
Abstract
Background:
Patients with Alzheimer’s disease (AD) experience various stressors that negatively impact well-being. Most studies have, however, small effect size and are limited by the experiences of severe patients. Therefore, we conducted a single-blind, randomized controlled trial, which has included patients at different stages.
Objective:
The stressor-oriented multicomponent program was designed as an intervention for AD patients to enhance well-being.
Methods:
Patients were randomly assigned to control or SOUL-P conditions according to disease severity. The SOUL-P group received 15 intensive sessions over 6 months and 6 maintenance sessions over a 6-month follow-up by a multidisciplinary team comprising psychologists, occupational therapists, and community nurses. The control group received a similar number of sessions by community nurses. Stress-related outcomes (primary stressors and well-being outcomes) were obtained from in-person baseline and follow-up interviews conducted at 6- and 12-months post-baseline. A treatment compliance survey was conducted at the intervention endpoint for patients.
Results:
Of the 863 patients screened, 218 (25.3%) were eligible. At 6 months, compared to controls, SOUL-P patients had improved quality of life (QoL) (p < 0.001; Cohen d = 0.56), depression (p = 0.020; Cohen d = –0.33), neurobehavioral symptoms (p = 0.034; Cohen d = –0.30), perceived stress (p = 0.030; Cohen d = –0.31), and family conflict (p = 0.026; Cohen d = –0.32). QoL, depression, perceived stress, and family conflict were still significantly different at 12 months. Most patients were satisfied with SOUL-P, while caregivers in the SOUL-P group reported overloading tasks.
Conclusion:
SOUL-P may reduce perceived stress and improve psychological outcomes in AD patients. Stressor-based interventions, patient-oriented goals, and a multidisciplinary team are essential features for a successful SOUL-P.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is the most common cause of dementia. AD affects over 33.9 million individuals worldwide [1] and 5.69 million individuals in China [2]. Reports indicate that 96% of people with dementia in China are cared at home [3]. There is a well-established negative association between stress and quality of life (QoL) in AD patients [4]. Stress-related emotional responses (e.g., anxiety and/or depression), psychological reactions (e.g., toxic cortisol levels) [5], and behavioral reactions (e.g., pacing around the house) may contribute to cognitive decline and AD progression [6], those responses also influenced individual’s well-being [7]. As Aftab and Jeste demonstrated [8], met psychological needs, remaining in comfortable relationships, and supported decision-making, which influenced emotion and QoL, are critical domains for the successful well-being of AD patients. As such, understanding the stress process in these patients and managing its effects on well-being outcomes remains a priority.
According to the main assumption of the stress process model (SPM) [9], primary stressors, characteristics of impairment and negative symptoms of patients with dementia in different background and context, have a direct or indirect impact on “secondary strains,” (e.g., family role strain) and downstream well-being outcomes such as anxiety, depression, QoL, and physiological reactions. Work by previous studies underscores that psychosocial interventions can have a positive impact on particularly stressors associated with a dementing illness. These studies have targeted cognitive symptoms [10], independence [11], difficult behavioral and psychiatric symptoms of dementia (BPSD) [12], and supportive services [13]. The ANSWER program used SPM to relieve caregivers’ stress. Compared to controls, intervention caregivers showed decreased care-related strain as indicated by lower emotional health strain, dyadic relationship strain, role captivity, and fewer symptoms of depression and anxiety [14]. Despite promising benefits in intervention, few studies have drawn upon global stressors for patients with dementia and the complex associations among stressors and related well-being outcomes have hardly been explored.
Limited studies outlined the biopsychosocial stressors that commence with symptom onset and proliferate over time or the relationships among stressors and outcomes experienced by people living with dementia until Judge [9] proposed the SPM for individuals with dementia. This conceptual model allowed researchers to gain valuable insight into the dementing experience from onset to later stages from the perspectives of patients, rather than relying on caregiver or other proxy reports [9]. The SPM includes five domains: background and context characteristics, primary stressors (including cognitive status, functional status, behavior problems, role captivity, perceived distress, and perceived dependency), secondary strains, and well-being outcomes (see Supplementary Material 1).
