the vitreous cavity to re-pressurize the eye. Biologic samples were removed from the eye, capped in sterile fashion, handed directly to a research assistant, and labeled with a non-identifiable study identification number. Apart from the collection of the vitreous samples, the entire operation for each study participant proceeded as it would under standard of care conditions. Samples were transported immediately to the laboratory on ice and stored at –80°C.
Biospecimen Analyses
Vitreous samples were centrifuged for 15 min at 12,000 rpm to separate the cellular contents, aliquoted at 100μL, and frozen at –80°C. Protein measurements were performed using the multi-detection SPECTOR 6000 Imager (Meso Scale Discovery (MSD), Rockville, MD) for immunoassay. A 100μL volume of vitreous fluid aliquot was diluted 1:1 with 1% Blocker A (MSD #R3BA 4) in wash buffer for a total volume of 200μL.
Samples were subsequently spun down at 17,000 g and 4°C for 15 min, and the supernatant was applied to the immunoassay. Assays were run per the manufacturer’s instructions and in duplicate. Standard immunoassay was used for beta-amyloid 1–40 and 1–42 (MSD #K15200E-2) and tau phosphorylated at threonine 181 (pTau181) together with total tau (MSD #K15121D-2), using capturing antibody AT270 against pTau181 (Thermo Scientific #MN1050) and T46 antibody against total tau as the detecting antibody (Thermo Scientific). Sulfo-tag conjugated anti-mouse secondary antibody (MSD) was used for signal detection by the MSD platform, and an MSD SECTOR S 600 Imager was used to measure analyte levels.
Apolipoprotein E (APOE) Genotyping
DNA was extracted from blood using a Qiagen QIAamp DNA extraction kit (Qiagen, Valencia, CA). Two single nucleotide polymorphisms (National Center for Biotechnology Information SNPs rs429358 and rs7412) were examined using TaqMan assays (Applied Biosystems, Foster City, CA). Allelic discrimination was automated using the manufacturer’s software. Positive controls, consisting of DNA for each APOE allele, were included on each plate and genotyped with restriction isotyping.
Statistical Analysis
Linear regression was used to test associations among AD biomarker levels, MMSE scores, and APOE allele number. The AD biomarker levels which were greater than zero were used after log transformation to fit the skewed distributions for the regression [59]. The associations for AD biomarker levels with MMSE scores were assessed, as well as associations between AD biomarker levels and APOE ɛ2 and ɛ4 allele number [60]. Associations between ocular conditions and AD biomarker levels were also assessed. Age and sex were used as covariates for all the models. We categorized education by degree or level, including 1) less than or equal to 8th grade level; 2) 9th grade to high school; and 3) greater than or equal to college (bachelors or associates), as done in a prior analysis [61, 62]. In regression models where MMSE was the outcome, education level was used as the covariate since the education levels of the patients could be associated with the performance MMSE task [63]. P-values of less than 0.05 were regarded as statistically significant, and in this exploratory study no correction was made for multiple comparisons.
RESULTS
Of the 95 patients recruited, a total of 80 patients were included for analysis; 15 were excluded from the study. Reasons for exclusion included incomplete vitreous specimen collection, insufficient or no blood collection, storage and labeling discrepancies, patient(s) did not meet literacy requirements, and/or elective withdrawal from the study. Of the 80 patients included in analysis, there were 53 males and 27 females. The range of age was 19–87 years. Mean age among females was 60.8 years (n = 27, SD 17.9) and mean age among males was 53.2 years (n = 53, SD 13.4). Twenty-nine individuals self-identified as White Caucasian, 28 as Black or African American, 12 Hispanic, 3 Asian, 1 American Indian or Alaska Native, and 7 as other (2 Portuguese, 1 Spanish, 1 Brazilian, 1 Japanese/Polish, and 2 declined to report). Summary statistics of the AD biomarker levels are described in Table 1.
