
Abstract
Background:
Alzheimer’s disease (AD) causes memory deficit and alterations in other cognitive functions, mainly in adults over 60 years of age. As the diagnosis confirmation is performed by a postmortem neuropathological examination of the brain, this disease can be confused with other types of dementia at early stages. About 860,000 Mexicans are affected by dementia, most of them with insufficient access to adequate comprehensive health care services. Plasma biomarkers could be a rapid option for early diagnosis of the disease.
Objective:
This study aimed to analyze some plasma biomarkers (amyloid-β, tau, and lipids) in Mexican AD patients and control subjects with no associated neurodegenerative diseases.
Methods:
Plasma amyloid-β peptides (Aβ40 and Aβ42), total and phosphorylated tau protein (T-tau and P-tau), and cholesterol and triglyceride levels were quantified by enzyme-linked immunosorbent assay in AD patients and control subjects.
Results:
In Mexican AD patients, we found significantly lower levels of Aβ42 (p < 0.05) compared to the control group. In contrast, significantly higher levels of P-tau (p < 0.05) and triglycerides (p < 0.05) were observed in AD patients compared to controls. Furthermore, a significant correlation was found between the severity of dementia and plasma P-tau levels, Aβ42/Aβ40 and P-tau/T-tau ratios, and triglycerides concentrations. This correlation increased gradually with cognitive decline.
Conclusion:
The detection of these plasma biomarkers is an initial step in searching for a timely, less invasive, and cost-efficient diagnosis in Mexicans.
INTRODUCTION
Alzheimer’s disease (AD), a neurodegenerative disorder that causes memory disruption [1] and cognitive impairment [2], is the most common form of dementia (50–60%of all cases) [3]. This disease primarily affects adults > 60 years old [4], representing 10.4%of the population in Mexico in 2015; this percentage is estimated to double by 2029 [5].
The neuropathology of AD is characterized by neuronal loss [6], the presence of intracellular neurofibrillary tangles formed by hyperphosphorylated tau proteins, and extracellular senile plaques composed of amyloid-β (Aβ) peptides [7]. The pathological accumulation of Aβ in the brain is caused by the enzymatic cleavage of the amyloid-β protein precursor (AβPP), which renders two main amyloid peptides, Aβ40 and Aβ42 [8].
Age is the most important risk factor for AD, although heart disease, dyslipidemia, hypertension, type 2 diabetes mellitus, obesity, hypercholesterolemia, and genetic predisposition are also considered risk factors [9]. Epidemiological and biological evidence suggests an association between serum cholesterol levels and the development of AD [11, 12]. In the central nervous system (CNS), cholesterol is mainly found in myelin sheaths and plasma membranes of astrocytes and neurons [10] and has an essential role in the synthesis, deposition, and clearance of Aβ. Cholesterol is known to interact with Aβ reciprocally: cell cholesterol levels modulate Aβ generation, whereas Aβ alters neural cholesterol dynamics, leading to tauopathies [13].
The APOE ɛ4 allele, a strong genetic risk factor for AD, is associated with earlier and higher deposition of Aβ [14]. Apolipoprotein E (APOE) is the primary transporter of cholesterol in the brain, and its isoforms differentially modulate brain cholesterol levels. A significant association between APOE and Aβ signaling and clearance has been described [14]. Therefore, it is essential to understand the potential role of peripheral cholesterol in cerebral Aβ deposition.
The relationship between tau and Aβ plasma levels and their accumulation in the brain has been described previously. In one study, imaging findings using florbetaben-positron emission tomography (18F-FBB PET) showed that lower plasma Aβ42/Aβ40 ratio correlates with higher brain Aβ plaque burden [15]. Similar studies reported associations between plasma Aβ42/Aβ40 ratio and cortical fibrillar Aβ burden [16–18]. Additionally, it has been reported that plasma P-tau181 and total tau are differentially associated with neuroimaging in AD pathology. Across the diagnostic groups, plasma P-tau181 was consistently associated with both Aβ and Tau-PET, whereas total plasma tau was associated with cortical thickness. Plasma P-tau181 showed not only a stronger association with brain Aβ-PET but also high sensitivity and specificity for predicting elevated brain Aβ throughout AD clinical severity [19].