The Stressor-Oriented mUlticomponent intervention and the weLl-being of Patients with Alzheimer’s disease (SOUL-P) program was developed based on the SPM in dementing illness. The SOUL-P is a mitigating approach anchoring the six primary stressors described above, reducing stress, and maximizing the well-being of AD patients. This intervention is intended to support patients at different stages who report at least one predictor of stress-related psychosocial outcomes [15]. Occupational therapists, psychologists, and community nurses jointly evaluate the primary stressors and degree of negative symptoms. Participants work with a multi-disciplinary team (MDT) to identify personally relevant goals relating to their stressors. The MDT determines the intervention plan, including tasks or activities, and treatment dose according to the goal. Participants work with the MDT to implement this plan over several sessions conducted in the home setting. Progress toward attaining the identified goals is evaluated through self-reported questionnaires and stress-related physiological indicators.
Given the limited research addressing SPM and care interventions for homebound patients, the potential of the SPM framework to enrich patients’ health needs to be investigated. This paper presents the protocol of SOUL-P and related randomized controlled trial, aiming to explore the acceptability and effectiveness of the program to AD patients. We hypothesized that this multi-domain stressor-related intervention would improve the general well-being of AD patients. The changes in depression, anxiety, QoL, and physiological reactions, as indicators of well-being outcomes, should be correlated with the improvements of stressors.
METHODS
Design
This was a randomized, single-blind controlled trial. After undergoing face-to-face baseline assessment and receiving a resource packet, 218 participants were randomly assigned to the SOUL-P or control groups. Outcomes were assessed at 6- and 12-months post randomization. The trial was conducted in nine communities in Chongqing city. Ethical approval was given by the hospital Ethics Committee, and the study was registered in the Chinese Clinical Trial Registry. Participants and study partners provided written informed consent.
Participants
Participants were recruited from the community healthcare centers in Chongqing city. Participants were contacted first by official accounts of WeChat, poster, mailings, and word of mouth, and then by a follow-up phone call to explain the project, determine interest, and screen for eligibility. The screening process for these community-dwelling participants is depicted in Fig. 1.
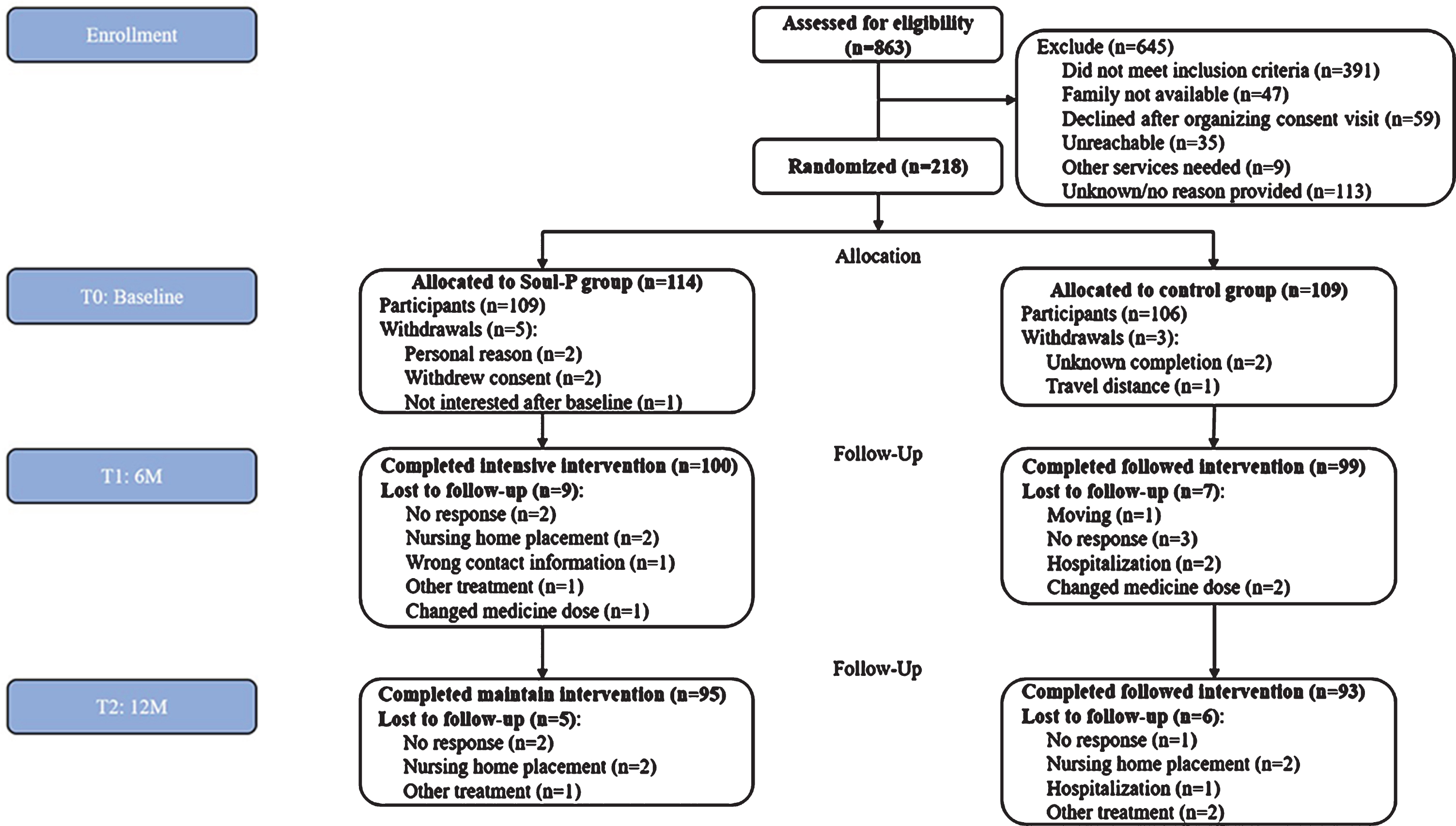
Consort Flow Diagram.
