
Abstract
Background:
Neuroprotection against Parkinson’s disease degeneration by photobiomodulation has been reported in animal models but no true placebo-controlled human studies have been published.
Objective:
To understand if photobiomodulation therapy can produce clinically significant differences in physical performance measures in people with Parkinson’s disease; and what frequency of treatment is necessary to initiate clinical change.
Methods:
In a participant and assessor-blinded, randomized, placebo-controlled pilot study, 22 participants received either sham and/or active laser photobiomodulation (904 nm, 60 mW/diode, 50 Hz) for 33 s to each of 21 points at the cranium and intra-orally, on one, two or three times/week for 4 weeks. Two treatment phases were separated by a 4-week wash-out (Phase 2). Upper and lower limb physical outcome measures were assessed before and after each treatment phase. The Montreal Cognitive Assessment was evaluated prior to treatment Phase 1, and at the end of treatment Phase 3.
Results:
Montreal Cognitive Assessment remained stable between start and end of study. No measures demonstrated statistically significant changes. With regular treatment, the spiral (writing) test and the dynamic step test were most sensitive to change in a positive direction; and the 9-hole peg test demonstrated a minimum clinically important difference worthy of further investigation in a larger, adequately powered clinical trial. A placebo effect was noted.
Conclusion:
The results support the notion that combined transcranial and intra-oral photobiomodulation therapy needs to be applied at least 2 to 3 times per week for at least four weeks before some improvement in outcome measures becomes evident. Longer courses of treatment may be required.
INTRODUCTION
Parkinson’s disease is a common and progressive neurodegenerative disorder. Clinical manifestations may include altered muscle tone, bradykinesia, muscle rigidity, akinesia, resting tremor, micrographia, autonomic dysfunction, disorders of sleep, and cognitive decline, all of which significantly impact the quality of life for the person with PD and their carer [1]. According to the GBD 2016 Parkinson’s Disease Collaborators [2], Parkinson’s disease is the fastest growing of all neurological disorders globally with prevalence doubling over the last generation.
Parkinson’s disease develops as a result of nerve cell loss in an area of the midbrain (the substantia nigra) [3]. In humans, it is estimated that when motor (movement) signs first appear and a diagnosis is possible, there is already a significant loss of dopamine nerve cells. The cause of Parkinson’s disease is unclear. One hypothesis is associated with dysfunction of the mitochondria. Under certain conditions there can be a progressive accumulation of mutations in mitochondrial DNA that reduces mitochondrial efficiency and ATP yield. This process leads to an increase in toxic reactive oxygen species, generating oxidative stress and subsequent nerve degeneration [4, 5].
Treatment for Parkinson’s disease has previously been divided in to pharmacological, surgical and rehabilitative approaches [6]. Dopamine replacement drug therapy remains the mainstay of medical treatment for Parkinson’s disease and implantation of deep brain stimulators can be offered [7]. Dopamine drug therapy aims to replace the lost dopamine, while deep brain stimulation aims to introduce stimulation to basal ganglia pathways impaired by the loss of dopamine. Dopamine drug therapy, although effective in assisting communication between cells in the impaired mid-brain [8] can cause side effects (more common in the medium term) that may cause alterations in other neural pathways [9]. The surgical implantation of a deep brain stimulation system is usually recommended to patients after the efficacy of drug treatment declines or when the disease has progressed sufficiently. Surgical management is invasive and carries risks and may not have sustainable outcomes. For example, in a multi-center study with 4-year follow-up, although some indicators were improved, gait, postural stability, and speech were noted to worsen significantly after deep brain stimulation [10].
The primary goal of adjuvant rehabilitation is to optimize function and minimize the deleterious effects of the condition [11] with some evidence of short-term, clinically important benefits in walking speed and balance [12], but there is no agreement on the specific requirements for a rehabilitation program. Exercise may induce an interplay between degenerative and regenerative mechanisms [11] reducing chronic oxidative stress by stimulating mitochondrial biogenesis and neurotransmitter synthesis [13]. The promotion of physical activity is considered the only justifiable intervention for the prevention of Parkinson’s disease, but low adherence rates limit the benefits of exercise [14]. Identifying alternative non-invasive methods of stimulating cellular activity in neurons within the impaired mid-brain may prove highly beneficial to people with Parkinson’s disease and could be used as an adjunct for other treatment methods.
Photobiomodulation therapy (PBMt) is a safe, non-invasive, and non-thermal method that is based on a substantial body of research dating back to the 1960s [15]. The mechanisms of action are proposed to involve the stimulation of mitochondrial action by the absorption of photons in specific transmembrane proteins (e.g., cytochrome c oxidase), resulting in increased ATP production, leading to reduced oxidative stress, anti-inflammatory effects, improved cellular energy, increased synthesis of enzymes, and increased focal cerebral blood flow [16]. Studies of the effect of PBMt applied to the cranium in people with another neurodegenerative condition (Alzheimer’s disease) have reported progressive improved cognitive function following a 6-week regimen of treatment [17]. In a review of neurological and psychological applications of transcranial PBMt, Rojas and Gonzalez-Lima [18] describe the positive effects seen in animal models of stroke, traumatic brain injury, Alzheimer’s disease, or cognitive impairments using cranial applications of PBMt. These authors also note that PBMt has demonstrated no deleterious effects on the structure and function of the brain at the doses evaluated. Studies have applied both transcranial (e.g., WARP-LED) or intracranial (e.g., optical fiber device) methods to deliver light therapy at irradiances ranging from 1–700 mW/cm2 [19–23] and have reported no adverse effects on brain tissue structures and function [16, 24].
