
Abstract
Background:
It is unclear if latent cognitive profiles can distinguish between dementia with subcortical vascular lesions and Alzheimer’s disease (AD) at the incipient stage, and if they differ in performance from the Petersen subtypes.
Objective:
To identify latent cognitive profiles in a naturalistic population of patients from a memory clinic sample, and investigate the derived classes not only in terms of conversion to AD, but also in terms of conversion to dementia with subcortical vascular lesions. Another objective was to compare the derived classes to the Petersen subtypes.
Methods:
We performed a latent profile analysis (LPA) on standardized neuropsychological test scores from 476 memory clinic patients (age 64±8) without dementia, and analyzed progression to dementia after 2 years.
Results:
The LPA resulted in two classes with impaired cognition (Amnestic and Slow/Dysexecutive) and two classes with normal cognition (Normal-Low and Normal-High cognition). Belonging to the Amnestic class predicted progression to all-cause dementia and to AD; belonging to the Slow/Dysexecutive class predicted progression to all-cause dementia, AD, and dementia with subcortical vascular lesions. Of the Petersen MCI subtypes, only amnestic multi-domain MCI predicted progression to all-cause dementia, AD, and dementia with subcortical vascular lesions.
Conclusion:
Latent cognitive profiles separated between AD and dementia with subcortical vascular lesions, while the Petersen subtypes did not. However, similar to the Petersen subtypes, LPA classes work better for ruling out progression to dementia than for case finding.
Keywords
INTRODUCTION
Mild cognitive impairment (MCI) is a syndrome characterized by a decline in cognitive function greater than what is considered normal, yet different from mild dementia as activities of daily life are intact or only minimally disturbed. MCI as a single entity construct has a high sensitivity, but a low specificity, in predicting conversion to dementia [1, 2]. In 2004, Petersen introduced a two-dimensional method for classifying MCI into subtypes [3]: MCI with or without memory impairment as one dimension, and with or without impairment in more than one cognitive domain as another dimension. The Petersen subtypes were suggested to represent the incipient stages of different etiologies of dementia [3, 4]. The heterogeneity captured by subtyping may improve the prognostic accuracy of MCI; however, amnestic multi-domain MCI may be the most common subtype in both incipient Alzheimer’s disease dementia (AD) and subcortical vascular dementia [2, 5]. It is unclear whether the Petersen subtypes actually discriminate between these dementia etiologies at the incipient stage.
Cluster analysis is an analytic approach that has been used to create homogenous groups based on cognitive data, as a data-driven rather than a theoretical alternative to the Petersen subtypes [6–10]. The individual-based latent variable mixture model latent profile analysis (LPA) is considered to have several advantages compared with cluster analysis, partly because it is considered less subjective [11]. LPA uses maximum likelihood estimation to model the classification uncertainty of the individual to a latent class [12, 13]. Further, using LPA within-person interactions between variables can be studied, which is not possible in the more traditional variable-based analytic approaches. LPA also has the ability to handle missing data, thereby allowing for inclusion of individuals with non-complete datasets into the analyses [14, 15].
Previous studies using LPA classification of memory clinic patients based on cognitive tests have typically found a group with severe impairments in memory and attention or executive function, one or more groups with dominant memory impairment, and one or a couple of groups with normal cognitive function [16–18]. Progression to dementia has been most common in the more severely impaired group, less common in the group with dominant memory impairment, and unusual in the normal groups. One study [18] also found a higher frequency of APOE ɛ4 carriers as well as of pathological levels of cerebrospinal fluid (CSF) t-tau, p-tau, and amyloid-β1–42 (Aβ1–42) in the group with more severe mixed impairments.
There are some limitations in the previous studies that have used LPA to analyze cognitive classes in memory clinic patients. Hanfelt et al. [19] reported no longitudinal outcomes and no biomarker associations, and their dataset consisted of a mixture of smaller samples recruited both at memory clinics and from the community. Köhler et al. [16] used z-scores based on scores of the patient grand mean rather than healthy controls to calculate the profiles, thus making it difficult to interpret their findings. Eppig et al. [18] described the progression to AD but not to other types of dementia. Further, they used data from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) cohort, which has episodic memory impairment as a prerequisite for inclusion. Thus, it should not be possible to find cognitive profiles with intact memory using the ADNI dataset.
