
Abstract
Background:
TAR DNA-binding protein-43 (TDP-43) and neurofilament light chain (NfL) are promising fluid biomarkers of disease progression for various dementia.
Objective:
We would explore whether blood levels of NfL and TDP-43 could predict the long-term progression to dementia, and the relationship of TDP-43 levels between cerebrospinal fluid (CSF) and blood.
Methods:
A total of 86 non-dementia elderly received 7-year follow-up, and were divided into 49 stable normal control (NC)/mild cognitive impairment (MCI) subjects, 19 subjects progressing from NC to MCI, and 18 subjects progressing from NC/MCI to dementia. Blood TDP-43 and NfL levels, and cognitive functions were measured in all subjects. Furthermore, another cohort of 23 dementia patients, including 13 AD and 10 non-AD patients received blood and CSF measurements of TDP-43.
Results:
In cohort 1, compared to stable NC/MCI group, there were higher levels of blood TDP-43 at baseline in subjects progressing from NC/MCI to dementia. The combination of baseline blood TDP-43 levels with demographics including age, education, and diabetes had the detection for dementia occurrence. Baseline blood levels of NfL are negatively associated with cognitive function at 7-year follow-up. In cohort 2, we found there were no relationship between CSF and blood levels of TDP-43. Moreover, the levels of TDP-43 in CSF was positively associated with the age of patients, especially in AD group.
Conclusion:
Single blood TDP-43 could not estimate dementia occurrence; however, TDP-43 combined with demographics has the predictive effect for dementia occurrence and NfL level is associated with a decrease of cognitive function.
INTRODUCTION
The burden of cognitive impairment is dramatic-ally growing with the elderly in the world. The estimated annual conversion rate for patients with mild cognitive impairment (MCI) is 5–10% [1]; however, less than 50% will have developed dementia over a period of 10 years [2]. Identification of factors con-tributing to progression from MCI to dementia is crucial. Neurodegenerative dementia includes multiple types, such as Alzheimer’s disease (AD), frontotem-poral dementia (FTD), dementia with Lewy bodies, progressive supranuclear palsy, and others. Previous studies focused more on predicting AD in elderly population, and the combination of three cerebrospinal fluid (CSF) biomarkers including amyloid-β1–42 (Aβ1–42), total tau (t-Tau), and phosphorylated tau (p-Tau) with hippocampus atrophy on MRI have been extensively studied [3]. Recently, other biomarkers have been described to have potential for predicting dementia occurrence. Neurofilament light chain (NfL), a neuronal-specific intermediate filament of the axonal cytoskeleton, is associated with axonal injury or degeneration. Blood concentration of NfL has been found to increase in various dementia individuals with FTD, AD, and other neurodegenerative disorders [4, 5]. TAR DNA-binding protein-43 (TDP-43), a nuclear protein, is primarily involved in alternative splicing and transcriptional regulation [6]. Evaluating blood levels of TDP-43 was detected in 46% of patients with clinical FTD and 22% of patients with AD, compared to 8% of controls [7]. Furthermore, a study demonstrated that plasma levels of phosphorylated TDP-43 correlated with the extent of TDP-43 postmortem brain pathology in FTD [8].
In a clinical perspective, individuals classified to be at short-term risk, i.e., within 1 or 2 years, can re-ceive more active treatment [9], and previous studies focused little on long-term risk of dementia. In the present study, we explored whether blood levels of NfL and TDP-43 could predict the long-term progression to dementia in community elderly, and the relationship of TDP-43 levels between CSF and blood. In our analysis, we described the predictive power of a combination of blood TDP-43 with demographic information to determine dementia occurrence from community elderly.
MATERIALS AND METHODS
Cohort 1 was part of the China Longitudinal Ageing Study (CLAS) of Cognitive Impairment, which was a community-based study initiated in 2012. There were 86 non-dementia elderly involved in the present study, who underwent a screening process that included medical history, physical examination, blood tests, baseline and 7-year follow-up assess-ments of cognitive function by a face-to-face interview. All participants were Mandarin-speaking Han Chinese. According to the follow-up results, 86 sub-jects were divided into three groups including cognitively stable (stable normal control (NC), stable mild cognitive impairment (MCI), and MCI turning into NC) (n = 49), NC progressing into MCI (n = 19), and NC/MCI progressing into dementia (n = 18) groups.
