
Abstract
Background:
No studies have been conducted to date on the dimensional and discrete classification of emotions to study the emotional reactivity of older adults with Alzheimer’s disease (AD). Additionally, the presentation of film clips with affective content is currently one of the most effective and widely used Mood Induction Procedures (MIPS). However, it has been scarcely used in AD patients.
Objective:
Based on the dimensional and discrete models of emotion, this study examines the emotional reactivity of older adults with AD, using a popular set of film clips to induce emotions.
Methods:
We compared the responses of older adults aged over 65-years with mild to moderate AD (n = 15) and a healthy comparison group (n = 17) to six target emotions: disgust, fear, anger, sadness, amusement, and tenderness.
Results:
The results showed significant differences in the reactivity of fear, anger, and sadness between AD patients and healthy comparison group. However, the responses of the two groups to positive film clips were similar. Only in the amusement clip did the AD participants show a higher intensity response.
Conclusion:
These findings suggest that the characteristic loss of cognitive abilities in AD is related to a reduction in the ability to react to emotional stimuli, especially negative ones. However, these abilities seem to be preserved when it comes to positive emotions. Future research is necessary to investigate whether the positivity effect is present in AD patients.
INTRODUCTION
Alzheimer’s disease (AD) is currently defined as a progressive amnesiac disorder, with the subsequent appearance of other cognitive, behavioral, and neuropsychiatric changes that impede social function and activities of daily living [1]. The most common clinical phenotype of AD is characterized by a significant and progressive early episodic memory deficit, which remains dominant in the later stages of the disease and is associated with other cognitive impairments (executive dysfunction, language, praxis, and complex visual processing) and neuropsychiatric disorders. In addition, the deterioration characteristic of the disease also involves other areas, such as social cognition and emotions [2]. Although the literature on this subject is scarce, research indicates that deterioration of emotional processing appears even from the early stages of the disease and evolves according to the progress of the disease [3]. In this sense, patients with very mild AD present difficulties in recognizing and discriminating expressions of complex emotions [4]. However, it has also been studied that patients with AD can identify emotional targets, indicating decreased ability to discriminate, but not the absence of this ability [5]. Some studies have concluded that the recognition of basic emotions declines, except for expressions of anger [6], while other studies suggest a better preservation of happiness than other negative basic emotions [7, 8]. A recent systematic review found that expressing the six basic emotions, patients with AD recognize amusement more readily and anger and sadness with greater difficulty in photographs [9]. Another recent systematic review shows that perception of negative emotions (anger, sadness, and fear) is affected largely than the emotion of happiness, which shows high accuracy in both AD and mild cognitive impairment (MCI) patients [10]. This discrepancy could be explained from a neurocognitive perspective. Both hippocampal and amygdala atrophy have been demonstrated in early AD and MCI, possibly explaining the deficit in the perception of fear, which relies on this brain circuitry [10, 11]. Likewise, both works suggest that the recognition of emotional expressions is directly related to specific cognitive capacities and suggest greater difficulty for the perception of negative emotions. Accordingly, it can be considered that the effect of positivity [12] remains despite the presence of the disease. The positivity effect refers to the tendency of older people to prioritize achieving emotional gratification. In this regard, the work by Bohn et al. [13, 14] provides support for the view that decreased cognitive resources accompanying normal aging lead to an increased emphasis on optimizing emotional wellbeing. They find that decreased cognitive resources in AD also lead to the manifestation of this preference, sometimes exaggerating the focus.
Works studying the emotions in AD and MCI patients have mainly used techniques that include photographs of facial expressions. However, the most recent research seems to be oriented toward more ecological and standardized methods than facial expressions [9]. A review of the literature shows that mood induction procedures (MIPs) provide the strongest causal evidence of the psychological and physiological effects of emotions in the laboratory [15]. Of all the procedures, one of the most widely used is the presentation of film clips. This method consists of watching movie scenes with intense emotional content. One of the main reasons is that it facilitates the evocation of psychophysiological, cognitive, and motor responses to emotion, in addition to its high ecological validity [16, 17].
In addition, research has focused on studying emotional responses from either the dimensional model perspective or the discrete model perspective. The dimensional model posits that the basic components of emotions are dimensions, such as valence (emotional tone) and arousal (excitement level) [18], while the discrete model suggests the basic components are discrete entities, such as sadness, disgust, and amusement [19]. The two perspectives are often compared and contrasted. Nevertheless, to understand the complex emotional response system, it is important to consider both models [20]. Related to research on aging, a recent study shows that exploring both models simultaneously provides a better understanding of the older adults emotional reactivity [21]. However, and to the best of our knowledge, no previous studies have focused on both models in AD patients.
