
Abstract
Background:
Using immunoprecipitation-mass spectrometry, we recently developed and validated a plasma composite biomarker for the assessment of amyloid-β (Aβ) levels. However, as yet, its relationship with clinical outcomes remains unclear.
Objective:
We aimed to examine the relationship between this plasma Aβ composite biomarker and cognitive function in cognitively normal older adults in two independent cohorts.
Methods:
Participants enrolled in the Australian Imaging, Biomarkers and Lifestyle (AIBL) study and the National Centre for Geriatrics and Gerontology (NCGG) study had undergone Aβ neuroimaging using positron emission tomography (PET), cognitive assessments and provided blood samples. We derived a high-performance plasma Aβ composite biomarker by immunoprecipitation with mass-spectrometry.
Results:
Both continuous and categorical measures of the plasma Aβ composite biomarker were significantly related to decline in episodic memory and executive function. The magnitude of effects of the plasma Aβ composite on episodic memory and executive function were comparable to that observed for the effects of PET Aβ levels on these same outcome measures.
Conclusion:
Several plasma Aβ biomarkers have been developed, but none have yet been applied to investigate their relationship with cognitive outcomes. Our results have important implications for the use of this biomarker in the detection of at-risk individuals.
INTRODUCTION
Alzheimer’s disease (AD) is characterized by the abnormal accumulation of amyloid-β (Aβ) and hyperphosphorylation of tau. Advances in neuroimaging and fluid biomarkers show these processes occur in cognitively normal (CN) individuals several decades before symptom onset [1]. This protracted preclinical AD period provides a unique opportunity to understand AD pathogenesis including the extent to which it may be modified by population demographics, genes, and comorbid diseases. Unfortunately, widescale assessment of Aβ in CN older adults is limited because Aβ biomarkers, measured through positron emission tomography (PET) or cerebrospinal fluid (CSF) sampling, are expensive and/or invasive.
Recently, we showed in two independent cohorts, that a plasma Aβ composite biomarker, which was generated by combining plasma ratios of APP669–711/Aβ1–42 and Aβ1–40/Aβ1–42 as measured by immunoprecipitation-mass spectrometry (IP-MS) assay, had very high areas under the receiver operating characteristic curves (AUCs) (94–96%), with an accuracy of ∼90% for the classification of high Aβ levels based on Pittsburgh Compound B (PiB) PET [2]. This plasma Aβ composite biomarker may therefore have great clinical utility for predicting Aβ levels. However, as with all putative plasma biomarkers for AD, understanding the prognostic value for clinical outcomes is also important. In CN adults, this can be ascertained by determining the nature and magnitude of relationships between plasma Aβ composite scores and cognition, measured both on a single occasion, and prospectively over disease relevant time intervals. Therefore, in CN older adults, we examined the relationship between plasma Aβ composite score, and cognition assessed both cross-sectionally and prospectively over 7.5 years.
MATERIALS AND METHODS
Participants
CN older adults (n = 156) enrolled in the Australian Imaging, Biomarkers and Lifestyle (AIBL) study underwent Aβ PET neuroimaging and provided blood samples. AIBL participants completed neuropsychological testing up to 5 timepoints, with a follow-up interval of 18-months. The AIBL study design, including recruitment methods, has been detailed previously [3]. Data from 57 CN older adults enrolled in the National Centre for Geriatrics and Gerontology (NCGG) was also analyzed [2]. NCGG participants completed neuropsychological testing up to 4 timepoints, with a follow-up interval of 12 months. Both the AIBL and NCGG studies were approved by institutional ethics committees (Human Research Ethics Committee, St Vincent’s Health, Australia; NCGG Ethics Committee Japan), and written informed consent was obtained from all participants [2, 3].
PET neuroimaging
Positron emission tomography (PET) neuroimaging for Aβ in both AIBL and NCGG has been described previously [2]. In AIBL, one of three radioligands (PiB, florbetapir, flutemetamol) was used. In NCGG, only PiB was used. Consistent with previous studies, Aβ status was classified as either low (Aβ–) or high (Aβ+). Threshold values for Aβ+ vary by radiotracer, so a linear regression transformation was applied to normalize the values called Before the Centiloid Kernel Transformation (BeCKeT) [4]. Participants with BeCKeT scores ≥1.40 at their most recent scan were classified as PET Aβ+ and those below the threshold were classified PET Aβ–.