Inclusion criteria were as follows: 1) aged 65 years and older; 2) formal International Classification of Disease, 10th revision (ICD-10) diagnosis of AD without any record of other types of dementia (if not available, the diagnosis was confirmed by a neurologist); 3) having endorsed at least one of five negative experiences associated with psychosocial outcomes (embarrassment about memory loss, physical health strain, relationship strain, lower perceived instrumental activities of daily living, difficulty with and lower self-efficacy perception) [16]; 4) community-dwelling with no plans for placement in long term care within 1 year; 5) ability to see and hear well enough to participate in the group; 6) having a family member, who had at least 1 year caring or had at least 4 days or 7 hours per week contact; 7) consent to study participation; and 8) patients receiving any medication were allowed in this study; however, cholinesterase inhibitors or psychotropic drugs were required to have been on medication for a minimum period of 90 days before baseline [17].
Patients were excluded if: 1) they had a terminal illness with a life expectancy of less than 12 months or more than three acute hospitalizations in the past year; 2) were involved in-home rehabilitation (nursing, psychotherapy, and occupational therapy) or another trial; and if 3) their medicine dose was changed within 6 weeks on cholinesterase inhibitors (e.g., donepezil, galantamine, rivastigmine) or psychotropic drugs (e.g., tricyclic antidepressants, tiprazolam, wuling capsule). The cholinergic system is important for neuronal function in memory, learning, and other essential aspects of cognition, and cholinesterase inhibitors may induce bias results [18]. Moreover, antipsychotic medication leads to reduced cortisol concentrations in patients and in healthy controls [19]; patients with a 4) total failure of communication or Mini-Mental State Examination (MMSE) score ≤3 [20] were also excluded.
Sample size
Power calculation was based on previous research [21] showing a moderate effect size of improvement in QoL and analyzed by PASS v.11 (Power Analysis and Sample Size software, NCSS LLC Inc., Kaysville, UT, USA). To achieve 80% power to detect a medium effect size of 0.5 with alpha 0.05 in primary and secondary outcomes for a two-sample comparison of means, 172 patients and their caregivers were required to complete the trial. Allowing for an estimated attrition of 20%, we required randomization of 216 patients with dementia.
Randomization and masking
AD patients were stratified by the Clinical Dementia Rating scale (mild, moderate, or severe group) [22] and a random number for each group between 10–99 was generated at random.org/integer-sets/The indicator for randomization was the remainder after the obtained number was divided by two (0 = intervention group, 1 = control group). The blocking numbers were developed by the program statistician and blinded to others. Each patient was randomized by the project director after providing a written informed consent. Group allocation was not actively disclosed to participants, and they were advised not to discuss the intervention during testing sessions.
