
Abstract
Background
Dance combines cultural and aesthetic elements with behaviors important for brain health, including physical activity, social engagement, and cognitive challenge. Therefore, dance could positively impact public health given the rapidly aging population, increasing incidence of Alzheimer’s disease and related dementias, and lack of uptake of exercise in many older adults. Despite a high volume of literature, existing literature does not support evidence-based guidelines for dance to support healthy aging.
Objective
To conduct a scoping review of the dance intervention literature in older adults and provide information to facilitate a more consistent approach among scientists in designing dance interventions for older adults that stimulate physical and neurocognitive health adaptations.
Methods
Study characteristics (sample size, population, study design, outcomes, intervention details) were ascertained from 112 separate studies of dance reported in 127 papers that reported outcomes important for brain health (cardiorespiratory fitness, balance and mobility, cognition, mood, and quality of life).
Results
High heterogeneity across studies was evident. Class frequency ranged from < 1 to 5 classes per week, class length from 30–120 minutes, and intervention duration from 2 weeks to 18 months. Studies often did not randomize participants, had small (< 30) sample sizes, and used varied comparator conditions. Over 50 tests of cognition, 40 dance forms, and 30 tests of mobility were identified.
Conclusions
Based on these results, important future directions are establishing common data elements, developing intervention mapping and mechanistic modeling, and testing dosing parameters to strengthen and focus trial design of future studies and generate evidence-based guidelines for dance.
Keywords
INTRODUCTION
In 2003, epidemiological evidence showed that dance was the only leisure time physical activity (PA) associated with reduced risk of developing Alzheimer’s disease and related dementias (ADRD). 1 Dance is a multidimensional activity combining physical, artistic, and cultural elements that uniquely stimulates mind-body connection, encourages multi-planar movement, and may elicit creativity.2,3 Dance also incorporates many targets of interventions aimed at improving or maintaining neurocognitive health with aging, such as increasing PA, social engagement, and cognitive stimulation through motor learning, sequencing, memory, spatial awareness, and dual tasking.4–8 Over the past 20 years, research on the effects of dance in older adults, both with and without neurodegenerative conditions, has rapidly advanced. Still, the state of the science does not yet provide a level of evidence for a dance “prescription” and there are many interesting open questions about what constitutes the “medicine” of dance.
Exercise is medicine
Strong evidence supports the idea that PA is important for maintaining and improving neurocognitive and physical health in older adults, including those with neurodegenerative diseases such as ADRD. Cross-sectional evidence shows that older adults with slowed gait, 9 low cardiorespiratory fitness (CRF),10,11 hypertension,12,13 or metabolic disease14–16 (all factors directly impacted by PA) are at higher risk for ADRD. Furthermore, individuals who meet recommended PA targets have lower amyloid17,18 and tau burden 19 and risk of developing dementia.20–22 Engaging in PA benefits neurocognition in older adults, 23 evidenced through maintained or improved cognitive performance, especially in the executive function domain;24–33 improved or maintained brain volumes;34–37 increased cerebral blood flow;38–40 increased serum brain-derived neurotrophic factor 41 that is correlated with hippocampal volume; 42 and altered functional brain networks, including improved connectivity43,44 and modular structure of the brain.39,45 Previous research indicates that aerobic exercise may improve cognition in people with mild cognitive impairment (MCI) or Alzheimer’s disease (AD)46–48 (but also see 49 ). In short, PA is a potent lifestyle medicine, as illustrated by international uptake of the “Exercise is Medicine” initiative. 50
The “Exercise is Medicine” initiative arose from evidence that engaging in and maintaining moderate to vigorous intensity PA might attenuate the effects of ageing through maintained or improved CRF (e.g., 51 ) as well as through mechanisms mentioned above. PA-promoting interventions tested in older adults have traditionally focused on exercise, defined as structured PA of at least moderate intensity with the express purpose of improving health or fitness. 52 Importantly, as highlighted in the Physical Activity Guidelines Advisory Committee report, 53 which informed the current Physical Activity Guidelines for Americans, 54 the health benefits of aerobic PA accrue regardless of the intent of activity; exercise does not produce unique health benefits relative to other physical activities such as active transport, work around the home, or dance. Moreover, structured exercise is a poor fit for widespread and lasting activity behavior change. For instance, increases in aerobic activity following exercise interventions are rarely maintained one year or more post-study intervention 55 and maintenance of PA is believed to be necessary for continued benefit.