Other researchers have reported the development of neuroprotection against Parkinson’s disease degeneration stimulated by PBMt in animal models [25–27]; and the basic science research and anecdotal clinical evidence, offers support for the benefits of PBMt in humans with Parkinson’s disease [25–29]. In primates, in which a Parkinson’s disease state was modelled by a neurotoxin, the application of PBMt reduced the signs of motor dysfunction as well as promoted neural protective responses and in some cases neuro-regeneration of impaired nerve cells [27]. Moreover, PBMt was well tolerated and improved sleep-wake cycles in people with Parkinson’s disease [1, 30]. The applicability of PBMt, the positive animal study responses, and the lack of side effects suggest that PBMt could be a viable adjunct to current treatments for Parkinson’s disease [31]. Due to the broad range of parameters already evident in the literature there remains uncertainty regarding the PBMt dosing factors for use in Parkinson’s disease. This study set out to clarify two of those factors a) number of treatments per week, and b) if the effect of treatment is sustained after cessation of treatment.
While Saltmarche et al. [17] demonstrated changes in humans with Alzheimer’s disease, no placebo-controlled study combining transcranial and intra-oral PBMt has yet explored this method of treatment in humans with Parkinson’s disease. In a preliminary N = 1 clinical study [32] evaluating the feasibility of using light therapy in Parkinson’s disease (VieLight 810nm LED; 6 applications/week for 4 weeks; 40 Hz; 50%duty cycle; mixed fluence and irradiance), we demonstrated trends toward improvement in four domains of the Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS; non-motor and motor experiences of daily living, motor examination, and motor complications) but no change in other objective measures. Based on this work, we set out to understand in a participant and assessor-blinded, randomized, placebo-controlled pilot study if (1) combined transcranial and intra-oral PBMt can produce clinically significant differences in physical performance measures typically used in research involving people with Parkinson’s disease; and (2) what frequency of treatment was necessary to initiate clinical change. The results of this study will inform proof of concept and future, adequately powered placebo-controlled clinical trials in this field.
METHODS
Participants
A total of 22 participants diagnosed with Parkinson’s disease by a movement disorders specialist neurologist (AL) were recruited with the expectation of a 10–20%drop-out rate. Participants were randomly allocated to one of either placebo intervention or active intervention in Phase 1. Participants were required to meet the criteria for inclusion and exclusion (Table 1).
Inclusion and exclusion criteria
Intervention protocol
The study was divided into three phases, each of 4 weeks duration with the intention of determining whether the frequency of active treatment (one, two, or three applications per week) had any bearing on outcomes, as well as providing an opportunity to assess for a placebo effect. Phase 1 constituted a treatment period, Phase 2 a wash-out period, and Phase 3 a further treatment period. Participants were randomized in to two groups (Table 2) and all participants received intervention during at least one of the study phases.
Group intervention protocol and experimental phases
All participants presented to the clinic three times a week in Phase 1 and Phase 3. Group 1 received the placebo intervention in the first 4 weeks termed Phase 1 (hence for ease of reporting is also referred to as the placebo group); and in the last 4 weeks termed Phase 3, received one placebo treatment and two active PBMt treatments weekly. Group 2 received the active intervention three times weekly during Phase 1; and two placebo treatments and one active treatment during Phase 3. Participants were blind to the treatment protocol although they were aware that they could be receiving either of the following options (placebo, once a week, twice a week or three times a week treatment). The researcher administering the PBMt was blind to which device was active or placebo, and for each participant the blinded researcher followed a weekly color coded protocol provided to them. The PBMt devices displayed the same visual and auditory cues although only one device was designed to emit PBMt. The examiners collecting participant outcome data were blind to the group allocation of each participant.
Photobiomodulation parameters
The Class 3B Irradia Australia Mid-Laser 2.5 was utilized in this study (Table 3 and Fig. 1). The application points are demonstrated in Figs. 2 3. Power output of the device was checked weekly using a NOVA II laser power/energy meter (Ophir Australia).
