
Abstract
Background:
Although cerebral microbleeds (CMBs) are commonly observed in patients with Alzheimer’s disease (AD), their clinical relevance for AD remains unclear.
Objective:
We investigated the significance of CMBs in AD by examining the relationship between CMBs and cerebral blood flow (CBF) in patients with AD.
Methods:
Thirty-four patients (aged 77.9±7.6 years; 17 men) with probable AD and multiple (≥8) CMBs were selected from 394 consecutive patients. For each lobe of the brain, the correlation between the number of CMBs observed on susceptibility-weighted images and the decrease in CBF observed on single-photon emission computed tomography was assessed.
Results:
The number of microbleeds was significantly correlated with the severity of decrease in the occipital lobe (Spearman’s r = 0.531, p < 0.001) and temporal lobe (r = 0.437, p < 0.001) but not in the frontal lobe (r = 0.201, p = 0.101) and parietal lobe (r = 0.178, p = 0.146). These results were unchanged in the partial correlational analysis after controlling the effect of other small vessel disease such as lacunars and white matter hyperintensities.
Conclusion:
Multiple CMBs are associated with cerebral hypoperfusion in AD. The effects of CMBs on CBF differed according to brain location, possibly reflecting different distributions of the underlying cerebral amyloid angiopathy and AD-related histopathology, such as neurofibrillary tangles.
INTRODUCTION
Cerebral microbleeds (CMBs) are a manifestation of small vessel disease that can be detected using magnetic resonance imaging (MRI). CMBs can be recognized as small hypointense foci in the brain on T2*-weighted gradient-recalled echo or susceptibility-weighted imaging (SWI) and are histologically represented by hemosiderin deposits in macrophages, mainly located around small vessels [1]. CMBs are associated with cerebrovascular disease and dementia, particularly Alzheimer’s disease (AD) [2–5]. CMBs are thought to play a crucial role in the pathophysiology of AD, demonstrating a link between amyloid pathology and neurovascular changes [6]. Most studies have not reported an influence of CMBs on neuropsychological test scores [5, 7]. By contrast, Goos et al. reported a significant impact of CMBs on the severity of cognitive impairment in a study involving AD patients with numerous CMBs [8]. Taken together, these previous findings suggest the possibility that the subtle effects of CMBs on cognitive functions cannot be detected in patients with a small number of CMBs.
In AD, lobar distribution of CMBs is thought to be indicative of cerebral amyloid angiopathy (CAA) [2, 10], while CMBs in deep locations are thought to result from an underlying hypertensive vasculopathy. CAA is a common small vessel disease associated with deposition of amyloid-β (Aβ) protein in the walls of small-to-medium-sized arteries, arterioles, and capillaries [11]. We hypothesized that if CMBs had an impact on the clinical AD manifestations through CAA, their effects on the cerebral blood flow (CBF) may be more prominent than their influence on cognitive impairment. Thus, in the present study, we investigated the possible impact of CMBs on the CBF in AD patients with multiple CMBs.
MATERIALS AND METHODS
Patients
All procedures followed the Clinical Study Guidelines of the Ethics Committee of Kumamoto University, Kumamoto, Japan and were approved by the Internal Review Board. A written informed consent was obtained from patients and their caregivers in compliance with the research standards for human research for all participating institutions and in accordance with the Helsinki Declaration.
