
Abstract
Observational studies strongly supported the association of low levels of circulating 25-hydroxyvitamin D (25OHD) and cognitive impairment or dementia in aging populations. However, randomized controlled trials have not shown clear evidence that vitamin D supplementation could improve cognitive outcomes. In fact, some studies reported the association between vitamin D and cognitive impairment based on individuals aged 60 years and over. However, it is still unclear that whether vitamin D levels are causally associated with Alzheimer’s disease (AD) risk in individuals aged 60 years and over. Here, we performed a Mendelian randomization (MR) study to investigate the causal association between vitamin D levels and AD using a large-scale vitamin D genome-wide association study (GWAS) dataset and two large-scale AD GWAS datasets from the IGAP and UK Biobank with individuals aged 60 years and over. Our results showed that genetically increased 25OHD levels were significantly associated with reduced AD risk in individuals aged 60 years and over. Hence, our findings in combination with previous literature indicate that maintaining adequate vitamin D status in older people especially aged 60 years and over, may contribute to slow down cognitive decline and forestall AD. Long-term randomized controlled trials are required to test whether vitamin D supplementation may prevent AD in older people especially those aged 60 years and may be recommended as preventive agents.
INTRODUCTION
Alzheimer’s disease (AD) is the most common neurodegenerative disorder [1–4]. It is well known that extracellular deposition of amyloid plaques mainly consisting of amyloid-β (Aβ) peptide is one of the core pathological features of AD [1, 4–6]. Meanwhile, multiple lines of evidence indicate that oxidative stress is involved in the pathogenesis of AD [7]. Importantly, Aβ is toxic in neuronal cell cultures through a mechanism involving free radicals [7]. The clearance of Aβ could protect against apoptosis which could usually induce the oxidative stress and further cause damage in the brain of AD patients [8].
Evidence from animal models of AD shows that vitamin D could reduce oxidative stress, prevent neurons from dying, and further mediate the clearance of Aβ plaques by activating macrophages [8]. In addition, various studies using animal models of aging and AD showed that vitamin D supplementation could protect against biological processes associated with AD and enhances learning and memory performance [9]. Meanwhile, human observational or genetic studies have also investigated the role of vitamin D in AD, and strongly supported the association of low levels of circulating 25-hydroxyvitamin D (25OHD) and cognitive impairment or dementia in aging populations [8–14].
Importantly, Mendelian randomization studies have been used to determine the causal inferences and showed that genetically increased vitamin D levels could reduce the risk of AD [15–17]. However, randomized controlled trials have not shown clear evidence that vitamin D supplementation could improve cognitive outcomes [9, 18]. In fact, there is still a controversial link between vitamin D levels and cognitive performance [9]. In a recent review, Landel et al. discussed the specificity by which vitamin D could improve cognitive performance in humans [9]. Landel et al. suggested a possible age threshold [9]. In brief, some studies reported the association between vitamin D and cognitive impairment based on individuals aged 60 years and over [9].
Until now, it is still unclear that whether vitamin D levels are causally associated with AD risk in individuals aged 60 years and over. Here, we performed a Mendelian randomization (MR) study to investigate the causal association between vitamin D levels and AD using a large-scale vitamin D genome-wide association study (GWAS) dataset and two large-scale AD GWAS datasets from the International Genomics of Alzheimer’s Project (IGAP) and UK Biobank with individuals aged 60 years and over [19, 20].
MATERIALS AND METHODS
Study design
MR is based on three principal assumptions. Here, we described these three principal assumptions using the association between vitamin D levels and AD as an example. First, the instrumental variables (genetic variants) should be significantly associated with the exposure (vitamin D levels), such as the genome-wide significant level (p < 5.00E-08) [21, 22]. Second, instrumental variables should not be associated with confounders [21, 22]. Third, instrumental variables should affect the risk of the outcome (AD) only through the exposure (vitamin D levels) [21, 22]. In general, the second and third assumptions are collectively known as independence from pleiotropy [23]. Here, MR is based on the large-scale publicly available GWAS summary datasets in vitamin D and AD. All participants have given informed consent in all these corresponding original studies [19, 20].
