
Abstract
Background:
Asthma and chronic obstructive pulmonary disease (COPD) are common comorbidities in persons with Alzheimer’s disease (AD). However, pharmacotherapy of these diseases may have opposite mechanisms of action; anticholinergics in asthma/COPD and acetylcholinesterase inhibitors (AChEI) in AD.
Objective:
To investigate whether existing asthma/COPD affects the choice of AD medication, and the survival of the patients with AD.
Methods:
In this retrospective cohort study, data from the MEDALZ-study, which includes all community-dwelling persons with AD during 2005–2011 in Finland (n = 70718) was utilized. Persons with asthma/COPD (N = 7211) were defined as having a special reimbursement for asthma/COPD, or long-term use (≥250 days) of inhaled anticholinergics, inhaled corticosteroids, or leukotriene antagonists during the year before AD diagnosis. We compared persons with and without asthma/COPD regarding the choice of the initial antidementia medication (AChEI versus memantine) with logistic regression and mortality with Cox regression model during the follow-up (up to end of 2015).
Results:
Memantine was favored over AChEIs as first-line treatment to AD in persons with asthma/COPD compared to those without asthma/COPD (odds ratio 1.23, 95% confidence interval (CI) 1.15–1.31). Memantine was also more commonly used among those who used multiple asthma/COPD medications (7.9% of memantine initiators used ≥3 asthma/COPD medications compared with 5.5% of those who initiated with AChEI). Mortality was higher in persons with asthma/COPD compared to those without asthma/COPD (adjusted hazard ratio 1.10, 95% CI 1.07–1.13).
Conclusion:
More frequent use of memantine instead of AChEI may result from an attempt to prevent possible worsening of asthma/COPD by AChEIs. Vulnerable persons with both AD and asthma/COPD need individually assessed pharmacotherapy for their medical conditions.
Keywords
INTRODUCTION
Pharmacotherapy of Alzheimer’s disease (AD) is currently based on acetylcholinesterase inhibitors (AChEI) (donepezil, rivastigmine, galantamine) and the NMDA antagonist, memantine [1, 2]. AChEIs increase the concentration of acetylcholine in cholinergic synapses, resulting in small improvements in cognitive functioning in mild to moderate dementia, whereas memantine produces small benefits in moderate to severe dementia on behavior, global functioning, and activities of daily living [3, 4]. Memantine blocks NMDA receptors, preventing the deleterious effects of excitotoxicity caused by pathologically elevated levels of glutamate [3]. It has also been well tolerated without significant adverse effects [2, 5]. The Finnish clinical care guideline for cognitive disorders states that AChEIs are the first-line treatment for mild AD, but if there is contraindication for AChEI use, treatment can start with memantine [6]. In moderate-severe AD, both AChEIs and memantine can be used.
In Finland, the incidence of obstructive lung diseases (OLD) among adults starts to increase from the age of 40 years and continues at a high level until the age of 80. It is highest among persons aged 60–64 years [7]. Among persons with OLD, 17–19% have both asthma and chronic obstructive pulmonary disease (COPD), [8] and their proportion increases with age [8]. Age increases the prevalence of a combined diagnoses (two out of three) of asthma, COPD, or emphysema, with prevalences of 41.5%, 58.8% and 65.5% among patients with OLD in the age groups 60–69, 70–79 and >80 years, respectively [8]. The prevalence of asthma among older population is about 10% [9].
