
Abstract
Background:
Depressive symptoms were thought to increase the risk of vascular dementia. Previous studies reported widespread white matter damages in the subcortical vascular mild cognitive impairment (svMCI), but little is known about the mechanism of depressive symptoms in svMCI.
Objective:
In the current study, we aim to explore the white matter microstructural alterations in svMCI with depressive symptoms, and their associations with clinical measurements.
Methods:
Fifty-eight subjects including 18 svMCI with depression (svMCI+D), 17 svMCI without depression (svMCI-D), and 23 normal controls (NC) were included in the study. Voxel-based analyses were performed on fractional anisotropy (FA) and mean diffusivity (MD).
Results:
Compared to NC, both svMCI groups showed decreased FA in the bilateral insula and the left precentral gyrus, and increased MD in the cerebellum. Compared to svMCI-D, svMCI+D showed increased FA in left precentral gyrus. Moreover, svMCI+D showed significant correlation between the increased MD in the cerebellum and the Hamilton Depression Rating Scale (HAMD) scores.
Conclusion:
Our findings of white matter alterations might be associated with executive function and memory performance in the svMCI patients. Moreover, the structural alterations in the cerebellum might underlie the mechanism of depressive symptoms in svMCI patients.
INTRODUCTION
Subcortical vascular dementia (SVaD) is mainly caused by cerebral small vessel lesions, showing lacunae and extensive white matter lesions [1] on magnetic resonance imaging (MRI) images. Similar to Alzheimer’s disease, SVaD has a long incubation period, with the evidence that the white matter is known to be disrupted as early as the age of 30 [2]. Subcortical vascular mild cognitive impairment (svMCI) is widely believed to be the prodromal stage of SVaD [3–6]. Since the deterioration process from svMCI to SVaD could be slowed by modifying risk factors [7], exploring the structural abnormalities in the patients with svMCI is extremely important to early intervention of SVaD.
Previous studies showed that depressive symptom is one of the risk factors for dementia. For instance, Bassuk et al. found that the presence of depressive symptoms presaged cognitive loss in elderly people with moderate cognitive impairments [8]. Michael et al. reported that comorbid depression could accelerate cognitive decline in dementia [9]. Furthermore, a cohort study with 17 years follow up period showed that depressive symptoms increased the risk of dementia by 50% [10]. Similarly, several systematic review and meta-analyses studies showed that depressive symptom was a major risk factor in developing dementia [11–14]. Moreover, a greater risk (caused by depressive symptoms) for vascular dementia compared to other types of dementia was found in the Maastricht Ageing Study [15]. This is further supported by the study which reported that the increased risk of vascular dementia would be related to depression [16]. However, although the phenomenon is widely reported, little is known about the mechanism underlying depressive symptoms in the svMCI.
Diffusion tensor imaging (DTI) is widely used to investigate the white matter microstructure changes in various neuropsychiatry diseases [17–20] by measuring the fractional anisotropy (FA) and mean diffusivity (MD) [21]. Decreased FA and increased MD in a wide range of brain regions with white matter hyperintensities and their surrounding penumbras were identified in the patients with svMCI [22, 23]. Moreover, other studies also reported that damages of specific white matter fibers were associated with certain cognitive impairments in patients with svMCI [24, 25]. However, these studies were mainly focused on svMCI, with little attention paid to svMCI with depressive symptoms. Recently, a DTI study on MCI with depressive symptoms found disintegration of white matter tracts within the frontal, temporal, and limbic regions which are important to regulate the affect and emotion [26]. Moreover, significantly lower FA was also identified in SVD patients with depression [27]. These two studies draw our attention to investigate microstructural changes related to the svMCI with depressive symptoms.
In the current study, we assessed white matter microstructural damage measured by FA and MD in svMCI patients with and without depressive symptoms. Furthermore, correlations between the altered FA/MD and the clinical measures (Montreal Cognitive Assessment test, MOCA [28] and Hamilton depression rating scale, HAMD scores) were investigated, respectively.