The ambiguity of the previous results motivated us to carry out an exploratory research in order to improve our understanding of the subject and to examine differences in emotional processes among healthy older adults with AD when using film clips as the MIP. Additionally, in emotional induction procedures, different positive emotions are not typically studied, but rather a generic label of happiness, and this practice is even more prevalent when studying individuals with AD. However, some studies are revealing psychophysiological and subjective discrimination between different positive emotions, such as amusement and tenderness, in young adults [22, 23] and older adults [21].
The aim of this study is to provide an opportunity to better understand the links between cognition and emotion in the presence of AD. It was hypothesized that cognitive deficits in AD patients could modify the perception of negative emotions. In contrast, there may be no difference in the processing of positive emotions, and this may be related to the impact of the positivity effect.
METHODS
Sample
Participants diagnosed with mild to moderate AD (n = 17) and healthy comparison group (HC) participants (n = 17) were recruited from the neurology service of the General Hospital of Valencia (Spain) and a research volunteer pool at the Department of Psychology at the University of Castilla- La Mancha (UCLM). Exclusion criteria in both groups were: <65 years, significant asymptomatic neurovascular disease, history of previous symptomatic stroke, medical condition significantly affecting the brain, history of alcohol or substance abuse, history of diagnosed psychiatric disorder or current comorbidity, and moderate or severe depressive symptoms. HC participants were only included if they had scores≥23 on the Mini-Mental State Examination (MMSE) [24] and≤3 on the Global Deterioration Scale (GDS) [25]. Participants’ diagnosis of probable AD followed the criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition [26], with MMSE scores between 18 and 23 and GDS between 3 and 4. Two AD participants were excluded because they scored > 4 in GDS, leaving a total of 15 in the AD group. Clinical diagnosis was the end result of an extensive evaluation, including medical history and physical and neuropsychological examinations and was determined by consensus between the neurologists and a neuropsychologist. The Ethical Committee on Human Research of the University of Valencia approved this study (UV-INV_ETICA-1217558), which was conducted in accordance with the Declaration of Helsinki and all participants gave their written informed consent to participate in the study.
We calculated the statistical power, using the G*Power software (v. 3.1.9.6.) for the MANOVA F-test with repeated measures and two groups. For an effect size f = 0.2, β/α ratio = 3.16, n = 34, 6 measurements, non-centrality parameter λ= 8.16, 1 and 32 degrees of freedom, α err prob = 0.05, β err prob = 0.18, Pillai V = 0.19, we obtained a critical value of F = 3.16 and a power = 0.81.
Measures
In addition to the GDS [25] and Beck Depression Inventory (BDI-II) [27], all the participants completed a battery of neuropsychological tests assessing the main cognitive domains.
The GDS [25] describes seven clinically distinguishable global stages ranging from normality (1) to severe dementia of the Alzheimer type (7). The GDS analyzes patients’ ability to function, reflected in daily living and instrumental activities, as well as psychiatric morbidity based on progressive cognitive loss. Mood alteration was measured with the BDI-II [27]. This questionnaire has 21 items that assess symptoms of depression including anhedonia, sadness, loss of energy or interest, eating or sleeping disturbances, loss of concentration, and suicidal ideation. Scores from 14 represent the range of depression, with 14–19 being considered mild depression, 20–28 considered moderate depression, and 29–63 indicating severe depression [28]. The MMSE [24] was used as an index of global cognitive functioning; the maximum score is 30 points. This screening test estimates the existence and severity of cognitive impairment, without providing a diagnosis of any specific nosological entity. Scores from 23 to 21 indicate mild dementia, scores from 20 to 11 are considered moderate dementia, and a score below 10 points indicates severe dementia.
In addition, we applied the Memory Alteration Test (M@T) [29]. The M@T is a screening test for amnestic MCI and AD that assesses verbal episodic and semantic memory. It has five subtests: encoding, temporal orientation, semantic memory, free recall, and cued recall (applied if the subject fails the free recall part). The maximum M@T score is 50 points and a score below 37 is an optimal cut-off score.