Intervention
The SOUL-P protocol is described in Supplementary Material 2. In this multicomponent intervention, 1) all SOUL-P patients were exposed to each treatment element: assessments of six stressors, four outcome indexes, and physical environment; 2) interactive identification of goals was performed by joint discussion of possible retraining and solutions, which were based on six primary stressors. The tailored intervention consisted of up to 15 1 h sessions over a 6-month period with the MDT (six home visits by an occupational therapist, six home visits with psychological therapist, and three home visits with community nurse), followed by six 1 h maintenance sessions over the subsequent 6 months conducted in the participant’s home by the MDT. MDT members were required to have dementia-related care experience. SOUL-P therapists received a 2-week additional training in the intervention method. Treatment fidelity was monitored through a twice-monthly supervision and a work checklist (delivery content and duration) submitted by the interventionists, both of which were reviewed by investigators. Data collection and the administration of the intervention were performed by the same therapist.
The primary goal of the control group was to provide non-directive usual support for patients by other trained community nurses (not SOUL-P members). This control group also received 15 home visits (1 h each) over the subsequent 6 months and six home visits to match the social engagement received by the SOUL-P group. The role of the nurses was to provide unconditional healthcare to patients and caregivers and to establish a supportive relationship. Nurses provided basic healthcare, such as management of pain and medication, sleep and diet advice, chronic disease monitoring, assessment of home safety, and salivary collection, as per community visits. Healthcare fidelity was monitored through twice-monthly supervision and a work checklist (delivery content and duration) submitted by community nurses, both of which were reviewed by the investigators. The community nurses did not communicate with any other staff involved in the SOUL-P trial.
Outcomes
Outcome measurements
A detailed description of outcomes measurements is provided in Supplementary Material 3. We collected information from all patients at baseline, post-intervention, and at 6 months. The process of assessment was conducted by therapists trained in techniques with the purpose of promoting the capacity of individuals with cognitive decline to provide responses. Measures included: the Quality of Life in Alzheimer’s Disease (QoL-AD) survey [23], Geriatric Depression Scale (GDS) [24], Rating Anxiety in Dementia (RAID) [25], MMSE [26], Direct Assessment of Functional Status (DAFS) [27], Neuropsychiatric Inventory (NPI) [28], Family Environment Scale (FES) [29], and Perceived Stress Scale (PSS) [30]. All self-reported questionnaires, except for the NPI, were performed via a structured interview by therapists. We adopted several methods to improve the efficiency of data collection such as increasing font size, using graphics instead of text, using dichotomous answers (yes/no), and performing scenario simulation.
Saliva collection
Saliva samples were collected using the Salivette device (Pangtong biotechnology co. LTD, Chongq-ing, China). The first sample was collected from participants by community nurses in the evening before the clinic visit, prior to going to sleep. The second sample was to be collected in the morning 45 min after awakening and the third sample at 2 p.m. Participants were instructed not to brush their teeth before saliva sampling, to allow at least 30 min to pass after eating or drinking before taking the evening sample, and to refrain from eating and drinking until after the morning sample was collected [31]. Salivary cortisol was analyzed using an enzyme-linked immunosorbent assay kit (Jianglai biotechnology co. LTD, Shanghai, China). Intra-assay and inter-assay variability were <9% and 11%, respectively. The lower detection limit was 0.1 nmol/L for a 50μL salivary sample, and the detection range was 1.5–48 nmol/L.
Self-report survey responses in patients and caregivers (SOUL-P versus Control group)
At 12 months, we evaluated study compliance of both groups using a self-made survey comprising two parts: one directed to patients, including overall benefits, completion rate, perceived independence, confidence to coping with problems, lessened distress, intimacy, better life; and one directed to caregivers, including overloading of tasks and time consumption. Items were answered by dichotomous answers (yes/no) for both patients and caregivers.
Statistical analysis
Statistical analysis was performed by IBM SPSS v.23 (SPSS Inc., Chicago, IL, USA) with a significance level set at p < 0.05. All analyses were two-sided. Analyses included all participants and baseline, 6-month, and 12-month data. Descriptive statistics were calculated for each group. T-tests or χ2 tests were conducted to determine between-group differences at baseline All data were analyzed according to the intention-to-treat principle, and the outcome indicators were analyzed in the full analysis set (FAS) and per protocol set (PPS). A mixed linear model procedure was selected to accommodate for multiple repeated measures. Bonferroni post-hoc adjustments (5% significance level) were used to test differences among T0, T1, and T3. Cohen’s d was used to measure the effect size using the t-values of two independent samples, and was interpreted as small (0.2 to 0.5), medium (0.5 to 0.8), or large (0.8) [32].