Dance as a unique means of engaging in PA
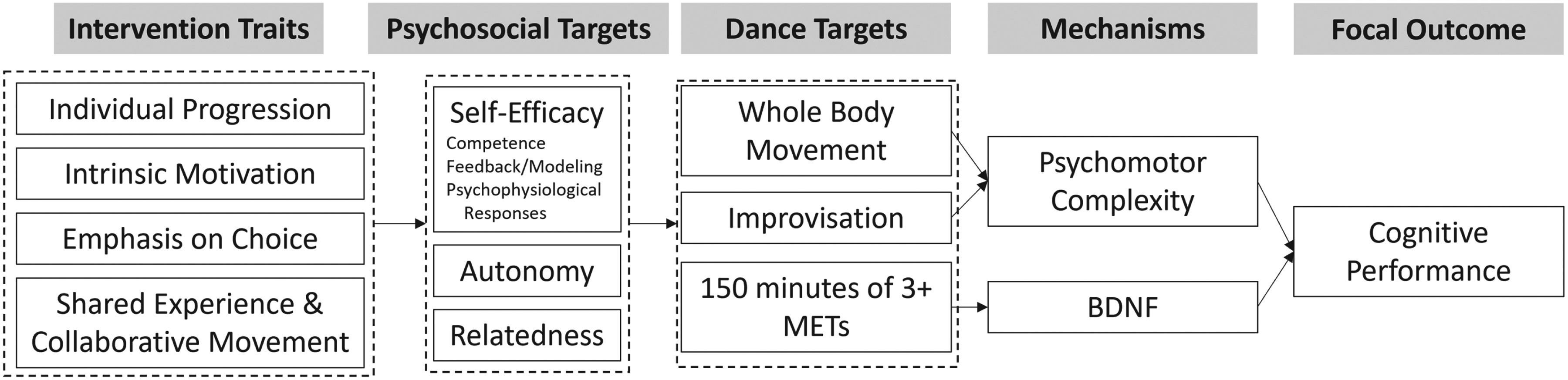
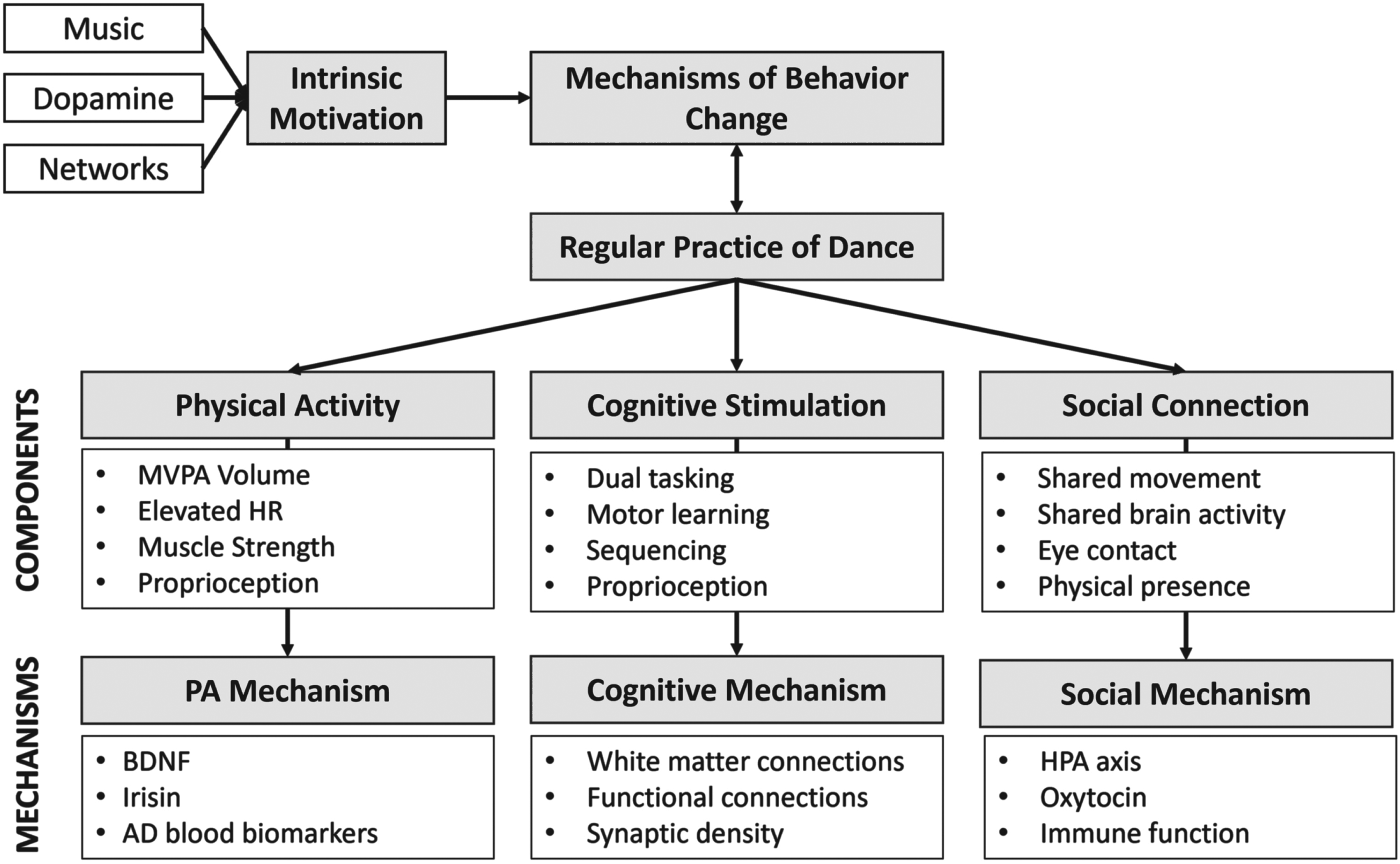
One challenge in promoting dance as a form of PA to promote healthy brain and body aging is gaps in knowledge about 1) the active components of dance as an intervention and 2) “dosing” of dance. “Active components of dance” refers to the traits of an intervention that lead to desired health and behavioral outcomes; essentially the “medicine” of dance. For example, Figure 1 shows an intervention map, a strategy for illustrating the hypothesized relationships between potential active components of dance to health outcomes of interest for aging. “Dosing” refers to an understanding of key characteristics of the dance intervention, including cardiovascular intensity, class length (minutes), class frequency (number of classes per week), and intervention duration (length of participation in weeks) needed to attain the outcome of interest.56,57 Establishing a health-enhancing dose is complicated by the fact that dance affects multiple outcomes of interest simultaneously, such as balance, CRF, cognition, and depression. These outcomes may be associated with different active components or require different doses to achieve a measurable change. For example, measurable changes in CRF may occur more rapidly than measurable changes in cognition. The diversity of methods and outcomes used in dance literature also reflects the diversity of different fields of study interested in dance, as well as the varied populations for which dance may be beneficial. This heterogeneity in turn creates challenges for understanding the effects of dance on key outcomes and designing new studies for older adults that aim to definitively assess the multimodal effects of dance on physical and neurocognitive health.
Aims of this review
There are many good systematic reviews of dance that have summarized the effects of dance on specific outcomes.58–69 Because the purpose of systematic reviews is to reliably synthesize results across studies, they are restricted to studies that minimize bias, meet rigorous reporting requirements, and are homogenous enough in the populations targeted and outcomes measured that results can be combined. One consequence of the rigor of these reviews is that they are not very inclusive; most have paper sample sizes of 22 or less, and many include samples as small as 5. As an example, McNeely and colleagues found 218 studies of dance in older adults but only 20 met requirements for review. 60 This means that the characteristics of studies included in these reviews are likely not representative of the dance literature as a whole. We feel this is important because despite the voluminous literature about the effects of dance in aging, there are few definitive recommendations that can be generated. Our hypothesis is that the reason for the mismatch between the volume of dance literature and lack of definitive recommendations is because of the heterogeneity of methods, populations targeted, intervention characteristics, and outcomes. Therefore, the overall aim of this review was to summarize the scope of the existing literature of dance interventions in older adults that reported on outcomes important for brain health, specifically CRF, balance and mobility, cognition, mood, and quality of life. We aimed to ascertain the heterogeneity of published studies in key study characteristics including sample size, class frequency, class duration, intervention duration, outcomes assessed, forms of dance used, randomization, and comparator groups. Such information may facilitate a more consistent approach among scientists in designing dance interventions for older adults that stimulate physical and neurocognitive health adaptations.
