
Abstract
Background
Alzheimer’s disease (AD) is the leading cause of dementia. Genetic components play an important role in AD and have been widely evaluated by genome-wide association studies (GWAS) and exome sequencing, and some common and rare genetic variants have been identified. In addition to genetic factors, environment factors have a role in AD. Growing evidence from observational studies linked impaired kidney function to cognitive impairment and AD; however, there are inconsistences in these findings.
Objective
To determine the causal effects of impaired kidney function and chronic kidney disease (CKD) on AD.
Methods
Mendelian randomization (MR) methods have been widely used to infer causal associations between exposure and outcome. Here, we conducted an MR study to investigate the causal effects of impaired kidney function and CKD on the risk of AD by analyzing large-scale GWAS datasets from FinnGen and CKD Genetics (CKDGen) Consortium.
Results
We found no significant but a suggestive effect of CKD on decreased risk of AD using inverse-variance weighted (IVW) (p = 8.46E–02) and simple mode (p = 7.60E–02) methods. We identified a statistically significant effect of the estimated glomerular filtration rate (eGFR) on increased risk of AD using IVW (p = 1.11E–02), weighted median regression (p = 5.60E–03), and weighted mode (p = 2.45E–02) methods.
Conclusions
Together, our findings indicate that high eGFR levels may increase the risk of AD. These findings need to be verified in future studies.
Keywords
Introduction
Alzheimer’s disease (AD) is the leading cause of dementia.1–3 Genetic components play an important role in AD, and have been widely evaluated by genome-wide association studies (GWAS) and exome sequencing, and some common and rare genetic variants have been identified.1,4, 1,4 In addition to genetic factors, environment factors are involved in AD. Growing evidence from observational studies linked impaired kidney function to cognitive impairment and AD; however, there are inconsistences in these findings.5–9
An observational study from the Rush Memory and Aging Project showed that a low estimated glomerular filtration rate (eGFR) at baseline was associated with rapid cognitive decline in 886 elderly people without dementia. 5 Sixteen years of follow-up of 191,970 elderly participants without dementia in the UK Biobank showed that moderately to severely impaired kidney function increased the risk of all-cause dementia (hazard ratio (HR) = 1.53, 95% CI: 1.32–1.76), vascular dementia (HR = 1.51, 95% CI: 1.13–2.02), and AD (HR = 1.27, 95% CI: 1.00–1.60, p = 0.046). 7
Kjaergaard and colleagues conducted a meta-analysis of 468,699 Scandinavians 9 and found that compared with the reference eGFR, mildly impaired (HR = 1.14, 95% CI: 1.06–1.22) and severely impaired (HR = 1.91, 95% CI: 1.21–3.01), but not moderately impaired (HR = 1.31, 95% CI: 0.92–1.87) eGFR significantly increased the risk of all-cause dementia. 9 However, only impaired (HR = 1.24, 95% CI: 1.08–1.43), but not moderately impaired (HR = 1.32, 95% CI: 0.87–1.99) or severely impaired (HR = 1.19, 95% CI: 0.70–2.04) eGFR significantly increased the risk of AD. 9 A recent 17 years of follow-up of 6,256 participants indicated that impaired kidney function did not increase the risk of all-cause dementia, AD, or vascular dementia. 8 Xu and colleagues evaluated the relation between eGFR and the risk of dementia in 329,822 elderly residents of Stockholm without dementia or kidney replacement therapy. 6 They found that compared with elderly residents with eGFR levels of 90–104 mL/min, elderly residents with eGFR levels≥105 mL/min had increased risk of all-cause dementia (HR = 1.30, 95% CI: 0.90–1.87, p = 0.16), vascular dementia (HR = 2.00, 95% CI: 1.02–3.95, p = 0.04), but not AD (HR = 0.76, 95% CI: 0.37–1.59, p = 0.47). 6
These inconsistent findings of the relationship between impaired kidney function and AD suggest that observational evidence may be problematic because observational studies often include confounding factors and reverse causality. 10 Mendelian randomization (MR) is an alternative and widely used way to infer causal associations between exposure and outcome. 10 Here, we conducted a MR study to investigate the causal effects of impaired kidney function and chronic kidney disease (CKD) on the risk of AD by analyzing large-scale GWAS datasets.