Conversely, some studies have shown no association between Aβ accumulation in the brain and plasma [20] and cerebrospinal fluid (CSF) Aβ levels in AD patients [21]. Furthermore, no changes in plasma Aβ concentrations in patients with sporadic AD have been observed in other reports [22–26]. In contrast, other studies have shown higher plasma concentrations of this peptide [27, 28].
Regarding the concentrations of tau protein in plasma, the results are contradictory. Some studies have reported no variations in plasma levels of this protein between dementia patients and healthy controls [29]. Conversely, other authors have reported that this protein increases in the plasma of AD patients [30, 31].
Given the different results reported for other populations, we considered it necessary to quantify these biomarkers in Mexican patients with AD. We aimed to determine the potential of plasma Aβ and tau protein levels and cholesterol and triglyceride concentrations to serve as biomarkers of AD in Mexican patients.
MATERIALS AND METHODS
Subjects
All participants were of Mexican origin. Participants were recruited from two national reference centers in Mexico City: The Dementia Clinic, Instituto Nacional de Neurología y Neurocirugía Manuel Velasco Suárez (INNN), and the Neurology Service, Hospital de Especialidades Bernardo Sepúlveda, Centro Médico Nacional Siglo XXI, Instituto Mexicano del Seguro Social (IMSS). Initially, patients were interviewed to be referred to the sub-specialty required for each case. Patients with dementia diagnosis underwent brain magnetic resonance imaging (MRI) and routine laboratory studies (complete blood count, comprehensive metabolic panel, and thyroid profile). An overall standardized evaluation was conducted by protocol, including medical, physical, neurological, cognitive, and behavioral history. For systematic cognition assessment, the following tests were performed: Mini-Mental State Examination (MMSE), Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE), semantic and phonological verbal fluency (VF), and the Clock Drawing Test (CDT). Moreover, the behavior was evaluated with the Neuropsychiatric Inventory (NPI). Also, functionality was assessed through the Functional Activities Questionnaire (FAQ). These evaluations allowed excluding other primary pathologies and establishing an etiology once dementia was confirmed. Clinical diagnosis of AD was performed according to DSM-5 and NIA-AA criteria [32]. According to the MMSE score, the severity of cognitive impairment was classified as follows: 21–26, mild; 12–20, moderate; and < 12, severe.
The inclusion criteria for patients were the following: 1) patients with confirmed dementia syndrome diagnosis were required to be able to read and write; 2) age ≥60 years old; and 3) MMSE score ≤ 20. We excluded individuals with the following characteristics: 1) acute or exacerbated chronic disease present within 30 days before the interview that could affect the quality of response to questionnaires (according to the medical staff); 2) decreased alertness; 3) severe aphasia; 4) visual and hearing impairment; 5) other neurological diseases that could have influenced the diagnosis of dementia; and 6) living in a nursing home.
The inclusion criteria for controls were the following: 1) age ≥ 60 years; 2) no symptoms or complaints of memory deficiency reported either by the informant or the participant; 3) MMSE score ≥ 24; and 4) able to read and write. We excluded individuals with the following criteria: 1) any acute or severe chronic illness; and 2) any condition (diminished alertness, severe aphasia, impaired vision or hearing) that would complicate the completion of the questionnaires.
The control group included individuals with no associated neurodegenerative disease (n = 51). According to the MMSE score, AD patients were divided into moderate (MCI) (n = 26) and severe (SCI) (n = 24) cognitive impairment. The following demographic data were collected from the participants’ medical records: sex, age, MMSE score, educational level in years of study (0, illiterate; 1-6 elementary school; 7-9, junior high; 10-14, high school), and socioeconomic level (1-2, low; 3-4, median; 5-6, high).