Participants were selected from a consecutive series of 394 patients who attended the Dementia Clinic of the Department of Neuropsychiatry, Kumamoto University Hospital from October 2010 to January 2015 and who were diagnosed with probable AD based on the clinical criteria published by the National Institute of Neurological Disorders and Stroke-Alzheimer’s Disease and Related Disorders Association [12]. All study participants were examined comprehensively by three senior neuropsychiatrists (M.I., M.H., and T.I.) with sufficient experience in examining patients with dementia. Participants underwent routine laboratory testing, which included measurements of vitamin B1, vitamin B12, and thyroid function, as well as standardized neuropsychological and neuropsychiatric examinations, including the Mini-Mental State Examination (MMSE) [13] and the Neuropsychiatric Inventory [14]. Structural neuroimaging of the brain was performed using MRI and single-photon emission computed tomography (SPECT) for cerebral perfusion. All results were used to achieve the diagnoses, which were confirmed by a team of neuropsychiatrists, neuropsychologists, and neuroradiologists. Participants who met with the following criteria were excluded from the study: 1) those with an evidence of focal brain lesions on MRI such as traumatic brain injury, brain tumor, or the acute phase of cerebral infarction or cerebral hemorrhage; 2) those who had any evidence suggestive of vascular dementia, such as focal neurological signs, abrupt deterioration, or stepwise progression of the cognitive deficit; 3) those with severe stenosis of the carotid arteries and intracranial cerebral arteries on magnetic resonance angiography; 4) those receiving anticoagulant therapy; 5) those with serious psychiatric diseases such as schizophrenia, major depression, or substance abuse before the onset of dementia, and 6) patients with poor SWI results because of severe motion or susceptibility artifacts.
We retrospectively reviewed the presence and number of CMBs on MRI in patients with AD. The present study consisted of participants with at least eight CMBs in the cerebral cortex. This cutoff was defined according to a previous study [8], resulting in a sample of 34 patients. Table 1 summarizes the clinical characteristics for patients with eight or more CMBs and those with less than eight CMBs. The mean age±standard deviation of the patients with eight or more CMBs was 77.9±7.6 years for the 17 men and 17 women, and the average MMSE score was 17.4±6.0. Twenty-five patients (74%) had hypertension, eight (24%) had diabetes mellitus, eight (24%) had dyslipidemia, and six (18%) received antiplatelet drug therapy.
Clinical characteristics of patients
Values are n or mean±SD. CMBs, cerebral microbleeds; MMSE, Mini-Mental State Examination.
Brain imaging
The major purpose of the present study was to investigate the influence of CMBs on CBF. Therefore, we segmented the cerebral cortex into eight lobar regions (right and left hemisphere)×(frontal, parietal, temporal, and occipital lobes) and examined the possible correlation between the number of CMBs seen on the MRIs and the relative CBF reduction observed on the SPECT image in each lobe.
MRI protocol
MR imaging was performed using a 3T unit (Magnetom Trio; Siemens, Erlangen, Germany). The MRI protocol included axial SWI (64 sections per slab, field of view = 230 mm, matrix = 256×256, section thickness = 2 mm, voxel size = 0.9×0.9×2 mm, TE = 20 ms, TR = 27 ms, flip angle = 15°), axial fluid-attenuated inversion recovery, axial T2-weighted turbo spin-echo, 3D T1-weighted magnetization-prepared rapid acquisition of gradient echo sequences, diffusion-weighted imaging, and MR angiography. SWI processing was performed with a software incorporated into the MR imaging system console, according to published methods [15]. SWIs were constructed by multiplying the magnitude of the signal by the filtered phase images to enhance the susceptibility effect, followed by 16-mm minimum intensity projection reconstruction.