Materials and methods
Study design
We performed two-sample MR to evaluate the causal effects of impaired kidney function and CKD on the risk of AD using large-scale publicly available and independent kidney function, CKD, and AD GWAS summary statistics. The study design is shown in Figure 1.
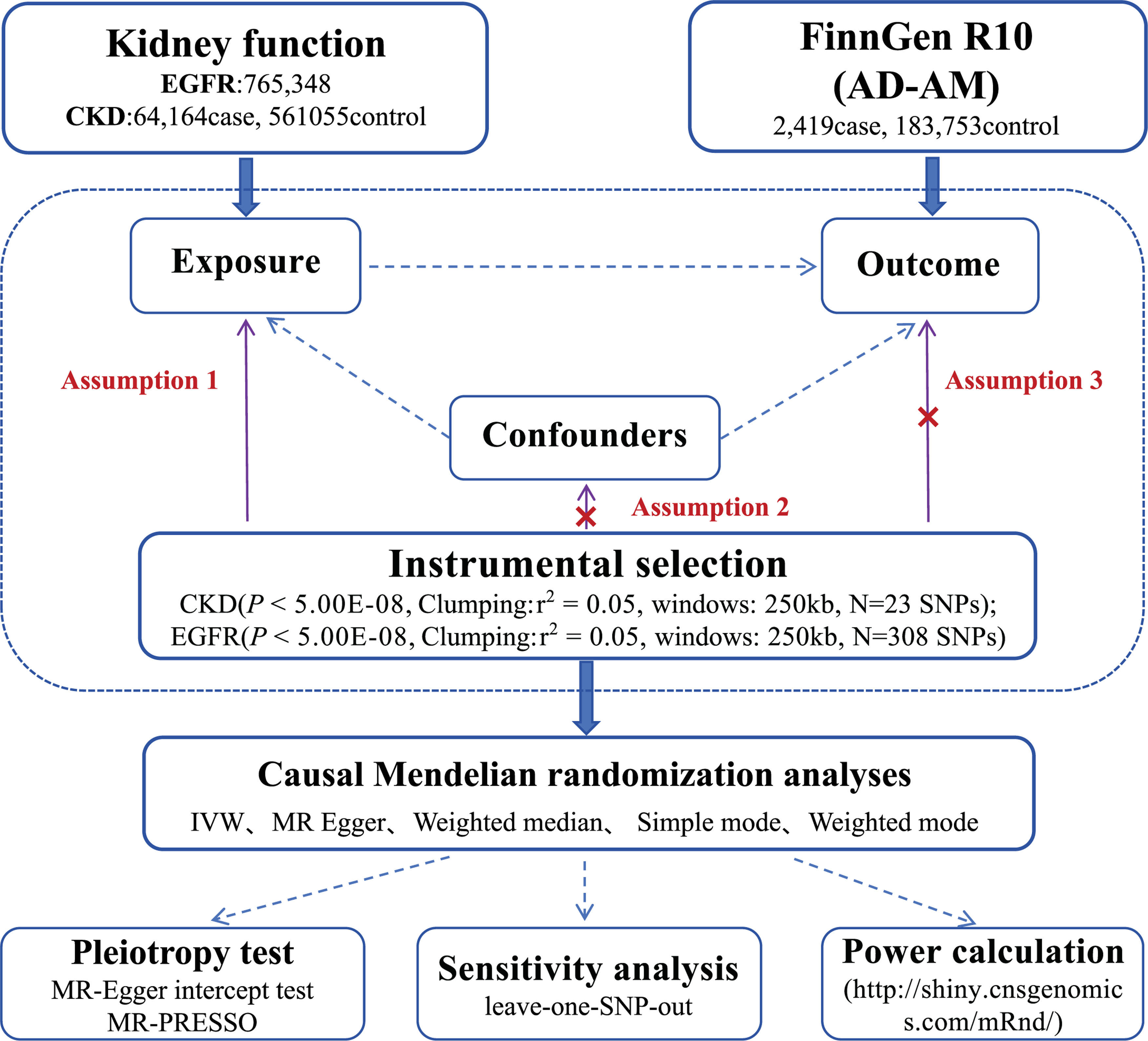
Study design used in this study.