The research protocol for human studies was reviewed and approved by The Research Ethics Commission (IMSS, R-2017-785-073) and the Committee On Human Experimentation (INNN, 100/07) from both institutions. All the experiments were performed according to the Declaration of Helsinki, 1975. The written informed consent form was obtained from the potential participants before their inclusion in the study. All the individuals who agreed to participate in the study signed an informed consent form. A caregiver, legal guardian, or other proxy gave consent on behalf of those with substantial cognitive impairment.
Sample collection
Non-fasting blood (4 ml/subject) was collected by venipuncture in heparinized tubes (BD Vacutainer) and centrifuged at 12000 RPM for 10 min at 4°C. The upper layer of the whole plasma containing platelets was separated and stored at –80°C until further analysis.
Biochemical assays
Enzyme-linked immunosorbent assay (ELISA) kits for amyloid-β 1-40 peptide (Aβ40), amyloid-β 1-42 peptide (Aβ42), and total tau protein were purchased from Cloud-Clone-Corp (CCC, USA).
For the standard curves, synthetic Aβ140 and Aβ142 peptides were dissolved in 0.5 ml of standard diluent and kept for 10 min at room temperature. The concentration of the stock solution was 1,000 pg/ml. Before the addition of samples, Aβ peptides were diluted in a buffer and added to the ELISA plate wells in duplicate. The standard curve was developed by plotting six points at the following concentrations: 1,000 pg/ml, 333.33 pg/ml, 111.11 pg/ml, 37.04 pg/ml, 12.35 pg/ml, and 0 pg/ml.
Standards and samples were added to the appropriate microtiter plate wells with a biotin-conjugated polyclonal antibody preparation specific for each Aβ peptide. Avidin conjugated to horseradish peroxidase (HRP) was added to each microplate well and incubated, and a tetramethylbenzidine (TMB) substrate solution was added to each well. A sulfuric acid solution was added to terminate the enzyme-substrate reaction. Subsequently, the plate was analyzed at a wavelength of 450 nm. The Aβ peptides concentration was determined by comparing the optical density of the samples with the standard curve. The detection limit was 3.12–200 pg/ml.
Tau protein levels in plasma were quantified using a High Sensitive ELISA kit for human Microtubule Associated Protein tau (MAPt) (Cloud-Clone Corp) and an ELISA kit for human phosphorylated tau (Phospho) [pS396] (Thermo Fisher Scientific). Samples, standards, and blanks were added to the appropriate wells. Then, detection reagents were added, and the plate was incubated for 60 min at 37°C. After washing the plate five times, the substrate solution was added to each well and incubated for 20 min at 37°C. Finally, a stop solution was added. The analysis was conducted at 450 nm using a spectrophotometer (Epoch Microplate Spectrophotometer, Biotek Instruments, Vermont, US).
Total cholesterol and triglycerides in blood plasma were determined for each participant in duplicate and quantified by commercial colorimetric kits (Teco Diagnostic, CA, USA).
Statistical analysis
Demographic data were compared using the exact Fisher’s test for sex and the Kruskal–Wallis test followed by post-hoc Dunn’s multiple comparisons for the other variables. Demographic data with significant differences were used as covariates (socioeconomic and educational levels). Log transformation was used to approximate normal distributions and perform a covariance analysis (ANCOVA) and a Bonferroni post-hoc test. Data were expressed as mean±standard error (SE). Pearson’s correlation coefficient (r) was used to determine the association between the severity of dementia and the levels of the biomarkers with a 95%confidence interval. Analyses were performed using the IBM SPSS Statistics 20.0 software package (SPSS Inc., Chicago, IL, USA). p-values < 0.05 were considered significant.
RESULTS
The demographic characteristics of the participants are shown in Table 1. Although no significant differences were found regarding sex, a higher percentage of females was found in both the overall number of patients with AD (74%) and the SCI group (96%). Significant differences were observed regarding the educational and socioeconomic levels (p < 0.05) compared with the control group.