Vitamin D genetic variants
We selected six genetic variants associated with circulating 25OHD levels achieving a genome-wide significant level (p < 5.00E-08) as the potential instrumental variables, which are around six loci including GC, NADSYN1/DHCR7, CYP2R1, CYP24A1, SEC23A, and AMDHD1 from a recent GWAS including 79,366 (all European descent) [24]. These six genetic variants are located at five different chromosomes (Table 1). Two genetic variants rs12785878 (chr11 : 71167449) and rs10741657 (chr11 : 14914878) are located the same chromosome 5. However, the distance between both variants is 56252571 bp. Hence, all these six genetic variants were independent and not in linkage disequilibrium, as described in the original study [24]. Here, we provided the summary results about the effect of each genetic variant on 25OHD levels and the standard errors in Table 1.
Characteristics of six genetic variants in vitamin D GWAS dataset
SNP, single-nucleotide polymorphism; EA, Effect Allele; NEA, Non-Effect Allele; EAF, Effect Allele Frequency; SE, standard error. Beta is the regression coefficient based on the vitamin D raising allele (effect allele).
IGAP AD GWAS dataset
The AD GWAS dataset is from the large-scale meta-analysis performed by the IGAP [20]. In stage 1, the IGAP performed a meta-analysis of 46 GWAS datasets including 21,982 cases and 41,944 cognitively normal controls of European descent from four consortia including the Alzheimer Disease Genetics Consortium (ADGC), Cohorts for Heart and Aging Research in Genomic Epidemiology Consortium (CHARGE), The European Alzheimer’s Disease Initiative (EADI), and the Genetic and Environmental Risk in AD/Defining Genetic, Polygenic and Environmental Risk for Alzheimer’s Disease Consortium (GERAD/PERADES) [20]. All patients with AD satisfied the NINCDS-ADRDA criteria or DSM-IV guidelines [20, 25]. The average age at onset for all AD cases is ≥73, and the average age at examination for 83% controls is ≥76 [20].
UK Biobank AD GWAS dataset
The UK Biobank is a large national and international health resource, which could be used to identify the causes of many complex diseases in middle aged and older individuals (http://www.ukbiobank.ac.uk) [26]. A total of 502,536 community-dwelling individuals aged between 37 and 73 years were recruited in the United Kingdom between 2006 and 2010 [26]. The proportion of women was 56% and the average age was 56 (SD 8) in both women and men [26]. Here, we selected a large GWAS of AD-by-proxy by analyzing 314,278 participants from the UK Biobank including 27,696 maternal cases and 14,338 paternal cases [19]. In this GWAS dataset, a proxy phenotype for AD case-control status was assessed via self-report [19]. Participants were asked to report “Has/did your father or mother ever suffer from Alzheimer’s disease/dementia?” Participants whose parents were aged less than 60 years, dead before reaching age 60 years, or without age information, were excluded [19].
Pleiotropy analysis
To meet MR assumptions, we performed a comprehensive pleiotropy analysis to assure that the vitamin D genetic variants affect AD risk not through biological pathways independent of vitamin D levels. For the known AD risk factors, we manually evaluated the association of vitamin D variants with the leading AD risk factors including low levels of education, midlife hearing loss, physical inactivity, high blood pressure (hypertension), type 2 diabetes, obesity, smoking, depression, and social isolation [27]. The significance threshold for the association of these six vitamin D variants with known confounders is a Bonferroni corrected significance threshold p < 0.05/6 = 0.00833. Here, we provided more detailed information about the manual pleiotropy analysis in the Supplementary Methods. For the unknown confounders, we selected two statistical methods including MR-Egger intercept test to assess the presence of potential pleiotropy [28], and Mendelian randomization pleiotropy residual sum and outlier (MR-PRESSO) test to identify the horizontal pleiotropic outliers [29]. Here, we provided more detailed information about the MR-Egger intercept test method in the Supplementary Methods. The threshold of statistical significance for evidence of pleiotropy is p < 0.05.