METHODS
Search strategy
The search strategy for this scoping review was developed by following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) protocol and the extension for scoping reviews for the search, summary, and reporting70–72 as well as additional guidance on selecting a review methodology, 73 synthesis without meta-analysis, 74 and chapters from the Cochrane Handbook for Systematic Reviews of Interventions.75–80 The following eligibility criteria were established in accordance with the PRISMA-PICOS framework: population, interventions, comparators, and outcomes. Figure 2 demonstrates the identification, screening, and inclusion process for studies in this review.
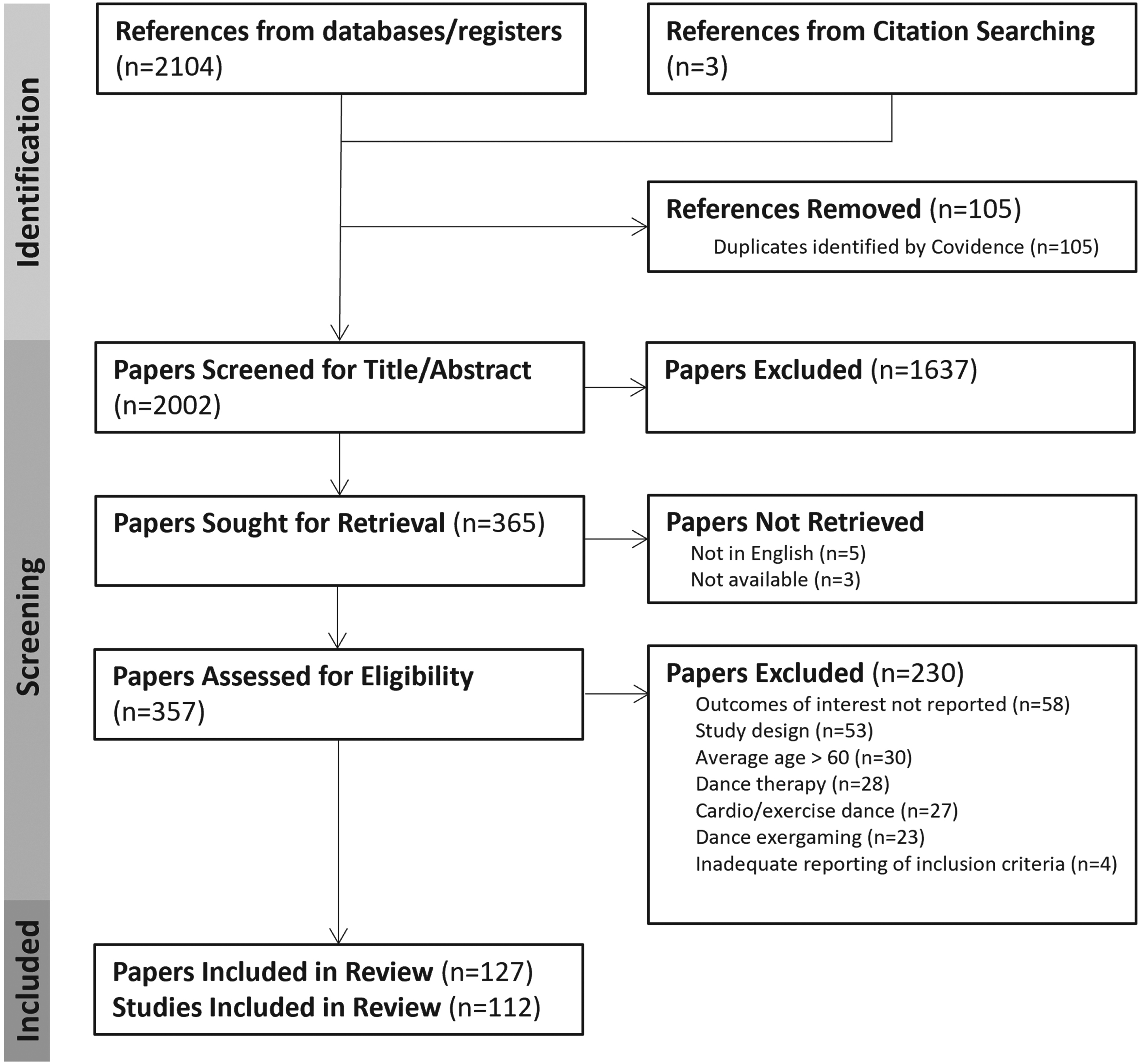
PRISMA Inclusion/Exclusion Diagram.
Criteria for inclusion/exclusion
Inclusion and exclusion criteria for papers in this review were guided by the aim to assess outcomes of participation in dance interventions for older adults. Only articles that could be found in English were used in this review. As the population of interest was older adults, studies where the average age of all participants was less than 60 were excluded. Studies were not restricted by disease categories if age and study design criteria were met. Therefore, this review includes studies focused on healthy older adults as well as those with chronic diseases, metabolic diseases, Parkinson’s disease (PD), and cognitive impairment.
Because the focus was on effects of dance interventions, only studies that measured outcomes of interest at baseline and follow-up were included. Cross-sectional studies, case studies, observational studies, and other reviews were excluded from this review. Randomization was not required for a study to be included in the review. All forms of dance and all settings of dance classes were included. Dance classes could be presented at any frequency and for any duration of time. Due to our interest in dance as an artistic practice to improve health rather than as a therapeutic tool, dance therapy interventions were excluded. Similarly, interventions that used exergaming or virtual reality were excluded. Dance fuses physical and cultural practices, with artistry and affect often playing a role. PA, while it may be a by-product of dance, is not the primary goal. For this reason, in cases where the moving-to-music phenomenon was explicitly designed as a “form of exercise” (e.g., Zumba, aerobic dance) it was excluded. Studies that provided dance in addition to other interventions or therapies whose study design did not isolate the effects of dance on older adults were excluded.