Demographic data on the studied population
Data are presented as mean±SD or frequencies and percentages; n, number of participants. aFisher’s-exact test; bKruskal-Wallis test. AD, Alzheimer’s disease; MMSE, Mini-Mental State Examination; MCI, moderate cognitive impairment; SCI, severe cognitive impairment; SD, standard deviation. Socioeconomic level: 1-2, low; 3-4, median; 5-6, high. Educational level (years): 0, illiterate; 1-6 elementary school; 7-9, junior high; 10-14, high school.
We analyzed the biochemical markers concentrations considering the educational and socioeconomic levels as covariates. In Table 2, data from the ANCOVA including both the unadjusted and adjusted means can be observed. No statistical differences were observed in cholesterol concentrations between groups. In contrast, the other studied markers showed statistical differences when compared between groups.
Analysis of covariance (ANCOVA) and comparisons between groups
UM, unadjusted means; AM, adjusted means; SD, standard deviation; SE, standard error; 95%CI, 95%confidence intervals. aComparison between controls and the MCI group. bComparison between controls and the SCI group. Education and socioeconomic levels were included as covariates.
Regarding Aβ peptides, we observed significantly higher plasma Aβ40 levels in the MCI group compared with the control group (Fig. 1A), whereas plasma Aβ42 levels were significantly lower in both MCI and SCI groups when compared with the control group (Fig. 1B). Furthermore, the Aβ42/Aβ40 ratio was significantly lower in the MCI and SCI groups when compared with the control group (Fig. 1 C).
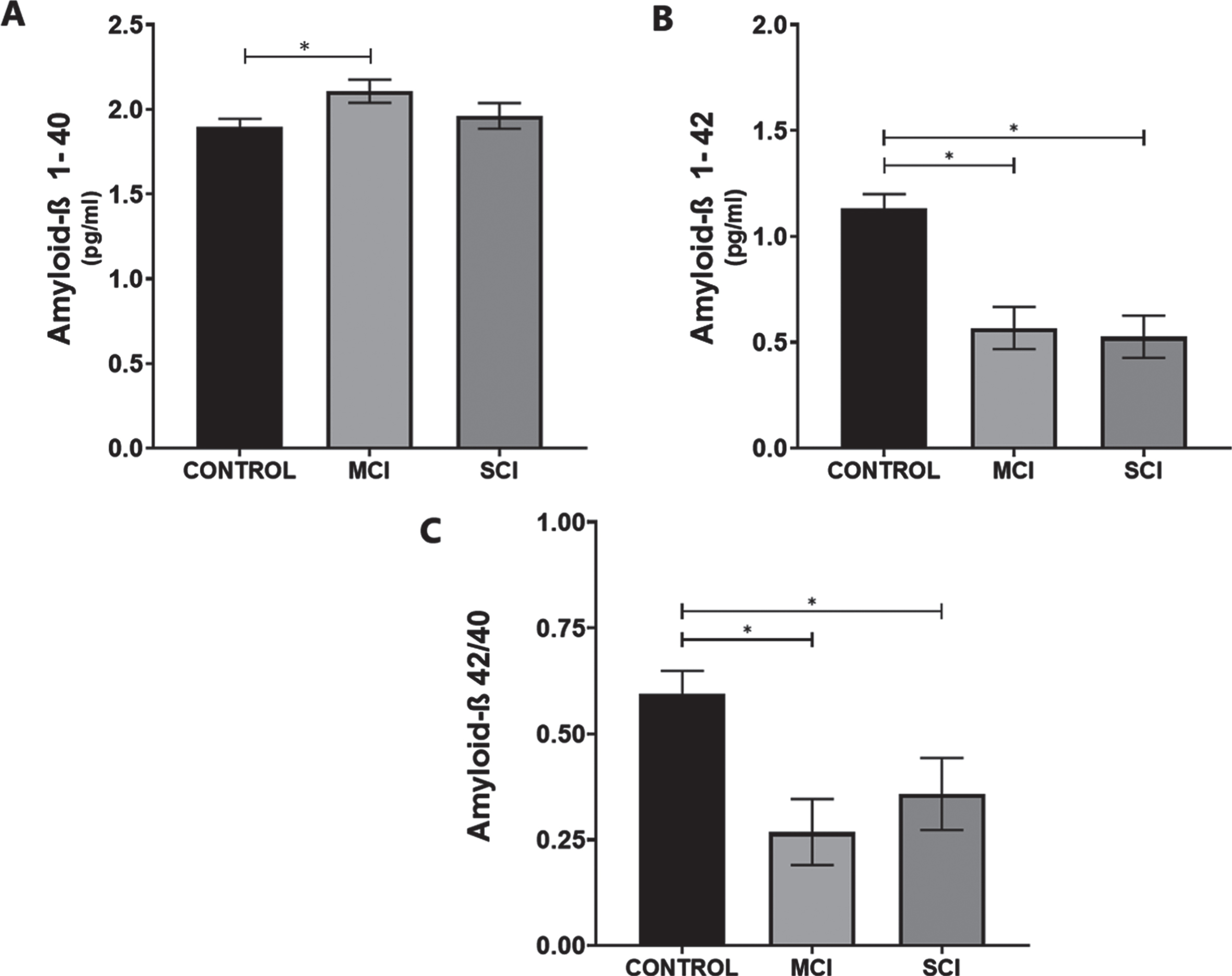
Plasma Aβ peptides in Mexican AD patients in different stages of the disease. Plasma A) Aβ40, B) Aβ42 levels, and C) Aβ42/Aβ40 ratio in controls (n = 51), and mild cognitive impairment (MCI; n = 26) and severe cognitive impairment (SCI; n = 24) groups. Data are presented as mean±SE. *p < 0.05 versus control group.
The analysis of tau protein showed significant differences between AD groups and controls. Plasma T-tau levels were lower in the MCI and SCI groups with respect to the control group (Fig. 2A). In contrast, plasma P-tau protein levels in both AD groups were higher than in the control group (Fig. 2B). Consequently, we observed a significant increase in the P-tau/T-tau ratio in both MCI and SCI groups compared to the control group (Fig. 2 C).