Hypoxemia is a common condition in COPD that also correlates with neuropsychological impairment [10]. COPD is associated with a high risk of cognitive disorders and it is suspected to be due to hypoxemia, hypercapnia, and hypoperfusion which may accentuate neuronal damage [11–14]. In addition, asthma has negative effects on cognition [15]. Asthma and COPD treatment are based on inhaled corticosteroids, short- and long-acting beta-agonists, and inhaled long-acting anticholinergics [7, 17]. As muscarinic antagonists have the opposite mechanism of action than cholinesterase inhibitors, their concomitant use may decrease the beneficial effects of AChEI medication in AD patients, although inhaled drugs have only limited passage to the blood stream and across the blood-brain barrier (BBB) [18]. However, permeability of BBB is increased in AD patients [19, 20]. Inhaled muscarinic antagonists, such as ipratropium, tiotropium, and oxitropium, are non-selective antagonists. As prevalence of both asthma/COPD and AD are high in the oldest age groups, many asthma/COPD patients will develop AD which may complicate their treatment. On the other hand, asthma/COPD may impact on selection of antidementia pharmacotherapy due to potential pharmacodynamic interaction between muscarinic antagonists and AChEIs. According to the Finnish clinical care guideline of cognitive disorders, in general, the use of anticholinergics should be avoided in persons with AD; however, it is likely that beneficial effects of inhaled anticholinergics used in COPD overweigh their possible CNS adverse effects [6].
In this paper we have investigated if previously diagnosed asthma/COPD affects the selection of AD medication in newly diagnosed AD patients. In addition, we investigated if asthma/COPD affects the survival of persons with AD.
METHODS
We used data from the MEDALZ-study [21] which includes all 70,718 community-dwelling persons who received a clinically verified diagnosis of AD during 2005–2011 in Finland. The Special Reimbursement register, including data on persons entitled for higher reimbursement of medication due to chronic diseases, was utilized in identification of persons for the MEDALZ-study cohort. For the reimbursement of anti-dementia medications, a diagnostic process of AD is to be conducted according to a predefined protocol set by the Social Insurance Institution of Finland (SII). This protocol includes symptoms consistent with AD, exclusion of alternative diagnoses, and computed tomography or MRI scan according to the NINCDS-ADRDA [22] and DSM-IV criteria. The SII evaluates the fulfillment of the criteria according to the certificate confirmed by a geriatrician or neurologist and grants special reimbursement if the criteria are fulfilled.
Data has been collected from several nationwide registers: Prescription register (years 1995–2015), Special Reimbursement register (1972–2015), Hospital Discharge register (1972–2015), and socioeconomic data since 1970 and causes of death 2005–2015 from Statistics Finland. All of the registers cover all residents and can be linked through personal identification numbers. The Prescription register includes the dispensing of reimbursed medications, excluding over-the-counter medications and drugs used during hospital care (when drugs are provided by the caring unit and not recorded in the register). Medications for asthma/COPD are reimbursed, with very few exceptions. Asthma and COPD are included under the same reimbursement code in the Special Reimbursement register. For COPD, this reimbursement is granted only for severe COPD cases. Medications are categorized according to Anatomical Therapeutic Chemical – classification system (ATC) codes [23].
At the time of the AD diagnosis, persons were grouped as having asthma/COPD versus not having asthma/COPD, and persons who were diagnosed with asthma/COPD after AD diagnoses (N = 305) were excluded from the analyses. Persons with asthma/COPD were defined as having a special reimbursement for asthma/COPD before the AD diagnosis or long-term use (≥250 days) of inhaled anticholinergics, corticosteroids or leukotriene antagonists during the year preceding the AD diagnosis (defined in Supplementary Table 1). Long-term use could include one or several of the above-mentioned drug classes as long as the number of days exposed to any asthma/COPD medication was ≥250. Duration of asthma/COPD medication use was defined according to the PRE2DUP method [24]. The PRE2DUP method is based on the calculation of sliding averages of daily dose (in Defined Daily Doses, DDDs), according to individual drug use patterns. This method takes into account personal purchasing behavior, changing dose, stockpiling of drugs, and hospitalizations.
The follow-up started at the date of diagnosis of AD which represented baseline for this study. The initial antidementia medication was assessed as being either AChEI, memantine, or both (initiated at the same time), and compared between persons with and without asthma/COPD. Switches were defined as any changes in antidementia medication (switches between medications and concomitant use). Thus, our definition of switches may also include concomitant use of AChEI and memantine and we did not assess whether use of both medications (the first and second) were continued. Definitions of drug classes are provided in the Supplementary Table 1. The type and the number of asthma/COPD medications used at the initiation of antidementia medication were analyzed. The reasons for the end of antidementia medication use were death, long-term (>90 days) hospitalization/institutionalization, end of the study follow-up (December 31, 2015), and the discontinuation of medication use, which ever occurred first.