MATERIALS AND METHODS
Participants
Fifty-eight subjects including 35 svMCI and 23 NC were involved in the current study. The svMCI were recruited from the department of encephalopathy and psychology in Shenzhen Traditional Chinese Medicine Hospital and the NC were recruited from the local community via advertisements. The Institutional Review Board of Shenzhen Traditional Chinese Medicine Hospital approved the current study (Approval number: 2016-02), and all subjects provided informed written consents. Moreover, all subjects underwent the demographics, clinical, medical, drugs treatment history, neuropsychological assessments, and brain MRI scanning including hippocampal assessment at screening, and their demographic data were listed in Table 1.
Demographic data and clinical measures
ANOVA showed significant differences in MOCA and HAMD scores. a–c: post hoc analysis revealed the source of ANOVA (asvMCI+D versus NC, bsvMCI-D versus NC, and csvMCI+D versus svMCI-D). ANOVA, analysis of variance; MOCA, Montreal Cognitive Assessment; HAMD, Hamilton Depression Scale; svMCI+D, subcortical vascular mild cognitive impairment with depression; svMCI-D, subcortical vascular mild cognitive impairment without depression; and NC, normal controls.
Patients were recruited based on following criterion: 1) over 50 years old; 2) cognitive complaints by the patients/caregivers; 3) cognitive decline in one or more domain but no dementia (clinical dementia rating (CDR) of one or more domain≥0.5, the global score≤0.5, and the MOCA < 26); 4) normal activities of daily living; and 5) the T2 FLAIR images showed white matter hyperintensity (WMH) with Fazekas rating scale score≥2, or multiple (>3) supratentorial subcortical small infarcts (<20 mm), or one/more subcortical small infarcts in the caudate nucleus, globus pallidus, or thalamus. Moreover, all the patients were excluded if they have any of these: 1) cortical and watershed infarcts, hemorrhages, and WMH with specific causes; 2) atrophy in hippocampal or entorhinal cortex; 3) major depression or schizophrenia according to the Diagnostic and Statistical Manual of Mental Disorders-V (DSM-V) or HAMD score > 17; 4) other disorders that may affect cognition; 5) other major disorder such as cancer; and 6) drug abuse.
The NC was evaluated using the SCID Non-Patient Edition to confirm lifetime absence of Axis I illness. Other exclusion criteria were: history of psychiatric illness in any two lines of first to third degree biological relatives, history of seizures, previous head trauma with loss of consciousness, disorders that may affect cognition, serious medical or surgical illness, substance abuse or dependence, or contraindications for MRI.
Clinical measurements
The global cognitive function was evaluated by MOCA. Depressive symptoms were measured by the 17-item HAMD. In clinical trials, scores more than 17 points are thought as clinically significant depression, and less than 7 points are considered as clinical recovery (not of any clinical significance). Thus, patients with HAMD-17 scored 7–17 were classified into svMCI+D. In order to ensure that the patients in the current study were pure vascular mild cognitive impairment rather than vascular depression, we excluded patients with HAMD-17 scored more than 17 points. Finally, 18 subjects with svMCI+D and 17 subjects with svMCI-D were included in the current study.
Data acquisition
MRI scanning was performed using a 3T GE MR750 scanner. The diffusion weighted images (DWI) were acquired with the following parameters: 25 diffusion images with b = 1000 s/mm2 and 4 non-diffusion-weighted images (b = 0 s/mm2), repetition time = 8000 ms, echo time = 101.1 ms, field of view = 256×256 mm2, matrix size = 256×256, slice thickness = 4 mm, and slice number = 38.
Statistical analysis of demographic and clinical measures
The difference of gender was tested by chi-square test, whereas difference of other demographic and clinical data was analyzed using one-way analysis (ANOVA) among the three groups. Bonferroni corrections were used as multi-comparison corrections. Then, post hoc t tests were performed to detect the specific differences between any two groups. All the above analyses were implemented by IBM SPSS 19.