We are unaware of any studies that have analyzed cognitive data using cluster or latent profile analysis with both AD and vascular dementia of the subcortical type, one of the most common causes of dementia [20, 21], as outcome. Furthermore, an issue might be that many studies have been based on the same (ADNI) dataset [6, 18]. Therefore, we used LPA in a naturalistic population of patients from a memory clinic sample, and investigated the derived classes not only in terms of conversion to AD, but also in terms of conversion to vascular dementia of the subcortical type. We also compared the progression rates in the LPA-derived classes with those in the Peterson subtypes and examined differences in CSF biomarkers and the frequency of APOE ɛ4 carriers in the LPA-derived groups.
MATERIALS AND METHODS
Participants
The data presented here were derived from the Gothenburg MCI study [22, 23], a longitudinal observational study conducted at the Sahlgrenska University Hospital, Mölndal, Sweden. We included consecutive patients seeking care between 2000 and 2014. The inclusion criteria comprised age between 40 and 79 years and self and/or informant reported cognitive decline with a duration of at least 6 months. The exclusion criteria included severe somatic or psychiatric disorder, substance abuse, or being classified as having dementia at the baseline examination (see Procedures for details).
We also included healthy controls from the Gothenburg MCI study, primarily recruited from senior citizen organizations and via information meetings. Several of them were spouses of patients. All healthy controls were thoroughly interviewed by a research nurse prior to inclusion to ensure that they were physically and mentally healthy. None of the controls had self-reported or observed signs or symptoms of cognitive impairment.
This study was approved by the local ethics committee (Diary No.: L091-99, 15 March 1999 and T479-11, 8 June 2011). Written informed consent was obtained from all participants.
Baseline demographics and 2-year follow-up
In the Gothenburg MCI study, 545 patients without dementia (58% women, age at baseline 63.7±8.3 years, education years 12.6±3.6, Mini-Mental State Examination (MMSE) 28.4±1.5) were included. Exclusions were made due to inconclusive data on years of formal education (n = 23) and no assessment by neuropsychological instruments (n = 46). Thus, the final sample consisted of the 476 remaining patients (59% women, age at baseline 63.9±8.0 years, education years 12.5±3.6, MMSE 28.4±1.5) (Table 1).
Baseline descriptive statistics; demographics, genetic markers, cerebrospinal fluid biomarkers, and neuropsychological tests
m, mean; SD, standard deviation(s); Aβ1–42, Amyloid-beta1–42; P-tau, cerebrospinal fluid phosphorylated tau protein; T-tau, total cerebrospinal fluid tau protein; MMSE, Mini-Mental State Examination; APOE ɛ4, Apolipoprotein E ɛ4 allele; s, seconds; RAVLT, Rey Auditory Verbal Learning Test; PaSMO, Parallel Serial Mental Operations; TMT, Trail making Test; COWAT, Controlled Oral Word Association Test letters F A S; VOSP, the silhouettes part of the Visual Object and Space Perception Battery. NOTE. *, significantly different from Slow/Dysexecutive; †, significantly different from Amnestic; ‡, significantly different from Normal-Low; significantly different from Normal-High. No superscript indicates that there were no significant differences. Depressive symptoms were either Geriatric Depression Scale 20 (GDS20)≥6 or Montgomery-Åsberg Depression Rating Scale (MADRS)≥10.
Ninety-three patients (60% women, age at baseline 61.8±8.2, education years 12.5±3.6, MMSE 28.3±1.6) lacked 2-year follow-up data. The remaining 383 patients (58% women, age at baseline 64.4±7.9, education years 12.5±3.6, baseline MMSE 28.5±1.4) were available for analysis of outcome after 2 years.
Procedures
Neuropsychological tests
The neuropsychological test battery was administered either by a licensed psychologist or a supervised psychologist in training. The examination was completed in two sessions of 1.5–2 h. We selected six tests with the aim to cover cognitive domains commonly tested in MCI research: delayed recall from the Rey Auditory Verbal Learning Test (RAVLT) [24] (episodic memory), letters F, A, and S from the Controlled Oral Word Association Test (COWAT) [25] (language or fluency), the Trail Making Test (TMT B) [26] (complex attention), total number of correct items backward and forward on the Digit Span test [27] (working memory), the silhouettes part of the Visual Object and Space Perception Battery (VOSP) [28] (visuospatial function), and the Parallel Serial Mental Operations Test (PaSMO) [29] (executive function). In the PaSMO test, the patient is asked to rattle off the Swedish alphabet from A to Ö, with each letter followed by its corresponding increasing number. For patients who could not finish TMT B within 180 s, 180 s was imputed in the data set (37 patients). Seven patients were unable to complete the PaSMO test; for these patients, we imputed the longest recorded time of any patient without dementia in our data set (310 s).