Statistical analysis
Descriptive statistics for baseline variables were conducted with chi squared tests (p-values). We also calculated 95% confidence intervals for proportions. Factors associated with choice of memantine (compared with AChEI) were investigated with logistic regression analyses among those who initiated the use with monotherapy of either AChEI or memantine. Both univariate and multivariable models were computed. The analyses were adjusted for age, gender, time since AD diagnoses, asthma/COPD, diabetes, rheumatoid arthritis and other connective tissue diseases, cardiovascular disease (coronary artery disease, hypertension, chronic heart failure), epilepsy, stroke, substance abuse, osteoporosis, baseline use of antipsychotics, antidepressants, benzodiazepines and related drugs, opioids, and proton pump inhibitors (PPIs) (measured at the index date).
Mortality was compared between persons with and without asthma/COPD with the Cox proportional hazard model and unadjusted Kaplan-Meier curves. Two follow-up times were used, including the unlimited follow-up time (maximum follow-up time for each person in terms of data linkage, variation from four to ten years), and also a 4-year follow-up from the initiation of the study as this was the maximum follow-up time in terms of data linkage available for everyone in the cohort. Analyses were adjusted for factors found to be associated with adverse respiratory outcomes and risk of death among persons with AD [25–27], which included age, gender, diabetes, rheumatoid arthritis and other connective tissue diseases, cardiovascular disease (coronary artery disease, hypertension, chronic heart failure), epilepsy, stroke, substance abuse, osteoporosis, baseline use of antipsychotics, antidepressants, benzodiazepines and related drugs, opioids, and proton pump inhibitors. Mortality risk results were expressed as hazard ratios (HRs) with 95% confidence intervals (CIs).
Statistical analyses were performed using SAS (version 9.4; SAS Institute Inc., Cary, NC, USA). The Kaplan Meier curve was drawn with RStudio with survival data calculated by SAS. According to the Finnish legislation, no ethics committee approval or patient consents were required as de-identified register-based data was used and the participants were not contacted.
RESULTS
In general, persons with AD and asthma/COPD (N = 7,211) had more diagnosed chronic diseases than those without asthma/COPD (N = 63,202) (Table 1). Diabetes, rheumatoid arthritis and other connective tissue diseases, as well as epilepsy were more common among persons with asthma/COPD.
Demographics, comorbidities, and respiratory drug use of the study population
Antidementia medication initiation
Persons with and without asthma/COPD initiated antidementia medication equally (94% of both groups initiated use; Table 2). Among persons with asthma/COPD, AChEI was initiated slightly less frequently (74.0% versus 77.8%) and memantine more frequently (19.2% versus 15.5%) than in persons without asthma/COPD. Switches from AChEI to memantine and from memantine to AChEI were more common in persons without asthma/COPD than in persons with asthma/COPD. Death was a more common reason for ending AChEI or memantine use in persons with asthma/COPD (16.1%) than in persons without asthma/COPD (12.7%).
Initiations and switches/discontinuations of AD medication in AD patients with and without asthma/COPD
AD, Alzheimer’s disease; COPD, chronic obstructive pulmonary disease; AChEI, acetylcholine esterase inhibitor; CI, confidence interval. “Other change” includes switches from combination to AChEI, from combination to memantine, and switches within combination use.
Choice of antidementia medication according to asthma/COPD medication use
Compared with AChEI initiators with asthma/COPD, memantine initiators were more commonly using either inhaled anticholinergic (13.7% and 9.8% of initiators of memantine and AChEI, respectively), inhaled combination (36.8% and 31.7%, respectively), or leukotriene antagonist (12.6% and 9.8%, respectively) as asthma/COPD medication. Of memantine initiators, 7.9% had at least 3 asthma/COPD medications compared with 5.5% of those initiating with AChEI (Table 3).