RESULTS
Demographic characteristics
Of the 863 screened AD patients, 218 (25.3%) were eligible and were willing to participate in the study. Patients were randomized to either the SOUL-P group (n = 109) or control group (n = 106) (Fig. 1). Of the 109 participants in the SOUL-P group, 44 (40.4%) were at the mild stage, 37 (33.9%) at the moderate, and 28 (25.7%) were at the severe stage; their mean (SD) MMSE score was 13.9 (5.8). Of the 106 participants in the control group, 38 (35.8%) were at the mild stage, 37 (34.9%) at the moderate stage, and 31 (29.2%) were at the severe stage, while their mean (SD) MMSE score was 15.0 (6.4). Comparison of baseline demographic and clinical characteristics between the SOUL-P and control group did not reveal any significant differences (Table 1). Study attrition was low, with 16 patients (8.0%) lost by 6 months and 11 (5.6%) not completing the follow-up at 12 months.
Demographic Characteristics of AD Patients
CDR, Clinical Dementia Rating scale. M (SD), mean (standard deviation).
6-month outcomes
No significant differences were detected between AD patients in the SOUL-P and control conditions for measures completed (Table 2), including anxiety, MMSE, DAFS, cohesion, expressive and family relationship. Significant improvements were observed in QoL (DIF 1.573; 95% confidence interval [CI], 0.793–2.352; p < 0.001; Cohen d = 0.56) and depression (DIF, –0.955; 95% confidence interval [CI], –1.757– –0.154; p = 0.020; Cohen d = –0.30) for SOUL-P patients (baseline to 6 months) compared with those of the control group patients, representing a small to medium effect. Improvements were seen mostly in NPI (DIF, –2.785; 95% confidence interval [CI], –5.359– –0.211; p = 0.034; Cohen d = –0.30), PSS (DIF, –0.461; 95% confidence interval [CI], –0.878– –0.044; p = 0.030; Cohen d = –0.31), and family conflict (DIF, –0.313; 95% confidence interval [CI], –0.588– –0.038; p = 0.026; Cohen d = –0.32), representing a small to large effect. SOUL-P patients showed improvement in salivary cortisol compared to that of controls, but this was not statistically significant.
Outcomes of SOUL-P and Control Group Patients among Baseline, 6-Month, and 12-Month (PPS)
Qol-AD, the Quality of Life in Alzheimer’s Disease; GDS, the Geriatric Depression Scale; RAID, Rating Anxiety in Dementia; MMSE, Mini-Mental State Examination; DAFS, the Direct Assessment of Functional Status; NPI, The Neuropsychiatric Inventory–Questionnaire; PSS, Perceived Stress Scale; Conflict, Cohesion, and Expressive were subitems in Family Environment Scale (FES), which means Family Relationship.
12-month outcomes
QoL-AD (DIF, 2.185; 95% confidence interval [CI], 1.349–3.022; p < 0.001; Cohen d = 0.75), depression (DIF, –1.234; 95% confidence interval [CI], –2.038–0.430; p = 0.003; Cohen d = –0.44), PSS (DIF, –0.840; 95% confidence interval [CI], –1.202– –0.479; p < 0.001; Cohen d = –0.67), family relationship (DIF, –1.001; 95% confidence interval [CI], –1.677– –0.325; p = 0.004; Cohen d = –0.43), and family conflict (DIF, –0.422; 95% confidence interval [CI], –0.715– –0.130; p = 0.005; Cohen d = –0.41) were significantly different between SOUL-P and control groups at 12 months, representing a medium to large effect (Table 2). After 12 months of intervention, patients and caregivers reported compliance to the intervention in both groups (Fig. 2). Compared with patients in the control group, those in the SOUL-P group reported more perceived independence (χ2 = 2.88, p = 0.09), lessened distress (χ2 = 3.51, p = 0.06), better intimacy (χ2 = 4.46, p = 0.04), and a better life (χ2 = 10.01, p = 0.002). Additionally, compared to the caregivers in the control condition, those in the SOUL-P group were more likely to report overloading tasks (χ2 = 15.32, p < 0.001). The results in the FAS for intergroup comparisons are provided in Supplementary Material 4.