Z-transformation of cognitive variables
We calculated z-scores for each test, adjusted for age and education, based on our healthy control group (see Supplementary Table 1 for details). The z-scores enabled better comparisons between different test scores. For tests where a high score is worse than a low (TMT B and PaSMO), scores where inverted.
Petersen subtypes
At baseline, we categorized all patients as amnestic single-domain, amnestic multi-domain, non-amnestic single-domain, or non-amnestic multi-domain MCI. We used a z-score of -1.5 as cut-off point. Patients with missing test data on one or more tests were not categorized (Table 2).
Categorization of Petersen subtypes
RAVLT, Rey Auditory Verbal Learning Test; aMCI-sd, amnestic single-domain mild cognitive impairment; aMCI-md, amnestic multi-domain mild cognitive impairment; naMCI-sd, non-amnestic single-domain mild cognitive impairment; naMCI-md, non-amnestic multi-domain mild cognitive impairment.
Biomarker validation
All CSF samples were collected by lumbar puncture in the L3/L4 or L4/L5 interspace at the standardized time point 8.30–9.00 am. The first 12 mL of CSF was collected in a polypropylene tube and immediately transported to the local laboratory for centrifugation at 2.000×g at +4°C for 10 min. The supernatant was pipetted off, gently mixed to avoid possible gradient effects, and aliquoted in polypropylene tubes that were stored at –80°C pending biochemical analyses, without being thawed and re-frozen. CSF biomarker cut-offs from Mattsson et al. were used [30]. Positive CSF T-tau and P-tau test results were defined as values above the cutoff (≥320 ng/L for T-tau and≥52 ng/L for P-tau), and positive CSF Aβ42 as values below the cutoff (≤482 ng/L). Blood samples were drawn in the morning in the fasted state. Plasma samples for determination of ApoE concentrations were stored at –80°C pending biochemical analyses, without being thawed and re-frozen.
Diagnostic assessment of dementia
The Global Deterioration Scale (GDS) [31] was used to determine the cognitive stage of the patients. A specialist physician or a registered nurse determined the GDS stage, which was based on the MMSE [32], the Clinical Dementia Rating (CDR) [33], item 13 to 20 of the Comparative Status Analysis (STEP) [34], and the Investigation of Flexibility (I-FLEX). STEP combines neurologic and psychiatric examination methods to identify common clinical signs and symptoms of dementia, and I-FLEX is a short form of the executive interview (EXIT) [35]. Patients were staged as GDS 4 if STEP was > 1, I-FLEX was > 3, CDR sum of boxes was > 1.0, and MMSE was≤25. GDS 4 corresponds to probable mild dementia equivalent to DSM-IV dementia criteria [36]. Therefore, GDS stage 4 or higher at follow-up was considered as conversion to dementia.
Patients who had progressed to dementia at follow-up were also classified in terms of probable etiology. The clinician who determined the specific dementia diagnoses had access to magnetic resonance imaging (MRI) images but was blinded to neuropsychological test results and CSF biomarker data. AD was diagnosed according to the NINCDS-ADRDA criteria [37] and subcortical vascular dementia according to the Erkinjuntti criteria [38]. Mixed dementia (Mix) was diagnosed if patients who fulfilled the cognitive criteria for AD (i.e., predominant parietotemporal lobe symptoms) as well as the cerebrovascular imaging criteria for subcortical vascular dementia—moderate or severe cerebral white matter changes on MRI. The diagnostic procedure was based on anamnestic and clinical symptoms assessed in a clinical interview, and the level of white matter changes was determined using a modified version of the Fazekas scale [39]. The diagnostic procedures have been described in detail elsewhere [22]. In the current study, we grouped subcortical vascular dementia and Mix, i.e., dementias with subcortical vascular lesions, together as dementia with subcortical vascular lesions [40].