eGFR, CKD, and AD GWAS datasets
The eGFR and CKD GWAS datasets were obtained from the CKD Genetics (CKDGen) Consortium. 11 The CKDGen Consortium performed a large-scale trans-ancestry eGFR GWAS meta-analysis of 765,348 individuals of European, East Asian, African-American, South Asian, and Hispanic ancestry and identified 308 eGFR genetic variants with genome-wide significance. 11 The CKDGen Consortium also conducted a large-scale trans-ancestry CKD GWAS meta-analysis of 625,219 individuals, including 64,164 CKD cases, and identified 23 CKD genetic variants with genome-wide significance. 11 The AD GWAS dataset was from FinnGen R10 and consisted of 2,419 AD cases and 183,753 controls; AD was defined to be atypical or mixed with more control exclusions (AD_AM_EXMORE). 12 Here, we selected the 308 eGFR genetic variants and 23 CKD genetic variants identified by the CKDGen Consortium GWAS meta-analysis as the potential instrumental variables (IVs). A summary of the GWAS summary data used in the present study is provided in Table 1, and detailed information about the 2,419 AD cases from FinnGen R10 is provided in Figure 2.
Summary of the GWAS data used this study.

GWAS, genome-wide association study; CKDGen, Chronic Kidney Disease Genetics Consortium; FinnGen, FinnGen R10.

Detailed information of the 2,419 Alzheimer’s disease cases from FinnGen R10.
Mendelian randomization analysis
MR analysis was performed using five methods, inverse-variance weighted meta-analysis (IVW), weighted median regression, MR-Egger, simple mode, and weighted mode, that are well established and widely described.13–17 We selected IVW as the main analysis method and the others as the sensitivity analysis methods. Potential pleiotropy was evaluated using both the heterogeneity test from Cochrane’s Q statistic and pleiotropy test from MR-Egger and Mendelian Randomization Pleiotropy RESidual Sum and Outlier (MR-PRESSO).18,19, 18,19 All the statistical analyses were conducted using R software (v4.2.2), and the meta, MendelianRandomization, 20 and TwoSampleMR 15 R packages. The causal effects of eGFR and CKD were reflected using the odds ratio (OR) and 95% confidence interval (CI), which correspond to the AD risk for each standard deviation increase in eGFR levels and CKD. The statistically significant causal association was defined as p < 0.05.
Strength of instrumental variables
We calculate the proportion of eGFR variance explained by the IVs using R2 as:
We calculate the proportion of CKD variance explained by the IVs
using R2 as:
Using R2, we evaluated the strength of IVs by calculating the F statistic as:
Results
Strength of instrumental variables
The MR analyses were conducted using 308 eGFR and 23 CKD genetic variants as the potential IVs; 304 of the eGFR genetic variants and the 23 CKD genetic variants were available in AD GWAS summary datasets provided in Supplementary Tables 1 and 2. After excluding palindromic genetic variants (A/T or C/G), 252 eGFR and 18 CKD genetic variants are selected for the MR analyses.
The proportion of eGFR variance explained by the 252 eGFR genetic variants was 6.86%, and the proportion of CKD variance explained by the 18 CKD genetic variants was 5.61%. All 252 eGFR and 18 CKD genetic variants as the IVs had F > 10; indeed, all 18 CKD genetic variants had minimum F > 644 and all 252 eGFR genetic variants had minimum F > 62 (Supplementary Tables 3 and 4). The leave-one-out analysis did not identify a single IV that affected the overall causal estimate (Supplementary Tables 3 and 4).
Mendelian randomization analysis
No statistically significant causal association was detected between CKD and AD using IVW, weighted median regression, MR-Egger, simple mode, or weighted mode (Table 2); however, a suggestive association was detected between CKD and decreased risk of AD using IVW (p = 8.46E–02) and simple mode (p = 7.60E–02) (Table 2).
Causal effects of eGFR and CKD on the risk of AD.

eGFR, estimated glomerular filtration rate; CKD, chronic kidney disease; AD, Alzheimer’s disease; SE, standard error; CI, confidence interval; MR, Mendelian randomization; IVW, inverse-variance weighted. A statistically significant causal association was defined as p < 0.05.