Mendelian randomization analysis
We first adjusted the effect alleles of six vitamin D genetic variants to be associated with increased vitamin D levels in Table 1. We then transferred and further aligned the effect alleles of these six genetic variants in diagnosed AD and self-report AD-by-proxy GWAS datasets to be consistent with the effect alleles of these six genetic variants in the vitamin D GWAS dataset. In these six vitamin D genetic variants, rs8018720 (G/C, G with the minor allele frequency (MAF) = 0.18) is an ambiguous palindromic variant (i.e., with alleles either A/T or C/G). Hence, we selected its proxy rs2144530 (C/T, C with the MAF = 0.18), which showed high linkage disequilibrium with rs8018720 (r2 = 1 and D′= 1) using the HaploReg v4.1 based on the linkage disequilibrium information in 1000 Genomes Project (CEU) [30].
Here, suppose we have successfully extracted the summary results including beta coefficients and their standard errors about the associations of each genetic variant G
j
(j = 1,…,6) with vitamin D levels (
Meanwhile, we conducted a leave-one-out permutation analysis by removing each genetic variant and recalculating the overall effect estimate, which could evaluate the influence of single genetic variant on the estimate. The odds ratio (OR) as well as 95% confidence interval (CI) of AD corresponds to about each genetically determined standard deviation (SD) (25 nmol/L) increase in natural-log transformed 25OHD levels. All analyses were conducted using the R package ‘MendelianRandomization’ [31]. The threshold of statistical significance for the potential genetic association between vitamin D levels and AD risk was p < 0.05.
Power analysis
The proportion of vitamin D variance explained by the six vitamin D genetic variants could be estimated by R2. It is estimated that these six vitamin D genetic variants could explain about 2.84% of the 25OHD variance (R2) [24]. The strength of the six vitamin D genetic variants could be evaluated using the first-stage F-statistic. F >10 could avoid bias in MR studies [32]. Here, we calculated the F-statistic and statistical power to estimate the minimum detectable magnitudes of association using the web-based tool mRnd (https://cnsgenomics.shinyapps.io/mRnd/) and a two-sided type-I error rate α = 0.05 [33].
RESULTS
AD summary statistics
Using the six vitamin D genetic variants, we extracted their corresponding AD and AD-by-proxy summary statistics in the IGAP and UK Biobank GWAS datasets, respectively, as provided in Supplementary Table 1 and Supplementary Table 2.
Pleiotropy analysis
The manual pleiotropy analysis showed that none of these six vitamin D genetic variants was significantly associated with known confounders at the Bonferroni corrected significance threshold (p < 0.05/6 = 0.00833). More detailed results are provided in Supplementary Table 3. MR-Egger intercept test showed no significant pleiotropy in the IGAP GWAS dataset (intercept = –0.001, and p = 0.927) and UK Biobank GWAS dataset (intercept = –0.012, and p = 0.086). In addition, MR-PRESSO test identified no horizontal pleiotropic outliers.
Mendelian randomization analysis
In the IGAP GWAS dataset, IVW showed that the genetically increased 25OHD levels (per 1 SD increase) were significantly associated with the reduced AD (OR = 0.62, 95% CI: 0.46–0.84, p = 0.002). Interestingly, two sensitivity analysis methods support the significant association of genetically increased 25OHD levels with the reduced AD with p < 0.05. The estimates from both sensitivity analysis methods were consistent with the IVW estimate in terms of direction and magnitude including weighted median (OR = 0.64, 95% CI: 0.46–0.89, p = 0.007) and MR-PRESSO (OR = 0.62, 95% CI: 0.51–0.75, p = 0.0047). Figure 1 shows individual genetic estimates from each of the 6 genetic variants in the IGAP GWAS dataset.