Total (T-tau) and phosphorylated (P-tau) tau protein in Mexican AD patients in different stages of the disease. Plasma levels of A) T-tau, b) P-tau, and C) P-tau/T-tau ratio in controls (n = 51), and mild cognitive impairment (MCI; n = 26) and severe cognitive impairment (SCI; n = 24) groups. Data are presented as mean±SE. *p < 0.05 versus control group.
In relation to plasma lipids, no changes were observed in plasma cholesterol concentrations in either of the analyzed groups (Fig. 3A). However, it is essential to note that cholesterol levels in the studied groups were higher than healthy cholesterol levels for seniors (< 200 mg/dl). A significantly higher concentration of plasma triglycerides was observed in both AD groups with respect to the control group (Fig. 3B).

Plasma lipids in Mexican AD patients in different stages of the disease. A) Cholesterol and b) triglycerides levels in controls (n = 51), and mild cognitive impairment (MCI; n = 26) and severe cognitive impairment (SCI; n = 24) groups. Data are presented as mean±SE. *p < 0.05 versus control group.
The correlation analyses between plasma biomarkers and the severity of dementia are shown in Table 3. We observed a significant correlation (p < 0.05) between the Aβ42/Aβ40 ratio, P-tau and P-tau/T-tau ratio, as well as triglycerides levels and both MCI and SCI groups.
Correlation between plasma biomarkers and the severity of dementia in patients with Alzheimer’s disease
Plasma Aβ peptides and tau protein levels were analyzed by ELISA. Aβ, amyloid-β; P-tau, phosphorylated tau; T-tau, total tau; MCI, moderate cognitive impairment; SCI, severe cognitive impairment. The association between the biomarkers and the severity of dementia was evaluated using Pearson’s correlation. *p < 0.05.
DISCUSSION
In this study, we evaluated plasma Aβ peptides, tau protein, and cholesterol and triglyceride levels in Mexican AD patients. We found significant differences in plasma Aβ peptides and tau protein levels and triglyceride concentrations between Mexican AD patients and controls. Additionally, we observed a significant correlation between the severity of dementia and plasma Aβ42/Aβ40 ratio, P-tau levels, plasma P-tau/T-tau ratio, and triglyceride concentrations.