Laser device* and photobiomodulation parameters
*Irradia (Australia) Mid-Laser 2.5
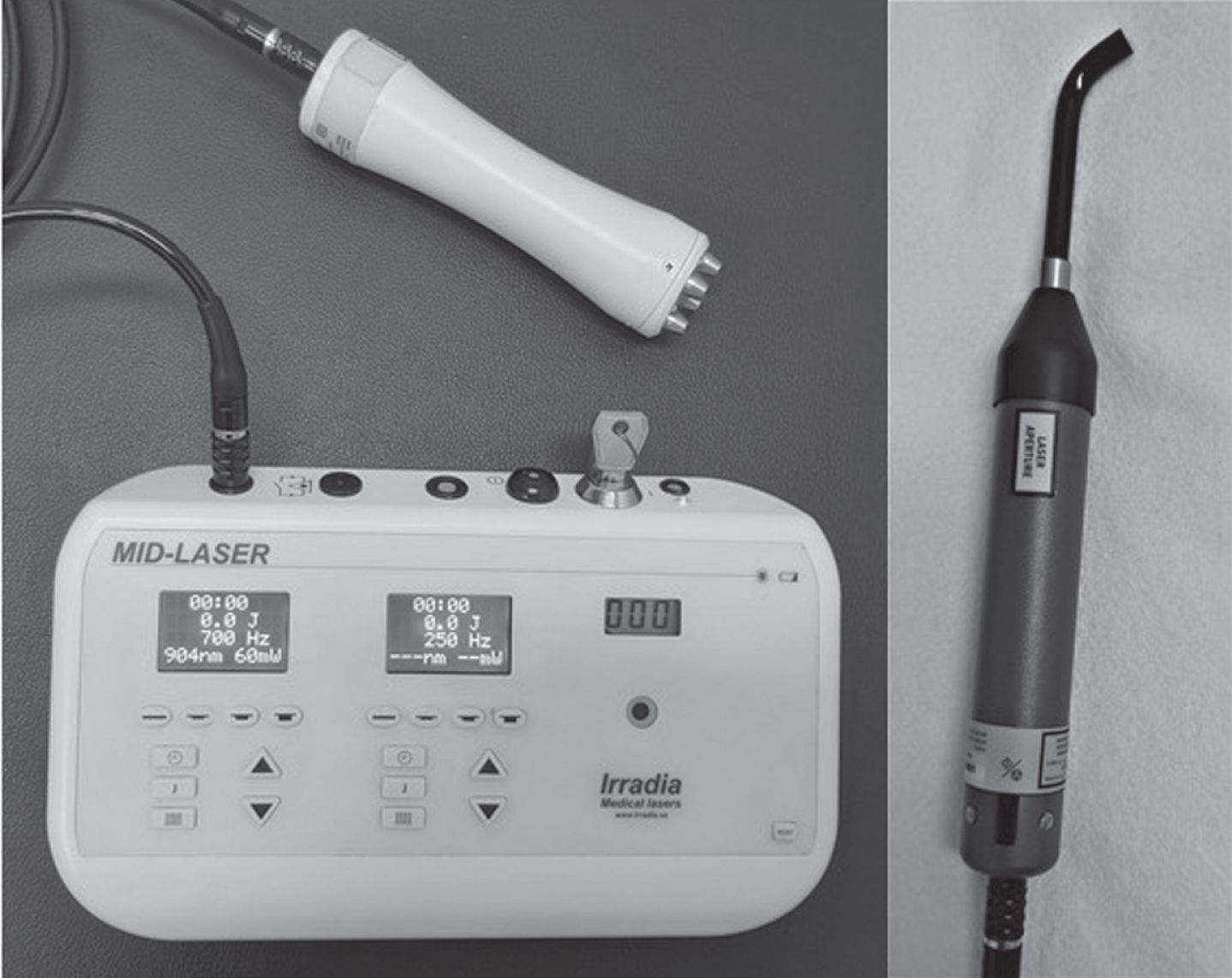
The PBM device used for transcranial and intra-oral applications.
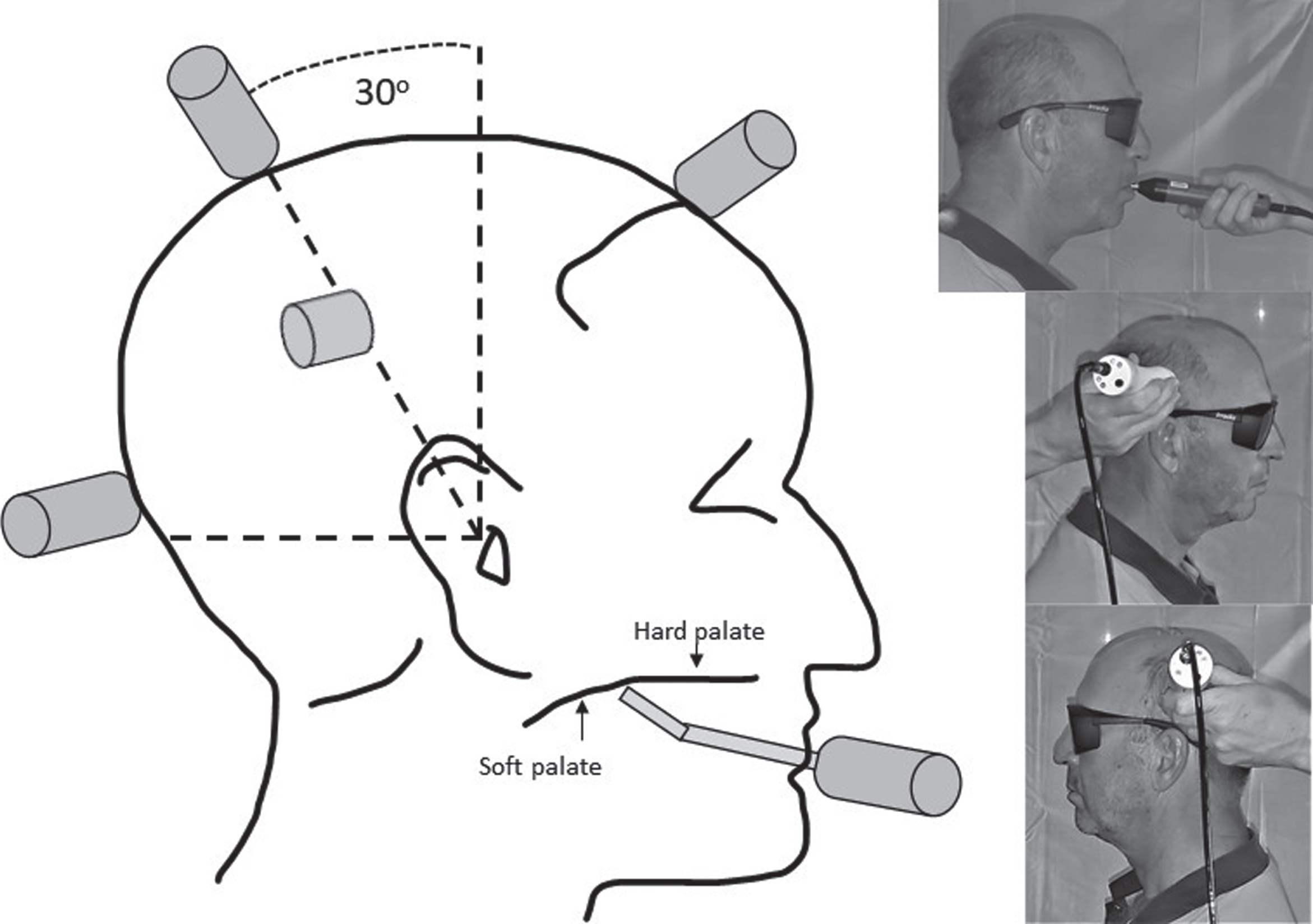
Lateral cranial and intra-oral application points for photobiomodulation (4-diode array to: left and right mid-parietal region at 30 degrees from vertical (as measured from external acoustic meatus); single diode with angulated extension to central soft palate at transition from hard to soft palate).