Outcomes
Outcomes were selected that are specifically relevant for maintaining brain health and mobility in older adults including cognitive performance (memory, global cognition, and executive functioning), psychological health (mood and quality of life), CRF (peak oxygen consumption (VO2peak)), and physical function (mobility and balance). Within studies reporting these outcomes, features of dance interventions relevant for determining “dosing” recommendations were also selected to be reported, including dance form, number of classes per week, class length in minutes, and duration of dance interventions in weeks. Finally, characteristics of study design were recorded, including sample size, randomization status, whether a study was a pilot study, and comparator groups. Sample size is reported as the number of participants enrolled. Randomization status was defined as yes/no and was determined by whether the study reported randomizing participants. Pilot study status was defined as the study identifying itself in the title or the body of the text as a pilot or feasibility study.
Search strategy
After the eligibility criteria were set, a search of the PubMed database was conducted in May of 2022 using the search terms: older adults AND dance AND cognition OR balance OR mobility OR mood. No start date was specified. The literature search was intentionally broad given the diversity of ways in which dance can be referred to in scientific and medical literature. This search resulted in 2104 possible candidate studies (see Figure 2 for a PRISMA diagram of the article screening process). These studies were then imported to Covidence.org 81 by DT. Covidence is a web-based collaboration software platform that streamlines the production of systematic and other literature reviews. First, 105 duplicate references were removed. Second, two authors (DT and PR) independently screened 2002 articles based on title and abstract to determine whether they met inclusion criteria for study type and age range. This initial screening removed 1,637 articles and 365 articles were evaluated for eligibility based on the criteria listed above. This resulted in the inclusion of 127 total papers, which included studies where multiple papers were written about the same study populations, for example, one paper reporting physical function outcomes and another reporting cognitive outcomes. Thus, the final number of separate studies reported on was 112. Table 1 lists the included studies.
List of all papers included

RESULTS
Study characteristics
The overall sample size of studies included in the review varied widely, from 6 to 424 (Figure 3a). Many studies had small sample sizes: approximately a quarter of the studies reviewed (n = 29, 25.4%) had a total enrolled sample size in all study conditions of 20 or fewer participants, and 41.2% (n = 47) had 30 or fewer total participants. Half of the studies (n = 57, 50%) had fewer than 20 participants in the dance arm of the study. Small sample sizes may reflect the fact that 40% (n = 46) of the included studies identified themselves as pilot or feasibility studies.

Studies had a variety of comparator groups (Figure 3b). The most common comparator group was life as usual (n = 41, 35.9%). Approximately a quarter of the studies (n = 31, 27.2%) had no comparator group at all. The remaining studies included a variety of comparator groups: conventional exercise such as walking, physical therapy, swimming, or exercise/sport classes (n = 15, 13.2%); stretching and mind/body activities such as tai chi (n = 12, 10.5%); education classes/attention control (n = 16, 14.0%); other forms of dance (n = 6, 5.3%) and music appreciation or music instrument learning (n = 2, 1.75%). Participants were randomized to study conditions in approximately half of the total 112 studies (n = 61, 53.5%), which was about 75% of the 83 studies that had comparator groups.
Potential differences in outcomes of dance in older adults may be related to the study populations targeted (Figure 3c). Studies in this review included overall healthy older adults (n = 51, 44.7%), people with Parkinson’s disease (n = 31, 27.2%), and people with MCI or dementia (n = 13, 11.4%). Additional populations include cognitively normal older adults with chronic breathlessness (n = 1), chronic obstructive pulmonary disease (COPD; n = 1), chronic stroke (n = 1), cancer (n = 1), metabolic disease (n = 2), chronic heart failure (n = 2), visual impairment (n = 3), obesity (n = 2), and fall risk (n = 2). Of the 112 studies, n = 10 studies (8.9%) included only women and in n = 37 (33.0%), women comprised 80% or more of the study sample. Five studies (4.5%) did not report sex.
Forms of dance
Another source of heterogeneity in the literature on the effects of dance in older adults is the multiplicity of dance forms tested. The literature review contained 41 different forms of dance listed as the main type of dance by the authors of the included papers (Table 2). Some dance forms listed included multiple specific dance forms, for example, studies that identified the dance form as “ballroom dance” included 5–11 different forms of ballroom dances in one intervention. Counting of each of these forms as an individual form, 68 different forms of dance are represented across the studies. Twenty-one studies used multiple forms of dance in the intervention. Forms included both partnered and non-partnered dance. Supplemental Table 1 organizes dance forms by individual form rather than the term reported by the authors.
