
Abstract
Background:
The role of cerebral microbleeds (CMBs) in cognitive impairment remains controversial.
Objective:
To investigate the possible links between the presence, progression, number, and location of CMBs and cognition.
Methods:
We assessed 792 subjects from the Alzheimer’s Disease Neuroimaging Initiative who underwent both brain 3 Tesla MRI scans and cognitive testing. The association between CMBs and cognitive change was explored using linear mixed-effects models (LME).
Results:
Presence and number of CMBs were associated with memory (β= –0.03, p = 0.015; β= –0.01, p = 0.003), executive function (β= –0.04, p = 0.010; β= –0.01, p = 0.014), and global cognitive function (β= –0.06, p = 0.025; β= –0.03, p < 0.001). Progression of CMBs showed significant negative associations with executive function (β= –0.05, p = 0.025) and global cognitive function (β= –0.12, p = 0.015). The relations with cognitive performance (memory, executive function and global cognitive function) were mainly driven by lobar CMBs (β= –0.03, p = 0.041; β= –0.04, p = 0.010; β= –0.07, p = 0.029, respectively), especially those located in temporal lobe (β= –0.08, p = 0.027; β= –0.13, p = 0.001; β= –0.26, p < 0.001, respectively). Furthermore, white matter hyperintensities may mediate the association between CMBs and cognition.
Conclusion:
The presence, progression, number, and location of CMBs, especially those located in temporal lobe, are associated with cognitive decline. These findings suggest CMBs play a role in cognitive impairment.
INTRODUCTION
Cerebral microbleeds (CMBs) are 2–10 mm small, homogeneous, round foci of low signal intensity on gradient-echo T2* sequences [1]. CMBs are now accepted as a manifestation of cerebral small vessel disease (SVD) which is a suggested cause of cognitive impairment and dementia [2–4]. The pathogenesis of CMBs commonly involves vessel wall damage due to hypertensive vasculopathy (deep regions) and cerebral amyloid angiopathy (CAA) (lobar regions) [5, 6]. As such, it has been suggested that CMBs may provide an intriguing link between cerebrovascular pathology and neurodegenerative pathology in cognitive dysfunction and dementia [6].
The effects of CMBs on cognitive function have been evaluated in previous studies. However, there are inconsistent results regarding the cognitive consequences of CMBs [7–13]. Many studies found an association between the presence of CMBs and worse cognitive performance, among which some found the strongest association for deep CMBs [7, 12], whereas others showed cognition was most strongly associated with lobar CMBs [9–11], and still others reported no region-specific associations [13]. What’s more, some studies only reported associations between CMBs and global cognition, while others also showed associations with specific cognitive domains [12, 14]. In addition, few studies have evaluated the effects of CMBs progression on cognitive function.
Therefore, in the present study, we sought to elaborate the possible links between the presence, progression, number, and location of CMBs and cognitive function, as evaluated by an extensive neuropsychological battery.
METHODS
Alzheimer’s disease neuroimaging initiative study
Data used for this study was obtained from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (http://adni.loni.usc.edu). The ADNI was launched in 2003 as a public-private partnership with the primary objective of testing whether serial MRI, PET, other biological markers, as well as clinical and neuropsychological assessments can be combined to measure the progression of cognitive impairment (MCI) and early Alzheimer’s disease (AD). Further information can be found at http://www.adni-info.org/ and in previous reports [15–18].
Standard protocol approvals, registrations, and patient consent
As stated in the ADNI procedures manual, ADNI centers obtain local Institutional Review Board protocol approval, and patient consents are obtained at the participants’ initial screening visit.