We found a statistically significant causal association between eGFR and AD using IVW (p = 1.11E–02), weighted median regression (p = 5.60E–03), and weighted mode (p = 2.45E–02) (Table 2). Each standard deviation increase in eGFR levels was significantly associated with increased risk of AD (beta = 1.945, standard error = 0.766, 95% CI: 0.443–3.446, p = 1.11E–02). Importantly, the directions of MR estimates from MR-Egger and simple mode were consistent with those from IVW, weighted median regression, and weighted mode; however, no statistically significant causal association was detected using MR-Egger and simple mode (Table 2). The forest plot for overall causal effects of eGFR and CKD on the risk of AD using five MR methods is shown in Figure 3. The scatter plot of the individual causal effects of eGFR and CKD on the risk of AD using five MR methods is shown in Figure 4.
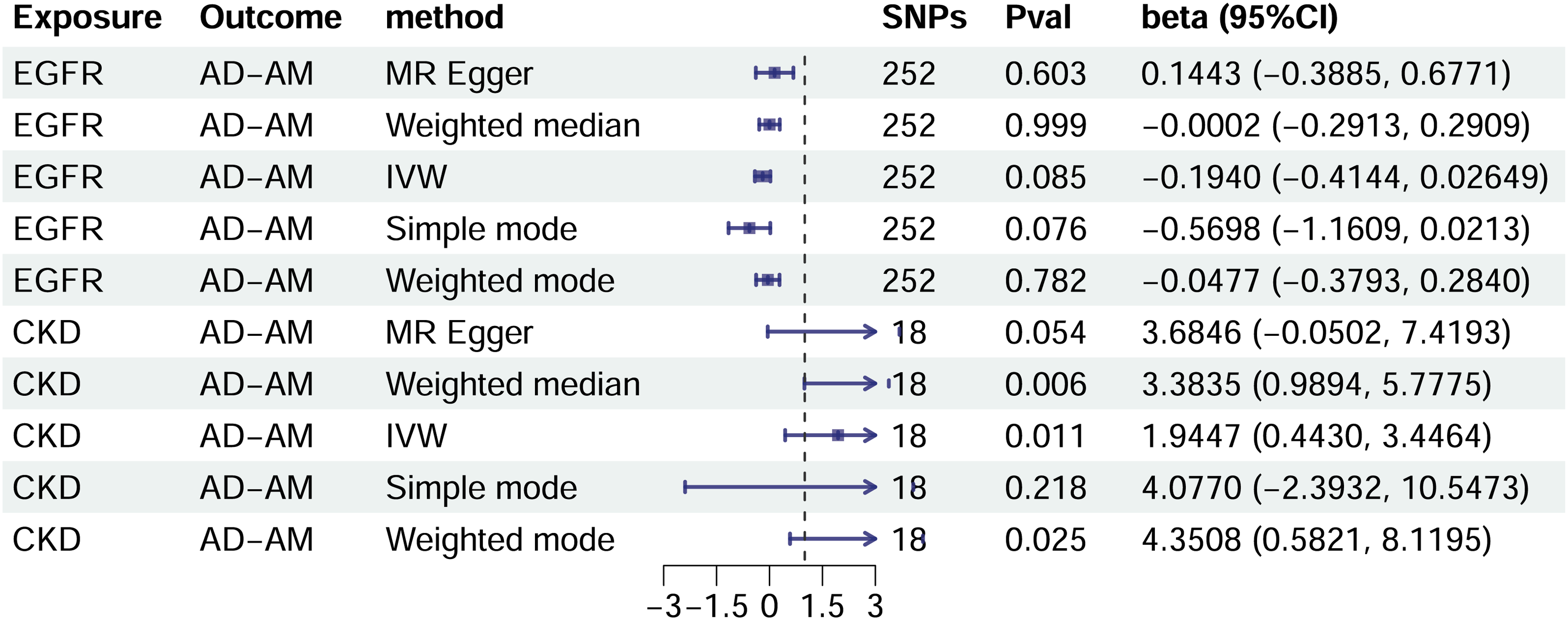
Forest plot of the overall causal effects of eGFR and CKD on the risk of AD using five MR methods. eGFR, estimated glomerular filtration rate; CKD, chronic liver disease; AD, Alzheimer’s disease; MR, Mendelian randomization.