Blood processing and plasma storage
AIBL blood processing and plasma storage procedures have been provided in detail previously [2]. Briefly, plasma was isolated from whole blood collected in Sarstedt s-monovette 7.5 ml EDTA tubes (Sarstedt) with pre-added Prostaglandin E1 (PGE1, Sapphire Bioscience) to produce a final PGE1 concentration of 33 ng ml–1 of whole blood. Processing started after bloods had equilibrated with room temperature and within 1 h of collection. Whole blood was centrifuged at 200 g for 10 min at room temperature (no deceleration) to generate a platelet-rich plasma (PRP) layer. The PRP was transferred using 3 ml transfer pipettes (Livingstone) to a new 15 ml polypropylene centrifuge tube (Greiner Bio-One CELLSTAR). Both the collection tube and 15 ml tubes were centrifuged at 800 g for 15 min at room temperature, maximum deceleration. Plasma was combined into a new 15 ml polypropylene tube and spun at 3,200 g for 30 min to remove debris. Plasma, as 250μl aliquots, was stored in 1 ml capacity NUNC 2D barcoded Bank-IT polypropylene cryovials (NUNC) and frozen immediately on dry ice before long-term storage in vapor-phase liquid nitrogen. In the NCGG study, plasma was isolated from whole blood collected in 7 ml EDTA-2Na tubes (Venoject II, TERUMO). Within 5 min of blood collection, whole blood was centrifuged at 2273 g for 5 min at room temperature. Otherwise, the blood was temporally stored on ice for up to 30 min, and then centrifuged. The plasma was immediately transferred to storage tubes (48 Jacket Tubes 2.0 ml External-Type, FCR&Bio) as 250- or 500μ l aliquots, and frozen immediately in a –80°C freezer.
Plasma Aβ measurements
The plasma samples were blindly analyzed at Koichi Tanaka Mass Spectrometry Research Laboratory (Shimadzu corporation) without any clinical or imaging information. Plasma Aβ levels were measured using IP-MS, which quantifies Aβ-related peptides of different mass in matrix-assisted laser desorption ionization-time-of-flight (MALDI-TOF) mass spectrometry after they have been isolated and enriched from abundant plasma proteins by immunoprecipitation using the specific affinity of an antibody. In detail, 250μl of plasma was mixed with an equal volume of Tris buffer containing 10 pM stable-isotope-labelled (SIL) Aβ 1–38 peptide (AnaSpec, San Jose, CA), 0.2% w/v n-dodecyl-β -d-maltoside (DDM), and 0.2% w/v n-nonyl-β -d-thiomaltoside (NTM). The stable isotope labelled (SIL) Aβ1–38 peptide was used as internal standard for normalization of signals for all Aβ related peptides in the mass spectrum. General antibody beads, prepared by coupling intact IgG monoclonal antibody 6E10 (BioLegend) directly to Dynabeads M-270 Epoxy (Thermo Fisher Scientific), were used for immunoprecipitation. The plasma Aβ-related peptides and internal standard were immunoprecipitated by incubating the antibody beads with the plasma sample for 1 h. The bound peptides were washed and eluted with glycine buffer (pH2.8) containing 0.1% w/v DDM. After the pH was adjusted to 7.4 with Tris buffer, the IP was repeated once and the bound peptides were eluted with 70% acetonitrile containing 5 mM HCl. The eluted peptides were applied on four wells of a 900μm μFocus MALDI plateTM (Hudson Surface Technology, Inc., Fort Lee, NJ) which was prespotted with the α-cyano-4-hydroxycinnamic acid (CHCA) and methanediphosphonic acid (MDPNA) in advance. Mass spectra were acquired using a MALDI-linear TOF mass spectrometer (AXIMA Performance, Shimadzu/KRATOS, Manchester, UK) equipped with a 337 nm nitrogen laser in the positive ion mode. The m/z value and signal variability in the mass spectrometer were calibrated externally with a mixture of standard peptides to improve precision of the Aβ-related peptide signal peak. The peak intensities were extracted using Mass++ software ver. 2 (Shimadzu, Kyoto, Japan). The peptide mass tolerance for quantification was set within 2.5 Da of the theoretical mass. The limit of detection was established at an S/N of 3:1. One assay produced four mass spectra and the levels of plasma Aβ-related peptides were obtained by averaging the four spectra normalized with SIL-Aβ1–38. The normalized intensity was used as plasma Aβ-related peptide levels. The quantitativity and reliability of the IP-MS assay were carefully validated by several methods as described previously [2].