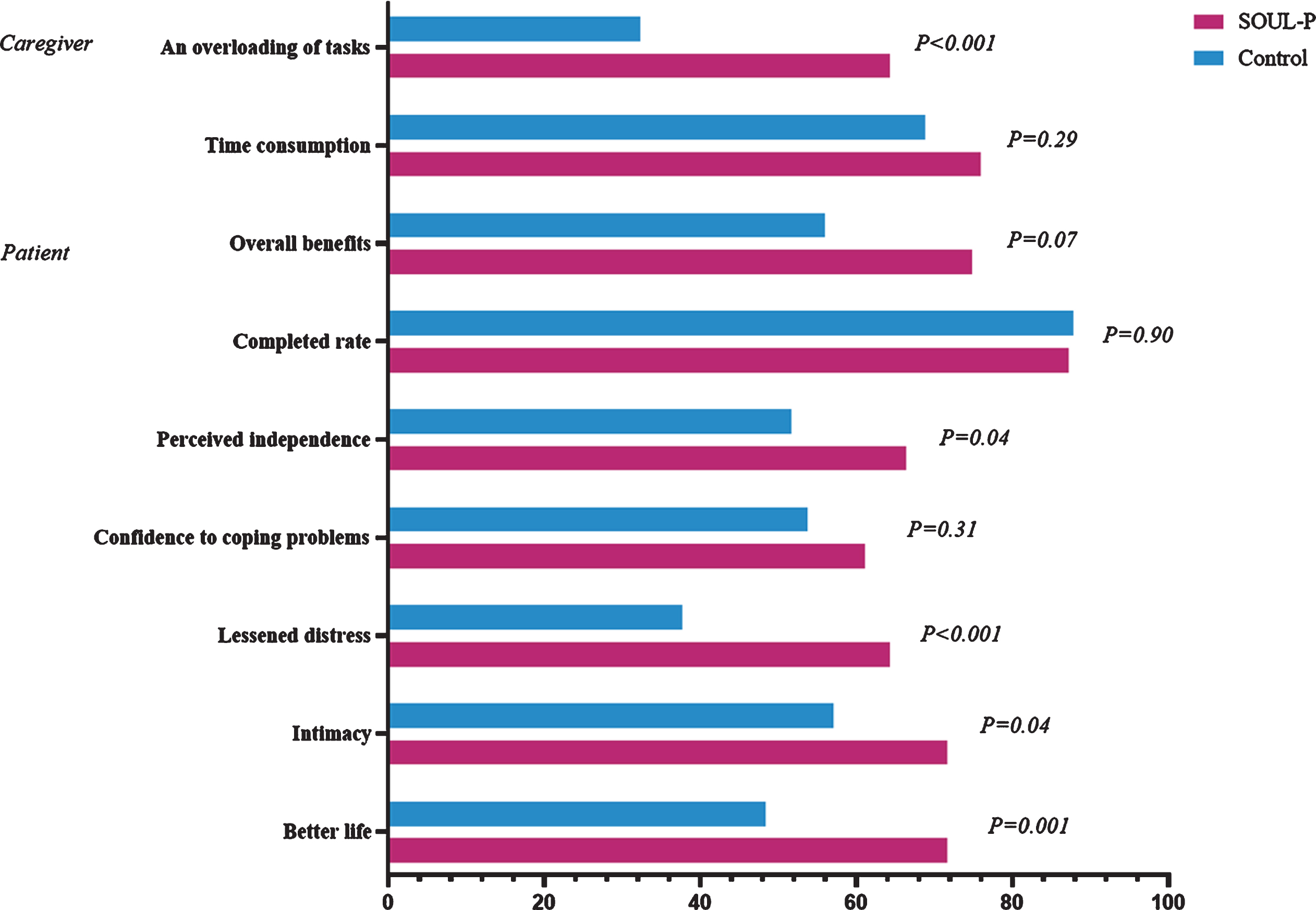
Self-report Survey Responses by SOUL-P and Control Group Participants. Percentages indicate those responding “yes” for study compliance items for caregiver or patient items. Percentage Responding “Yes”.
Comparison of pre-post scores for outcomes in the SOUL-P group
A pre-post-test was performed to investigate the efficacy of SOUL-P for patients. QoL-AD (DIF, 0.925; 95% CI, 0.045–1.805; p = 0.036; Cohen d =0.34), depression (DIF, –1.209; 95% CI, –2.200 –0.218; p = 0.011; Cohen d = –0.43), PSS (DIF, –1.057; 95% CI, –1.578– –0.537; p < 0.001; Cohen d = 0.68), and family conflict (DIF, –0.495; 95% CI, –0.812– –0.177; p < 0.001; Cohen d = 0.54) were significantly different after 6 months. Compared with baseline data, significant improvements were observed in QoL-AD (DIF, 2.004; 95% CI, 1.088–2.920; p < 0.001; Cohen d = 0.75), depression (DIF, –1.400; 95% CI, –2.391– –0.409; p = 0.002; Cohen d = 0.51), PSS (DIF, –1.624; 95% CI, –2.112– –1.135; p < 0.001; Cohen d = 1.13), and family conflict (DIF, –0.368; 95% CI, –0.696– –0.040; p = 0.022; Cohen d = 0.38) after 12 months (Table 3). The results of in the FAS for intragroup comparison are presented in Supplementary Material 5.