The Beijing version of the Montreal Cognitive Assessment (MoCA) [10] and Mini-Mental State Examination (MMSE) [11] were used to measure cognitive function. At baseline, 86 non-dementia elderly including 67 NC and 19 MCI, were required to meet the following criteria for inclusion in the study: 1) Han Chinese, ≥60 years old; 2) cognitive normal; 3) in accordance with the MMSE cutoff score, uneducated subjects ≥18, elementary school educated subjects ≥21, and higher than middle-school educated subjects ≥25 [12]; 4) no major medical abnormalities, including nervous system disease or unstable, acute or life-threatening medical ailments; and 5) able to complete the study. Absence of dementia was diagnosed according to Clinical Dementia Rating (CDR) and cognitive scores. When CDR = 0 and cognitive scores in accordance with MMSE cutoff score, subjects were included in absence of dementia.
At baseline and follow-up period, NC was in accordance with the criteria of non-dementia and MoCA score ≥23 [13], and MCI was diagnosed according to Petersen’s criteria [14] and MoCA score <23 [13]. Based on cognitive test scores, patients displaying at least one memory deficit with or without an additional deficit in another domain were included in the MCI group. At follow-up period, dementia and probable AD was diagnosed according to the criteria from the Diagnostic and Statistical Manual for Mental Disorders IV (DSM IV), and from the National Institute of Neurologic and Communicative Disorders and Stroke/Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) [15].
Cohort 2 were 23 dementia patients from a cohort of the Shanghai Brain Aging study, including AD (n = 13) and non-AD dementia (n = 10). The participants received clinical examination, blood tests, CSF tests, MR imaging scans, and cognitive function assessments. In AD cases, the clinical and neuropsychologic diagnosis remained in accord with the results of biomarkers of neurochemical dementia diagnostics (NDD), which were analyzed by enzyme-linked immunosorbent assays (ELISA) including Aβ42, Aβ42/40, tau, and p-Tau [16].
This study was carried out in accordance with the recommendations of the Shanghai Mental Health Center ethical standards committee on human experimentation. All subjects provided written consent to participate in the research.
Measurement of blood TDP-43 and NfL
Peripheral blood samples were collected from all subjects by venipuncture into a coagulation promoting tube (Ethylenediamine tetraacetic acid, EDTA) in the baseline period, which were collected and centrifuged at 800 g for 20 min at 4°C. CSF samples were collected via lumbar puncture at the L3/4 or L4/5 space, which were centrifuged at 3000 g for 5 min at 4°C to remove cells. CSF and plasma samples were stored at –80°C, and were shipped frozen on dry ice for analyses. Plasma samples collected at baseline were detected after 7 years of follow-up. Plasma/CSF NfL and TDP-43 were quantified using an ultra-sensitive Simoa technology (Quanterix, MA, US) on the automated Simoa HD-X platform (GBIO, Hangzhou, China) per manufacturer’s instruction. NfL assay (Cat No: 102258) and TDP-43 assay (Cat. No. 103293) kits were purchased from Quanterix and used accordingly. Plasma samples were diluted at a 1:4 ratio for plasma NfL, plasma/CSF TDP-43, and at a 1:100 ratio for CSF NfL assays. Calibrators and quality controls were measured in duplicate. All sample measurement was performed on a single run basis. Operators were unaware of participants’ disease status.
Data analysis
Demographics, lifestyle, physical disease, and cognitive scores were analyzed using variance analysis for continuous variables and a χ2 test for cat-egorical variables. The results of plasma TDP-43 and NfL concentration were both not normally distributed and would be transitioned with logarithms or trigonometric functions to fit the normal distribution. The demographic factors with difference between groups (marked by an asterisk in Table 1) were regressed on analysis of covariance.
Characteristics of participants in cohort 1
Logistic regression analysis was employed using the diagnosis of 7-year follow-up as dependent variable (non-dementia = 1, dementia = 2), with plasma TDP-43 concentration as independent variable. Cov-ariates in these models included demographics (age and education), lifestyle (drinking, smoking, tea), and physical diseases (hypertension and diabetes). Significant covariates would be included to build the prediction model. Diagnostic accuracy of plasma TDP-43 levels combined with several significant covariates were assessed by receiver operation cha-racteristic (ROC) curve analysis. The Pearson correlation coefficient was used to explore potential the associations of plasma TDP-43 and NfL with cognitive scores. All statistical analyses used SPSS version 17.0 software with two-tailed p value of 0.05.