DTI image preprocessing
Preprocessing of DTI was conducted using FSL software (FMRIB Software Library, Oxford, UK, http://www.fmrib.ox.ac.uk/fsl/). The eddy current-induced distortions and head motion were corrected by aligning the DWI scans to the b0 images [29]. Then the Brain Extraction Tool was performed to extract the cerebral tissue and generate the binary brain mask [30]. The ellipsoid was modeled at each voxel within the brain mask using the eddy corrected DWI scans, and the FA and MD maps were calculated by the resulting diffusion tensor eigenvalues (λ1,λ2,λ3).
Voxel-based analyses
First, FA and MD maps were normalized to MNI space with a spatial resolution of 2×2×2 mm and smoothed with Gaussian filter kernel of 8 mm. Then, voxel-based one-way ANCOVA were conducted to detect group differences of FA and MD among the three groups with age, education, and gender as the covariates. All multi-comparison corrections were performed by Gaussian random field (GRF) corrections (a voxel-level of p < 0.001; and a cluster level of p < 0.05). Furthermore, two sample t-tests were performed to investigate the differences of FA and MD between any two groups with age, education, and gender as the covariates.
The peak points of clusters showing significant differences of the FA or MD map across the three groups were recorded as the center of spherical ROIs with a radius of 10 mm by MRIcron. Then the mean FA and MD of these ROIs were calculated in the three groups respectively.