Regarding Aβ peptides, we found significantly low plasma Aβ42 levels in the MCI and SCI group, whereas only significant high Aβ40 levels in the MCI group. In the search for biomarkers to identify early and pre-symptomatic stages of some neurodegenerative diseases, particularly AD, plasma is a promising source for research since it is the least invasive and easy to collect at a low-cost sample [33]. Aβ levels in plasma have been quantified [27, 28], but evidence has shown discrepancies among these results. Some studies have reported low Aβ40 levels and high Aβ42 plasma levels in AD patients [34, 35]. Conversely, other studies have reported low Aβ42 plasma levels associated with increased risk of dementia [36], which are consistent with our findings.
Furthermore, other studies report no changes in plasma Aβ levels between AD patients and controls [37–39]. However, most authors agree that the Aβ42/Aβ40 ratio provides more information than Aβ levels individually. Similar to our observations, other studies have reported that individuals with low plasma Aβ42/Aβ40 ratio are at somewhat more significant risk of developing AD as the Aβ42/Aβ40 ratio has been linked to cognitive decline over time [40–42].
One factor contributing to variability among studies may be ethnicity since most of the studies have been conducted in either European countries or the United States, where most of the population is Caucasian [39, 40]. Cosentino et al. included Caribbean Hispanic, African American, and non-Hispanic White patients and reported that stable or decreasing Aβ42 levels and the Aβ42/Aβ40 ratio at follow-up were associated with global cognitive decline [35]. These findings support our results regarding plasma Aβ42 levels in Mexican AD patients, although patient follow-up was not performed.
Sex is another factor that may account for differences among studies [43, 44]. A relatively higher risk of AD in females has been reported, suggesting interactions between the hormonal decline associated with menopause and Apolipoprotein E (APOE) ɛ4 [45]. Namely, among APOE ɛ4 carriers, women are at greater risk for developing AD than men [46, 47]. However, the APOE genotype was not addressed in the patients studied here.
Another explanation for plasma Aβ42 levels decrease could be its accumulation and subsequent formation of amyloidogenic plaques in the brain [17]. Therefore, as cognitive decline progresses in AD patients, brain Aβ burden and plasma Aβ concentrations would increase and decrease, respectively.
Regarding the differences reported in plasma Aβ and tau concentrations in patients with AD, another consideration to be made is the origin of the sample. Several authors used blood samples, while others have access to CSF to search for biomarkers in patients with AD. Due to the miscellaneous nature and the large size range of blood components, plasma samples are much more variable than CSF [48].
We observed that plasma total tau protein levels were lower in the AD groups, whereas a higher concentration of the phosphorylated form (P-tau) was identified in these groups compared to the control group. Similarly, we observed a significant correlation between the increased P-tau/T-tau ratio and cognitive impairment. This correlation indicates that higher concentrations of P-tau could be found in plasma since the early stages of the disease and suggests an association between tau levels and cognitive decline [49, 50]. A possible explanation for this observation could be that neurofibrillary tangles deteriorate the blood-brain barrier, which allows the leakage of the Aβ peptides and tau protein in AD patients [51]. Therefore, plasma tau levels might reflect neuronal damage and the subsequent drainage of tau from the brain parenchyma to the CSF and blood [52, 53]. Based on other studies, an increase of tau levels in the late stages of AD was expected [54]. However, no significant difference was observed between the MCI and SCI groups. Our results are similar to other studies in which cognitive status was not related to tau deposition in patients with Parkinson’s disease [55].