Initial choice of AD medication according to asthma/COPD drug categories among persons with AD and COPD
AD, Alzheimer’s disease; COPD, chronic obstructive pulmonary disease; AChEI, acetylcholine esterase inhibitor.
Factors associated with memantine initiation
Asthma/COPD increased the probability of memantine being the first antidementia drug choice independent of comorbid conditions and medications (OR 1.23, 95% CI 1.15–1.31). Other factors associated with memantine use were age >80 years, male gender, cardiovascular disease, stroke, substance abuse, and use of antipsychotics, BZDRs, opioids, and PPIs (Table 4). Among those persons (with or without asthma/COPD) who initiated antidementia drug use, the share of memantine as the initial drug increased from 11.1% in persons aged 66–75 years to 23.6% in persons older than 85 years. Similarly, as the time from AD diagnosis to initiation of AD medication increased from <60 days to >120 days, the share of memantine increased from 14.0% to 20.4%, with a respective decrease in AChEI initiations.
Factors associated with memantine being the first antidementia drug instead of AChEI among persons with Alzheimer’s disease
COPD, chronic obstructive pulmonary disease; BZDR, benzodiazepines and related drugs; PPI, proton pump inhibitor; aOR, adjusted odds ratio; CI, confidence interval. Adjusted for age, gender, time since AD diagnoses (≤2 months, >2–4 months, >4 months), asthma/COPD, diabetes, rheumatoid arthritis, cardiovascular disease, epilepsy, stroke, substance abuse, osteoporosis, antipsychotics, antidepressants, benzodiazepines and related drugs, opioids, and PPIs.
Mortality associated with asthma/COPD
During the first four years of follow-up, 39.8% (N = 2,869) of persons with asthma/COPD and 33.8% (n = 21,346) of persons without asthma/COPD died, and risk of death during four years of follow-up for persons with and without asthma/COPD is presented in Fig. 1. The unadjusted risk of mortality during the first four years was higher among persons with asthma/COPD than in persons without asthma/COPD (HR 1.24, 95% CI 1.19–1.29) and remained elevated after adjustments with other medical conditions and medications at baseline (adjusted HR 1.10, 95% CI 1.06–1.15).