AD biomarker levels in picograms per milliliter (pg/ml)
Among the 80 study participants, the mean MMSE score was 27 (mean of 27.4 among females (n = 27, SD 3.6) and 26.9 among males (n = 53, SD 3.0). MMSE score mean, range and median values are presented in Table 2 and are separated by level of education. In the 8th grade education level group, 40% of these individuals had abnormal MMSEs, with 30% exhibiting mild cognitive impairment and 10% moderate cognitive impairment. In the high school educated group, 4 of 30 (13%) individuals had mild cognitive impairment and 1 of 30 (3%) had moderate cognitive impairment. In the college educated group, 4 of 40 (10%) individuals had mild cognitive impairment. Parameters for impairment level (mild versus moderate) are provided in the footnote for Table 2 [62, 63]. Descriptive qualifications of cognitive impairment based on MMSE scores are not uniform among the literature. While scores of <24 are generally considered abnormal, MMSE scores can be influenced by education level. College-educated individuals with MMSE scores less than 27 have been shown to have a greater risk of dementia [63]. Therefore, individuals with scores <27 in this category were designated as having cognitive impairment.
Distribution of level of education among patients and MMSE scores
†Associate or Bachelors degree. *In 8th grade and high school groups, mild cognitive impairment was indicated by an MMSE score of 19–23; and moderate cognitive impairment by an MMSE score of 10–18; In the college group, mild cognitive impairment was indicated by an MMSE score of <27; no MMSE scores were below 25 in this group.
In the association tests with the AD biomarkers, lower MMSE scores, indicating poorer cognitive function, were significantly associated with lower levels of Aβ40 (p = 0.015), Aβ42 (p = 0.0066), and tTau (p = 0.0085) (Table 3A, Fig. 1a-c) in the vitreous humor. The level of p-Tau181 was not associated with MMSE scores (p = 0.40). In some of the vitreous samples, the measured protein levels were less than the assay detection limits (Aβ40, n = 2; Aβ42, n = 3; tTau, n = 8; p-Tau181, n = 5), and these were excluded from the analyses. AD biomarkers were also analyzed against the two APOE alleles (ɛ2, n = 17 and ɛ4, n = 21) in study patients. We observed an association between the ɛ4 allele with reduced Aβ40 level (p = 0.053) and the ɛ2 allele with increased p-Tau level (p = 0.056), but these associations did not reach statistical significance (Table 3A, Fig. 2a, b).
Regression results for AD markers versus MMSE scores and APOE allele count, controlling for age, sex and education
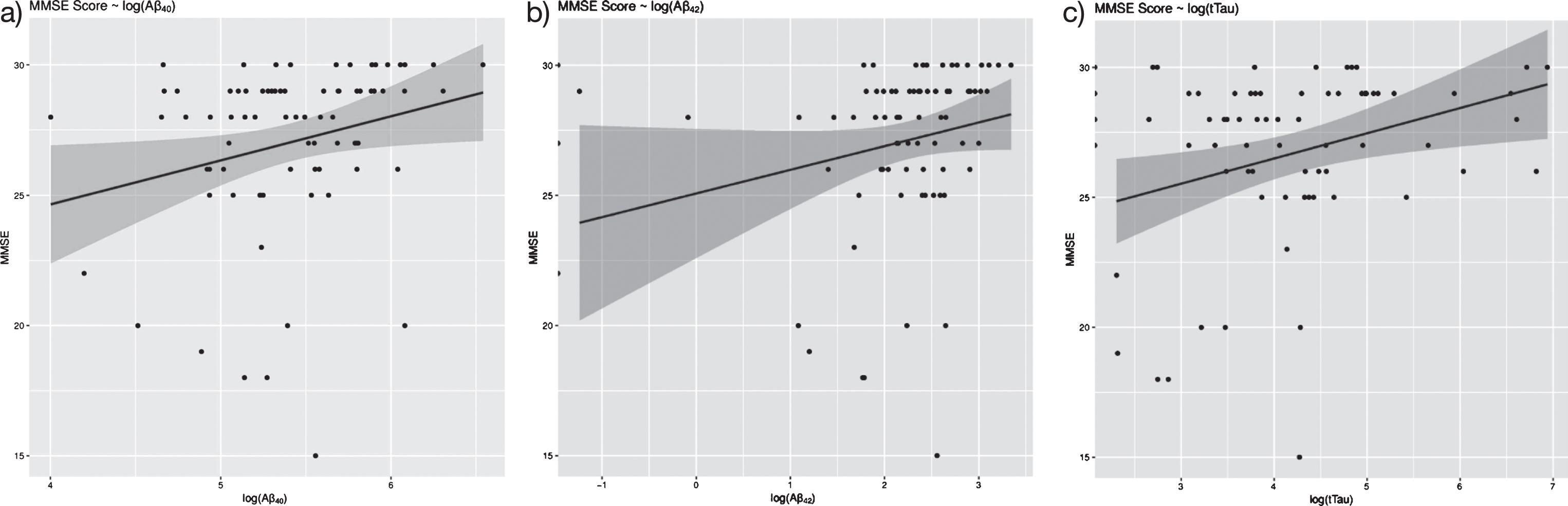
MMSE scores versus vitreous AD biomarkers in patients undergoing vitrectomy surgery. Lower MMSE scores (i.e., lower cognitive status) correlated with lower vitreous levels of Aβ40, Aβ42, and tTau. Linear regression analyses are shown for MMSE versus (a) log(Aβ40) (n = 78, p = 0.015), (b) log(Aβ42)(n = 77, p = 0.0066), and (c) log(tTau) (n = 75, 0.0085).