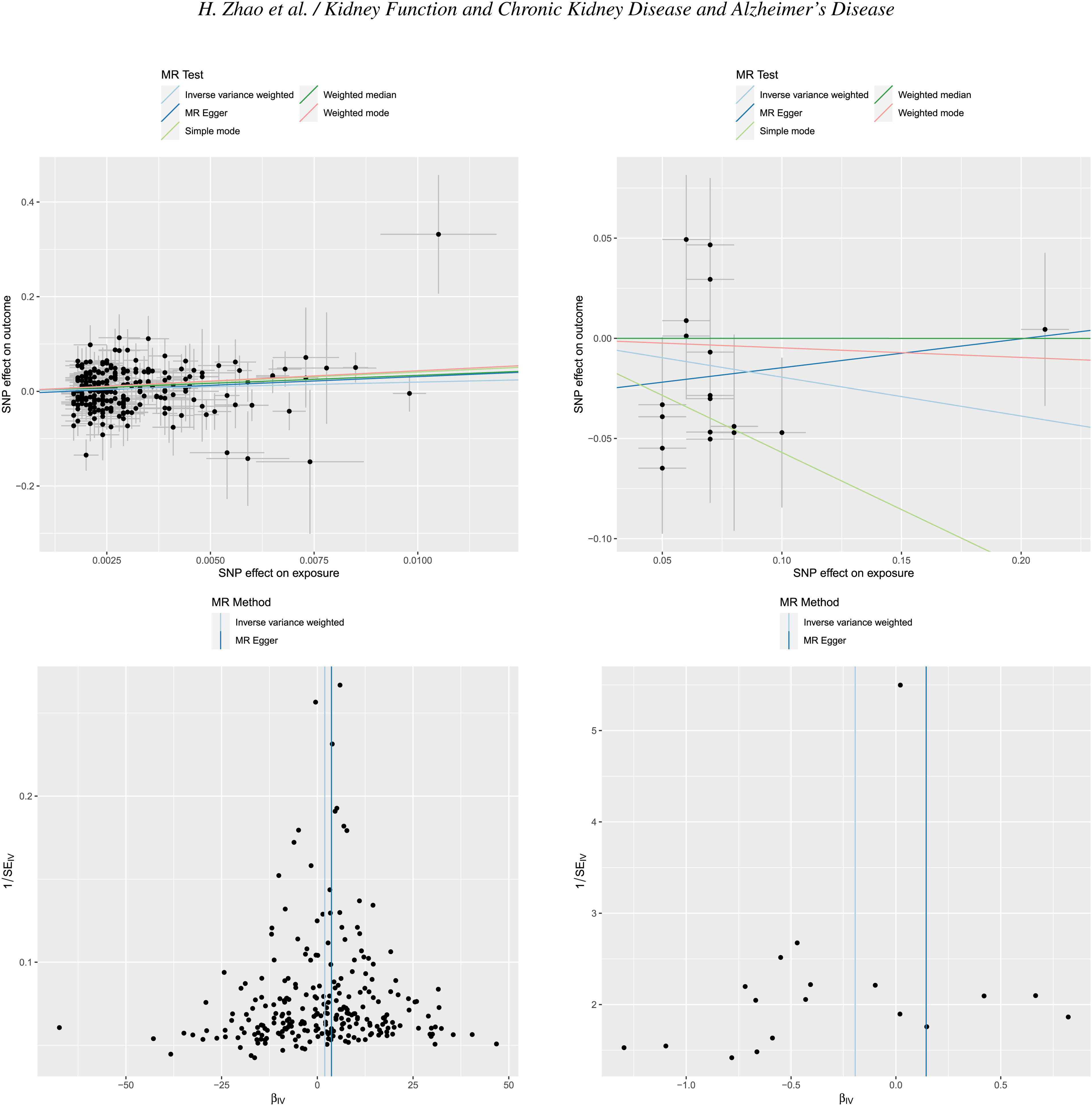
Scatter plot of the individual causal effects of eGFR and CKD on the risk of AD using five MR methods. eGFR, estimated glomerular filtration rate; CKD, chronic liver disease; AD, Alzheimer’s disease; MR, Mendelian randomization.
Pleiotropy analysis
No clear pleiotropy was detected using the heterogeneity test with Cochrane’s Q statistic p > 0.05 in IVW and MR-Egger. The MR-Egger intercept test and MR-PRESSO global test also supported the lack of clear pleiotropy (Table 3). Together, all these findings show that the 252 eGFR and 18 CKD genetic variants met the IV assumptions.