Reported forms of dance

“Dosing” parameters: Frequency, class length, duration, and intensity
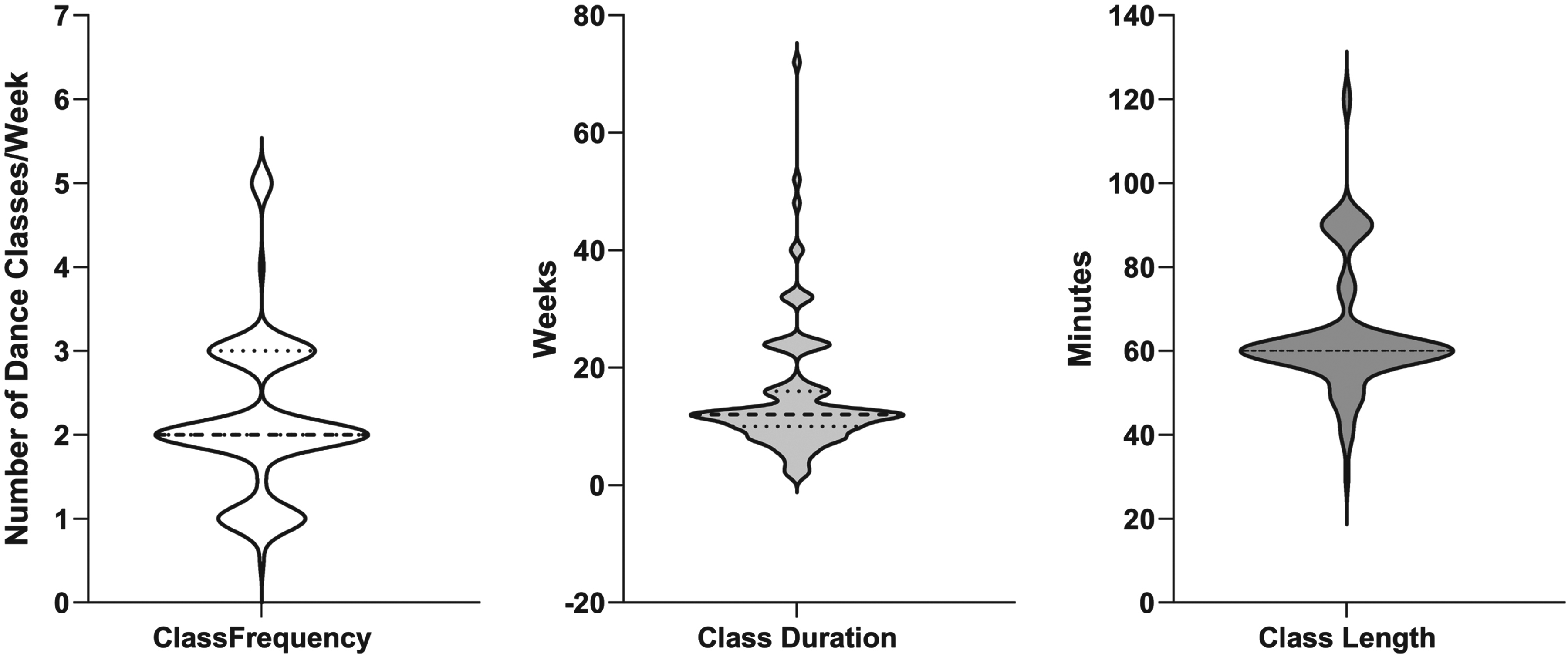
The weekly frequency of dance interventions in the studies reviewed varied from less than once per week to more than 4 times per week (Figure 4). Dance classes were most commonly offered 2x/week (n = 54, 48.2%), followed by 3x/week (n = 27, 24.1%), and then 1x/week (n = 22, 19.6%). Three studies asked participants to complete 1–2 classes per week, and six studies provided class ≥4x/week. Dance classes were most commonly offered for 60 min (n = 63, 56.3%). Some studies ranged in the duration of classes82–85 or asked that participants engage in additional at-home classes.86–89 One study did not report class duration. The duration of the dance interventions varied from 2 weeks to 78 weeks (1.5 years) (Figure 4). The most common duration of dance interventions reported was approximately 3 months (12 weeks, n = 31, 27.6%). The cardiovascular intensity of dance classes assessed via a heart rate monitor was reported in 7 studies (6.25%).83,90–94
Assessments of balance and mobility
Mobility and balance were the mostly commonly measured outcomes in dance studies in older adults. Mobility was assessed in 77 studies (68.8%) using over 30 different measures of gait, lower body strength, and physical function. The Timed Up and Go (TUG) was the most commonly administered test (n = 28, 25.0% of all studies, 36.4% of studies testing mobility). The TUG involves rising from a chair, walking in a straight line, turning, and returning to sit in the chair. The TUG has two additional dual-task variations, the cognitive TUG, which involves performing a cognitive task while completing the movements described, and the manual TUG, in which participants carry a full glass of water while completing the movements. Each of these variations was used in 4 studies (3.6% of all studies; 5.2% of studies testing mobility). The Unified Parkinson’s Disease Rating Scale (UPDRS) is a common outcome measure that is specific to Parkinson’s disease and was administered in 25 of the 31 included studies of dance in people with Parkinson’s disease (80.6% of studies on people with Parkinson’s disease; 22.3% of all studies; 32.5% of studies testing mobility). The 6-minute walk test (6MWT) was the next most commonly administered test of mobility and was used in n = 23 studies (20.5% of all studies; 30.0% of studies testing mobility). The 6MWT measures the distance that can be walked in 6 minutes and is a measure of fitness and endurance. Gait speed was also commonly assessed (n = 20, 17.9% of all studies, 26.0% of studies testing mobility) and was measured walking forward and backward and over distances ranging from 3 to 20 m. Eleven studies used an instrumented mat to test parameters such as variability or cadence in addition to gait speed. Table 3 includes a list of all the mobility measures reported.

Balance was measured in n = 60 studies (53.6% of all studies) using 18 different measures (Table 4). The most common measure was the Berg Balance Scale, used in n = 24 studies (21.4% of all studies, 40.0% of studies testing balance). This may be in part because of its sensitivity to fall risk in people with Parkinson’s disease; 15 of the studies that used the Berg Balance Scale were assessing effects of dance in people with Parkinson’s disease. The next most common outcome was static balance assessed via changes in center of pressure measured with a force plate (n = 10, 8.9% of all studies; 16.7% of studies testing balance).

Self-reported balance and mobility and balance confidence were reported in addition to assessing balance and mobility directly. Nine studies of people with Parkinson’s disease used the Freezing of Gait Questionnaire (8.0% of all studies). For non-disease specific measures, the Activities Specific Balance Confidence Scale was most commonly used (n = 7, 6.3% of all studies). A complete list of the 8 questionnaires used is found in Table 4.