Cognitive composites
Cognition was measured using the AIBL cognitive composites [5]. Briefly, scores for each AIBL neuropsychological test were standardized to the mean and standard deviation of the entire baseline sample and then averaged to provide the following composites: episodic memory (California Verbal Learning Test, Second Edition [CVLT-II] delayed recall, Logical Memory delayed recall, Rey Complex Figure Test delayed recall); executive function (Category Fluency Fruit/Furniture Switching, Letter Fluency); language (Boston Naming Test, Category Fluency Animals/Boys’ Names total score); and attention (Digit Symbol, Digit Span) [5]. The episodic memory composite in the NCGG cohort was computed by averaging standardized scores for Logical Memory total and delayed recall.
Data analysis
At first, the ratio of normalized intensity of Aβ1–42 with APP669–711, and Aβ1–40 was computed. We used Aβ1–42 as the denominator, because these ratios (APP669–711/Aβ1–42 and Aβ1–40/Aβ1–42) showed a normal distribution without requiring any transformation, whereas using Aβ1–42 as the numerator did not [2]. Then, the composite biomarker was generated by averaging the normalized scores (z-score to NCGG database) of APP669–711/Aβ1–42 and Aβ1–40/Aβ1–42 as previously described [2]. Plasma Aβ status was determined as Aβ+ if plasma Aβ composite scores were ≥0.376 and Aβ–is plasma Aβ composite scores were <0.376, consistent with our previous report [2]. More detailed information on the computation of this composite is presented in the Supplementary Material.
All statistical analyses were conducted in RStudio using R version 3.3.1. As most participants (75%) had undergone cognitive assessments prior to blood sampling, baseline (time 0) was treated as the timepoint at which the blood sample used to determined plasma Aβ status was obtained. As such, retrospective and prospective cognitive data were modelled longitudinally with linear mixed-effects models (unstructured covariance matrix), and time and participant specified as random factors. All continuous variables were standardized to the baseline mean and standard deviation of the entire group. Group mean slopes were extracted, and effect size of difference (Cohen’s d) between groups were computed. As this was an exploratory investigation in a novel area of biomarker research in which important clinical outcomes are expected, a significance level was set at an uncorrected p < 0.05, in order to balance the risk of false positive findings against the identification of potentially important relationships. Additionally, effect sizes are used to guide interpretation about the meaningfulness of statistical tests and comparisons, and effect sizes <0.2 were classified as trivial and not interpreted regardless of statistical significance [6]. To replicate the effects of plasma Aβ on longitudinal cognitive function, we repeated all longitudinal analyses and derived group mean slopes for NCGG CNs for the measure of episodic memory. All β estimates reported have been standardized.
RESULTS
Baseline demographic, clinical, and cognitive characteristics
Clinical and demographic characteristics were equivalent across groups defined according to their plasma Aβ composite score in both the AIBL and NCGG cohorts (Table 1). Consistent with previous work in this cohort [2], a greater proportion of individuals were classified as Aβ+ using PET in the plasma Aβ+ group. The plasma Aβ+ group also had a higher proportion of APOE ɛ4 carriers. Overall, demographic and clinical characteristics of the AIBL and NCGG CN cohorts were equivalent (Table 1).
Baseline demographic and clinical characteristics of the AIBL and NCGG cohorts
Baseline demographic and clinical characteristics of the AIBL and NCGG cohorts
*Note: time between assessments in AIBL is 18 months, and in NCGG is 12 months.