RESULTS
Demographic and clinical variables
In cohort 1, demographics and cognitive scores for stable NC/MCI (n = 49), progressing from NC to MCI (n = 19), and progressing from NC/MCI to dementia (n = 18) subjects are shown in Table 1. The demographic data with difference between groups are indicated by asterisk and controlled by covariance analysis. As expected, differences in cognitive scores were observed.
In cohort 2, demographics and cognitive scores for AD dementia (n = 13) and non-AD dementia (n = 10) subjects are shown in Table 2.
Characteristics of participants in cohort 2
Levels of TDP-43 and NfL
In cohort 1, plasma levels of TDP-43 and NfL are shown in Table 1. Logarithmic transition for plasma TDP-43 significantly differed between stable NC/ MCI and progression to dementia groups (F = 4.493, p = 0.038). There was no difference of trigonometric transition for plasma NfL between any two groups. Correlation analysis found that baseline levels of plasma NfL was negatively associated with cognitive function of 7-year follow-up, including MMSE scores (r = –0.231, p = 0.033) and MoCA scores (r =–0.250, p = 0.02) (Fig. 1).
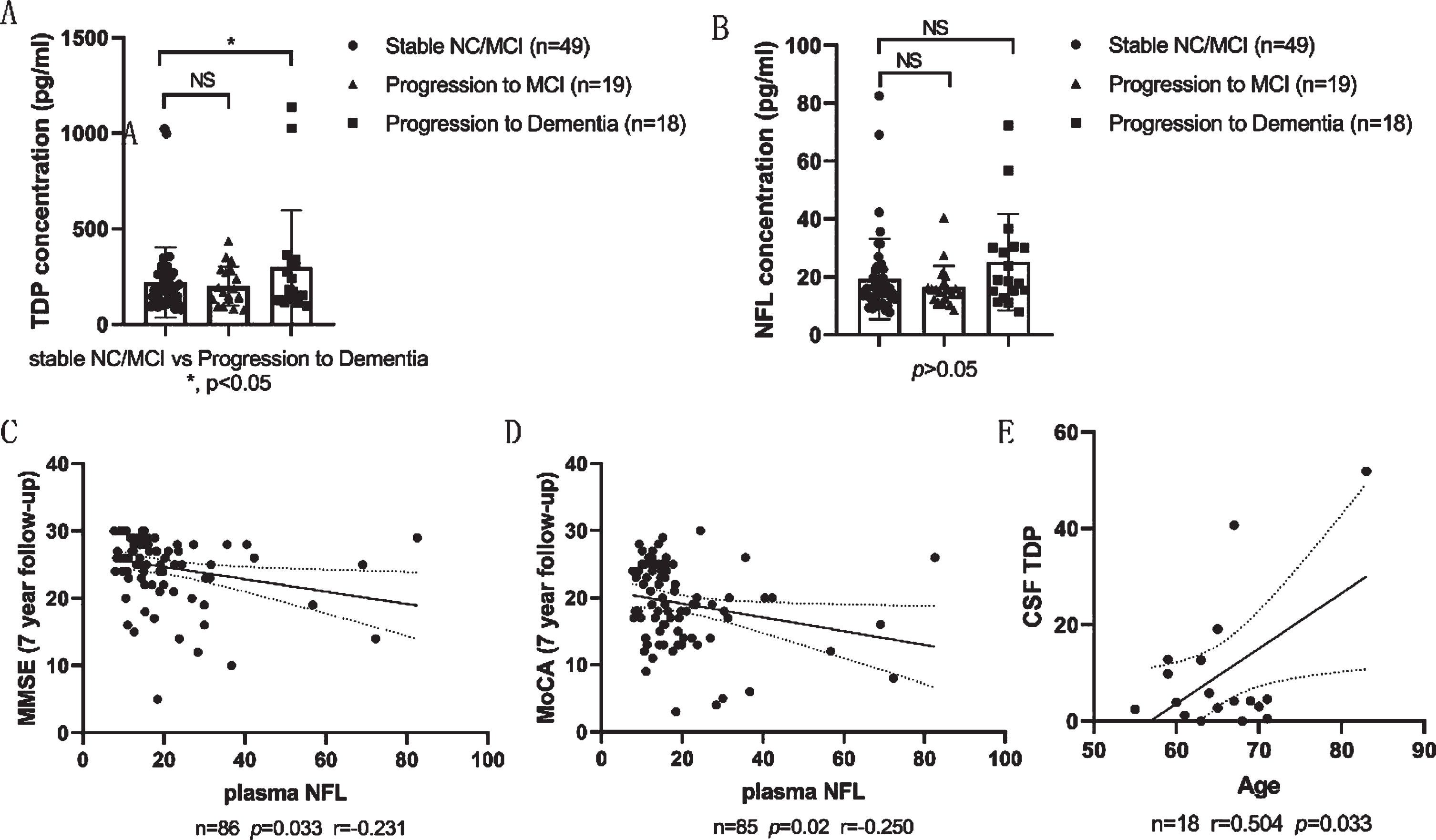
The plasma levels of TDP-43 and NfL in stable NC/MCI, progression to MCI, and progression to dementia subjects in cohort 1, correlations of plasma NfL with cognitive scores in cohort 1, and correlations of CSF TDP-43 with age in cohort 2. A) There were significant differences of plasma TDP-43 between stable NC/MCI and progression to dementia groups. B) There were no significant differences of plasma NfL between any two groups. C, D) Correlation plots showed negative correlations between plasma NfL of baseline and cognitive scores of 7-year follow-up including MMSE and MoCA scores in cohort 1. E) Correlation plots showed positive correlation between CSF TDP-43 and age in cohort 2.
Two groups including non-dementia (n = 68) and progressing from NC/MCI to dementia (n = 18) were involved in the ROC curve analysis. The area under the curves (AUC) of plasma TDP-43, age, and edu-cation levels for patients progressing to dementia were 0.576 (95% CI = 0.421–0.731), 0.712 (95% CI = 0.574–0.850), and 0.659 (95% CI = 0.516–0.806), respectively. The odds ratio (OR) for plasma TDP-43 alone and NfL alone in Logistic regression ana-lysis was 1.002 (p = 0.056) and 1.035 (p = 0.02) respectively. Multiple factors were involved in the logistic regression, and the following were identified as