Assessments of cognition
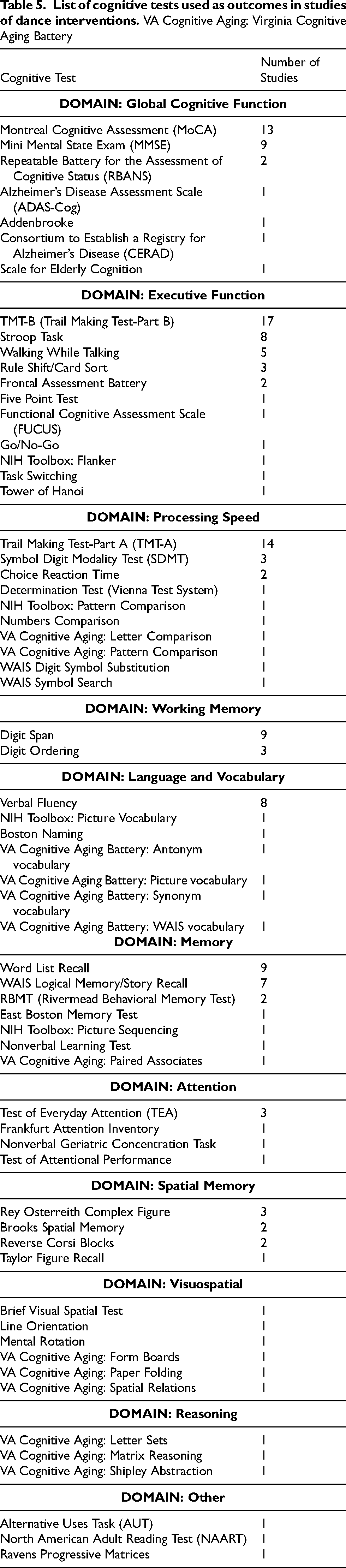
We identified n = 39 studies (34.8% of all studies reviewed) that tested cognition. Most dance studies that reported cognitive data targeted healthy older adults (n = 19; 17.0% of all studies; 48.7% of studies testing cognition) or included older adults with MCI or dementia (n = 11; 9.8% of all studies; 28.2% of studies testing cognition). Fewer focused on people with Parkinson’s disease (n = 7; 6.3% of all studies; 18.0% of studies testing cognition) or metabolic conditions (n = 3; 2.5% of all studies). More than 50 different cognitive tests were used to evaluate dance-induced changes in cognitive domains including global cognition, executive functioning, memory, spatial memory, attention, visuospatial function, working memory, and processing speed. The individual cognitive tests used were quite varied; over 30 tests were used in only one study. Table 5 lists the cognitive tests cited in the reviewed literature. The Trail Making Test (TMT) was the most commonly administered test. The TMT has two parts that can be administered separately. The TMT-B, which tests executive function, was administered in 17 studies (15.2% of all studies, 43.6% of studies testing cognition). The TMT-A is more a test of processing speed and was administered in 14 studies (12.5% of all studies, 35.9% of studies testing cognition). The Montreal Cognitive Assessment (MoCA) was the most commonly administered test of global cognitive function. It was designed as a screening tool for MCI and was administered in 11 studies (9.8% of all studies, 28.2% of studies testing cognition).
Assessments of depression, anxiety, and quality of life
Mood is often hypothesized to change in response to dance because of the social engagement inherent to many dance forms as well as the positive affective impact of light-to-moderate intensity aerobic PA. 95 Depression, anxiety, or mood state was measured in 35 studies (31.3% of all studies). Depression was measured in 27 studies using 8 different measures. The most commonly used tools to measure depression were the Geriatric Depression Scale (GDS), a scale designed for administration to older adults (n = 16, 14.3% of all studies; 59.3% of studies testing depression), and the Beck Depression Inventory (BDI) (n = 6, 5.4% of all studies; 22.2% of studies testing depression). Anxiety was measured in 5 studies using 5 different inventories. Overall mood states were assessed in 4 studies using 4 different instruments.
Health-related quality of life is an important patient reported outcome that can change in response to PA intervention. 96 It is a subcomponent of overall quality of life that is highly salient to older adults and captures key components of mental and physical health. Quality of life was measured in about 40% of studies included in the review (n = 46) using 18 different measures. The most commonly administered quality of life survey was the Parkinson’s Disease Questionnaire (PDQ-39), which was administered in 16 of the 31 studies of dance and Parkinson’s disease that were included. The most commonly administered non-disease specific quality of life measure was the Medical Outcomes Studies 12 (SF-12) (n = 8, 7.1% of all studies), which has a mental and physical subscale.
Assessments of cardiorespiratory fitness
CRF was evaluated in ten studies (8.9% of all studies)94, 97–106 and was estimated by measuring peak oxygen consumption (VO2peak) using a treadmill (n = 5), PA questionnaires (n = 4), or walking endurance from the 6-minute walk test (6MWT; n = 1). Only one study using VO2peak showed a significant increase in CRF relative to control, and one other study showed a significant within-group increase in VO2peak. Two of the four studies that assessed CRF using PA questionnaires showed increased fitness after dance, and the one study that assessed fitness using the 6MWT did not show improvement.
DISCUSSION
The overall goal of this review was to summarize the scope of the existing literature of dance interventions in older adults to ascertain the heterogeneity in study design, outcomes, and populations for the purpose of informing future study design. The studies reviewed included over 40 different forms of dance, 12 different target populations, more than 50 different cognitive tests, over 30 different tests of mobility, and 18 different tests each of balance and quality of life. While collating heterogeneous research yielded a broad pool of studies, we acknowledge that the risk of bias from the authors and studies is a limitation of the review. The high heterogeneity across studies suggests dance as a whole is a robust intervention in aging; however, it also highlights gaps in the literature and opportunities for future research.
Dance intervention characteristics: “dosing” of dance
There is currently not an established understanding of the “dose” of dance necessary to achieve desired outcomes related to brain health, such as improved or maintained CRF and cognitive function. Within the 112 studies reviewed here, key dosing variables varied widely. Weekly frequencies varied from 1 class every 2 weeks to short-duration, intensive practices requiring 5 classes per week. Intervention durations ranged from 2 to 72 weeks and classes could last 30–90 minutes. Intensity of activity is an important component of dosing but is not often reported in studies of dance. Only 6% of the studies reviewed measured intensity objectively using heart rate monitors during classes. The review showed that the most common formula for a dance intervention in older adults was 60-min classes 2x/week for three months. To date, no studies have directly compared various doses of dance to determine the relationship between dose and outcomes. Such research would provide basic information about whether the frequency, intensity, and duration of dance required to achieve optimal benefits is feasible for older adults. This is of particular importance given that dance may have limited public health value if the optimal frequency is not feasible for older adults to maintain or is too costly to deliver in the community. Conversely, should most health benefits associated with dance be attainable through simply achieving a consistent weekly volume of dance behavior, then future dance interventions will have considerable leeway to achieve key health outcomes while also prioritizing fun, scalability, and sustainability. It should be noted that contemporary PA guidelines have adopted just this approach in response to accumulating evidence that most health benefits associated with PA can be achieved through diverse means so long as a sufficient weekly volume is met. Another gap highlighted here is a need for information about the characteristics of different forms of dance. Potentially important characteristics to consider included partnered versus non-partnered, amount of learned choreography, types of movement involved, and intensity.