Statistical analysis
Mplus software (version 8.1) was used to perform the latent profile analysis based on the z-scores calculated for the six cognitive variables. Model parameters were assessed using maximum likelihood (ML) estimation. We tested solutions with 1 to 5 classes to find the number of latent classes that best fit the data. The models were compared using a bootstrapped Lo-Mendell-Rubin likelihood test (LMR) [41], iteratively adding classes. A significant LMR test (p < 0.05) indicates a better fit with data than a solution with one fewer classes. We then took the Bayesian Information Criterion (BIC) [42] and the sample-size adjusted BIC (SSA-BIC) [43] into consideration, with lower values indicating better model fit for both. Lastly, we took entropy into account, which gives an indication of the accuracy of classification of participants into their respective classes, with higher values indicating a higher accuracy [44]. Latent profile analysis was performed allowing both means and variance in the latent groups to vary.
We used the Tukey-Kramer test to compare means of multiple groups on continuous variables (age, education, MMSE, Aβ1–42, T-tau, P-tau, RAVLT delayed, PaSMO, TMT B, Digit Span, COWAT, VOSP), and the Steel-Dwass test to compare categorical variables (sex, depressive symptoms, APOE ɛ4 carriers, APOE ɛ4 homozygotes, Aβ1–42 positive, T-tau positive, P-tau positive) among multiple groups (see Table 1). To assess the ability of various cognitive classifications to predict outcomes, we used logistic regression models with dementia and specific dementia diagnoses as dependent variables, and cognitive group as the independent variable. All analyses were performed using JMP© version 13 (SAS Institute, Cary, NC, 1989-2017).
Rates of progression to all-cause dementia, AD, and dementia with subcortical vascular lesions
AD, Alzheimer’s disease dementia
RESULTS
Identifying baseline latent cognitive profiles
The fit analysis indicated that a three or four class solution fit the data best (Supplementary Table 1). The fit indices (AIC, BIC, SSA-BIC) improved (decreased) for each added class until the five class model where BIC increased, indicating that a four class model solution would be the most proper choice. The Adjusted LRT suggested improved fit, compared with k-1 class model, in the two and three class models, but not in the four and five class models, pointing to the three class model as the best model. In the two, three and four class models, no very small classes (n < 5%) appeared, whereas one class in the five class model included less than 2% (n = 8), indicating that this model was not appropriate. Weighting the statistical information together, the three or four class models appeared to be the best models. On conceptual grounds, in the four class solution all four groups appeared relevant as clinical categories and could represent distinct trajectories or etiologies. The extra class in the four class model did not overlap with the three classes in the three class model and thus represented relevant new information. Consequently, the four class model was chosen as the most appropriate model, based on statistical as well as conceptual arguments.
Between class differences at baseline
Class 1 (Slow/Dysexecutive) had very low z-scores (below –3.0) on PaSMO and TMT B, and z-scores between –1.0 and –1.5 on the other tests. Class 2 (Amnestic) had z-scores< –2.0 on RAVLT A7 (delayed word list recall), and z-scores between 0.0 and –1.5 on the other tests. Class 3 (Normal-Low) had no mean z-scores lower than –1.5, and z-scores slightly below 1.0 on PaSMO and TMT B (executive function and complex attention/processing speed). Class 4 (Normal-High) had all z-scores around or slightly above 0 (Fig. 1).

Latent Profile Analysis results; z-scores normalized for age and education. RAVLT, Rey Auditory Verbal Learning Test; PaSMO, Parallel Serial Mental Operations; TMT, Trail making Test; COWAT, Controlled Oral Word Association Test letters F-A-S; VOSP, the silhouettes part of the Visual Object and Space Perception Battery.
Demographic variables
Patients in the Slow/Dysexecutive and Amnestic classes were older than those in Normal-Low and Normal-High. Patients in the Normal-Low class had fewer years of education than those in Amnestic and Normal-High. There were no significant class differences in sex distribution. Average MMSE score in the Normal-High class was higher than that in the Slow/Dysexecutive, Amnestic, and Normal-Low classes, and higher in the Normal-Low class than in the Slow/Dysexecutive class. There were no significant differences in the occurrence of depressive symptoms between the LPA classes (Table 1).