the significant factors for dementia occurrence after 7 year-follow-up, including age, education, pla-sma TDP-43 levels, and diabetes at baseline, not plasma NfL levels. Above significant covariates were included to build the prediction model in the logistic regression analysis, and B value of constant was 15.378, age 0.102, plasma TDP–43 0.006, education –0.149, and diabetes 3.341, respectively. ROC curve analysis revealed that AUC of prediction model for progression to dementia patients was 0.836 (95% CI = 0.733–0.939) (Table 3).
The prediction model of plasma TDP-43 combined with demographics is a good parameter to distinguish subjects (from NC/MCI to dementia) from subjects (non-dementia) through a single cross-sectional analysis at baseline
*prediction model 1: –8.394 + 0.074× age –0.115× education +1.403× diabetes. *prediction model 2:15.378 + 0.102× age –0.149×education +3.341×diabetes +0.006×plasma TDP-43. 95% CI, 95% confidence interval; AUC, area under the curves; ROC, receiver operation characteristic.
In cohort 2, we did not observe significant correlation of TDP-43 between plasma and CSF levels in the total group and in AD dementia group. There was none correlation between CSF TDP-43 and CSF AD biomarkers including Aβ42, Aβ42/40, tau, and p-Tau in AD dementia group. However, a significant correlation between age and CSF TDP-43 levels was observed in the full sample (r = 0.448, p = 0.041) and in AD dementia patients (r = 0.658, p = 0.028) (Table 2, Fig. 1).
DISCUSSION
In the present study, our cohort 1 included non-dementia elderly which was generated from the CLAS study. 86 non-dementia elderly received 7-year follow-up, and were divided into 49 stable NC/MCI subjects, 19 subjects from NC to MCI, and 18 subjects from NC/MCI to dementia. 1) Compared to stable NC/MCI group, there were higher levels of blood TDP-43 in subjects progressing from NC/MCI to dementia. The combination of baseline blood TDP-43 levels with demographics information had the detection for dementia occurrence. 2) Baseline blood levels of NfL were negatively associated with cognitive function of 7-year follow-up. Our cohort 2 con-sisted of 23 dementia patients from a cohort of the Shanghai Brain Aging study, including 13 AD pat-ients and 10 non-AD patients. 1) We found there was no relationship of TDP-43 between CSF and blood levels. Moreover, 2) the levels of TDP-43 in CSF was positively associated with the age of patients, especially in the AD group.