It is important to emphasize that “dance” describes a highly diverse family of behaviors, and differences across the type and structure of dance class can be expected to affect the mechanisms that drive change in health-related outcomes. As an example, participating in a high-energy African dance form may lead to greater elevation in heart rate and therefore may have a more robust effect on CRF. These effects may differ depending on class duration, proportion of class time spent moving, intensity of activity, frequency of weekly dance sessions, recovery time between sessions, and duration of a program. These parameters may also positively or negatively affect perceptions of stress or restoration, the development of social connection, and perceptions of fun, which may in turn affect both short term physiological benefit and the likelihood of long-term engagement in dance as an activity behavior.
Additionally, responses may differ by the cultural background and other demographic characteristics of the individual. Dance historically has been undertaken for social connection, enjoyment, and cultural engagement. When practiced for these reasons, PA resulting from dance may be considered as a by-product of dance participation. Dance scholar Judith Lynne Hanna defines dance as “human behavior composed of purposeful, intentionally rhythmical, and culturally influenced sequences of communicative nonverbal body movement and stillness in time, space, and with effort” and specifies that every genre of dance has its own aesthetic with standards of appropriateness and competency. 107 These expressive and aesthetic components of dance distinguish it from most typical forms of exercise and may contribute to experiences of enjoyment and meaning attached with dance activity. Even when dance is undertaken for the purpose of health, the health effects may be judged differently. As an example, the Native American Jingle Dress Dance is ritually engaged in to improve the health of an individual or community, rather than the health of the performer.
These considerations highlight the importance of intervention mapping. 108 The process of intervention mapping encourages the researcher to clearly state hypothesized links between key components of an intervention, psychological and physiological mediators, and the targeted outcome of interest. Importantly, this allows design of studies to systematically target intervention characteristics to determine their impact on the outcome of interest. Figure 1 depicts an example intervention map that links traits of a dance intervention to psychosocial mediators of behavior change, which affect uptake and engagement in dance behaviors that in turn drives changes in physiological mediators underlying changes in cognitive performance. Notably, each section of this figure guides both intervention design and measurement selection.
Heterogeneity of study design and outcomes
Previous systematic reviews and meta-analyses of the dance literature have used only a fraction of the published literature. One reason for that may be the heterogeneity of study design and outcomes. In addition to the variability in dosing parameters, studies included a wide range of comparator conditions that we grouped into eight categories and included different aerobic exercise interventions, tai chi and other mindful movement or stretching classes, support groups, education or cultural groups, music classes, music appreciation, waitlist, and life as usual. Approximately 25% of the studies we reviewed did not have a comparator group.
Outcomes within each domain of interest (mobility/balance, cognition, CRF, mood, quality of life) were quite diverse. A relatively recent review in the Journal of the American Medical Association 109 summarizes the literature on balance, mobility, and fall risk in older adults, including many of the studies reviewed here. They observed that dance-based interventions are associated with a 31% reduced risk of falls, an effect most pronounced in interventions that met 3x/week or more and lasted 12–24 weeks. Significant effects were also seen for mobility, physical function, and lower body strength. The authors note that there is substantial heterogeneity noted in mobility, physical function, and lower body strength domains, which corroborates our review of the literature. Mobility and balance were the most frequently measured outcomes in studies of dance and aging. Over 30 different measures of mobility were reported. Gait speed was commonly measured, but was measured over a variety of distances, forward and backward, and instrumented. Eighteen different balance measures were reported.
Overall, the measures most widely used for balance (and also cognition) are relatively simple outcomes that can be administered easily and briefly in a clinical or community setting. However, part of the unique potential benefit of dance is that it trains complex movements that are likely to benefit older adults navigating the real world. While ease of administration and clinical relevance are clear benefits to these measures, their simplicity may undervalue these changes. For example, there are no widely used measures we are aware of that reflect key aspects of changes in movement in response to dance that may be specific to dance, such as improvements in cross-lateral movements, speed and sequencing of movements, or movement confidence. One important gap to fill for dance research might be a dance-specific measure of balance and/or mobility that captures aspects of movement that change in response to dance. This measure could be augmented by using instrumented testing, such as motion capture or inertial measurement units to improve sensitivity. The rapid evolution of more technologically sophisticated methods such as inertial measurement units may provide important insights into more subtle patterns of changes in gait or balance that are associated with maintaining or improving cognition and mobility. Given that changes in gait may precede detectable cognitive decline in people with dementia, technology that facilitates a more detailed understanding of the relationship between movement patterns and cognition and how those are altered by interventions like dance could yield important insights.
Cognition is an outcome that is important to older adults and previous systematic reviews of the literature suggest it may be improved by dance.56,69 However, the heterogeneity of cognitive testing used in dance studies hinders the aggregation of knowledge of the effects of dance on cognition. The studies included here used over 50 different cognitive tests, and over 30 cognitive tests were used in only one study (that is, they were included in one study but not repeated in any other studies). Part of the reason for the heterogeneity of cognitive tests used is that there is a major gap in understanding what cognitive domains are affected by dance, and what tests of cognition are most sensitive to dance intervention. Dual tasking, motor learning, and sequencing are not often tested as outcomes, although they are cognitive abilities that are arguably inherently trained in most forms of dance.
CRF is an important potential mediator of the benefits of dance in older adults. However, only 8% of the studies included in the review assessed CRF at all, and only half of these used VO2peak testing. It is worth noting that two studies assessing VO2peak were excluded because they had an average age less than 60, yet they still included older adults. Bellardinelli et al. 110 randomized 130 people with chronic heart failure to 8 weeks of 3x/week waltz or aerobic exercise training and observed comparable improvements in VO2peak between the two arms. The study by Rossmeissl et al. 111 followed 14 postmenopausal women with obesity who completed 12 weeks of Zumba classes 2–3x/week. This study did not observe increased VO2peak.