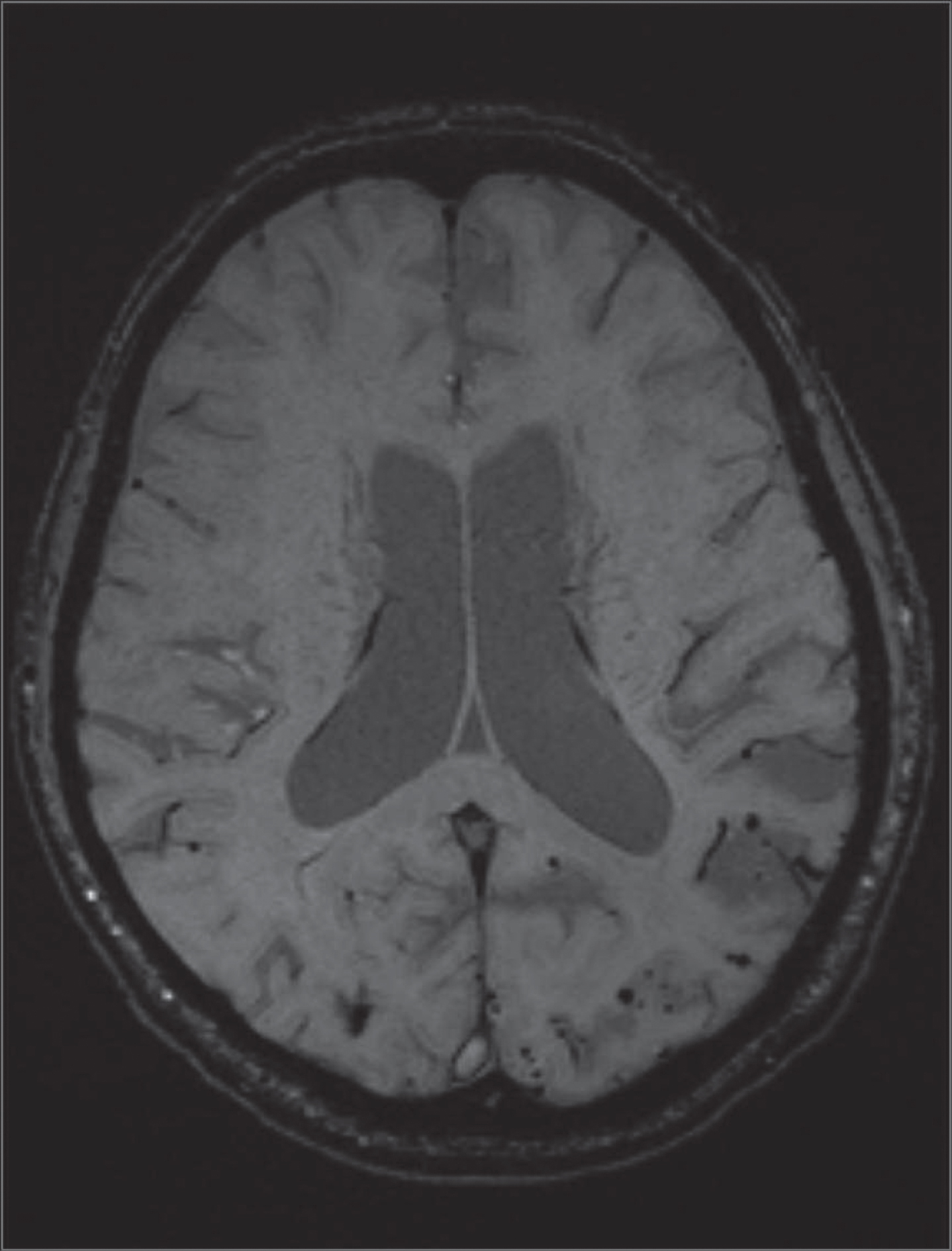
Example of an SWI image of a patient with multiple CMBs. A 78-year-old man with AD presented with many small hypointense foci as seen in the left occipital lobes. SWI, susceptibility-weighted imaging; CMBs, cerebral microbleeds; AD, Alzheimer’s disease.
Evaluation of microbleeds
All SWIs were independently analyzed by one investigator (Y.H.) who was blinded to the clinical data. We assessed the number and location of small hypointense foci on 2-mm contiguous SWI. A 16 minimum intensity projection SWI was used to differentiate the small hypointense foci from veins. Small hypointense foci that suggested microbleeds were structurally defined as homogeneous, round foci of low signal intensity having a diameter <10 mm. Flow-void artifacts of pial blood vessels and hyposignals inside a lesion that were compatible with an infarct were determined as hemorrhagic transformations instead of microbleeds. The total number of hypointense foci in each of the eight regions of analysis was determined.
CMBs are often accompanied by other neuroimaging markers of small vessel disease (SVD) such as cortical superficial siderosis (cSS), lacunars, periventricular white matter hyperintensities (WMH), subcortical WMH, and prominent periventricular spaces, all of which could influence the CBF. Thus, the presence of cSS and lacunars and the degree of WMH were separately determined by a neuroradiologist with sufficient experience examining patients with dementia (N.T.), who was blinded to the clinical data. We defined cSS as linear hypointensities on the surface of cerebral cortex gyri on SWI. Lacunars were defined as lesions with diameters >2 mm hypointensity on T2-weighted images and hyperintensity on FLAIR images. The degree of WMH severity was rated visually on axial FLAIR images using the Fazekas scale as grade 1 (punctate), grade 2 (early confluent), or grade 3 (confluent) both in the periventricular and subcortical region [16]. In the present study, we defined the presence of WMH as Fazekas grade ≥3. We assessed the presence of cSS, lacunars, and WMH in each of eight regions of analysis as with microbleeds. We did not analyze the impact of periventricular spaces on the CBF because of the methodological problems of a quantitative assessment technique of those.