Midline cranial application points for photobiomodulation (4-diode array to: central sagittal suture line at 30 degrees from vertical, central frontal region at hairline, central occipital protuberance).
Outcome measures
All physical outcome measures were conducted at four time points: T1 - baseline (pre-intervention); T2 - end of first 4-week intervention period; T3 - end of 4-week wash-out period; and T4 - end of second 4-week intervention period. The time of day of testing as well as medication was controlled. For each participant, all four assessment appointments were scheduled at the same time of the day, and all were asked to delay their morning Parkinson’s disease medication until after outcome measure testing was completed to ensure each participant was in their “off” medication period at the time of the assessment. Participants attended with their carers to each outcome measure appointment.
Objective measures were collected that included two upper limb performance measures and two lower limb performance measures. These tests had been validated in previous research for use in Parkinson’s disease, and/or had been correlated with MDS-UPDRS ratings by other authors. As it was important to understand the participants’ capacity to comprehend instructions, the Montreal Cognitive Assessment (MoCA) scale was assessed at the start and end of the study. Additionally, several other outcome measures were collected with specialist examiners including all domains of the MDS-UPDRS, the 39-item Parkinson’s Disease Questionnaire (PDQ-39) and the Parkinson’s Disease Sleep Scale (PDSS). The data from these instruments are not presented in this paper due to unexpected poor inter-rater reliability (MDS-UPDRS), or minimal differences being noted (PDQ-39 and PDSS).
Objective upper limb outcome measures
Firstly, the 9-hole peg test was evaluated as an indicator of hand dexterity and upper limb function as described by Gammon et al. [33]. Secondly, the Spiral (writing) test (as described by Saunders-Pullman et al. [34]) evaluated upper limb tremor as participants were asked to trace within the boundaries of a pre-drawn spiral from the center outwards using the unsupported dominant hand.
Objective lower limb outcome measures
The Timed-Up-and-Go test was evaluated and is well-described, reliable and an easy to administer clinical measure of mobility in people with Parkinson’s disease [35]. As disorders of the basal ganglia affect balance and postural control, we also chose to assess the Dynamic Step Test as described by Smithson et al. [36]. This test is a simple, easy to administer and repeatable clinical test.
Cognitive
The MoCA scale is a widely used and easily administered screening tool for mild cognitive impairment with established reliability and validity [37].
The study was approved by an ethics board of the appropriate Australian National Health and Medical Research Council and met the requirements of the National Statement on Ethical Conduct in Human Research (Mater Misericordiae Limited HREC 18/MHS/26). The study was conducted from June to September in 2018.
Data analysis
Baseline and changes in pre-specified outcome measures (Post-Pre) were compared between groups using Student’s t-tests. Changes in outcome measures from 1st treatment and from 2nd treatment within patients were compared using paired t-tests for each group separately. p-values were not adjusted for multiple testings. Stata 15 was used for all analyses.
RESULTS
Power output measures of the PBM device remained stable throughout the study.
Demographic indicators
Table 4 describes the participant characteristics at the time of their recruitment to the study. Due to difficulties in transport and time demands, one participant in Group 2 withdrew after participating in Phase 1. A second participant passed away due to comorbidity (Chronic Obstructive Airways Disease) during Phase 1. All other participants completed all phases of the study; however, one participant had fallen prior to the final assessment in Phase 3 and was unable to complete the lower limb objective measures. While randomly allocated participants in Group 1 were slightly older than those in Group 2, the difference was not significant (p = 0.30). The stage of disease as indicated by Hoehn and Yahr scores was similar between groups.
Participant characteristics at time of randomization
Data are presented as n (%) or mean (standard deviation).
Performance measures: Overall
Table 5 demonstrates the means and standard deviations for each group over the four measurement time points. The MoCA score remained stable between entry to and exit from the study for all participants.
Means (Standard Deviation) of outcomes at each time point for each group
Data are presented as mean (SD). 9-HPT, 9-hole peg test (DH, Dominant Hand; NDH, Non-dominant Hand); TUG, Timed-Up-and-Go test; SWT, Spiral (writing) test; DST, Dynamic Step Test (DST RLS, Right Leg Stance; DST LLS, Left Leg Stance. [T1, baseline (pre-Phase 1); T2, end of treatment Phase 1; T3, end of wash-out Phase 2, and before commencement of Phase 3; T4, end of treatment Phase 3].