Participants
Subjects of this study were participants enrolled in ADNI-grand opportunity (ADNI-GO) and ADNI-2 from June 2010 until December 2018. The T2* GRE sequence for the identification of CMBs was added to ADNI MRI protocol in the ADNI-GO study and continued into ADNI-2 with longitudinal studies in the existing ADNI cohort and in the new participants of the ADNI-GO and ADNI-2 studies [16]. All subjects included in the study were aged 55–90 years and had underwent 3T MRI. Participants exhibiting definite CMBs at baseline confirmed by strict neuroimage protocol, which will be elaborated thoroughly in the following context, were classified as CMBs cases. Participants without definite or possible CMBs at baseline and follow-up were classified as non-CMBs controls. Participants without baseline or follow-up data of cognitive measures (memory, executive function, or global cognitive function) were excluded. We also excluded three patients with baseline CMBs counts >3 SD.
Finally, a total of 792 subjects (231 subjects with CMBs presence and 561 subjects with CMBs absence) were included in this study.
Brain MRI and rating of CMBs
The 3 Tesla MRI protocol included T2* GRE and T1-weighted three-dimensional MPRAGE sequences, which has been described previously (http://adni.loni.usc.edu/methods/documents/mri-protocols/). CMBs were defined as homogenous hypointense lesions up to 10 mm in diameter in the gray or white matter on T2* GRE images. All available T2* GRE scans of a subject were used for the rating of individual CMBs. The number and locations of CMBs were identified by trained image analysts and further confirmed by two radiologists experienced in reading the T2* GRE images (KK and CRJ). A summary list of image finding, lesion location, and basic clinical information was reported. Three values (possible, definite, rescinded) were used to describe the status of the finding. In this study, we included individuals with definite CMBs at baseline as cases and those without definite or possible CMBs at baseline and follow-up as controls.
According to whether there was an increase in the CMBs count during the follow-up period compared with baseline, we classified the case group into CMBs progression group and non-progression group. Also, subjects of the cases group were categorized by location as 1) lobar CMBs group, if they involved frontal, parietal, temporal, and occipital regions; 2) deep CMBs group, if they involved the basal ganglia, thalami, brainstem, or cerebellum; and 3) mixed CMBs group, if they involved both deep and lobar regions.
Assessment of cognitive function
ADNI created composite memory and executive function scores derived from tests used in its neuropsychological battery. The ADNI memory composite score (ADNI-Mem) was developed from the Rey Auditory Verbal Learning Test (2 versions), Alzheimer’s Disease Assessment Schedule Cognition (ADAS-Cog, 3 versions), Mini-Mental State Examination (MMSE), and Logical Memory data [19]. The executive function score (ADNI-EF) derives from Wechsler Adult Intelligence Scale-Revised Digit Symbol Substitution, Digit Span Backwards, Trails A and B, Category Fluency, and Clock Drawing [20]. The global cognitive performance was assessed using the MMSE, the most widely used measure for clinical trials, which evaluated various domains of cognitive function. Before regression analysis, all the raw test scores were transformed into standardized z scores. In our study, we included follow-up data for up to 8 years (mean, 4 years) and the specific details about the numbers of subjects at each visit of cognitive measures were shown in Supplementary Table 1.
Statistical analysis
Subgroup difference in baseline characteristics was evaluated by χ2 test for categorical variables and t-test or one-way ANOVA for continuous variables. All continuous variables were expressed as mean±standard deviation (SD) and categorical variables were expressed as the number of patients with a percentage. The associations of the presence, progression, number, and location of CMBs with cognitive performance were investigated using the linear mixed-effects (LME) models adjusted for age, gender, education level, APOE ɛ4 status, and baseline diagnosis. To evaluate the relation between CMBs location and cognitive decline, subjects were divided into four groups (no CMBs, strictly lobar, deep, and mixed). Next, we categorized the lobar CMBs into strictly frontal, temporal, parietal, and occipital groups to further explore the association between the specific locations of lobar CMBs and cognitive function, using non-CMBs group as reference. Furthermore, since white matter hyperintensities (WMH) were previously associated with cognitive decline [21], causal-steps approach and Sobel test were performed to test whether WMH mediate the association between the CMBs and cognition. Lastly, participants were divided into four subgroups according to amyloid-β42 (Aβ42) and phosphorylated tau (P-tau): Aβ–Ptau–, Aβ–Ptau+, Aβ+Ptau–, and Aβ+Ptau+. We conducted subgroup analyses to explore the association between CMBs and cognition.