Outcomes for SOUL-P Patients before and after Intervention Implementation (PPS)
Qol-AD, the Quality of Life in Alzheimer’s Disease; GDS, the Geriatric Depression Scale; RAID, Rating Anxiety in Dementia; MMSE, Mini-Mental State Examination; DAFS, the Direct Assessment of Functional Status; NPI, The Neuropsychiatric Inventory–Questionnaire; PSS, Perceived Stress Scale; Conflict, Cohesion, and Expressive were subitems in Family Environment Scale (FES), which means Family Relationship.
DISCUSSION
To our knowledge, SOUL-P is the first multicomponent intervention for stressors and strains of AD patients according to the SPM for dementia patient’s framework. In this randomized controlled study, we tested a broad array of outcomes related to well-being [33], including QoL, depression, anxiety, and cortisol level which represent physiological reactions to stress [34]. The trial combined physiological and psychological indicators, aiming to identify the potential of the SOUL-P to improve the well-being of patients. Although anxiety and salivary cortisol levels decreased only slightly, the SOUL-P significantly improved QoL (effect size: 0.56) and depressive symptoms (effect size: –0.33); these effects were maintained at 12 months. As QoL and depressive symptoms are the net result of the interaction among multiple stressors [9], the effect of SOUL-P seems to be driven by alleviating behavioral issues (e.g., objective stressors), perceived distress (e.g., subjective stressors), and family conflict (e.g., role strains), supporting the role of SPM in dementing illnesses.
In addition to illness-related physical impairments, patients usually experience complex psychological stress [35]. For example, a patient experiencing more episodes of agitation and apathy (e.g., objective stressors) may perceive this as internally distressing (e.g., a subjective stressor), leading to subsequent effects on family conflict (e.g., secondary strains). In contrast, individuals experiencing changes in appetite or sleep cycle (e.g., an objective primary stressor) may not appraise this as distressing (e.g., as a subjective stressor). Changes in psychological and emotional experience (subjective stressors) are a result of the cognitive, functional, and behavioral aspects of dementia [9]. Thus, a combination of psychological and occupational therapy is essential to assess and distinguish between objective and subjective stressors, thus facilitating the development of interventions to enhance AD patients’ well-being according to perceived changes in their own behaviors and emotions. However, an MDT including psychological and occupational therapists has not been developed for multidomain intervention programs for dementia, such as the ACT [36], EDUCA-II [37], and MIND projects [38]. These studies indicated null to small effect sizes on depression, QoL, and stress, as well as limited explanations regarding the potential coping mechanisms for psychological distress in individuals with cognitive impairment. Guided by the SPM and MDT [38], the SOUL-P was delivered by occupational therapists and psychologists to intervene with primary stressors. For instance, occupational therapists conducted “recreational-occupational activities” [39] for a patient and “self-report pleasant activities” by the psychologist to promote apathy, agitation, and wandering (i.e., NPI: effect size: –0.30), which may occur frequently in AD patients [40]. For decreased episodes of family conflict (effect size: –0.32), our MDT performed a single-task session (i.e., one-on-one conversation or life reflection) [41] and joint planning related to dependence and responsibility. A strength of this study is that it provides a base for the essential roles of psychologists and occupational therapists in concert with reducing family relationship strains and BPSD episodes.
Unlike studies that focus on individuals with mild dementia, this study recruited participants at late stages of AD because 1) the frequency of psychological symptoms (i.e., apathy, irritation, depression, anxiety) have been reported in AD progression [42]; 2) psychological symptoms demonstrate the highest correlation coefficient with QoL, and it was possible for most patients to score 3 or more on the MMSE to rate QoL using the QoL-AD [43]; 3) previous research has shown that patients, those including in the late stages of dementia, can share and exchange ideas, needs, and preferences in meaningful ways, which are more likely to improve distress [44]. Consequently, the MDT in this study provided emotional support, memory boxes, meaningful occupation, and social interaction requiring verbal and non-verbal skills (i.e., spanning eye gaze or stroke) based on the patient’s potential of adaptive interaction. For example, caregivers or patients were instructed to populate a memory box with items such as favorite books, possessions, photographs, memorabilia ornaments, etc. “...it brought back lots of memories...” (a moderate patient). The effective collaborative communication in patients, even those with severe dementia (MMSE score: 7–10) [42], revealed enhanced self-efficacy by maintaining activities or relationships to improve perceived stress (effect size: –0.31). These results are consistent with those of a previous study, which emphasized personal interaction strategies [45].