123I-IMP brain perfusion SPECT
123I-labeled N-isopropyl-p-iodoamphetamine (123I-IMP) brain perfusion SPECT studies were performed using a dual-detector, variable angle gamma camera with a 16-slice computed tomography scanner (Symbia T16; Siemens Healthcare, Erlangen, Germany) equipped with a low-medium energy general purpose collimator. Projection data were acquired for approximately 20 min after the intravenous injection of 123I-IMP (167 MBq in 1.5 ml). The image acquisition time (continuous mode, 3.0 min/rotation×8 rotations, 128×128 matrix) was 24 min. The energy peak was set at 159 keV with a 20% energy window. Transaxial images were reconstructed with filtered back projections using a Butterworth filter. The Butterworth filter (cutoff frequency: 0.35 cycles/cm, order: 8) was used as a post-processing filter for SPECT image reconstruction. The reconstructed slice thickness was 3.3 mm. Attenuation correction was achieved using Chang’s method, and no correction for scatter was performed. The reconstructed 123I-IMP SPECT images were normalized to the mean global activity with Neurostat (3D-SSP for three-dimensional stereotactic surface projections) using an image analysis software (iSSP version 3.5, Tokyo, Japan) [17, 18]. Further analysis was performed with stereotactic extraction estimation (SEE) software [19]. The SEE method uses a classification by Talairach Daemon Levels 1, 2, 3, and 5 [20].
In this study, we used a level-2 lobe-level classification as determined by the SEE method, and calculated a severity index (SI; the average Z-scores in each segment) and extent ratio (ER; the percentage of the coordinates within a segment that had Z-scores ≥2) for the frontal, parietal, temporal, and occipital lobes in each hemisphere.
Statistical analysis
The correlation between the number of CMBs and the CBF measures (SI and ER) was obtained using the SEE method and analyzed using Spearman rank correlation coefficients due to the non-normal distribution of the numbers of CMBs. First, the correlation between all 272 lobes (34 patients×2 hemispheres×4 lobes) was analyzed. Then, the correlation within each lobe was separately analyzed, since the distribution of CMBs differed among the cerebral lobes [21, 22]. Next, a partial correlation measures the relationship between the two variables while controlling the effect of other variables was performed. In this analysis, specific effects on the CBF of the number of CMBs were tested by using partial Spearman rank correlation coefficients, in which possible effects of cSS, lacunars, periventricular WMH, and subcortical WMH were separately determined. Statistical analyses were performed with SPSS software (Version. 22.0, IBM Japan, Tokyo, Japan). Results showing p < 0.05 were considered to be statistically significant.
RESULTS
In the 34 participants with multiple CMBs, the average number of CMBs was 65.1 (median: 29.5; range 10– 400). In 17 of 34 participants, microbleeds were located only in the cerebral lobes, and in other cases, many microbleeds were unevenly located in lobar and nonlobar regions. The number of CMBs was highest in the occipital lobe, followed by the temporal, frontal, and parietal lobes, respectively (Table 2). A Kruskal– Wallis analysis revealed significant differences in the number of CMBs among the four lobes (p = 0.011).
MRI characteristics in each lobe
Values are n and the mean±standard deviation. CMBs, cerebral microbleeds; WMH, white matter hyperintensity; cSS, cortical superficial siderosis.