APOE genotype and CSF biomarkers
There were more APOE ɛ4 carriers in the Amnestic class than in the Normal-Low class, and more homozygotes in the Slow/Dysexecutive class than in the Normal-Low class. CSF Aβ1–42 was lower, and CSF t-tau was higher, in the Slow/Dysexecutive and Amnestic classes than in the Normal-Low and the Normal-High classes. There were no significant differences in CSF p-tau (Table 1).
Baseline relationship between latent profiles and Petersen subtypes
At baseline, the majority of the patients in the Slow/Dysexecutive and Amnestic classes were classified as amnestic multi-domain MCI. In the Slow/Dysexecutive class, a little over a third of the patients were classified as non-amnestic multi-domain MCI. The Normal-High class mostly consisted of patients with no impairments (Fig. 2).
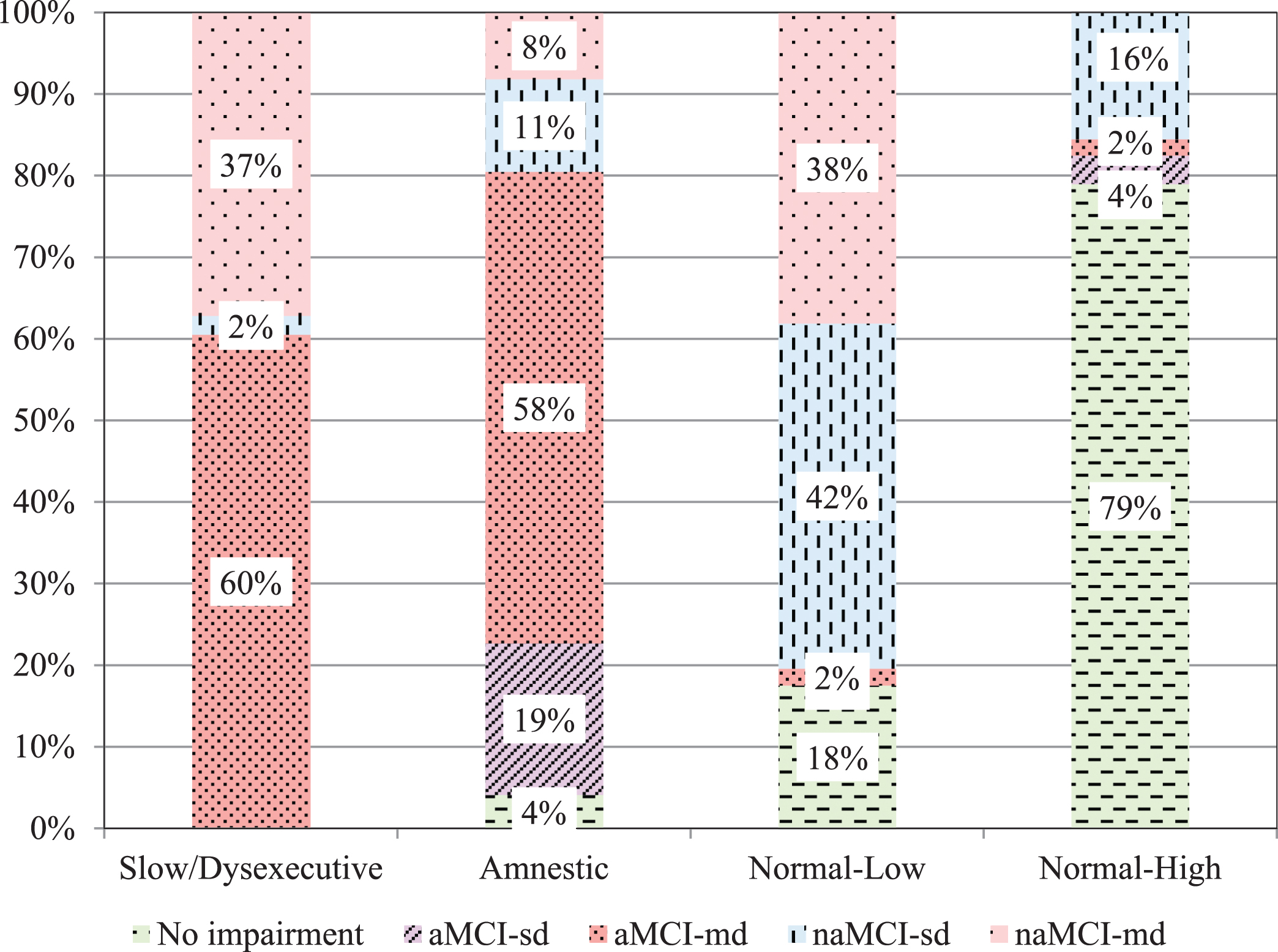
Distribution of Petersen subtypes in the LPA classes. aMCI-sd, amnestic single-domain mild cognitive impairment; aMCI-md, amnestic multi-domain mild cognitive impairment; naMCI-sd, non-amnestic single-domain mild cognitive impairment; naMCI-md, non-amnestic multi-domain mild cognitive impairment. NOTE. All group differences p < 0.05.