Verbal memory (short-term recall and delayed recall) was assessed using the Spain-Complutense Verbal Learning Test (TAVEC) [30]. The TAVEC is composed of three lists of words presented as “shopping lists”: a learning list (List A), an interference list (List B), and a recognition list (List C). This study uses List A, which is composed of 16 words belonging to four categories and is used as a standard learning test and as a measure of delayed memory. For the Immediate Verbal Learning Test, five consecutive trials are carried out; after each presentation, subjects are assessed according to the number of words they remembered correctly (scores from 0–16 on each trial, and scores from 0–80 on all five trials). For the measure of the Delayed Verbal Learning Test, 20 min after the immediate recall, the subject must remember the previously read list. This study uses the total number of words recalled after the five trials as the score.
Language and executive function ability were assessed using the Categorical Fluency (animals: name animals for 1 min) and Phonological Fluency (letter P: say words that begin with the letter “p” for 3 min) subtests of the Barcelona Test Revised (TBR) [31]. This test measures the capacity to access and evoke elements from the lexical and semantic warehouse. To score the test, one point is given for each correct word.
The Rey Complex Figure Test [32] assesses memory and other executive functions. The subject must carefully reproduce a complex geometric drawing and later (3 min) reproduce it from memory. The first part evaluates cognitive aspects such as planning, motor skills, operative memory, and visuo-constructive and spatial skills.
Finally, the affective state induced through each film clip was examined. On the one hand, valence and arousal dimensions were measured with the Self-Assessment Manikin (SAM) [33]: a self-report questionnaire (9-point Likert-type scale) that indicates how pleasant (9) or unpleasant (1) and how aroused (9) or relaxed (1) participants felt while watching the emotional film clips. The questionnaire uses graphic figures, which represent the different emotional states, and is therefore simple to administer in both age groups, regardless of cognitive abilities. On the other hand, discrete emotions were measured with the Differential Emotions Scale (DES) [34, 35]. This emotional scale has 18 items and uses a 7-point scale (1 = “not at all”, 7 = “very intense”) to rate the extent to which participants experience each state as they watch each film clip. The emotional categories used in this study were amusement, tenderness, anger, disgust, fear, and sadness.
Experimental procedure
Applying the inclusion and exclusion criteria indicated above to assign participants to the groups, the clinical and mood assessments were conducted in the first session (BDI-II, MMSE, and GDS). In the second session, neuropsychological measures were administered. The emotional induction was administered in a third session.
A popular film library, previously validated in young and older Spanish adults [16, 36], was selected to elicit seven target emotions: sadness, disgust, fear, anger, amusement, tenderness, and neutral. The selected scenes maintained the same features as those used in similar studies [17, 22]. The task was programmed and administered using E-prime 2 Professional (Psychology Software Tools, Inc.). Participants watched a single clip of each emotional target and the average duration of emotional induction was 35 min. In the laboratory (86 ft2), each participant performed the task individually on a 27” computer screen. The experimenter was present in the room to explain the procedure, highlighting the lack of correct or incorrect answers. The playback of the clips was controlled in such a way that (a) the order of the film clips was different for each participant; (b) no more than 2 clips with equal valence (negative or positive) were played consecutively; and (c) the neutral clips were presented in a fixed order before (practice trial and previous affect state measure) and after the experiment (emotional recovery). The participants confirmed they could see the screen and hear the sounds adequately before proceeding. Participants were told: ‘I will show you several film clips and would like you react spontaneously to the film. Some of the scenes are emotionally intense; if you feel upset, I can stop the film clip.’ After each of the clips, the participants completed the SAM and DES questionnaires to report their emotional reactivities. In addition, they were instructed to close their eyes, relax their muscles, and breathe regularly for about 2 min between clips. Figure 1 shows an example of a sequence from one event.

Experimental sequence. Time course of events in one sequence. A) Fixation cross. B) Mean length of exposure to the clip. C) Emotional self-report (SAM). D) Emotional self-report (DES). E) Relaxation.
Statistical analysis
The analyses were conducted using SPSS 21.0 (IBM) for Windows. Our preliminary analyses investigated group differences. First, we examined demographic differences between groups by running descriptive statistics (mean and standard deviation), gender differences by running a chi-squared test, and differences according to education level and neurocognitive ability by running an independent samples t-test.