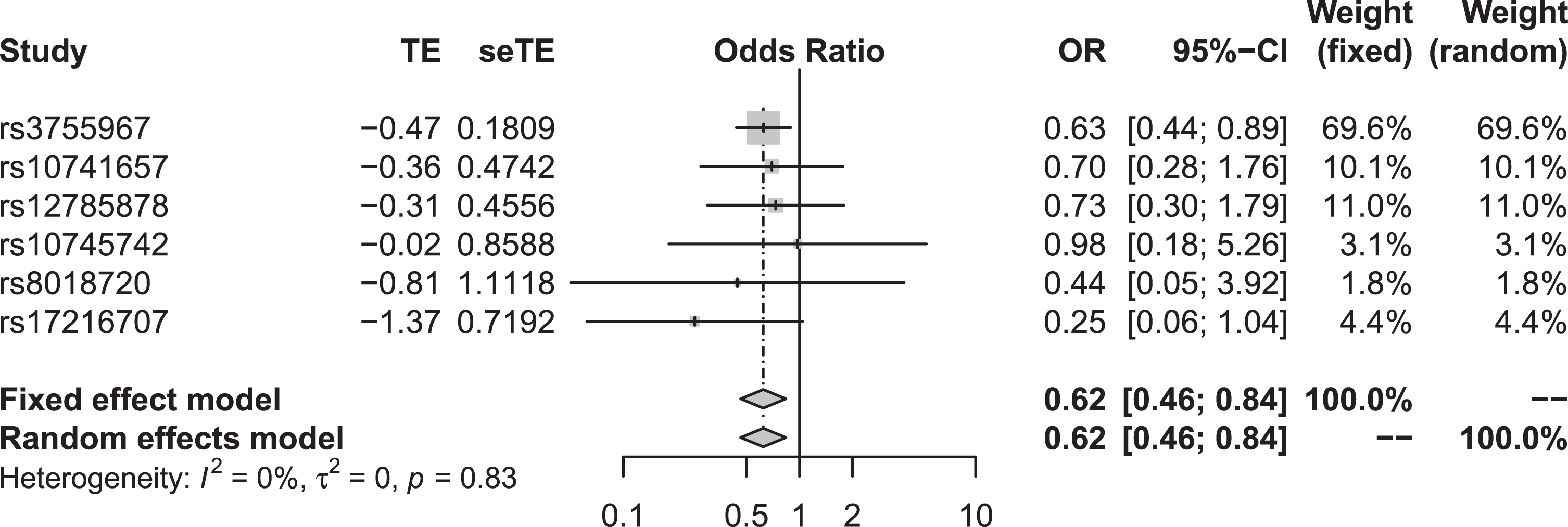
Individual genetic estimates from each of the 6 genetic variants using the IGAP GWAS dataset.
In the UK Biobank GWAS dataset, all these three methods showed suggestive effect of 25OHD levels on AD risk. The estimates are similar with those from the IGAP in terms of direction. However, the 95% CI included the null including IVW (OR = 0.88, 95% CI: 0.73–1.06, p = 0.19), weighted median (OR = 0.94, 95% CI: 0.76–1.14, p = 0.51), and MR-PRESSO (OR = 0.88, 95% CI: 0.74–1.06, p = 0.25). Figure 2 shows individual genetic estimates from each of the 6 genetic variants in the UK Biobank GWAS dataset.

Individual genetic estimates from each of the 6 genetic variants using the UK Biobank GWAS dataset.
In both the IGAP and UK Biobank GWAS datasets, the leave-one-out permutation analysis further showed that the direction and precision of the estimates between 25OHD levels and AD remained largely unchanged using all these three methods (Table 2). All these findings suggest that our results are robust.
Leave-one-out permutation analysis of the association between 25OHD levels and AD in the IGAP and UK Biobank datasets
IGAP, International Genomics of Alzheimer’s Project; IVW, inverse-variance weighted meta-analysis; MR-PRESSO, Mendelian randomization pleiotropy residual sum and outlier; OR, odds ratio; CI, confidence interval.
Power analysis
In the IGAP GWAS dataset, the first-stage F-statistic was 1869.57 > 10. Our study had 80% power to detect an OR of 0.87 or lower per SD (25 nmol/L) increase in circulating 25OHD levels for AD, which are comparable with effect size that have been observed in observational studies relating circulating 25OHD levels to risk of AD with OR = 0.80 [11], and OR = 0.69 [12]. The N required for 80% power is 6135. Interestingly, the power is 89% to detect the genetic association between increased 25OHD levels and reduced AD risk with OR = 0.62. In the UK Biobank GWAS dataset, the first-stage F-statistic was 9187.39 > 10. Our study had 80% power to detect OR of 0.91 or lower per SD (25 nmol/L) increase in circulating 25OHD levels for AD. The N required for 80% power is 160,101. Interestingly, the power is 95% to detect the genetic association between increased 25OHD levels and reduced AD risk with OR = 0.88.