Association of AD biomarkers and APOE alleles. Association between the ɛ4 allele and reduced Aβ40 level approached statistical significance (p = 0.053) (a), as did the association between the ɛ2 allele and increased p-Tau level (p = 0.056) (b). Associations were adjusted for age, sex, and education level. A value of “0” on the x-axis denotes non-carrier status, and “1” denotes carrier status.
Co-existent ocular conditions among study participants are presented in Supplementary Table 1. The association between ocular conditions and biomarker levels were analyzed, and vitreous biomarkers were not associated with most co-existent ocular conditions. However, levels of pTau181 and DR and age-related cataract (ARC) approached statistical significance. To investigate whether the presence of DR and ARC confounded associations between MMSE scores and biomarker levels, association tests were reconstructed after adjusting for DR and ARC (Table 3A, B). We did not observe any notable difference from the association tests after adjusting for DR and ARC, compared with the associations before adjusting for these two conditions. Table 4 shows in detail the association between each ocular condition and all biomarker levels.
Regression results for AD markers versus MMSE and APOE alleles after adjusting for age, sex, education; diabetic retinopathy and age-related cataract were additionally adjusted for
Association summary between the AD biomarker levels and co-existing eye diseases. AD biomarkers were used as the outcome, and disease status was used as the predictor. Age and sex were used as covariates. Significant associations are shown in bold
AMD, age-related macular degeneration; DR, diabetic retinopathy; GL, glaucoma; ARC, age-related cataract; RD, retinal detachment; MH, macular hole.
DISCUSSION
Prior studies have established the predictive value of Aβ1 - 42 peptide and tau protein levels in the CSF for early AD detection [50–58, 65]. All four AD-related proteins were detected in the vitreous humor in our study with lower Aβ40, Aβ42, and tTau significantly associated with lower MMSE scores, controlling for age, sex, and education (Fig. 1a-c). Previous studies have detected vitreous levels of the same proteins in patients with AD [25], but this is the first study to our knowledge to correlate protein quantities with levels of cognition, as measured by the MMSE. Importantly, Aβ40, Aβ42, and tTau levels did not correlate with underlying eye conditions, suggesting their specificity in association with cognitive change.
Although the mechanism by which proteins enter the eye is not known, it is generally accepted that the eye and brain are closely connected, as many diseases that affect the central nervous system can also affect the eye. As such, direct sampling of ocular fluid for quantification of Aβ and tau may provide an accessible and cost-effective means of AD diagnosis and prognostication. In early AD, ocular biomarkers may be present prior to the onset of clinically detectable cognitive impairment or dementia and testing for ocular biomarkers may be helpful for diagnosis.
Prior investigations on the role of the eye in AD have focused primarily on retinal markers of neurodegeneration obtained through ocular imaging techniques, most commonly with optical coherence tomography (OCT) scans or OCT angiography [49]. Specific markers include retinal volume, nerve fiber layer and ganglion cell layer thickness, drusen deposits, and choroidal thickness [8–20, 66]. While these studies suggest that retinal features have a strong association with AD, data obtained by OCT images can be confounded by common eye diseases (such as glaucoma, macular degeneration, and diabetic retinopathy) and the treatment of those eye conditions. Therefore, we postulate that retinal biomarkers measured by OCT images alone may not be sufficient as a diagnostic tool in early AD, and a more comprehensive approach that involves both OCT imaging and eye-based protein biomarkers is needed.