Heterogeneity test and pleiotropy test of MR results.

MR, Mendelian randomization; IVW, inverse-variance weighted; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate.
Discussion
Observational studies have produced inconsistent findings about the association between impaired kidney function and AD.5–9 Here, we performed an MR study to evaluate the causal effects of eGFR and CKD on the risk of AD by analyzing large-scale GWAS datasets. We found no significant but a suggestive effect of CKD on decreased risk of AD using IVW (p = 8.46E–02) and simple mode (p = 7.60E–02). We identified a statistically significant effect of eGFR on increased risk of AD using IVW (p = 1.11E–02), weighted median regression (p = 5.60E–03), and weighted mode (p = 2.45E–02).
These findings show that CKD may reduce the risk of AD, and genetically high eGFR levels may increase the risk of AD. Our MR results are consistent with those of recent observational studies. Kjaergaard and colleagues conducted a Danish nationwide cohort study that included 82,690 patients with kidney disease and 413,405 healthy controls from the general population. 24 They found that kidney disease was significantly associated with increased risk of all-cause dementia (HR = 1.08, 95% CI: 1.03–1.12) and vascular dementia (HR = 1.26, 95% CI: 1.14–1.40), but associated with decreased risk of AD (HR = 0.85, 95% CI: 0.78–0.92). 24 A cohort study of 4,320,824 Denmark individuals > 40 years old showed that kidney disease, including CKD, was associated with the risk of all-cause dementia (HR = 1.15, 95% CI: 1.10–1.20) and vascular dementia (HR = 1.43, 95% CI: 1.33–1.54), but not associated with the risk of AD (HR = 0.98, 95% CI: 0.94–1.03). 25
Our MR findings are the first to highlight the causal association between kidney function and AD. Two previous MR studies evaluated the causal effect of kidney function on the risk of AD.9,26, 9,26 Liu and colleagues used three kidney function measures, eGFR, CKD, and blood urea nitrogen (BUN), and evaluated their effects on six neurodegenerative diseases, namely AD, multiple sclerosis, Parkinson’s disease, frontotemporal dementia, amyotrophic lateral sclerosis, and Lewy body dementia. 26 They selected 264 independent BUN, 147 independent CKD, and 308 independent eGFR genetic variants. 26 However, only 93 BUN, 27 CKD, and 191 eGFR genetic variants were available in the AD GWAS dataset from a meta-analysis of the International Genomics of Alzheimer’s Project GWAS stage 1 (21,982 AD and 41,944 controls) and UK Biobank (53,042 proxy AD and 355,900 controls) datasets. 27 The MR analysis showed lack of statistically significant effects of eGFR, CKD, or BUN on the risk of AD. 26 Kjaergaard and colleagues selected four kidney function measures, eGFR, BUN, CKD, and the urinary albumin-creatinine ratio (UACR), and evaluated their effects on AD using multiple AD GWAS datasets such as FinnGen R5, IGAP, IGAP/UKB and ADSP/IGAP/PGC-ALZ/UKB. 9 They selected 169 eGFR, 24 CKD, 24 BUN, and 55 UACR genetic variants as the potential IVs; however, no statistically significant association of impaired kidney function with the risk of all-cause dementia and AD was detected. 9
In summary, our findings indicate that CKD was not significantly associated with the risk of AD, whereas high eGFR levels may increase the risk of AD. These findings need to be verified in future studies using large-scale sample sizes.
Acknowledgments
We thank Margaret Biswas, PhD, from Liwen Bianji (Edanz) (http://www.liwenbianji.cn/) for editing the English text of a draft of this manuscript.
Supplemental Material
Supplementary Table 1
Supplementary Table 2
Supplementary Table 3
Supplementary Table 4
Footnotes
Author contributions
Hainan Zhao (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Resources; Software; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing); Hongxia Yuan (Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Resources; Software); Ermin Wang (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration).
Funding
This work was supported by funding from the Project Guided by the Jinzhou Science and Technology Bureau (JZ2023B091), and the General Project of Liaoning Provincial Department of Science and Technology (2021-MS-335).
Declaration of conflicting interests
The authors have no conflict of interest to report.
Data availability
All relevant data are within the paper. The authors confirm that all data underlying the findings are either fully available without restriction through consortia websites, or may be made available from consortia upon request.