In the SOUL-P group, perceived distress, family relationship (i.e., conflict), and BPSD were significantly increased/decreased compared with control group, which may have partly contributed to the alleviation of the patients’ depressive symptoms. Depression is affected by a combination of perceived distress, family relationship strain, and the patient’s cognitive and functional impairments [9]. Notably, cognitive and functional statuses did not have any effect as psychosocial indicators. This may be due to 1) the inclusion of participants at both moderate and severe stages [10]; and 2) to the fact that consent of training and characteristics of SOUL-P were predominantly partial to psychological symptoms (e.g., multi-sensory therapy) and considered more suitable for patients with advanced dementia [46]. Furthermore, the association between poor cognitive performance in older adults and higher hypothalamic-pituitary-adrenal axis dissonance [47] may explain limited changes in saliva cortisol concentration in this study. Future research should explore additional components to be added to the SOUL-P to improve cognitive and functional stressors and boost treatment effects.
SOUL-P consisted of maintenance sessions between 7-12 months (one third of the therapy dose in the intensive sessions) [48]. Patients in the SOUL-P group exhibited further improvements in depression (effect size: –0.44), perceived stress (effect size: –0.67), family conflict (effect size: –0.41), relationship (effect size: –0.43), and QoL (effect size: 0.75) at the final maintenance session compared with the improvements observed at 6 months. These results may suggest that a booster session in SOUL-P may be useful. The caring domain of joint rehabilitation in SOUL-P caregivers included not only basic care but also prompt completion of daily rehabilitation training and home training recording. Though SOUL-P caregiver in this study reported overloading tasks, we did not interview their outcomes. SOUL-P is a multicomponent intervention for AD patients’ stressors and strains according to the stress process model (SPM) for dementia patient’s framework. All the stressors and outcome factors were derived from the SPM theory. Several studies have suggested the impact of the family caregivers’ well-being on the patients’ well-being [9]; in this study, however, the discrepancy of demographic characteristics with family members is likely to cause the comparability of the results is limited.
There are several limitations to consider. First, this study excluded patients with severe AD (MMSE score <7) to evaluate the SOUL-P based on illness characteristics and responses of participants; indeed, more verbal language could be produced in patients with severe stages (MMSE: 0–7) [20]. Thus, further research is needed to explore these patients’ underlying needs, for example by testing the differentiating personality characteristics of AD patients. Second, SOUL-P reflects the integration of interventions for subjective and objective stressors and is unable to determine specific treatment components. The next step will be to measure and track the dosage of multi component interventions by a more rigorous method. Third, SOUL-P may also affect caregiver pressure based on the self-report survey. Although ascertain training and outcomes relied on this, assessing the primary stressors of caregivers was not possible, and it was unclear how to best address their needs. The fourth limitation is the study’s generalizability. SOUL-P is a long-term care program performed by the MDT and funded by government health care programs. Thus, future research should examine caregiver burden and cost-effectiveness. Third, although SOUL-P was well designed as a stressor-related intervention for AD patients, future dyadic approaches should examine the impact of interventions on psychosocial outcomes for caregivers, along with comparing whether the effectiveness outcomes experienced are similar for both patients and caregivers. Additionally, BPSD may be over-reported, resulting in proxy reports by NPI, which may not subjectively reflect the current issues, i.e., may overestimate the occurrence and severity of under-recognition of BPSD in AD. Consequently, this questionnaire could be modified and adapted across cultures as self-report measures (dichotomous or Likert response), thereby enabling patients to express changes in their behavior.
To conclude, promoting the well-being of AD patients will require models beyond functional treatments. SOUL-P is a multi-component program that anchors the primary stressors and secondary strains of patients. Our study findings demonstrate that the SPM-based SOUL-P reduces depression and enhances the QoL of patients, even of those at advanced stages, by alleviating their perceived stress and family relationship.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/20-0652r2).