To the best of our knowledge, this is the first report investigating the effects of blood TDP-43 levels combining with demographics on predicting dementia occurrence through long-term follow-up. Previous histopathological studies demonstrated that about 50% of patients with FTD and 25% of patients with AD had TDP-43 pathology [6, 18]. Increased CSF levels of TDP-43 have been reported in patients with FTD and amyotrophic lateral sclerosis, and subsequently, increased plasma levels of TDP-43 have also been reported in FTD, amyotrophic lateral sclerosis, AD, and MCI [6, 19]. In our research, we also identified the increased expression of blood TDP-43 in subjects progressing from NC/MCI to dementia, compared to stable NC/MCI subjects. Although single blood TDP-43 had lower performance for pre-dicting dementia with total AUC of 0.576, the predictive model consisting of blood TDP-43 and demographic information including age, education, and diabetes factors, had good predictive value with total AUC of 0.836. A previous study found that the concentration ratio of TDP-43 in CSF to blood is about 1:200 [20]; however, our research of cohort 2 showed that CSF and blood TDP-43 levels did not correlate with each other, which was consistent with the study of Suarez-Calvet that demonstrated only phospho-TDP-43 in CSF and blood correlated [21]. The different result might be attributed to the limited samples of our research, or the potential fact that only phospho-TDP-43 was a surrogate marker for brain TDP-43 pathology. Anyway, the elderly with the tendency for developing dementia at an early stage might have alterations in TDP-43 metabolism. Moreover, we found a positive correlation between age and CSF TDP-43 levels in total subjects and AD patients respectively. Previous studies also demonstrated TDP-43 positive inclusions in limbic brain regions as limbic predominant age associated TDP-43 encephalopathy, which could be found in elderly individual (mostly 80 years of age or older) with and without AD [22].
Over the last two decades, an increasing number of studies had shown that NfL levels in CSF and blood were altered in CNS diseases and correlated with the disease characteristics. NfL was released from neurons in degenerative neuropathology [23], which was considered as a marker to detect the early stages of neurodegenerative dementia and was not specific to AD [24]. Previous studies showed that AD, vascular dementia, FTD, and other neurodege-nerative dementia diseases were associated with a significant increase in both CSF and blood NfL levels compared with a control cohort [24]. Our research did not show a significant increase in blood NfL expression in the elderly progressing from NC/MCI to dementia, compared with stable NC/MCI subjects. Consistently, previous studies reported only non-significant or barely significant increases of absolute NfL in blood in pre-symptomatic AD [25, 26]; however, NfL annual rate of change could distinguish NC and MCI as early as 16 years before estimated symptom onset with the use of serial NfL measurements [27]. The above information suggested the serial measurement of blood NfL was predictive for dementia rather than absolute measurement at a single time point [27]. Furthermore, in our research, baseline blood levels of NfL were negatively associated with cognitive function of 7-year follow-up assessed by MMSE and MoCA testing. Previous study also found that baseline serum NfL was highly associated with a decrease in cognitive function including MMSE and Logical Memory Scores [27], which was consistent with our results.
Limitation
There are several study limitations. The number of subjects involved in the follow-up study is insufficient, so that after divided into subgroups, the patients in the dementia group are less. The number of dementia patients detected by CSF testing is also insufficient. The follow-up duration is 7 years and can reflect dementia occurrence; however, lack of serial measurements of TDP-43 and NfL had lower value to predict for dementia.
Conclusion
In conclusion, blood levels of TDP-43 at baseline were significantly higher in subjects progressing from NC/MCI to dementia through 7-year follow-up. Blood TDP-43 levels combined with demographics information could predict dementia occurrence and blood NfL levels correlated with decrease in cognitive function.
ACKNOWLEDGMENTS
This study was supported by grants of Science Foundation of the Chinese Academy of Sciences (XDA1204101), Clinical research center project of Shanghai Mental Health Center (CRC2017ZD02), Shanghai Brain Health Foundation, National Scie-nce and technology support program of China (2009BAI77B03), and National Natural Science Foundation of China (81301139).
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/20-1263).