With cognition considered at the baseline visit, cognitive performance was not significantly worse in the plasma Aβ+ group when compared to the plasma Aβ–group, although the magnitude of difference between groups for the episodic memory composite was moderate (Table 2). The PET Aβ+ group performed significantly worse than the PET Aβ–group only on the episodic memory composite, and the magnitude of this impairment was also moderate (Table 3). With the plasma Aβ composite score and PET Aβ BeCKeT score considered as continuous measures, significant relationships were only observed between BeCKeT scores and episodic memory performance at baseline (Tables 2 and 3).
Baseline and longitudinal effects of the plasma composite biomarker on each cognitive composite in the AIBL cohort
Baseline and longitudinal effects of the plasma composite biomarker on each cognitive composite in the AIBL cohort
*Note: all β estimates reported have been standardized.
Baseline and longitudinal effects of PET Aβ levels (BeCKeT) on each cognitive composite in the AIBL cohort
*Note: all β estimates reported have been standardized.
When considered longitudinally, significant plasma Aβ group×time interactions were observed for episodic memory and executive function (Table 2; Fig. 1). No significant interactions between plasma Aβ group and time were observed for language or attention. The magnitude of difference between plasma Aβ–and plasma Aβ+ groups was moderate for both episodic memory (d = 0.54) and executive function (d = 0.51), and small for language (d = 0.20) and attention (d = 0.07). With plasma Aβ composite score considered as a continuous measure, higher composite scores were associated significantly with faster decline in episodic memory and executive function (Table 2), but not with change in language or attention. Similarly, continuous scores of APP669–711/Aβ1–42 and Aβ1–40/Aβ1–42 were significantly associated with faster decline in episodic memory (β(SE) = –0.073(0.28), p = 0.007 and β(SE) = –0.78(0.27), p = 0.005 respectively) and executive function (β(SE) = –0.061(0.025), p = 0.010 and β(SE) = –0.095(0.024), p < 0.001 respectively), but not language or attention (ps > 0.20). These analyses were repeated with sex and premorbid intelligence as covariates, and our results did not change significantly (Supplementary Table 1).
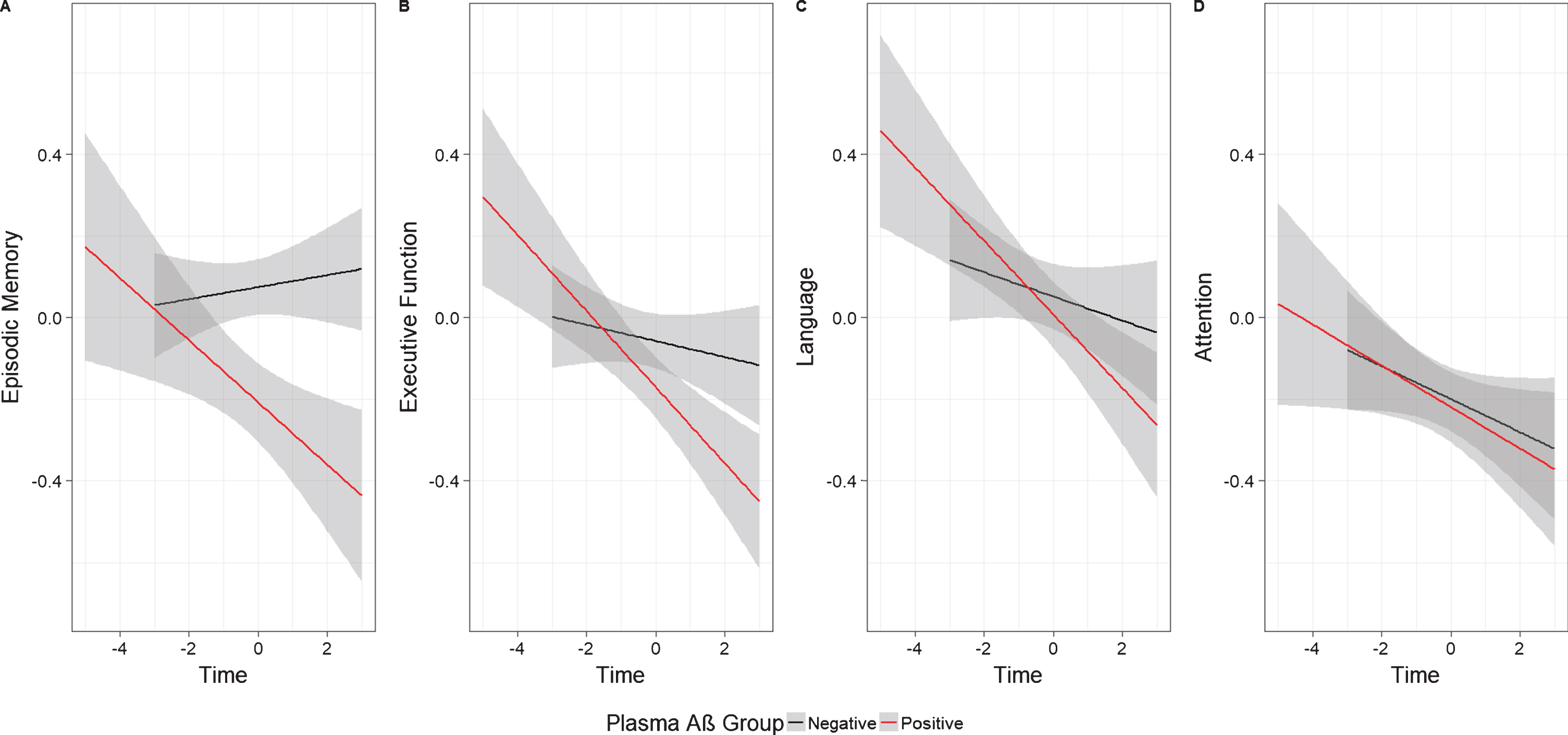
Plasma Aβ+ is associated with faster decline in (A) episodic memory, and (B) executive function, but not (C) language or (D) attention (shading indicates 95% confidence intervals).