We found the correlation between cognitive function and Aβ levels in the vitreous similar to that of CSF. A decrease in CSF Aβ42 in AD dementia has been validated in numerous papers [50, 67]. However, while tau protein is generally elevated in the CSF of patients with AD and other cognitive diseases [4], we found vitreous tau levels decreased with worse cognitive impairment. The etiology of the discrepancy between vitreous and CSF tau levels is unclear. There is limited information about tau distribution or tangle formation within the eye and prior studies on tau quantification in ocular fluid are limited [24, 25]. The pathophysiologic mechanisms that dictate the tau levels in the eye require further study.
There are several strengths to this study. As none of our patients had a diagnosis of AD, the correlation of vitreous biomarkers and cognitive function suggests a potential future tool for diagnosis of preclinical AD. Our results reaffirm other studies suggesting that patients with eye disease are an at-risk population for the development of AD [19, 38], and suggest that further investigation in patients with eye disease may yield results potentially generalizable to the population at large. Furthermore, the cross-sectional nature of this study performed at an urban academic teaching institution enabled us to capture a diverse group of patients and a broad spectrum of cognitive function.
Limitations to this study exist. As no patients in the study carried a diagnosis of AD, validation studies are needed to compare vitreous levels of AD proteins in patients with diagnosed cognitive impairment or definite AD to normal controls. Another limitation was the variance in co-existing ocular and systemic morbidities among study participants. While our analyses found no significant correlation between biomarkers and most co-existing eye conditions (Table 4), a variety of systemic diseases associated with ocular findings are known to affect cognition. For example, diabetes has been shown to lower cognitive health and increase the risk for development of AD, and many vascular conditions that affect neurologic function would be expected to have some effect on cognitive ability. Furthermore, MMSE is a crude assessment of cognitive function, and while it is highly specific and valid in detection of moderate dementia, in mild dementia it is only 55% sensitive [68]. It would be useful to demonstrate a correlation of ocular levels of Aβ and tau with more in-depth neuropsychological testing, and to correlate protein levels with CSF protein analysis, PET imaging, and serum genotyping. Lastly, in this study, the number of APOE ɛ2 and APOE ɛ4 alleles among study participants was low, which may have lowered the power of the study to detect associations between biomarkers, MMSE, and APOE alleles.
The utility of vitreous biopsy for AD biomarker analysis should also be considered. Vitreous biopsy can be accomplished in the operating room or office setting, but may not be significantly easier than already existing CSF testing techniques. The benefit of diagnostic vitrectomy must be weighed against the potential risk of an invasive procedure. Risks of vitrectomy surgery vary depending on the nature of the procedure performed and can include retinal detachment, hemorrhage, infection, or loss of vision. Diagnostic vitrectomies are performed routinely for diagnosis of primary vitreoretinal lymphoma, amyloidosis, and infectious endophthalmitis, where the need for ocular tissue diagnosis is paramount to guide treatment. In this study, a relatively large volume of vitreous fluid was obtained as it was safe and easy to do so in the operative setting. However, only a fraction of the volume extracted was needed for analysis. Assay detection limits necessitated 100μl of undiluted vitreous fluid. Portable vitrectomy technology is available for minimally invasive sampling of small volumes of vitreous humor which provides a logistically simpler and faster means of vitreous sampling in an office-based setting (VersaVIT 2.0, Synergetic and Intrector portable vitrectomy system, Insight Instruments) [69, 70]. Future directions include investigation to determine if other eye fluids, such as the aqueous humor or tear secretions, which are easier to access and less invasive, contain biomarker levels that are associated with cognition.
In summary, establishing a correlation between cognitive status and the presence of AD-related vitreous proteins is a novel concept that has not been investigated previously. Results of this study reveal an association between vitreous AD-protein levels and cognition, and suggest a potential role for ocular fluid analysis for diagnosis of preclinical AD.