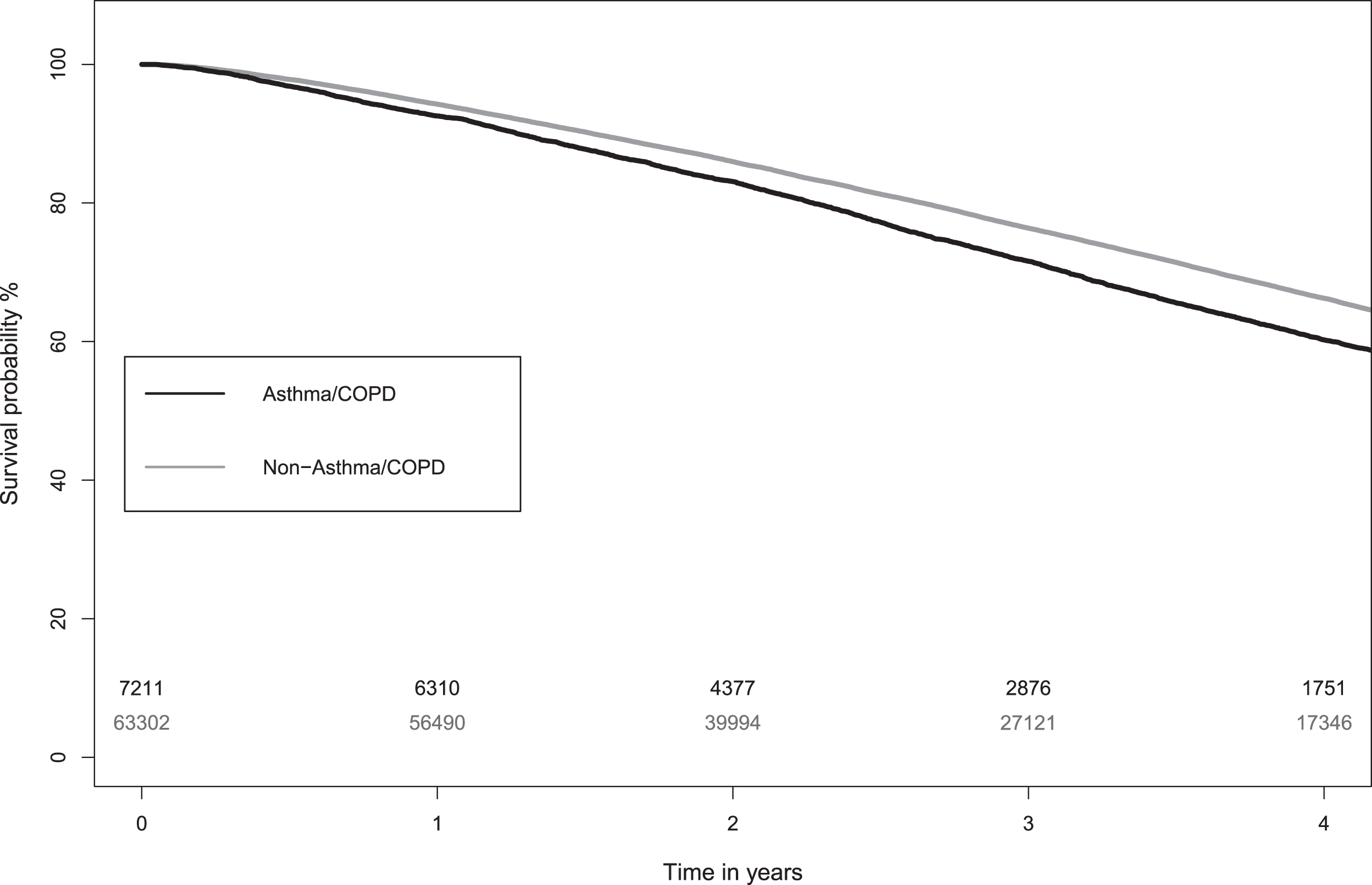
Unadjusted Kaplan-Meier survival plot showing the risk of death in people with Alzheimer’s disease with and without asthma/COPD. The number of persons at risk at each year mark are indicated in the lower part of the figure, with the same colors are the curves (black indicating Asthma/COPD and gray indicating Non-Asthma/COPD persons).
Altogether, during the median follow-up time of 4.8 years (IQR 3.1–6.5), 67.3% (N = 4,852) of persons with asthma/COPD died compared with 62.6% (n = 39,577) of persons without asthma/COPD. The unadjusted risk of mortality was higher among persons with asthma/COPD than in persons without asthma/COPD (HR 1.19, 95% CI 1.16–1.23). When adjusted with other medical conditions and medications at baseline (excluding AD drugs) the HR was 1.10 (95% CI 1.07–1.13).
DISCUSSION
In this study, we found that memantine was initiated as first-line AD treatment instead of AChEIs more frequently among persons with asthma/COPD than those without asthma/COPD. This was especially common in persons using inhaled anticholinergics alone or in combination with long-acting beta-agonist, or leukotriene agonists. These persons were likely to be at a more advanced stage of AD or had a poorer status of asthma/COPD, which both may be seen as contraindications for AChEI initiation. This is supported by the finding that the likelihood for initiation of memantine instead of AChEI increased when the number of asthma/COPD medications in use increased, indicating that the aim was to avoid the worsening of asthma/COPD and subsequent hypoxemia [6]. Another possible explanation is that the AD diagnosis might have been delayed among persons with asthma/COPD because cognitive decline has been considered to be at least partly hypoxia-related. Our data has no information about the stage of dementia nor asthma/COPD, but it is reasonable to assume that a higher number of asthma/COPD drugs is related to more severe asthma/COPD. Mortality was increased among persons with asthma/COPD compared to those without asthma/COPD, which is in agreement to previous studies [28].