All statistical tests were performed with the R version 3.4.2 and SPSS software version 20 (SPSS, Chicago, IL). A probability value of p≤0.05 was considered statistically significant.
RESULTS
Baseline characteristics of participants
A total of 792 participants (53.8% men, 72.7±7.1 years) were included in the study. Table 1 showed the baseline characteristics of study subjects according to the presence and progression of CMBs. In brief, there were 231 subjects (63.6% men, 74.4±6.7 years) with CMBs and 561 subjects (49.7% men, 71.8±7.1 years) without CMBs. Compared to participants without CMBs, those with CMBs were older and more likely to be male, to be APOE ɛ4 allele carriers, to have higher WMH volumes, and worse cognitive performance. Among subjects with CMBs, 76 (65.8% men, 76.4±6.1 years) showed increased CMBs counts, while 155 (62.6% men, 73.4±6.8 years) showed no progression of CMBs. Age, WMH volume, and cognition performance showed significant differences between progression group and non-progression group.
Baseline characteristics of study subjects according to the presence and progression of CMBs
CMBs, cerebral microbleeds; NC, normal cognition; MCI, mild cognitive impairment; AD, Alzheimer’s disease; WMH, white matter hyperintensities; ADNI-Mem, The ADNI memory composite score; ADNI-EF, The ADNI executive function score; MMSE, Mini-Mental State Examination. at-test or χ2-test.
Subject characteristics according to the location categories of CMBs were presented in Table 2. Of the 231 subjects with CMBs, 168 (72.7%) had strictly lobar CMBs, 27 (11.7%) had strictly deep CMBs, and 36 (15.6%) had mixed CMBs. Those with mixed CMBs had a higher average CMBs count.
Baseline characteristics of study subjects according to the location categories of CMBs
CMBs, cerebral microbleeds; NC, normal cognition; MCI, mild cognitive impairment; AD, Alzheimer’s disease; WMH, white matter hyperintensities; ADNI-Mem, The ADNI memory composite score; ADNI-EF, The ADNI executive function score; MMSE, Mini-Mental State Examination. aone-way ANOVA or χ2-test.
Association of the presence and progression of CMBs with cognitive decline over a period of 8 years
In an LME model adjusted for age, gender, education, APOE ɛ4 status, and baseline diagnosis, the presence of CMBs predicted decline in memory, executive function, and global cognitive function over time (β= –0.03, p = 0.015; β= –0.04, p = 0.010; and β= –0.06, p = 0.025, respectively). Compared to CMBs without progression, the progression of CMBs was significantly negatively associated with executive function (β= –0.05, p = 0.025) and global cognitive function (β= –0.12, p = 0.015), but not with memory decline (β= –0.03, p = 0.216) (Table 3).
Association of the presence and progression of CMBs with 8-year cognitive change
CMBs, cerebral microbleeds; The linear mixed-effects model was adjusted for age, gender, educational level, APOE ɛ4 carriership, and baseline diagnosis.
Association of the number and location of CMBs at baseline with cognitive decline over a period of 8 years
Table 4 and Fig. 1A–C demonstrated that higher CMBs counts at baseline were significantly associated with an increased rate of decline in both cognitive domains (memory, β= –0.01, p = 0.003; executive function, β= –0.01, p = 0.014) as well as global cognitive function (β= –0.03, p < 0.001).
Association of the number and location of CMBs with 8-year cognitive change
CMBs, cerebral microbleeds; The linear mixed-effects model was adjusted for age, gender, educational level, APOE ɛ4 carriership, and baseline diagnosis.