Table 6 demonstrates the statistical comparisons in physical outcome measures for each group at different time points. The first comparison is from the baseline measure (T1) to the end of the first 4-weeks of treatment (T2). The comparison highlights the difference in outcome measures for the placebo (Group 1) versus thrice weekly active PBMt (Group 2). The second comparison in Table 6 highlights the difference for twice weekly active PBMt (Group 1) and once weekly active PBMt (Group 2). The third comparison highlights the difference in outcome measures for each group between baseline (entry to the study) and exit from the study after the second 4-week period of treatment. While no statistically significant differences were found in these comparisons rsome data met published minimal clinically important differences (MCID) and for this reason rfurther exploration of the data was warranted.
Mean difference (Standard Deviation) between time points for each Group
Data are presented as mean (SD) and tested using student t-tests.[9-HPT r9-hole peg test; TUG rTimed-Up-and-Go test; SWT rSpiral (writing) test; DST rDynamic Step Test (RLS right leg stance and LLS left leg stance). T1 rbaseline (pre-Phase 1); T2 rend of first 4-week treatment Phase 1; T3 rend of wash-out Phase 2 rand before commencement of Phase 3; T4 rend of second 4-week treatment Phase 3.
Upper limb
Figures 4 5 illustrate the upper limb outcome measures of motor skills assessed at each assessment time point for each group. An upward slope from left to right in the trend line represents increased time to complete the tests (i.e. rreduced performance) rand a downward slope represents a reduced time to complete the tests (i.e. rimproved performance).
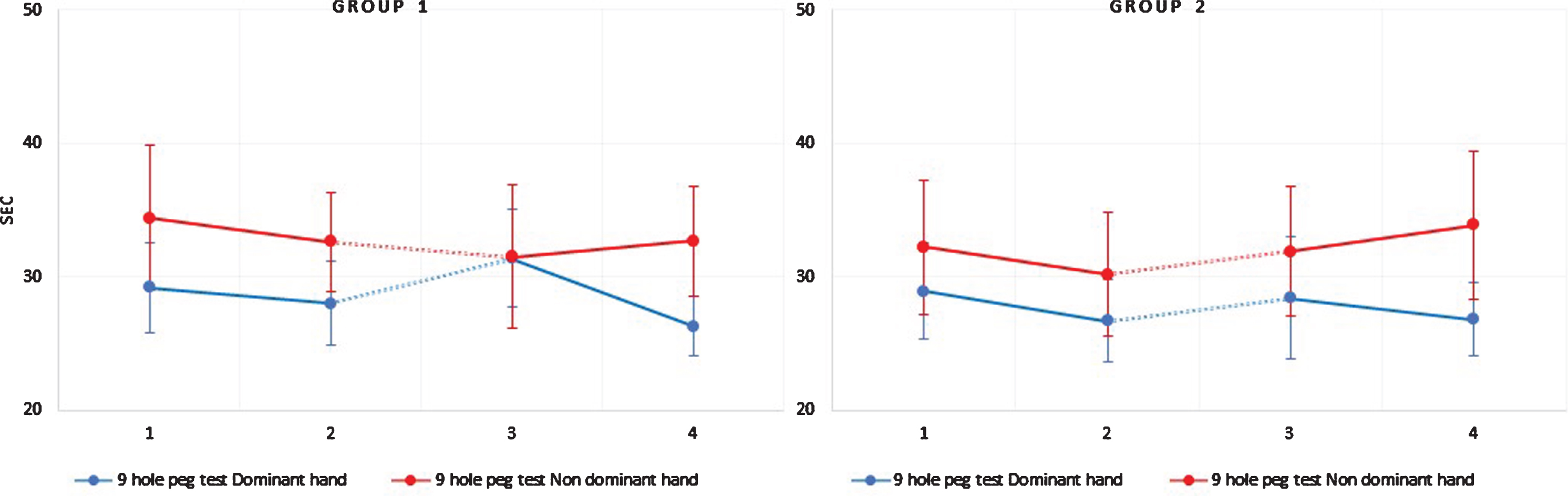
Mean of upper limb outcomes, 9-hole peg test for dominant, and non-dominant arms (with 95%CI at each time point by group). Dotted lines between T2 –T3 indicate the wash-out period for each group. T1: baseline (pre-intervention); T2: end of first 4-week intervention period; T3: end of wash-out period; T4: end of second 4-week intervention period.] T1-T2 = Phase 1; T2-T3 = Phase 2; T3-T4 = Phase 3.