DISCUSSION
Until now, there has been an increased research interest for observational studies, genetic association studies, and randomized controlled trials exploring the impact of vitamin D intake (diet and supplements) on AD, due to its roles beyond bone health and calcium homeostasis [8]. Observational studies have reported that vitamin D deficiency is associated with an increased risk of AD [8–12]. However, randomized controlled trials have not provided strong evidence that vitamin D supplementation could improve cognitive outcomes [9]. Evidence shows that vitamin D supplementation may improve cognitive outcomes in individuals aged 60 years and over [9]. Until now, it remains unclear whether there is a causal association between increased vitamin D levels and reduced AD risk in individuals aged 60 years and over. Hence, we performed a MR study. Our main analysis using IVW method showed that genetically increased 25OHD levels were significantly associated with reduced AD risk individuals aged 60 years and over. Importantly, the estimates from other two sensitivity analysis methods were consistent with the IVW estimate in terms of direction and magnitude. A leave-one-out permutation further suggested that these estimates were robust.
Comparison with randomized controlled trials
In 2004, Dhesi et al. selected 139 ambulatory subjects with vitamin D insufficiency (aged 65 years and over), and found that 25OHD levels in the treatment group increased significantly after 6 months post-intervention [34]. Importantly, vitamin D supplementation could improve functional performance, reaction time and balance [34]. In 2011, Stein et al. first performed a pilot study of 13 AD individuals aged > 60 with median Folstein Mini-Mental State Examination (MMSE) score 21.5 [35]. These 13 AD cases were treated with open label 3000 IU vitamin D2 tablets for 8 weeks, with dose adjustments to maintain 25OHD 135–160 nM [35]. Their results showed that the median 25OHD levels increased from 66 to 140 nM [35]. Median baseline AD assessment scale-cognitive subscale (ADAS-cog) was 25 and median improvement in ADAS-cog score was 6.0 points [35]. The Disability Assessment in Dementia (DAD) score increased in 11 out of 13, which indicated less disability [35]. In 2011, Dean et al. conducted a randomized controlled trial to investigate the effects of vitamin D supplementation on cognitive and emotional functioning in 128 young adults with the mean age of 21.8 years including 63 individuals in treatment group and 65 individuals in placebo group for 6 weeks [36]. Their results showed no significant changes in working memory, response inhibition, cognitive flexibility, hallucination-proneness, psychotic-like experiences, and ratings of depression, anxiety, or anger [36]. In brief, randomized controlled trials have provided evidence that vitamin D supplementation could improve cognition in individuals aged 60 years and over, but not in young adults. Hence, our findings are consistent with those from randomized controlled trials.
Comparison with Mendelian randomization studies
Until now, MR studies have been conducted to test whether genetically vitamin D levels are associated with AD [15–17]. There are three main differences between our current study and previous studies. First, previous MR studies selected four genetic variants including rs2282679, rs12785878, rs10741657, and rs6013897 [15, 16]. The effect sizes about these four genetic variants on 25OHD levels were estimated in the Canadian Multicentre Osteoporosis Study (N = 2,347) [15, 16]. Hence, compared with 2,347 samples, the effect of each variant on 25OHD levels from 79,366 individuals will be more accurate, as we used in the current study [24]. Second, previous MR studies only selected the AD GWAS dataset from the IGAP including 17,008 cases and 37,154 controls without any replication dataset [15–17]. Here, we selected the IGAP GWAS dataset including 21,982 cases and 41,944 controls as the discovery dataset, and the UK Biobank dataset as the replication dataset. Third, previous studies reported that genetically vitamin D levels were associated with reduced risk of AD, but did not highlight the possible age threshold. Here, we confirmed the age threshold that genetically vitamin D levels could reduce the risk of AD in individuals aged 60 years and over [9].
Strengths and limitations
This MR study may have several strengths. First, we selected a large-scale vitamin D GWAS dataset (N = 79,366), and two large-scale AD GWAS datasets from the IGAP (N = 63,926) and UK Biobank (N = 314,278). Second, both the vitamin D and AD GWAS datasets include subjects of European descent, which may reduce the influence on the potential association caused by the population stratification. Third, we selected six independent genetic variants as the instruments, which may reduce the influence of linkage disequilibrium. Fourth, we selected multiple MR methods, which may examine the robustness of the estimate with each other. Fifth, we performed both manual and statistical pleiotropy analyses, which may reduce the risk of pleiotropy.