Progression to dementia
After 2 years, 18% of the patients had progressed to dementia. 50% of these had developed AD, 41% dementia with subcortical vascular lesions (of them 59% had mixed dementia and 41% had subcortical vascular dementia), and 9% other kinds of dementia.
The conversion rates differed between the LPA classes. Progression to all-cause dementia was most common in the Slow/Dysexecutive class, followed by the Amnestic class. Few of the patients in the two normal classes progressed to dementia. In the Slow/Dysexecutive class, dementia with subcortical vascular lesions was more common than AD, and in the Amnestic class, AD was the most common diagnosis among patients who progressed to dementia (Table 3).
Logistic regression
We used logistic regressions with all-cause dementia, AD, or dementia with subcortical vascular lesions as the dependent variable to compare the ability to predict progression to dementia in each of the LPA classes and the Petersen subtypes. In these analyses, we controlled for years of age and education. The risk of progressing to all-cause dementia was higher in the Slow/Dysexecutive class than in the Amnestic class. The risk of developing AD was the highest in the Amnestic class, and only marginally significant in the Slow/Dysexecutive class. Furthermore, the risk of developing dementia with subcortical vascular lesions was significantly increased in the Slow/Dysexecutive class but not in the Amnestic class. Of the Petersen subtypes, only amnestic multi-domain MCI had higher risk than the other patients of progressing to all-cause dementia, AD, and dementia with subcortical vascular lesions (Table 4).
Results of logistic regression
OR, odds ratio; CI, 95 % confidence interval; LR χ2, likelihood ratio chi square; AD, Alzheimer’s disease dementia; aMCI-sd, amnestic single-domain mild cognitive impairment; aMCI-md, amnestic multi-domain mild cognitive impairment; naMCI-sd, non-amnestic single-domain mild cognitive impairment; naMCI-md, non-amnestic multi-domain mild cognitive impairment. NOTE. In all models, age and education were included as covariates. For each comparison, all patients not included in the group in question were used as reference category.
Finally, we investigated whether patients progressing to AD or dementia with subcortical vascular lesions differed in terms of baseline values of the neuropsychological tests, as well as on the learning and recognition part of RAVLT, but we found no significant differences (data not shown).
DISCUSSION
In the present study, we used latent profile analysis to group memory clinic patients without dementia based on cognitive test scores, and investigated the derived classes not only in terms of conversion to AD, but also in terms of conversion to dementia with subcortical vascular lesions. We found four classes: one Slow/Dysexecutive, one with Amnestic impairments, one with Normal-Low cognitive test scores, and one with Normal-High cognitive scores. Belonging to the Slow/Dysexecutive or Amnestic classes significantly predicted all-cause dementia, with the Amnestic class as the better predictor of AD and the Slow/Dysexecutive class as the only significant predictor of dementia with subcortical vascular lesions. In comparison, when applying the Petersen subtypes, only amnestic multi-domain MCI significantly predicted dementia, AD, and dementia with subcortical vascular lesions. Thus, a different approach to categorizing memory clinic patients without dementia may result in a better separation between incipient dementia with or without subcortical vascular lesions.
As expected, the LPA-derived classes differed in terms of baseline age (the Slow/Dysexecutive and Amnestic classes were older), and education (the Normal-Low class had fewer years of education than the other classes). This was accounted for, when possible, in the statistical analyses by using age and education as covariates. Furthermore, the differences between groups were also illustrated by alterations in CSF biomarkers. The Slow/Dysexecutive and Amnestic classes had higher levels of t-tau and lower levels of Aβ1–42 than the other classes, indicating more neuronal death and more build-up of amyloid plaques among these patients. The Amnestic class had more APOE ɛ4 carriers than the Normal-Low class, and the Slow/Dysexecutive class had more homozygous carriers than the Normal-Low class, which on its own would suggest a greater risk of developing dementia.