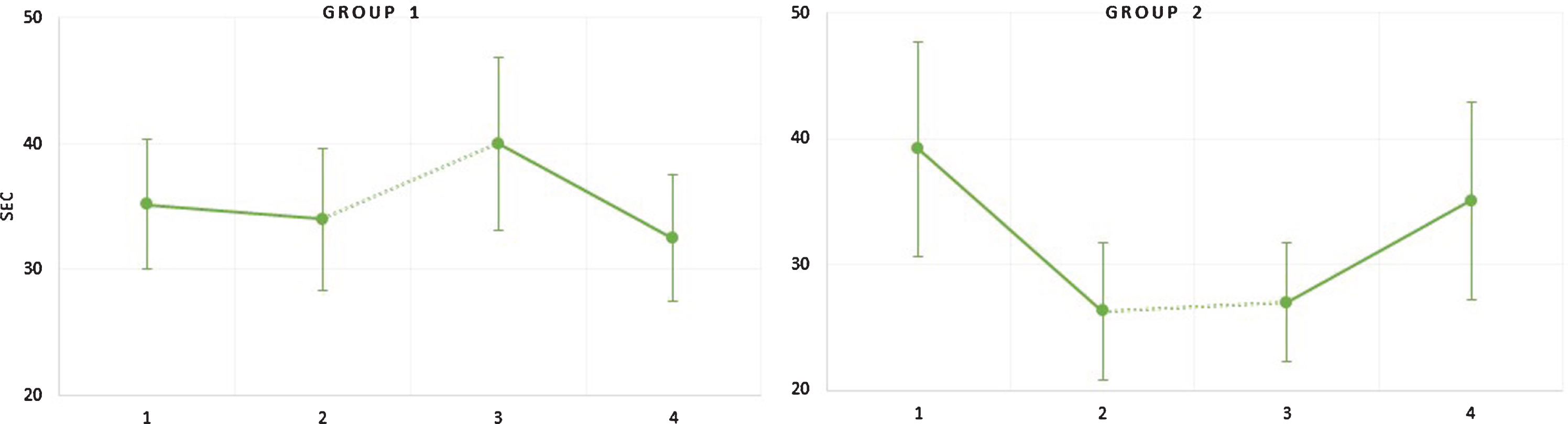
Mean of upper limb Spiral Writing Test outcomes (with 95%CI at each time point by group). Dotted lines between T2 –T3 indicate 4-week wash-out period for each group. [T1: baseline (pre-intervention); T2: end of first 4-week intervention period; T3: end of wash-out period; T4: end of second 4-week intervention period.] T1-T2 = Phase 1; T2-T3 = Phase 2; T3-T4 = Phase 3.
9-hole peg test
Both groups showed some improvement in the speed of completion of this test for the dominant hand during all phases. Based on published data [38], the 16%reduction in time to perform the test with the dominant hand in Group 1 when treated twice weekly with PBMt (in second 4-week treatment period), showed a MCID not evident during the earlier 4-week placebo treatment period, nor for the non-dominant hand in this group. Although there was minor improvement in the test (dominant hand) in Group 2 who received active PBMt in both treatment phases, the amount of improvement was not enough to be considered clinically nor statistically significant.
Spiral writing test
No published data regarding MCID or age-referenced normative data was found for the spiral (writing) test. Although not statistically different, Group 1 participants (who received placebo treatment during the first 4-week intervention phase) when treated later with twice weekly active PBMt demonstrated a 7.5-s reduction in time to complete the test without errors, which was markedly better than with the same group’s response after placebo treatment. Group 2 participants demonstrated even greater improvement in this upper limb functional instrument (12.9-s improvement) when treated 3 times/week during the first 4-week treatment period, but this outcome was reversed when active treatment reverted to only once per week in the second treatment period.
Table 6 displays the student t-test results comparing the change in outcomes between the start and end of the second 4-week phase of treatment (when Group 1 received twice weekly active treatment, and Group 2 received once weekly active treatment). Overall, the results suggest that upper limb fine motor control as expressed through the spiral (writing) test was improved with twice and thrice weekly active treatments. Moreover, the group that received active treatment in both treatment phases of the study demonstrated a slowing of speed in the spiral test (on average by 8.1 s) when treatment was reduced to 1 active treatment per week. The statistical comparison in the response of each group was close to significant (p = 0.056). Group 1 participants who received placebo treatment (thus no active treatment over the first 8 weeks of the study) demonstrated a decline in performance of the spiral test between baseline and the end of wash-out period (Fig. 5). By the end of the study, when Group 1 had received 2 x weekly active treatments for 4 weeks, their performance had improved such that the average time to complete this instrument was reduced by 7.1 s.
Lower limb
Timed-Up-and-Go test
As expected, the participants in each group were predictably slower than age-referenced norms for the Timed-Up-and-Go test [39], although Group 2 participants who received active treatment throughout, were approaching the age-referenced norm by the end of the study. As a reference, we used the 3.5-s MCID calculated by Costa-Ribeiro et al. [40] for the test in a participant group with Parkinson’s disease. Although there was improvement in time taken to perform the test in both groups, at the end of each intervention phase, the difference in time taken to perform the tests was not clinically nor statistically significant (Table 6). For both groups the time taken to complete the test improved between pre- and post-measures in each intervention phase; however, for Group 1 (placebo), the improvement is marginal and performances deteriorate by an average of 2.2 s during the wash-out phase (i.e., over the first 8 weeks without active PBMt, there is a decline in performance overall in this group). Conversely, Group 2 which received some active treatment in each intervention phase maintains its gains in test scores during the wash-out period (Table 5). Mean values for Group 2 indicate a major clinically important improvement (MCII) as defined by Wright et al. [41], whereas Group 1 scores at the end of the second intervention phase return to Baseline levels.
Dynamic step test
The results of the dynamic step test at each assessment point were not markedly changed although there was steady overall improvement in this outcome measure between baseline entry to the study and the final assessment in Group 2 participants who received PBMt in both treatment phases of the study.
DISCUSSION
The interest in using PBMt for managing symptomology in Parkinson’s disease has increased in recent years since the publication of animal research and case reports by other researchers. Ours is the first known prospective, randomized, placebo-controlled off-label study to compare intra-oral plus transcranial PBMt at 904 nm with sham PBMt utilizing different application regimen in a clinical study of people with Parkinson’s disease. Despite the small participant numbers, this pilot study achieved its aims of examining whether PBMt could influence physical performance measures over a 4-week period of PBMt application; and establishing whether the frequency of treatment was likely to be a factor in initiating clinical change. We utilized a large battery of tests, none of which demonstrated statistically different effects between groups, but some showed trends towards clinical improvement. When the results are viewed together, examined according to group, and compared between baseline and end of study, the spiral (writing) test (related to fine motor control and tremor) and the dynamic step test (indicative of lower limb dynamic stability) instruments were most sensitive to change in recruited participants, and are suggestive of being influenced by PBM in a positive direction. When the results are evaluated against limited published MCID data, the nine-hole peg test also demonstrated change worthy of further investigation in a larger, adequately powered clinical trial. We have also shown that there is a placebo effect of PBMt in humans that requires further investigation. Cognition as measured using the MoCA did not change between the start and end of the study.