Meanwhile, this MR study may also have some limitations. First, we could not completely rule out additional confounders. Until now, it is almost impossible to fully rule out pleiotropy present in any MR study [16, 37]. Second, the causal association between vitamin D level and AD risk may differ across different ancestries. Hence, it should be further evaluated in other ancestries. Third, leave-one-out permutation analysis showed that none of these six genetic variants could largely change the direction and precision of the estimates between 25OHD levels and AD (Table 2). However, GC rs3755967 variant could affect the significance, which indicates that vitamin D-binding protein (DBP) (encoded by GC) may have distinct effects on AD risk [15]. Hence, future studies are required to evaluate the effect of DBP on AD risk. Fourth, we observed significant association in the IGAP, but not in the UK Biobank, which indicates the difference between clinically diagnosed AD and self-report AD-by-proxy [19].
Conclusions
Until now, many clinical trials of therapies for AD have failed, especially the double-blind, placebo-controlled, phase III trial involving patients with mild dementia due to AD [38, 39]. Meanwhile, growing evidence shows that vitamin D is involved the development of AD and cognitive decline. Here, we demonstrate that there is a direct causal association between genetically increased vitamin D levels and AD risk in people of European descent aged 60 years and over. Hence, our findings in combination with previous literatures indicate that maintaining adequate vitamin D status in older people especially aged 60 years and over, may contribute to slow down cognitive decline and to forestall AD. Long-term randomized controlled trials are required to test whether vitamin D supplementation may prevent AD in older people especially those aged 60 years and may be recommended as preventive agents.
Footnotes
ACKNOWLEDGMENTS
We thank the International Genomics of Alzheimer’s Project (IGAP) for providing summary results data for these analyses. The investigators within the IGAP contributed to the design and implementation of the IGAP and/or provided data but did not participate in analysis or writing of this report. The IGAP was made possible by the generous participation of the control subjects, the patients, and their families. The i-Select chips was funded by the French National Foundation on AD and related disorders. EADI was supported by the LABEX (laboratory of excellence program investment for the future) DISTALZ grant, Inserm, Institut Pasteur de Lille, Université de Lille 2 and the Lille University Hospital. GERAD was supported by the Medical Research Council (Grant n° 503480), Alzheimer’s Research UK (Grant n° 503176), the Wellcome Trust (Grant n° 082604/2/07/Z) and German Federal Ministry of Education and Research (BMBF): Competence Network Dementia (CND) grant n° 01GI0102, 01GI0711, 01GI0420. CHARGE was partly supported by the NIH/NIA grant R01 AG033193 and the NIA AG081220 and AGES contract N01-AG-12100, the NHLBI grant R01 HL105756, the Icelandic Heart Association, and the Erasmus Medical Center and Erasmus University. ADGC was supported by the NIH/NIA grants: U01 AG032984, U24 AG021886, U01 AG016976, and the Alzheimer’s Association grant ADGC-10-196728. We also thank the Social Science Genetic Association Consortium (SSGAC), DIAbetes Genetics Replication and Meta-analysis (DIAGRAM) Consortium, Genetic Investigation of ANthropometric Traits (GIANT) consortium; BPExome, International Consortium of Blood Pressure (ICBP) consortium, Tobacco and Genetics Consortium (TGC), Psychiatric Genomics Consortium (PGC), Alcohol Genome-Wide Association (AlcGen) and Cohorts for Heart and Aging Research in Genomic Epidemiology Plus (CHARGE+) Consortia, NIAGADS Consortium, and Ukbiobank for access to their GWAS datasets. This research has been conducted using the UK Biobank resource (https://www.ukbiobank.ac.uk). We thank the individual patients who provided the sample that made data available; without them the study would not have been possible. This work was partially supported by funding from the Science and technology Beijing one hundred leading talent training project (Z141107001514006), Beijing Municipal Administration of Hospitals’ Mission Plan (SML20150802), and the National Natural Science Foundation of China (81620108011).