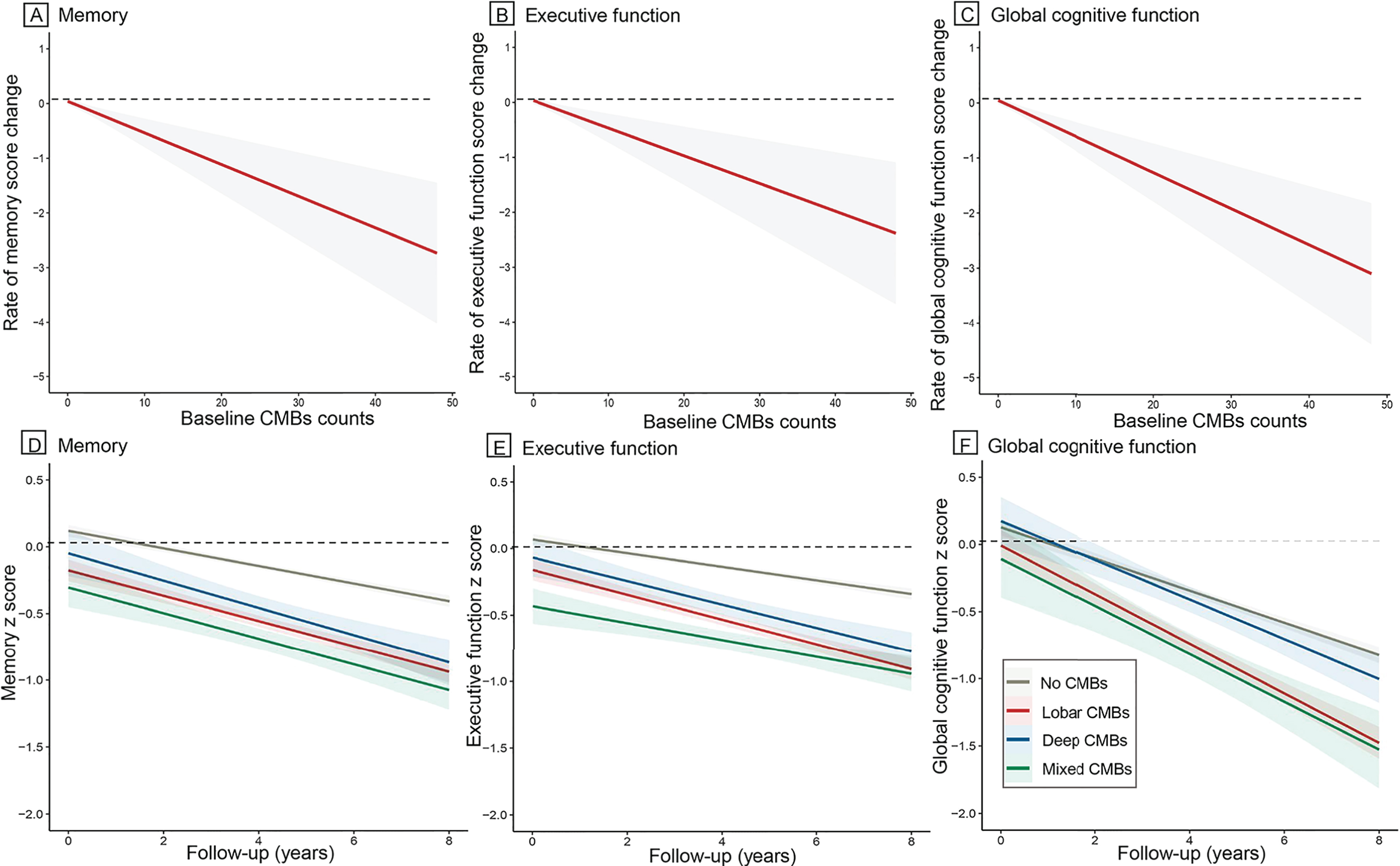
Association of the number and location of CMBs with cognitive decline over a period of 8 years. Higher CMBs counts at baseline were significantly associated with an increased rate of decline in memory (A), executive function (B), and global cognitive function (C). Presence of strictly lobar CMBs predicted a significant decline in memory (D), executive function (E), and global cognitive function (F), with non-CMBs group as reference. Data were from linear mixed-effects models adjusted for age, gender, education, APOE ɛ4 status, and baseline diagnosis.