For the spiral writing test, PBMt twice and thrice weekly over 4 weeks resulted in a marked reduction in time to complete the test when carried out using the dominant hand, results not observable in the placebo treatment period or when active treatment was applied only once per week. Our findings support case reports (e.g., [29]) suggesting that handwriting (as a reflection of fine motor skills) is beneficially influenced by regular application of transcranial PBMt. Hamilton et al. [42] suggested that PBMt over long periods (months) of application prevented expected deterioration in handwriting. In a Letter to the Editor, Santos et al. [43] reported a randomized, assessor blinded and sham controlled study examining twice weekly treatment for 9 weeks using red light emitting diode at 670 nm applied in alternating fashion to the temples of people with Hoehn and Yahr Stage 1–2 Parkinson’s disease. These authors utilized a sham protocol that included a short period of PBM irradiation, thus it cannot be considered a true placebo. Outcomes were measured during the medication “on” state thus potentially confounding the results. Participant numbers were slightly fewer than in our study. The 10 m walk test (fast rhythm) was the only outcome to show statistically significant improvement although the Timed-Up-and-Go test demonstrated the potential for improvement. Due to the marked differences in the protocols between this study and ours, it is not possible to effectively compare the results although it is interesting to note that tests of gait and balance appeared to be influenced by the applied PBM protocol. This finding reflects outcomes seen in other Australian studies of PBM in people with Parkinson’s disease in which one of the authors has been involved (Laakso, personal communication). Our results confirm that regular use of transcranial PBMt may be necessary to induce and/or maintain improvement in indicators of fine motor skills. The specific dosing aspects require further refinement and testing in adequately powered randomized, placebo-controlled clinical trials.
Although regular use of PBMt may be necessary to maintain improvement in some physical indicators, the results of the wash-out period in our study do not support observations that the effect of PBMt regresses significantly once regular application is interrupted. Saltmarche et al. [17] demonstrated a significant deterioration in cognitive scores and mental state toward baseline once 12 weeks of daily transcranial and intra-nasal PBMt was ceased in a group of participants with Alzheimer’s disease. This result may reflect different PBMt exposure parameters. In our study, there was minor deterioration in the nine-hole peg test and spiral writing test scores during the wash-out phase in Group 2 participants (who received active treatment) which did not become noticeable until the final assessment when one active treatment per week was not enough to mitigate deterioration in performance. As improvement in outcome measures in our study was not especially obvious, deterioration would not be expected to be especially noticeable either.
The dynamic step test results were more definitive than the nine-hole peg test and spiral writing test suggesting that 4 weeks of PBMt may have greater influence on lower limb balance than upper limb fine motor control. In Group 2, treatment with active PBMt three times per week and then once per week after the wash-out phase resulted in progressive improvement in the step test for both the dominant and non-dominant legs. These data support published outcomes in individual cases where speed and fluency of walking improved with treatment over many months [42]. Although our results were not reflected in the other measures of lower limb performance (including gait) they were clearly different to placebo and twice weekly active treatment. To our knowledge, the dynamic step test has not been used previously to evaluate the effect of transcranial PBMt in people with Parkinson’s disease although Maksimovich [44] reported improvements in functional activities of daily living (measured with the Barthel Index) in people with vascular parkinsonism after treatment with intracerebral transcatheter laser (633 nm) irradiation. Good dynamic balance would be required for some of the Barthel Index sub-scores, but these were not reported by the author. Of all the tests used in our study, the dynamic step test appears to have been influenced most markedly (although not statistically significantly different) by transcranial and intra-oral PBMt and would be worthy of further investigation.
Having noted a placebo effect in Group 1 participants, the performance measures of this group largely regressed during the wash-out period, more so than the group that received PBMt thrice weekly in Phase 1 and who, during wash-out, appeared to maintain changes in nine-hole peg test, spiral writing test and step test. When Group 1 participants received twice weekly active treatment in the second 4-week intervention phase, the nine-hole peg test (dominant hand) and spiral writing test outcome measures improved to a greater degree than during the placebo phase. Group 2, as noted earlier, did not benefit from one dose per week in the second 4-week intervention phase. These results support the notion that PBMt needs to be applied at least 2 to 3 times per week for at least four weeks before some improvement in outcome measures becomes clinically observable. Treatment for a longer duration of time and perhaps more often each week might be more beneficial, but this hypothesis would need further testing.
Knowledge regarding the molecular and cellular mechanisms of PBMT is increasing and de Freitas and Hamblin [45] have provided a detailed overview of these factors. Others have speculated on the mechanisms of how PBMT influences brain activity. For example, Salehpour et al. [23] listed several molecular and cellular mechanisms that might lead to a range of “brain-specific functional processes” stimulated by brain PBMT including increased synaptogenesis, blood flow, neuron progenitor cells and neurotrophins. The current study was not designed to evaluate mechanisms of action.