The lobar SI was highest in the temporal lobe, followed by the parietal, frontal, and occipital lobes. The second parameter, ER, also followed the same pattern (Table 3). This result suggests that the intensity and extent of CBF was most significantly decreased in the temporal lobes and was relatively preserved in the occipital lobes. One-way ANOVA revealed that both SI and ER differed significantly across lobes (both p < 0.001). The post hoc analysis indicated that SI and ER were significantly lower in the occipital lobe than in the other lobes (versus frontal lobe: p < 0.05, p < 0.001, respectively; versus temporal lobe: p < 0.001, p < 0.001; versus parietal lobe: p < 0.001, p < 0.001). The SI was significantly lower in the frontal lobe than in the temporal lobe (p < 0.001) and in the parietal lobe (p < 0.05). The ER was significantly higher in the temporal lobe than in any other lobe (p < 0.001 in each lobe).
Mean severity index and extent ratio in each lobe
*Effects of cortical superficial siderosis, lacunes and the degree of white matter hyperintensities being demonstrated separately. CMBs, cerebral microbleeds; SI, severity index; ER, extent ratio; r s , Spearman’s correlation coefficient.
Weak correlations between the number of CMBs and the SI (Spearman’s r = 0.146; p = 0.05); and the number of CMBs and the ER (Spearman’s r = 0.130; p = 0.05) were observed among all 272 lobes. However, in a further test within each lobe, we observed significant correlations between the number of CMBs and the SI in the occipital and temporal lobes, but not in the frontal and parietal lobes (Table 3). The correlation coefficient was highest in the occipital lobe, followed by the temporal lobe. The ER showed significant correlation with the number of CMBs in the occipital and temporal lobes. All the results were unchanged in partial correlational analysis expect the ER for all lobes became marginal (Table 3). Figure 2 shows a scatterplot demonstrating the association between the number of CMBs and the SI in the occipital lobe.
DISCUSSION

Scatterplot demonstrating the association between CMB count and CBF severity index in the occipital lobes. Each dot represents one patient. The number of microbleeds was significantly correlated with the severity of CBF decrease in the occipital lobe (Spearman’s r = 0.531, p < 0.001). CMB, cerebral microbleed.
A major finding of the current study was that the number of CMBs was negatively correlated with the presence of CBF. It should be noted that the relationship between CMBs and CBF differed between the cerebral lobes. We found significant correlations between the number of CMBs and both the intensity and the extent of CBF decrease in the occipital and temporal lobes, with the highest correlation coefficient being determined for the occipital lobe. Conversely, no correlation between these parameters was found in the frontal and parietal lobes. This difference might be explained by the different distribution of the underlying CAA pathology and AD-related histopathology, such as neurofibrillary tangles, among the cerebral lobes. CAA is associated with vasculopathies, including obstructive intimal changes, hyaline degeneration, microaneurysm-associated dilatation, and fibrinoid necrosis [23]. It has been reported that cerebral microinfarcts are a common finding in patients with CAA, and there is a strong association between cerebral microinfarcts at autopsy and microbleeds on MRI [24]. The CAA distribution has been reported to differ across cerebral lobes and is more likely to occur in the occipital and temporal lobes, corresponding to the present finding that the number of microbleeds was largest in the occipital lobe, followed by the temporal lobe. Thus, hypoperfusion derived from CAA is thought to be most pronounced in the occipital lobes and least severe in the parietal lobes. In apparent conflict with these data, many neuroimaging studies have reported that patients with AD show temporoparietal hypoperfusion from the early stages of the disease [25, 26], while CBF in the occipital lobe remains unaffected [27]. The temporoparietal areas showing hypoperfusion correspond to areas of significant histopathological burden in autopsy-confirmed AD [28]. Considering the possibility that our participants could have had both AD and CAA pathology, CMBs might be strongly correlated to decreased CBF in the occipital lobes where the CAA pathology is predominant. On the other hand, CMBs are thought to contribute little toward CBF decreases in the parietal lobe where AD pathology is predominant. In line with this, we found a weak correlation between the number of CMBs and the severity of CBF decrease in the temporal lobe, where AD and CAA pathologies are thought to coexist.