As has been observed previously in AIBL, statistically significant PET Aβ group×time interactions were observed for episodic memory, executive function, and language (Table 3, Fig. 2). The magnitude of difference between PET Aβ–and PET Aβ+ groups was moderate for both episodic memory (d = 0.47), executive function (d = 0.48), and language (d = 0.63), but small for attention (d = 0.18). With PET Aβ BeCKeT scores considered as a continuous measure, higher scores were associated significantly with faster decline in episodic memory, executive function and language, but not with attention (Table 3).

PET Aβ+ is associated with faster decline in (A) episodic memory, (B) executive function, and (C) language, but not (D) attention (shading indicates 95% confidence intervals).
In the NCGG cohort, the plasma Aβ+ group showed a faster rate of decline in episodic memory compared to the plasma Aβ–group, β(SE) = –0.208(0.097), p = 0.032, and the magnitude of this effect was, by convention, moderate (d = 0.62). With plasma Aβ composite score considered as a continuous measure, higher scores were also associated significantly associated with faster memory decline, β(SE) = –0.107(0.038), p = 0.006.
DISCUSSION
An elevated plasma Aβ composite score, measured in CN older adults using IP-MS, was associated with cognitive dysfunction. At the baseline assessment, individuals defined as Aβ+ based on either plasma Aβ composite scores or PET Aβ BeCKeT scores showed moderately worse episodic memory performance than matched Aβ–individuals; however, as has been shown in meta-analyses of the effects of Aβ+ classified from PET or CSF sampling [7], this impairment was small in magnitude. Longitudinal models in both the AIBL and NCGG cohorts showed that higher plasma Aβ composite scores were moderately related to accelerated decline in both episodic memory and executive function (Fig. 1). In the AIBL sample, plasma Aβ+ was not associated with changes in language or attention (Fig. 1). These cognitive domains were not assessed in the NCGG cohort. The magnitudes of decline in memory and executive function in plasma Aβ+ CN older adults were consistent with those observed when classification of Aβ+ was based on PET BeCKeT scores (Fig. 2), and also equivalent to that observed in previous observations of decline in episodic memory and executive function in other groups where Aβ+ has been classified on the basis of PET or CSF [5, 8]. The specificity of decline in memory and executive function in Aβ+ CNs is consistent with the predilection of very early AD pathologic processes for medial temporal lobe structures [9], upon which such cognition depends.