Correlation analyses
Correlation analyses were performed (respectively in svMCI+D and the svMCI-D) between neuroimaging-derived features (mean FA and MD) and clinical measures (MOCA and HAMD) by calculating the Pearson’s correlation coefficient. The results with p < 0.05 were considered as significant.
RESULTS
Demographic data and clinical measures
Demographic and clinical findings were shown in Table 1. The three groups showed no significance on age, gender, and education, but showed significant difference on MOCA and HAMD scores. The svMCI+D exhibited the heaviest cognitive impairment and the heaviest depressive symptoms indicating by MOCA and HAMD scores, respectively.
VBA results
Compared to NC, both svMCI+D and svMCI-D groups showed lower FA in the left insula (INS.L), right insula (INS.R), and the left precentral gyrus (PreCG.L). Interestingly, FA of the PreCG.L in the svMCI+D was significantly higher than that in the svMCI-D (Table 2 and Fig. 1).
Brain regions showing significant differences of FA and MD among svMCI+D, svMCI-D, and NC
L, left; R, right.
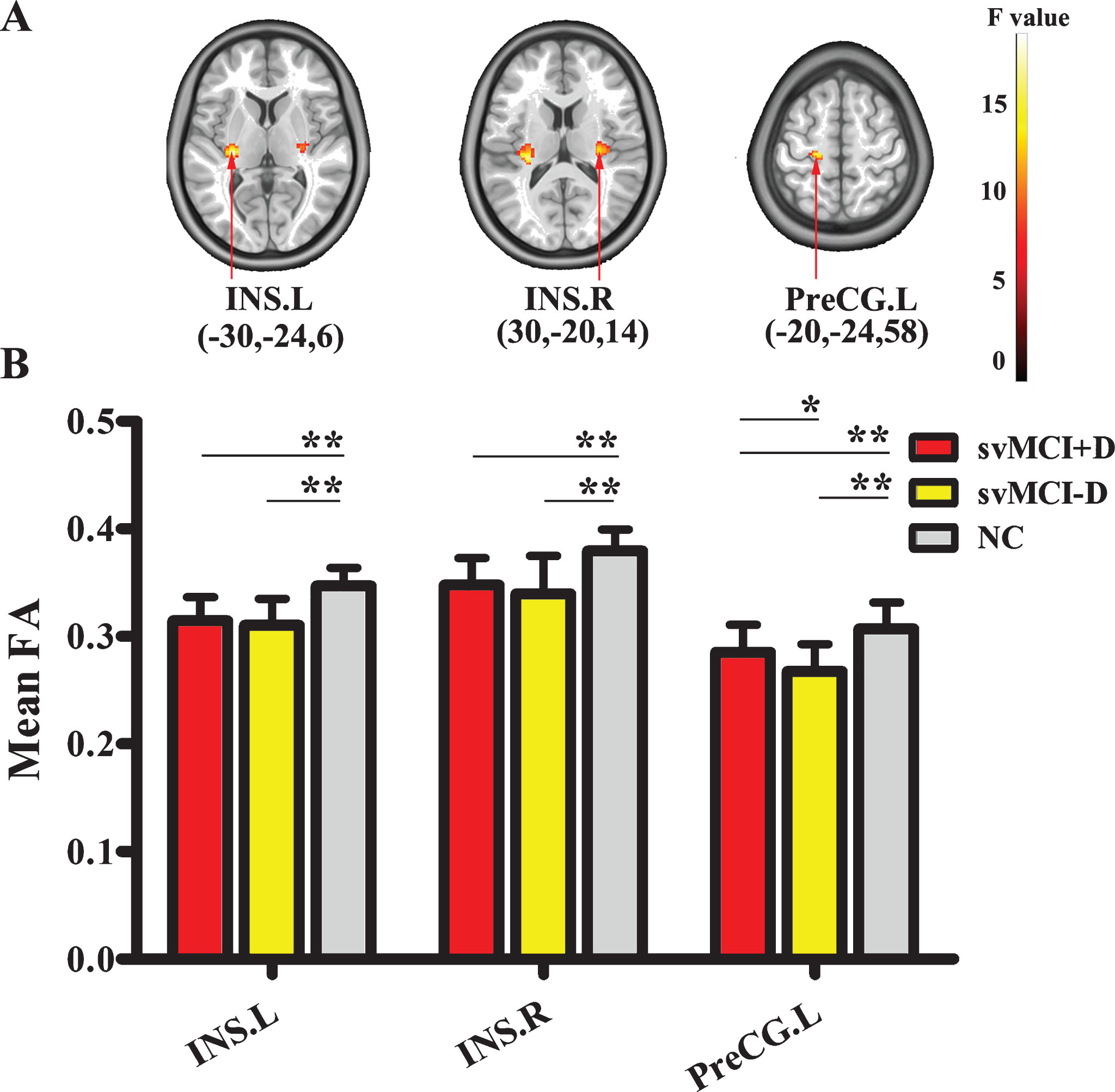
A) The results of FA among the three groups using ANOVA. B) The difference of mean FA in the INS.L, INS.R, and PreCG.L between any two groups using two sample t-tests (*p < 0.05; **p < 0.001;). INS.L, left insula; INS.R, right insula; PreCG.L, left precentral gyrus.