In the fully adjusted models, presence of strictly lobar CMBs predicted a steeper decline in global cognitive function (β= –0.06, p = 0.029) and specifically in memory and executive function (β= –0.03, p = 0.041 and β= –0.04, p = 0.010, respectively). Presence of strictly deep and mixed CMBs was not associated with cognitive decline (Fig. 1D–F; Table 4). Afterwards, lobar CMBs were categorized into groups of strictly frontal, temporal, parietal, and occipital CMBs to further explore the association between the specific location of lobar CMBs and cognitive function. Table 5 revealed that strictly temporal CMBs had the strongest association with decline in both cognitive domains (memory, β= –0.08, p = 0.027; executive function, β= –0.13, p = 0.001) and global cognitive function (β= –0.26, p < 0.001) decline over time, independent of covariates. Strictly frontal, parietal, and occipital CMBs were not significant predictors of longitudinal decline in cognitive function.
Association of CMBs location of lobar region with 8-year cognitive change
CMBs, cerebral microbleeds; The linear mixed-effects model was adjusted for age, gender, educational level, APOE ɛ4 carriership, and baseline diagnosis.
Mediation analyses
Rates of cognition change were estimated using longitudinal linear mixed-effects models controlling for age, gender, education, APOE ɛ4 status, baseline diagnosis, with the subject-specific annual change in cognition score as response variable. We demonstrated that CMBs were significantly associated with WMH (β= 0.26, p = 0.01), that WMH was significantly associated with rates of cognition change (β= –0.01, p < 0.001 for memory and executive function, β= –0.02, p < 0.001 for global cognitive function), and that the CMBs were significantly associated with rates of cognition change (β= –0.02, p≤0.05 for memory and executive function, β= –0.04, p≤0.05 for global cognitive function). Moreover, when controlling for WMH the associations between CMBs and rates of cognition decline were no longer significant (p > 0.05 for all). As such all conditions for complete mediation were met. For memory, executive function and global cognitive function, the Sobel test for mediation estimated that the percentages of total effect mediated by WMH were 38.4% (z = –3.79; p < 0.001), 26.8% (z = –3.31; p < 0.001), and 30.0% (z = –2.93; p = 0.003), respectively (Supplementary Figure 1).
Subgroup analyses according to Aβ42 and P-tau status
We found a significant association between CMBs and memory only in Aβ–Ptau–subgroup (β= –0.04, p = 0.014). However, no significant associations between CMBs and cognition decline in Aβ–Ptau+, Aβ+Ptau–, and Aβ+Ptau+groups (Supplementary Table 2).
DISCUSSION
In the present study, we found that the presence, progression, and higher number of CMBs were related to cognitive deterioration independent of age, gender, education, APOE ɛ4 status, and baseline diagnosis. The relations with cognitive performance were mainly driven by strictly lobar CMBs, especially those located in the temporal lobe.
The underlying mechanisms of the pathological association between CMBs and cognitive function are unknown. SVD has been associated with an increased risk of cognitive impairment or even dementia [2, 3]. As a manifestation of SVD, CMBs may cause focal damage and disrupt connections of functionally important cortical and subcortical tracts, leading to leading to damage of neural networks and interference with cognition [22, 23]. On the other hand, CMBs may represent a proxy measure of more generalized cerebral vascular pathology [7, 24]. In this scenario, a higher load of CMBs may thus indicate more extensive and severe subclinical microvascular damage, and their presence may influence cognition indirectly [24]. We found the progression of CMBs, which was defined as increased CMBs count during the follow-up period, predicted decline in executive function and global cognitive function. We also found a higher number of CMBs was associated with a decrease in cognition for 1 count increment, which as consistent with prior studies [12, 14].