None of the previous LPA studies [16, 18] has included dementia cases with subcortical vascular lesions. Therefore, our results regarding progression to AD versus dementia with subcortical vascular lesions provide novel information. Possibly, the lack of progression to dementia with subcortical vascular lesions in the previous studies could be due to differences in interpretations of criteria, or in views of which criteria to be applied, in a memory clinic setting. Such differences in the interpretation and implementation of dementia criteria could potentially result in that our categorizations of mixed dementia or subcortical vascular dementia might be viewed as atypical AD in other settings. We believe that dementia partially or fully caused by subcortical vascular lesions has been underreported, but this might also be a potential bias in the present study. The Gothenburg MCI study is focused on subcortical vascular dementia [22, 23], which could potentially result in a higher number of this diagnosis in our cohort.
Previous studies in similar materials [16–19] have identified varying numbers of latent profiles, ranging from 3 to 7. The groups have been largely similar to our classes, with one or two groups displaying normal cognitive test scores, one or two groups with predominantly memory impairments, resembling our Amnestic group, and one mixed group, similar to our Slow/Dysexecutive group. In our study, and the previous studies [16–18], progression to dementia was most common among patients with impairments in memory as well as complex attention or executive function, somewhat less common among patients with impairments only in memory, and uncommon among patients without cognitive impairments as compared with normative samples. None of the previous studies used criteria to identify dementia with subcortical vascular lesions, whereas our results show that different profiles may precede AD and dementia with subcortical vascular lesions. Eppig et al. [18] used data from the ADNI cohort, which has episodic memory impairment as a prerequisite for inclusion. Thus, it should not be possible to find cognitive profiles with intact memory using the ADNI dataset. Despite this, they found a rather large group of patients with normal function on a test of word list recall and recognition (n = 245, or 30% of the sample).
There were demographic differences between the studies of Eppig [18] and Köhler [16] and our study, and the selection of tests also differed. Despite these differences, the findings were of a similar type, which we interpret as a sign of stability of latent cognitive classes in memory clinic patients. However, Köhler’s data should be interpreted with some caution as their z-scores were calculated using the patient group grand mean, and the z-scores would probably have been lower if a normal sample had been used instead.
It is noteworthy that the rate of progression in our Slow/Dysexecutive class was higher than that in Eppig’s Mixed group, given the similar profiles and that Eppig’s sample was roughly 10 years older and had a higher prevalence of low CSF Aβ1–42 and high CSF p-tau. The study by Eppig et al. was based on ADNI data and had memory impairment as an inclusion criterion. This could have led to the exclusion of patients with predominantly vascular etiology as the cause of cognitive impairment, offering a possible explanation for the different results between the studies.
Amnestic multi-domain MCI constituted the majority of both the Slow/Dysexecutive and the Amnestic LPA classes. Normal-high most often corresponded to No impairment, Normal-Low most often corresponded to single-domain MCI, amnestic or non-amnestic. No previous study has compared the prevalence of LPA-derived classes to the traditional subtypes; of the Petersen subtypes, only amnestic multi-domain MCI significantly predicted dementia, AD, and dementia with subcortical vascular lesions. Thus, if the goal is to predict progression to all-cause dementia, amnestic multi-domain MCI may perform well, but to separate the risk of AD versus that of dementia with subcortical vascular lesions, a different approach might be more useful.
MCI subgroups generally have a low sensitivity and a high specificity for progression to dementia, whereas MCI as a single entity construct has a high sensitivity, but a low specificity [1, 2]. Possibly, it will be difficult to overcome this problem as a more inclusive set of criteria will result in high sensitivity and low specificity, and a more exclusive set of criteria will result in the opposite.
In Eppig’s data [18], as in ours, there were no significant differences in the ratio of APOE ɛ4 carriers, or in CSF biomarkers, between the Mixed/Slow/Dysexecutive and Amnestic groups. Even though dementia with subcortical vascular lesions was a more common outcome in the Slow/Dysexecutive class, 69% in the class had CSF Aβ1–42 levels below the cut-off, as compared with 50% in the Amnestic class, which more often progressed to AD. This finding may speak in favor of the notion that CSF Aβ1–42 has relatively low ability to discriminate between AD and dementia with subcortical vascular lesions. Alternatively, dementia with subcortical vascular lesions as conceptualized in our study could be a variant of AD.