MD of both svMCI+D and svMCI-D groups was increased significantly compared to NC in the cerebellum VIII (CERE) (Table 3 and Fig. 2).
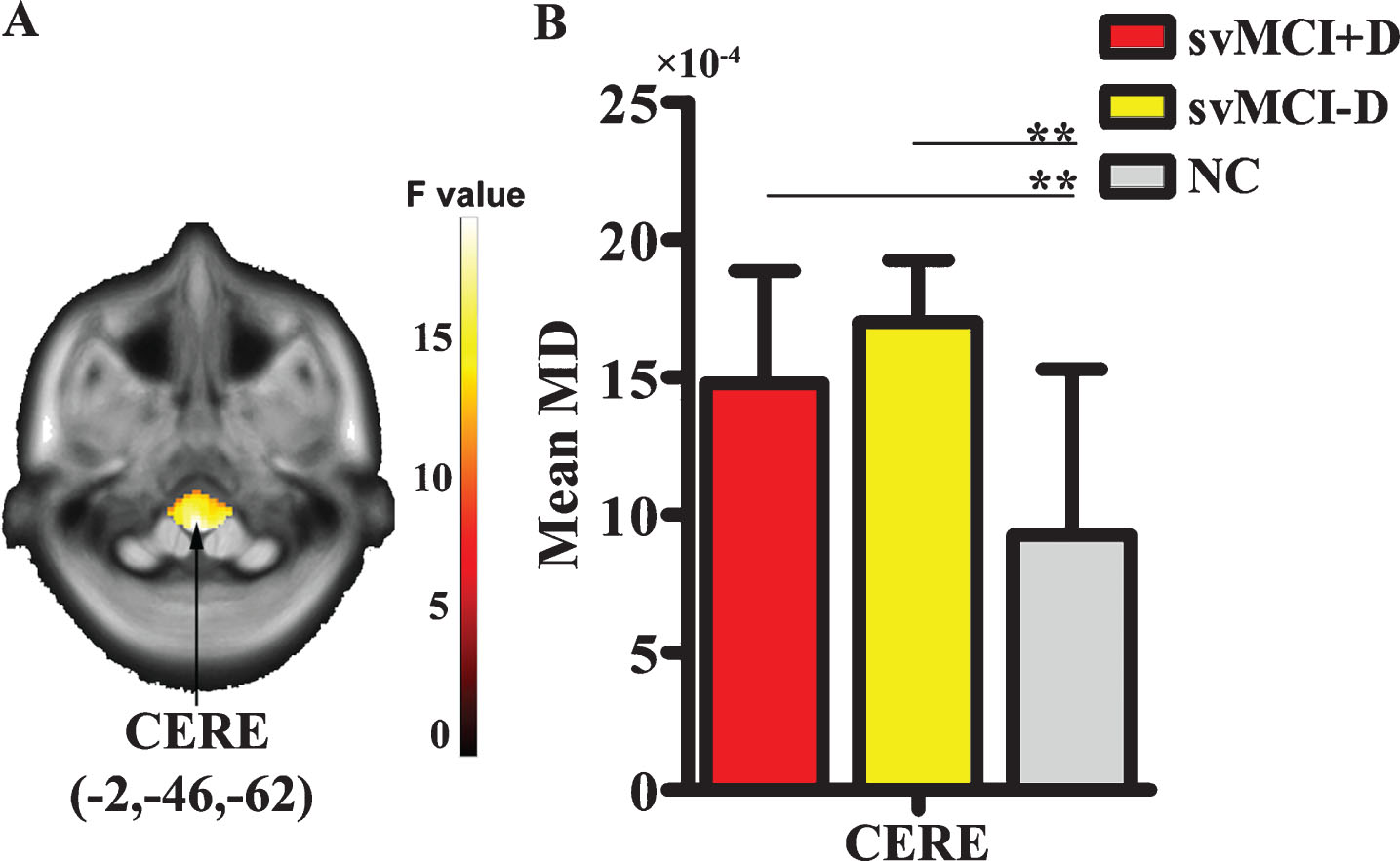
A) The results of MD among the three groups using ANOVA. B) The difference of mean MD in the CERE between any two groups using two sample t-test. CERE, cerebellum VIII.
Correlation results
A significant correlation between the HAMD score and the mean MD of CERE was identified in the svMCI+D (Fig. 3).
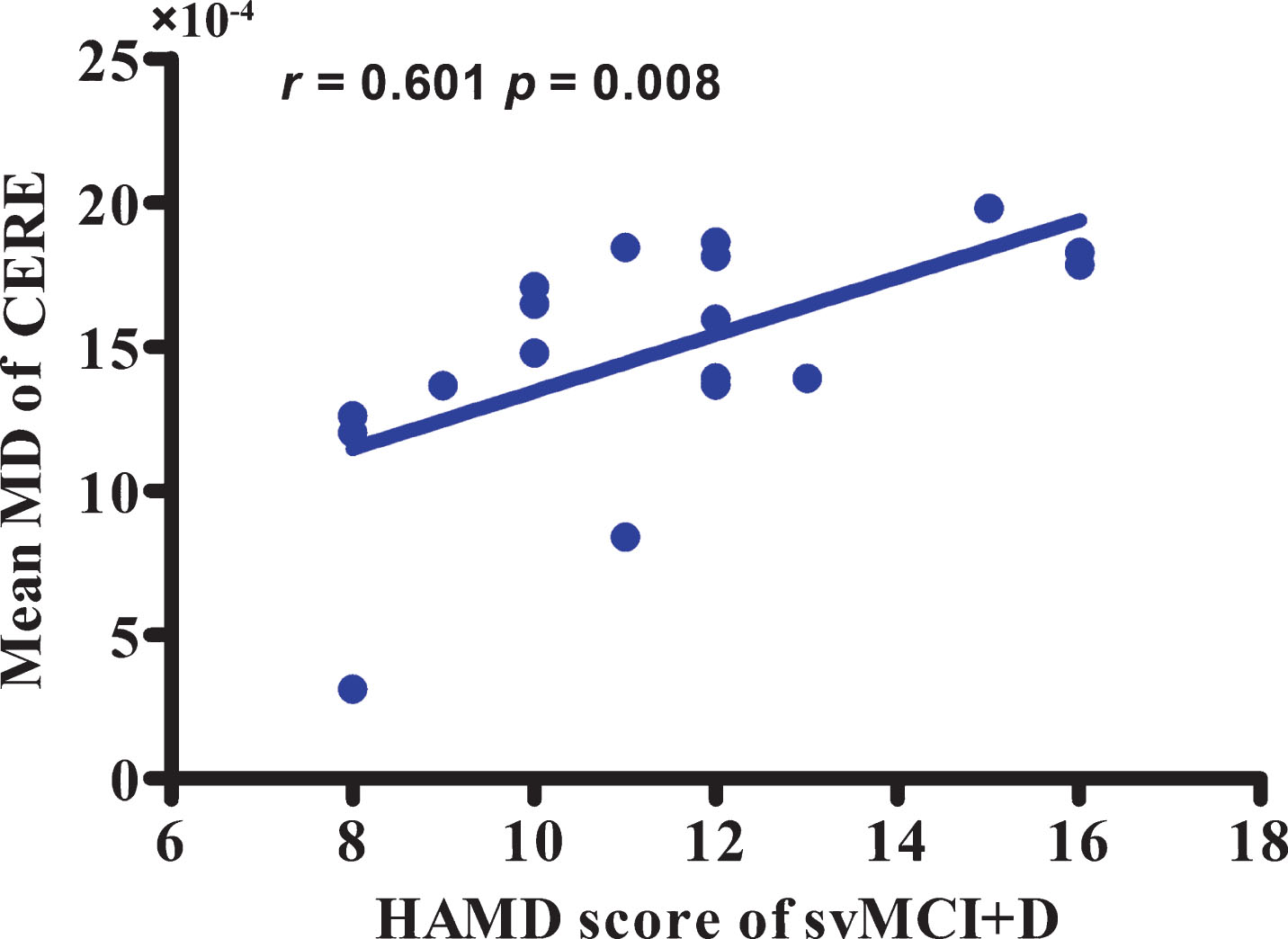
Correlation between the HAMD score of svMCI+D and the mean MD of CERE.
DISCUSSION
In the present study, we found significantly microstructural alterations among svMCI+D, svMCI-D, and NC using VBA. Compared to NC, both svMCI+D and svMCI-D groups exhibited a decreased FA in the bilateral INS and the PreCG.L, as well as an increased MD in the CERE. Moreover, it is worth noting that the svMCI+D showed higher FA than the svMCI-D in the PreCG.L.
The white matter microstructure of bilateral INS was found to be damaged in patients with svMCI with and without depressive symptoms. Numerous literatures consistently demonstrated structural and functional alterations in insula in MCI and depression patients. Structurally, MCI patients showed alterations in the gray matter and white matter of insula [31–33]. Functionally, disrupted insula network connectivity was identified in the MCI patients [31] and major depressive disorder [34–36]. Lower fALFF in insula was considered to be associated with memory performance [34]. Moreover, the INS has been reported to be implicated in a wide range of cognition domains [35]. Several studies showed significant associations between dorsal anterior insula and the higher cognitive processing [36, 37] and executive control [38]. Accumulating researches demonstrated that insula was a critical hub in the salience network [36, 39–41] and fronto-insulo-temporal network [42, 43], which indicated that insula functionally played a crucial role in social cognition [44–46]. Especially, some researchers suggested that the insula was involved in certain memory tasks and verbal component of working memory. Regional cerebral blood flow in insula was decreased as the load of memory increased [47] and bilateral insula was observed to be activated in another short-term memory study. Therefore, there is a hypothesis [48] that the cognition decline imputed to insula would likely be interpreted as diaschisis [49] or disconnection syndromes [50], which means the injury of insula would impact the performance of the connected brain region without injury. Given the evidences, the white matter damage of insula in svMCI might reflect diaschisis or disconnection syndromes to affect executive function and memory performance.