The inconsistencies in CRF findings emphasize important gaps in the literature on dance in older adults. One gap in current knowledge about dance for older adults is how much time during dance classes is spent moving at sufficient intensity to elicit CRF improvements. One study using English country dancing noted that self-reported in-class intensity was lower for dance than the stretching control and walking condition due to extended instruction required to learn monthly choreography sequences. 106 A key take-away is that an instruction protocol that allows for consistent participation in at least moderate-intensity activity is important when improving CRF is of interest. Another potential consideration in interpreting effects of dance on CRF is that at least two of the trials that did not observe increased VO2peak after dance targeted older adults with obesity. Because obesity can blunt the benefits of aerobic exercise on CRF,112–114 it may be important for trials planning to assess CRF in response to dance to take BMI or body composition into account during recruiting and randomization.
The inclusion of common data elements across studies of dance would be a major step forward for the field that would enable better aggregation of information across studies. Filling core gaps in knowledge about what tests best reflect dance outcomes in key domains for aging like mobility, balance, and cognition will be an important advancement for the field.
Heterogeneity of dance forms
The literature reviewed included many different forms of dance from different cultural traditions. This review did not attempt to fully characterize the dance forms or to define or categorize them separately from how they were reported by the authors. It is worth noting that endeavoring to do so would have changed this review in that many studies did not include much detail about the specific form used. Studies that used multiple dance forms often did not specify if every subject experienced every form of dance, for how long, and if there was a pre-specified order in which different dances were taught. Development of basic reporting requirements for dance interventions, as has been proposed for music interventions, 115 would enhance reproducibility.
Limitations and future directions
As already noted, this review was designed to capture the heterogeneity of the peer-reviewed literature about the effects of dance interventions on older adults. To meet this aim, the review was intentionally broad and inclusive. However, inclusivity comes with an increased risk of bias in the reported outcomes of included studies. The risk is somewhat mitigated by the fact that this review does not attempt to ascertain the effectiveness of dance, but rather heterogeneity of design characteristics of the included studies.
A future direction emphasized through this review is a need for the field of dance medicine to begin developing models that can be systematically tested. The diversity of methods, populations, dance forms, and outcomes highlighted in this review underscores the importance of crafting hypothesized intervention maps (as in Figure 1) and mechanistic models (example in Figure 5) that are relevant for different populations, dance forms, and outcomes of interest. This review did not include potential biological mediators of the effects of dance that would be necessary for generating mechanistic models of the effects of dance. Mechanistic models, as illustrated in Figure 5, complement intervention mapping by including more detailed biological and molecular factors hypothesized to be causal mechanisms of the effects of an intervention. For dance, there are multiple potential biological and molecular mediators that can be hypothesized from adjacent literature, but have been tested very little or not at all in the dance literature. For example, to our knowledge only one study has investigated whether dance affects levels of brain-derived neurotrophic factor, 85 yet the literature on exercise in aging shows that brain-derived neurotrophic factor along with other exerkines (factors released in response to exercise) may be key mediators of the benefits of physical activity. Another example of a relevant exerkine is irisin, which has recently been identified as a potential key factor linking physical activity to cognitive benefits of physical activity.116,117 Figure 5 provides an example of factors that might be considered for inclusion in a mechanistic model of dance. Most of these factors were not included in the review because they either have not been assessed in studies of dance, or have only been used in a small number of studies. We include Figures 1 and 5 to show examples of how dance researchers can craft hypothesized intervention maps and mechanistic models relevant to the target population, dance form, and outcome of interest. This is critical because there will be no single mechanism of dance, as the outcomes of interest are wide-reaching and will be differentially affected depending on what populations are targeted and which aspects of dance intervention are used in a given program.
The literature reviewed is primarily focused on answering the overall question of “why dance?” and providing evidence for the efficacy of dance to improve brain and body health in aging. However, in some cultures, there are many people that do not have a regular practice of dance and may have social or physical barriers to participating in group dance. As an example, many studies included have a higher proportion of women than men. It is important as a field to understand barriers to dance participation and potential negative consequences of dance in addition to the positive effects.
Finally, a unique consideration for future directions in the field of dance and aging is the need for close collaboration between dance artists and scientists. Incorporating perspectives of the artist from the inception of a study onward is absolutely essential. Professional dancers and choreographers can provide the scientific community with invaluable insight into the effects of dance they observe and the ways they modify classes to enhance certain outcomes they may wish to achieve pedagogically when they teach. Art and science are both forms of inquiry and employing both forms of inquiry fully will result in the most rapid and insightful advancements.
Conclusions
The study of dance in aging is a rapidly evolving, multidisciplinary field characterized by high heterogeneity of study design and outcomes. This scoping review of the literature reflects that high heterogeneity and suggests potential future directions that could help build consensus within the field about active components of dance, dosing parameters, and mechanisms. Important potential future directions include designing studies to test dosing parameters, establishing common data elements for dance studies, and development of intervention mapping and mechanistic modeling to strengthen and focus trial design.
Footnotes
Acknowledgments
The authors would like to thank the many individuals over time who have been part of our team and have contributed to our thinking about these topics as well as the reviewers, whose comments meaningfully improved the paper.
Author contributions
Paige E Rice (Data curation; Formal analysis; Writing – original draft); Deepthi Thumuluri (Data curation; Methodology; Writing – original draft); Rebecca Barnstaple (Conceptualization; Writing – review & editing); Jason T Fanning (Conceptualization; Writing – original draft; Writing – review & editing); Jessie Laurita-Spanglet (Conceptualization); Christina T Soriano (Conceptualization; Funding acquisition); Christina E Hugenschmidt (Conceptualization; Data curation; Formal analysis; Funding acquisition; Visualization; Writing – original draft; Writing – review & editing).
Funding
Funding support was provided by R01 AT00944 from the National Institutes of Health, National Center for Complementary and Integrative Health and R01 AG076669 from the National Institute on Aging.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data are available upon request.
Supplemental material
Supplemental material for this article is available online.