The combined results from our study, and the studies by Köhler and Eppig [16, 18], suggest that patients with more severe impairments in speed, attention, or executive functions, combined with mild or moderate memory impairments, and patients with more severe memory impairments combined with mild or moderate impairments in other cognitive domains display the greatest risk of progressing to all-cause dementia. Currently, criteria for MCI, or its equivalent in DSM V [45] mild neurocognitive disorder, suggest no cut-off for cognitive tests but describe patients with the disorder as typically scoring 1-2 standard deviations below the mean of the general population. Based on our findings, we suggest that new criteria could be developed, allowing for varying degrees of impairment in different domains. Such criteria may better capture the cognitive deterioration that precedes dementia due to AD or subcortical vascular lesions. Based on our results, we suggest that new MCI criteria could include, for instance, a severe or mixed MCI group with speed, complex attention, or executive function scores below –2 SD, and memory, language, visuospatial scores between 0 and –1.5, and a moderate or amnestic MCI group with memory scores below –1.5 SD and other scores between 0 and –1.5 SD. All other variations would be categorized as normal cognitive function, or subjective cognitive complaints depending on the difficulties reported by the patients and informants.
A main advantage with person-centered analyses, such as LPA, is that one may examine how several input variables interact within individuals, thereby revealing potentially complex patterns of within-person interactions. In addition, we primarily chose well known tests that are used by many clinicians, which may improve the understandability of our data. Another strength of the current study is that we used a healthy group to normalize neuropsychological test variables, rather than normative data based on different samples for each test.
The present study also has limitations. As data were collected from a large umbrella study recruiting consecutive clinical patients, the statistical power of the current study was not considered in the design. If the sample had been larger, most likely CIs would have been smaller and parameter estimates more precise. In order to truly evaluate the classes we found, a grouping algorithm would have to be formulated and validated in a different dataset. Furthermore, results derived from patients seeking care at a secondary-care memory clinic may not be representative of the general population or patients seeking care in other settings, limiting the generalizability of the results. We also pooled patients with subcortical vascular dementia (n = 12) and mixed dementia (n = 17) diagnoses in order to have group sizes possible to analyze; analyzing them separately would have yielded unreliable results. Moreover, combining mixed dementia and AD would theoretically separate AD pathology from vascular pathology, but it would have resulted in a very small dementia with subcortical vascular lesions group.
Conclusion
Using latent profile analysis, and thereby within-person interactions in several cognitive domains, we identified four discrete cognitive classes, different from the Petersen subtypes. The Slow/Dysexecutive class was most likely to progress to dementia with subcortical vascular lesions, and the Amnestic class was most likely to progress to AD dementia. The majority of the patients had little or no cognitive impairments and they were unlikely to progress to dementia regardless of etiology. Of the Petersen subtypes, only the amnestic multi-domain MCI group had a significant ability to predict progression to dementia, and it predicted progression to both AD dementia and dementia with subcortical vascular lesions. In MCI caused by different dementia etiologies, different cognitive domains may be impaired to varying degrees, a phenomenon that needs more attention. Overall, cognitive profiles can be used for memory clinic patients as a first step toward identifying persons at risk for future progression to dementia. Future work is needed to refine these profiles and improve their ability to accurately discriminate between individuals with MCI who will progress to dementia versus those who do not.
Footnotes
ACKNOWLEDGMENTS
We wish to thank the late Arto Nordlund for his contributions to the Gothenburg MCI Study. We would also like to thank Marie C. Johansson, Ewa Styrud, Christina Holmberg, Eva Bringman, and Neil Gouw for important assistance and feedback.
This work was supported by grants from the Sahlgrenska University Hospital, the Swedish Research Council, Swedish Brain Power, the Swedish Dementia Foundation, the Swedish Alzheimer Foundation, Stif telsen Psykiatriska forskningsfonden, the Hjalmar Svensson Foundation, Fredrik och Ingrid Thurings stif- telse, Stiftelsen Wilhelm och Martina Lundgrens Vetenskapsfond, Insamlingsstiftelsen för neurologisk forskning och Gun och Bertil Stohnes stiftelse, Konung Gustaf V:s och Drottning Victorias Frimurarestiftelse.