The most interesting finding of the study was that both svMCI showed decreased FA in the PreCG.L compared to NC, whereas svMCI+D showed increased FA in PreCG.L compared to svMCI-D. On the one hand, many neuroimaging studies have demonstrated the important role of the precentral gyrus in executive function [51, 52] and cognitive activities [53–55]. In addition, the decreased RSFC between the bilateral precentral gyrus and the entorhinal cortex was found in the svMCI [56]. Therefore, we suggested that the microstructure damage in the precentral gyrus were associated with cognitive impairments in svMCI. As for the increased FA in PreCG.L in the svMCI+D compared to the svMCI-D, two possible explanations were existed: compensatory effect and disease mechanism. In several previous studies [57–59], hyper-connectivity was considered a compensatory strategy to fulfill functions. Similar with our findings, hyper-activation in the left precentral gyrus was found in the major depressive disorder while performing a verbal working memory task [60, 61]. However, a recent study argued that only there is correlation between hyper-connectivity and the clinical measurements, there is compensation effect [62]. Unfortunately, no relationship between the increased FA in preCG.L and HAMD scores in the svMCI+D was found. Given these, we suggested that our findings were more likely to be associated with the disease mechanism of depression rather than compensatory effect. Moreover, the FA of preCG.L in the scMVI+D was significantly less than NC.
In addition, increased MD of cerebellum was identified in the svMCI+D. Although the cerebellum was traditionally thought to be associated with motor control, accumulating evidence supported that the cerebellum was also involves in emotion processing [63, 64]. Moreover, the abnormities of cerebellum, such as disrupted white matter [65], reduced gray matter volume [66–69], decreased regional homogeneity [70, 71], decreased activity [72], and increased functional connectivity were observed [73, 74] in depressing patients. Considering this evidence, it is reasonable to speculate that our findings of structural and functional alterations in the cerebellum might be associated with depressive symptoms in svMCI. This speculation was further supported by our correlation results, which showed significantly positively correlation between the increased MD and HAMD scores. Moreover, the disruption of CERE was concurrent with altered FA in preCG.L, which draw our attention to the cross cerebellar diaschisis (CCD) [75, 76]. CCD refers to the phenomenon that the cerebellar hypometabolism is related to the contralateral cerebral injury [77, 78], has been widely reported in previous studies after the first observation by Baron [79]. Indeed, previous research has demonstrated that the cerebellum atrophy would like to be secondary to the cerebellum injury in AD [80]. Although no significant correlation was identified due to limited samples, we cannot exclude the possibility that cerebellum is secondary alteration due to CCD. Further efforts are needed to reveal the real cause of the alteration in the CERE.
Besides all findings, three major limitations should be noted in the current study. First, the sample size was small. Second, there is no SVaD group for further analysis. A longitudinal study is needed to observe dynamic changes of the white matter related to depressive symptom from svMCI to SVaD. Last, since the vascular lesions are relatively small and distributed randomly in the whole brain as shown in the T2 FLAIR, it is extremely difficult to map all the lesions. Thus, we cannot associate our results with the distribution of vascular lesions to exclude the effects of the different damaged foci.
Conclusion
We found white matter alteration in the bilateral insula, PreCG.L, and CERE in svMCI patients with and without depressive symptoms in this study. These alterations might be associated with executive function and memory performance in the svMCI patients. Moreover, our findings of structural alterations in the cerebellum might underlie the mechanism of depressive symptoms in svMCI patients.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the Key R&D Program of Guangdong Province (No. 2018B030339001), Sanming Project of Medicine in Shenzhen (No. SZSM201612081), the National Key Research Program (No. 2017YFC1703606), Shenzhen Key Basic Research Grants (No. JCYJ20160331191401141, and KQJSCX20170731162830878), and the National Natural Science Foundation of China (Nos, 61671440, U1713215).