In AD, it has been reported that many CAA-related microbleeds are located in the cerebral lobes, few are located in the cerebellum, while very few are located in the basal ganglia and brain stem [29]. In addition, microbleeds have been reported to occur in local regions of concentrated amyloid deposits, particularly in the occipital and temporal lobes [30]. In almost half of the subjects in the current study, microbleeds were located only in the cerebral lobes, while in the other half they were located in both cerebral lobes as well as deep locations. The number of CMBs was largest in the occipital lobe, followed by the temporal lobe, frontal lobe, and parietal lobe. The distribution of CMBs observed here was in line with previous studies which reported presence of CMBs in posterior brain regions, particularly the occipital and temporal lobes in AD [21, 22] and followed the same pattern as that of CAA-related microbleeds. Considering that all 34 participants met the criteria for probable CAA based on the Boston diagnostic criteria for cerebral amyloid angiopathy [23], the CMBs observed in our study appeared to be strongly associated with the underlying CAA pathology.
The effect of CMBs on cognitive functions in AD is currently controversial. A small number of studies have found a positive relationship between the presence of CMBs and cognitive decline in patients with AD [8], while others have found no such causal relationship [7]. Although we did not directly examine the relationship between CMBs and cognitive dysfunction, we demonstrated the possible effects of multiple CMBs on CBF. Bordeleau et al. reported that severe chronic cerebral hypoperfusion induces microglial dysfunction leading to memory loss in an AD mouse model [31]. Similarly, Wang et al. suggested that chronic cerebral hypoperfusion can induce long-term increases in the number of silent synapses and long-lasting cognitive decline in rats [32]. Therefore, AD patients with multiple CMBs would be expected to develop some cognitive deterioration associated with chronic cerebral hypoperfusion. As indicated by the present study, the impact of CMBs on CBF differed between the lobes. In the frontotemporal association cortices, CMBs had a considerable effect on CBF, with almost no apparent effect in the parietal lobe. These findings suggest that neuropsychological tests specific to frontotemporal lobe functions might be able to detect the effects of CMBs on cognitive function. Indeed, Goos et al. showed that AD patients with multiple microbleeds performed worse on object naming (temporal function) and category fluency (frontal function) tasks compared with AD patients without microbleeds [8].
A previous study investigated the relationship between CMBs and CBF in patients with AD [33]. Unlike our study, Doi et al. reported that CMBs located in the occipital lobe and our lobe were associated with decreased CBF. The discrepancy between their findings and the current results is likely to be due to differences in methodological approaches. Furthermore, Doi et al. compared the frequency of CMBs accompanied by decreased CBF in the frontal, temporal, parietal, and occipital lobes and found that the frequency of CMBs associated with regional CBF decreases was significantly higher in the parietal and occipital lobes than in the frontal lobe. However, their method was unable to eliminate the influence of AD pathology on CBF, which is predominantly distributed in the temporoparietal lobes. Accordingly, their findings, indicating a relationship between CMBs and parietal blood flow decrease, should be interpreted with caution.
Several methodological issues limit the interpretation of the current results. First, the pathology underlying CMBs was not confirmed. However, Schrag et al. examined MRIs and postmortem brains of patients with AD, reporting that hypointense foci on SWIs indicated a variety of CAA-related pathologies [34]. Second, the diagnosis relied solely on a clinical basis without histopathologic confirmation. Thus, despite the exclusion of the patients with any evidence suggestive of vascular dementia, patients with vascular dementia were likely to be included in the present study. Third, the influence of conditions related to other small vessel diseases, such as WMH or lacunars might have affected the results needs to be considered. However, these MRI changes, frequently accompanied with AD, are unlikely to have significant impact on the present results because the correlation coefficients were unchanged after possible effects of other SVD were selectively checked. Fourth, our analysis only included AD patients with at least eight CMBs to emphasize the effects of CMBs on CBF. As a result, 360 patients who had fewer than eight CMBs were excluded from the analysis. Further analysis is needed to determine whether the positive correlation between the number of CMBs and CBF decrease is also applicable to AD patients with fewer than eight CMBs.
Footnotes
ACKNOWLEDGMENTS
The authors gratefully acknowledge the assistance of the Department of Radiology and the Department of Neuropsychiatry, Kumamoto University Hospital.
This work was supported by the Japan Society for the Promotion Science KAKENHI (grant number JP26461750, to M.I).