Several factors related to the PBM parameters may have had a bearing on the results of this study. We chose to use 904 nm wavelength and 2 J energy per application point based on results observed clinically by one of the researchers, by device availability including availability of a sham device, and its relatively high power output compared to other devices available to us. Published data in a rodent skin model suggests that 904 nm has deeper penetration than some other infrared wavelengths [46], although this last assertion was refuted in work by Anders and Wu [47] also in a rodent soft tissue model. In a review of the literature, Salehpour et al. [48] highlighted that penetration of light through the head in animal, human, and mathematical models is subject to many factors including age, the make-up and absorption characteristics of bone and other tissues, and the area of the skull which is irradiated. The authors recommended the use of infrared wavelengths for head applications of PBM, and specifically 810 nm which penetrates deeper in the human head than visible (red) wavelengths. As far as we have been able to ascertain, no studies have assessed human head penetration by 904 nm laser but our recent work using this wavelength has shown promise in people with Parkinson’s disease. Even though anatomically, the basal ganglia and substantia nigra are theoretically more accessible via an intra-oral pathway, we recognize that in using the intra-oral irradiation site rather than an intra-nasal approach, for example, the percentage of light transmitted within the cranium may have been less than desirable [49]; however, the device we used did not permit a feasible intra-nasal application at the time of the study.
Based on the work of Yue et al. [50], we decided to use a 4-diode laser array to aid with increased intracranial photon flux. The insights of Salehpour et al. [23] suggest that pulse frequencies between 1 and 100 Hz are advisable for cranial irradiation. We chose 50 Hz as a suitable resonant frequency to stimulate change as it was close to the 40 Hz gamma frequency used by Saltmarche et al. [17]. As there is no definitive evidence for optimal brain irradiation sites by PBM, we chose to apply PBMt at cranial points aligned with the work of Saltmarche et al. [17] who had shown benefit in reducing cognitive and behavioral measures in people with Alzheimer’s disease. Those points align with the default mode network which has been shown to have connectivity with the basal ganglia [51]. Salehpour et al. [31] and others have synthesized the literature regarding the molecular effects of PBM in animals with induced or transgenic Parkinsonism, finding a range of effects potentially pointing to molecular mechanisms of action. Our team decided instead to integrate the evolving theory suggested by Naeser’s group (e.g., [52]) that the default mode network is influenced by PBM, and other work suggesting a thalamocortical connectivity [53] which might also be influenced or activated by photonic energy when applied via the intra-oral route. To avoid the possibility of overdoing the number of sessions of PBM which might result in reduced effectiveness [54], we chose to limit the overall treatment to a maximum of 3 treatments/week for 4 weeks. We believed that by doing so, we might be able to identify a minimum period of treatment required for detecting change in the outcomes measured, thus providing further guidance for future clinical application. Although efforts have been made to synthesize the literature regarding parameters for use in brain irradiation with light, all of these factors remain to be adequately investigated and combinations of different parameters need to be explored.
Strengths and limitations
No randomized and effectively placebo-controlled study has previously attempted to evaluate the effect of 904 nm PBMt on outcome variables in people with Parkinson’s disease when treated using a combination of transcranial and intra-oral methods of application. Given the variability of how Parkinson’s disease presents in individuals, the variation in our findings is not unexpected. Based on recent findings by Horsager et al. [55], the brain-first/body-first sub-types of Parkinson’s disease may have had some bearing on the outcomes. Future studies may need to ascertain such sub-groupings in the recruitment of participants in order to apply the most appropriate treatment method and application site. More likely however, is the influence of ‘dose’ (and specifically the regularity and duration of treatment) on the participant. Twice and thrice weekly treatment demonstrated changes in some measures that were similar to minimal clinically important change in other studies and, if one were able to extrapolate, may have continued to do so if the treatment had continued beyond 4 weeks. We capped our intervention time at 4 weeks as the burden in time for participants to attend a clinic 3 times per week for a total of 8 weeks was judged as being reasonable. Future studies that include participant self-administration of PBMt at home may alleviate the burden of attending a clinic and allow longer treatment time and longer-term follow-up of different treatment and assessment protocols. As a pilot, this study proved to be under-powered, but our paper has contributed to the understanding of the degree of the placebo effect and the positive effect that it demonstrates in people with Parkinson’s disease. Studies proposing to use placebo PBMt in their protocols may find these data of value. We suggest that enough information is now available from published case series and pilot studies that future research in this field is warranted including randomized, placebo-controlled clinical trials.
CONCLUSION
This pilot study is the first to use a combination of transcranial and intra-oral 904 nm PBMt in people with diagnosed Parkinson’s disease in a participant and assessor-blinded, randomized, placebo-controlled study of 4 weeks’ duration with a maximum of 3 doses/week (total of 12 treatments), a wash-out period of 4 weeks and a further intervention period. While no statistically significant differences were identified, some MCID were identified. Upper limb spiral writing test and nine-hole peg test, and the lower limb dynamic step test appeared to be most sensitive to change. Future studies should evaluate longer periods of PBMt application (at least 3 times/week for more than 4 weeks) and longer follow-up period.
Footnotes
ACKNOWLEDGMENTS
Cromwell Property Group Foundation and Dolben Inc. for philanthropic funding to support clinical backfill of researcher time.
Active Rehabilitation Foundation for in-kind administrative support of the project.
Mr. John Fitzgerald and staff of Active Rehabilitation Physiotherapy Pty Ltd for in kind support of team members and resources, use of facilities and administrative assistance.
Dr. Ann Liebert and Dr. Dan Johnstone for valuable ongoing discussions regarding potential dosing parameters; in addition, we wish to acknowledge the work in animal models of Profs. Jonathan Stone and John Mitrofanis that assisted the protocol development for this project.
Irradia Australia for assistance in provision of intra-oral and placebo devices.