Regarding lipid concentrations, our findings showed that cholesterol levels were higher than healthy ranges for elderly adults (< 200 mg/dl) in both groups of Mexican AD patients and the control group. However, we found no significant differences in plasma cholesterol levels between the AD and control groups. These high cholesterol levels in Mexican adults (> 60 years of age) indicate a risk of developing other diseases, such as high blood pressure, type 2 diabetes, and metabolic syndrome [56–59]. These comorbidities are related to neurodegeneration [60, 61] and suggest that high lipid concentrations could lead to systemic hyperlipidemia that might cause damage to the blood-brain barrier [62] and facilitate the migration of proteins such as Aβ and tau to the bloodstream. In addition, some authors have reported that APOE4 carriers display both hypertriglyceridemia and hypercholesterolemia [63]. Furthermore, APOE4 is associated with glucose hypometabolism in the brain of older adults [64]. In astrocytes, APOE4 expression reduces the ability to degrade Aβ peptides and provides one mechanism for the increased formation of amyloid plaques [65].
Moreover, we observed higher levels of triglycerides in AD patients than controls. Although cardiovascular diseases are not a direct cause of neurodegenerative diseases, several studies have implicated heart disease as a risk factor for dementia [66–68]. High levels of triglycerides can cause atherosclerosis, which in turn increases the risk of cardiovascular events. These high levels of triglycerides could be the result of other AD-related comorbidities, such as type 2 diabetes mellitus and the metabolic syndrome [59]. Furthermore, a longitudinal cohort study in cognitively healthy individuals concluded that midlife increased levels of triglycerides could predict brain Aβ pathology, supporting the involvement of lipids in very early stages of AD development [68]. In contrast, other studies do not support the hypothesis that the risk of AD is associated with plasma lipid concentrations [69]. Therefore, further research and follow-up in a larger sample of Mexican AD patients is necessary to clarify this.
Several authors have studied the influence of socioeconomic factors such as educational and socioeconomic status (SES) in healthcare, particularly for AD. However, the results of this association are ambiguous. In some studies, no association between the risk of AD and SES was found [70], while other studies report an association between low SES and high risk for AD [71]. Another study indicated that SES is associated with a higher risk for AD in Black people than White people in the US [72]. No ethnic differences were registered in our study population. However, our results indicated a higher SES in the SCI group compared to the other two groups. An explanation for this finding may be because SES can influence the educational level and better health culture, as reported in other developing countries [73]. Therefore, people with higher SES and educational levels have greater access to medical check-ups in health institutions where chronic diseases such as AD can be detected and treated. In contrast, it is more difficult to receive medical care for low-income and low-educated people, even more so from public health institutions, due to their high demand in the country. However, the influence of these factors on AD should be studied further.
This type of study is essential in the Mexican population, for which this is a strength of our research. However, some limitations of the study warrant consideration. First, non-fasting blood samples were collected, and we did not assess whether patients were under any anti-cholesterol medications, which may have revealed differences in cholesterol levels among groups. Second, the APOE genotype was not determined. Third, the study did not include subjects with other types of dementia or neurodegenerative diseases. Therefore, our findings could not be used to differentiate between AD and other dementias in the Mexican population. Fourth, we consider that the sample size was relatively small. Future research is needed to determine whether these plasma compounds could be a more useful diagnostic marker for Mexican AD patients in combination with neurodegenerative neuroimaging measures. In addition, follow-up of these participants would be essential to analyze whether these markers change over time.
The number of adults > 60 years of age who may develop AD will be a public health issue and economic concern worldwide. Overall, the present results are an early step in determining whether peripheral blood analysis could aid in an early AD diagnosis.
Footnotes
ACKNOWLEDGMENTS
This work was submitted in partial fulfillment of the requirements for the Ph.D. degree of Tzayaka Castillo Mendieta at Doctorado en Ciencias Biológicas y de la Salud (UAM-I). Tzayaka Castillo Mendieta received financial support from CONACyT (308389) and CIS/IMSS/ (99096803). Christian Guerra-Araiza received financial support for this project from FIS/IMSS (Project No. FIS/IMSS/PROT/G17-2/1718). The funders had no participation in the design of the study, collection, and analysis of data, decision to publish, or preparation of the manuscript. The publication of this paper was supported by a grant from the Secretaría de Educación, Ciencia, Tecnología e Innovación de la Ciudad de México CM-SECTEI/200/2020 Red Colaborativa de Investigación Traslacional para el Envejecimiento Saludable (RECITES) de la Ciudad de México.