We found that the associations with cognitive decline differed according to the location of CMBs and thus possibly differed with underlying vasculopathy. Depending on location, CMBs are commonly related to two different SVD pathologies: hypertensive vasculopathy (deep regions) and CAA (lobar regions) [5, 6]. Some studies reported that deep CMBs were associated with cognitive impairment [7, 8], whereas others including ours showed an association of lobar CMBs with cognitive decline [9, 25]. We further found that the relation between lobar CMBs and poor cognitive performance was mainly driven by CMBs located in the temporal lobe. A cross-sectional study showed that frontal and temporal CMBs correlated with cognitive performance in non-demented elderly patients, independent of other coexisting SVD-related lesions [26]. We also observed a negative association between frontal CMBs and executive function change. However, the association did not reach statistical significance (β= –0.05, p = 0.052). A recent report on the distribution of lobar CMBs, which took lobar volumes and clustering effects into account, found that lobar CMBs were significantly more often located in the temporal lobe [9]. This suggests that the relation observed between temporal CMBs and worse cognitive performance might, at least in part, be explained by the higher number of CMBs in this region compared with other regions if one would take the volume of the temporal lobe into account. The temporal lobe is known to be more affected by cerebral amyloid angiopathy [26]. Therefore, our findings are suggestive of a role for cerebral amyloid angiopathy in the pathogenesis of CMB-related cognitive impairment. Previous studies [11, 27] showed impaired speed was associated with a high load of lobar CMBs, suggesting that the vascular damage and ischemia caused by (or predisposing to) CAA [28, 29] can reflect overall vascular damage.
In addition, we found the presence of mediation effect of WMH for the relationship between the CMBs and cognition, but the specific mechanism was not yet clear. Previous evidence suggested that CMBs virtually always coexisted with other SVDs (lacunes and WMH) [22, 26], indicating that these lesions had a shared effect on cognition. Pathological studies showed that WMH was usually considered to represent ischemic-associated demyelination and axonal degeneration [30]. A reasonable hypothesis would be CMBs, as a proxy measure of cerebral vascular pathology, may indicate more extensive and severe subclinical microvascular damage and influence cognition indirectly.
Our study has several limitations. First, the ADNI cohort mainly enrolled Caucasians, who were more highly educated, and had fewer comorbidities than a community population at this age. Second, although we have adjusted for as many potential confounders as possible based on available data, residual confounding factors may still exist. Third, the cohort excluded people with severer comorbid vascular pathologies, which may moderate the associations we found [31]. Therefore, although we did not find a significant effect of deep or mixed CMBs on cognition, a significant association may be found in people with severer vascular diseases. Fourth, the sample sizes of temporal, parietal, and occipital groups were relatively small. This may lead to lower statistical power, reducing the chance of detecting a true effect of CMBs on cognition. Therefore, although we did not find a significant effect of parietal or occipital CMBs on cognition, we recommend appropriate caution should be taken when interpreting the results and further validation in further study with a larger sample size is required.
In summary, the presence, progression, number, and location of CMBs, especially those located in the temporal lobe, are associated with cognitive decline. These findings suggest that CMBs are important indicators of the microvascular contribution to cognitive impairment and highlight the role of CAA in cognitive deterioration.
Footnotes
ACKNOWLEDGMENTS
This study was supported by grants from the National Natural Science Foundation of China (81771148, 91849126), Shanghai Municipal Science and Technology Major Project (No.2018SHZDZX03) and the State Key Laboratory of Neurobiology and Frontiers Center for Brain Science of Ministry of Education, Fudan University. Data collection and sharing for this project was funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; PiramalImaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California.