The accurate measurement of plasma Aβ1–40 and Aβ1–42 levels using conventional ELISA-based techniques, which employ only antibody affinity, has been limited because the concentration of total protein in plasma is ∼100 times higher, and that of Aβ is ∼50 times lower than that in CSF [10]. By using IP-MS, we were able to distinguish accurately the mass of each Aβ peptide fragment in addition to enrichment through immunoprecipitation [2]. Other plasma Aβ assays have been developed that predict cerebral Aβ levels, for example, through stable isotope labeling kinetics [11], immunomagnetic reduction [12], immuno-infrared-sensor labelling [13], immunoprecipitation and liquid chromatography-mass spectrometry [14], and measuring free and total Aβ fractions in plasma [15]. The sensitivity and specificity of these assays for cerebral Aβ range from 0.70–1.00 and 0.69–0.92, suggesting some good clinical utility. However, as yet, none of these plasma Aβ markers have been applied to investigate the clinical sequelae of preclinical AD, a stage where such assays may ultimately be most useful.
The current finding that Aβ+ classified using IP-MS is related to decline in those aspects of cognition that are central to the early symptomatic manifestation of AD suggests strongly that this plasma Aβ composite marker will provide a useful prognostic marker for clinical outcomes and so formal studies of these characteristics are warranted. It also demonstrates the potential for its use in the identification of at-risk individuals for enrollment into prevention trials of AD, and a strong foundation for determining the extent to which this plasma Aβ composite marker can provide an index of changes in Aβ levels as disease progresses, or treatment with Aβ lowering agents.
Footnotes
ACKNOWLEDGMENTS
The AIBL study would like to thank all participants of the study and the clinicians who referred participants. The AIBL study (![]() ) is a consortium between Austin Health, CSIRO, Edith Cowan University and the Florey Institute, The University of Melbourne. Partial financial support was provided by the Alzheimer’s Association (US), the Alzheimer’s Drug Discovery Foundation, an anonymous foundation, the Cooperative Research Centre for Mental Health, CSIRO Science and Industry Endowment Fund, the Dementia Collaborative Research Centres, the Victorian Government Operational Infrastructure Support program, the McCusker Alzheimer’s Research Foundation, the National Health and Medical Research Council, and the Yulgilbar Foundation. Funding sources had no role in study design, data collection, data analyses or data interpretation. The NCGG study group thank all participants of the study, clinicians who referred patients, all the staff who supported the MULNIAD project, and the NCGG Biobank members for the management of plasma samples. The NCGG study was supported by The Research Funding for Longevity Sciences (25–24 and 26–30) from the National Center for Geriatrics and Gerontology, and partially supported by Research and Development Grants for Dementia from the Japan Agency for Medical Research and Development, AMED. This study is registered under UMIN ID: 000016144.
) is a consortium between Austin Health, CSIRO, Edith Cowan University and the Florey Institute, The University of Melbourne. Partial financial support was provided by the Alzheimer’s Association (US), the Alzheimer’s Drug Discovery Foundation, an anonymous foundation, the Cooperative Research Centre for Mental Health, CSIRO Science and Industry Endowment Fund, the Dementia Collaborative Research Centres, the Victorian Government Operational Infrastructure Support program, the McCusker Alzheimer’s Research Foundation, the National Health and Medical Research Council, and the Yulgilbar Foundation. Funding sources had no role in study design, data collection, data analyses or data interpretation. The NCGG study group thank all participants of the study, clinicians who referred patients, all the staff who supported the MULNIAD project, and the NCGG Biobank members for the management of plasma samples. The NCGG study was supported by The Research Funding for Longevity Sciences (25–24 and 26–30) from the National Center for Geriatrics and Gerontology, and partially supported by Research and Development Grants for Dementia from the Japan Agency for Medical Research and Development, AMED. This study is registered under UMIN ID: 000016144.
YY Lim is supported by a Career Development Fellowship from the National Health and Medical Research Council (NHMRC) (GNT1162645).