Asthma/COPD with hypoxia has negative effects on cognition and thus, cognitive disorders and dementia are more prevalent among these persons than in persons without asthma/COPD [10, 28]. Therefore, effective treatment (including inhaled anticholinergics) of asthma/COPD is essential. On the other hand, AChEIs are the first-line treatment in mild and moderate dementia. Therefore, the decision of concomitant use of these opposing drug groups should be considered based on individual assessment of each patient.
Only a limited fraction (10–60%) of inhaled drugs is deposited in the airways [29] and therefore the amount of swallowed drug (available for gastrointestinal absorption) is high. Inhaled anticholinergics are quaternary ammonium compounds and thus, they are poorly absorbed in the gastrointestinal tract and normally do not cross the BBB [18]. However, they still have potential to cause systematic adverse effects such as constipation and urinary retention as well as increased heart rate [18]. In fact, the impairment of cognitive function has been noted with inhaled anticholinergics [30].
In addition, the BBB, which regulates the transport of molecules into and from the central nervous system (CNS), has been reported to be compromised and dysfunctional in AD, leading to its increased permeability. This allows drugs that would not normally pass the BBB to enter the CNS [19, 20]. Furthermore, the aging process affects sensitivity to drugs, as post-receptor responses and chemical interactions in drug exposure may be changed. In addition, older people have impaired hepatic and renal clearance leading to a prolonged elimination half-life and accumulation of several anticholinergic medicines and their metabolites [31]. Cholinergic activity is decreased in AD and vulnerability to anticholinergics is further increased in patients suffering from AD [32]. All of these changes increase the risk of cognitive decline caused by anticholinergics.
Adherence to inhaled therapy has been found to be suboptimal in persons with asthma and COPD, and cognitive impairment further decreases adherence [33, 34]. In addition, poor inhalation technique is common among persons with cognitive impairment [34]. In our study, we were able to determine medication purchases, but there is no information on the actual use of the drugs. It is likely, that the actual use of inhaled medications were lower than what would be expected from the purchases. This would lead to a smaller risk of interactions with AChEIs. On the other hand, suboptimal treatment of asthma/COPD may increase the hypoxia-related impairment in cognition.
The strength of our study is the inclusion of all community-dwelling persons with a clinically verified AD diagnosis in Finland, and assessment of their asthma/COPD, and thus the results are generalizable to community-dwelling older AD patient population. The major limitation of our study is the lack of information about severity of AD and asthma/COPD. In addition, we were unable to differentiate whether the persons had asthma, COPD, or both of these conditions. On the other hand, concomitant diagnosis of these conditions is common among persons with older age, and both conditions are treated with the same drugs. However, it is possible that compared to persons with asthma, those with COPD have poorer health status and lifestyle factors (e.g., it is likely that they smoke more often), leading to increased mortality risk.
AChEIs have been found to produce small, short-lived improvements in cognition in mild to moderate AD, and marginal benefits with severe disease. Memantine may have marginal effect on mild to moderate AD, and small benefits in moderate to severe AD [2, 3]. Therefore, in moderate to severe AD, both antidementia medications (AChEIs and memantine) may be effective and initiation of memantine instead of AChEI does not necessarily mean that antidementia treatment is to be suboptimal. On the other hand, AChEIs seem to be more effective than memantine in mild dementia, and in this case the favoring of memantine over AChEIs in persons with asthma/COPD may have a negative effect on cognition when compared with AD patients without asthma/COPD using AChEIs.
In conclusion, among persons with AD the use of AChEIs was less common and the use of memantine increased in persons with asthma/COPD compared to persons without asthma/COPD. Besides differences in the stage of AD, this may result from an attempt to prevent problems that may arise from the concomitant use of two drug classes with opposing mechanisms of action. As those with asthma/COPD had a higher risk of mortality than persons without asthma/COPD, the drug treatment of AD in persons with concomitant asthma/COPD should be carefully considered, and it should be based on an individual assessment in this vulnerable group of older patients.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/19-0850r2).