Second, we examined the previous affect state and the effect of a mood induction procedure using films. For each participant, there was a two-factor subjective evaluation (SAM: valence and arousal, and DES: six discrete emotions). We conducted separate MANOVAs to analyze dimensional emotional variables (valence and arousal) and discrete emotional states. Five MANOVAs were conducted to analyze neutral, negative and positive emotional states. To determine whether the dependent variables were distributed normally within the groups, we conducted the Kolmogorov-Smirnoff test. Statistical significance was interpreted using the criterion of p≤0.05.
RESULTS
Our preliminary analyses revealed differences between groups in some of the variables examined prior to the emotion induction (Table 1). Neurocognitive screening revealed differences between the AD and HC groups in all the cognitive variables considered. The AD group obtained significantly lower scores in all the main cognitive domains compared to the HC group.
Basic socio-demographic characteristics and neuropsychological screening scores reported by group
AD, Alzheimer disease; HC, healthy comparison group; M@T, Memory Alteration Test; Mini-Mental State Examination; TAVEC, Complutense Verbal Learning Test; TBR, Test Barcelona Revised. p≤0.05.
For the main research question of whether emotional reactivity by AD adults are different from the emotional reactivity by HC adults, we separately analyzed neutral, negative, and positive emotional states.
First, we examined the scores for the initial neutral stimulus. A 2 (valence and arousal: neutral state before the task) x 2 (groups: AD versus HC) MANOVA showed no significant main effect of group, Pillai’s trace [V = 0.00, F (2, 29) = 0.42, p = 0.959, η2p = 0.00]. AD and HC groups reported no differences in valence and arousal levels above their baseline state.
Negative assessment
In the assessment of the four negative emotions, we conducted two separate MANOVAs. To examine the dimensional emotional variables, both valence and arousal were included as dependent variables for each emotion in the MANOVA test. To examine the discrete emotional variables, the target emotions (anger, disgust, fear, and sadness) were included as dependent variables on a second MANOVA test. For dimensional variables, an 8 (valence and arousal: anger versus fear versus sadness versus disgust)×2 (groups: AD versus HC) MANOVA showed a significant main effect of group, Pillai’s trace [V = 0.46, F (8, 22) = 3.18, p = 0.015, η2P = 0.53]. The inter-subject effects in relation to the group were studied by comparing their scores on the dependent variables. In particular, individuals with AD scored film clips lower for the conditions of fear, anger, and sadness. For discrete emotional variables, a 4 (emotional targets: anger versus fear versus sadness versus disgust)×2 (groups: AD versus HC) MANOVA revealed no significant main effect of group, Pillai’s trace [V = 0.25, F (4, 27) = 2.24, p = 0.091, η2P = 0.25]. Although the results were not significant, it was decided to analyze the inter-subject effects in relation to the group, given the little scientific evidence on this topic and as this study is a first approach to the problem. In this sense, differences were observed in the study of inter-subject effects. Specifically, the AD participants scored the film clips for the fear and anger conditions lower than the HC participants.
Positive assessment
In the assessment of positive emotions, we also conducted two separate MANOVAs. To examine the dimensional emotional variables, both valence and arousal were included as dependent variables for each emotion in the MANOVA test and to examine the discrete emotional variables, the target emotions (amusement and tenderness) were included as dependent variables in a second MANOVA test. For the dimensional variables, a 4 (valence and arousal: amusement versus tenderness)×2 (groups: AD versus HC) MANOVA revealed no significant main effect of group, Pillai’s trace [V = 0.85, F(4, 27) = 1.17, p = 0.344, η2P = 0.14]. In the same way as the negative emotion analyses, we examined the inter-subjects effect, even though the main effect of group was non-significant, as a first approach to the problem. No differences were observed in the study of inter-subject effects for dimensional variables. To examine the discrete emotional variables, a 2 (emotional targets: amusement versus tenderness)×2 (groups: AD versus HC) MANOVA found a significant main effect of group, Pillai’s trace [V = 0.23, F (2, 29) = 4.52, p = 0.020, η2 p = 0.23]. In this sense, the AD participants rated the amusement condition film clip higher than the HC participants. Table 2 presents the effects, in terms of valence, arousal and emotional target of each condition, with respect to the neutral, negative, and positive emotional induction of AD and HC participants. In addition, the graphic results are presented in Figs. 2, and 4.
MANOVA univariate F-tests for negative and positive emotions scores reported by film condition and group
The discrete and dimensional emotions scores were evaluated by film clip target. AD, Alzheimer disease; HC, healthy comparison group; DES, Differential Emotions Scale; SAM, Self-Assessment Manikin.
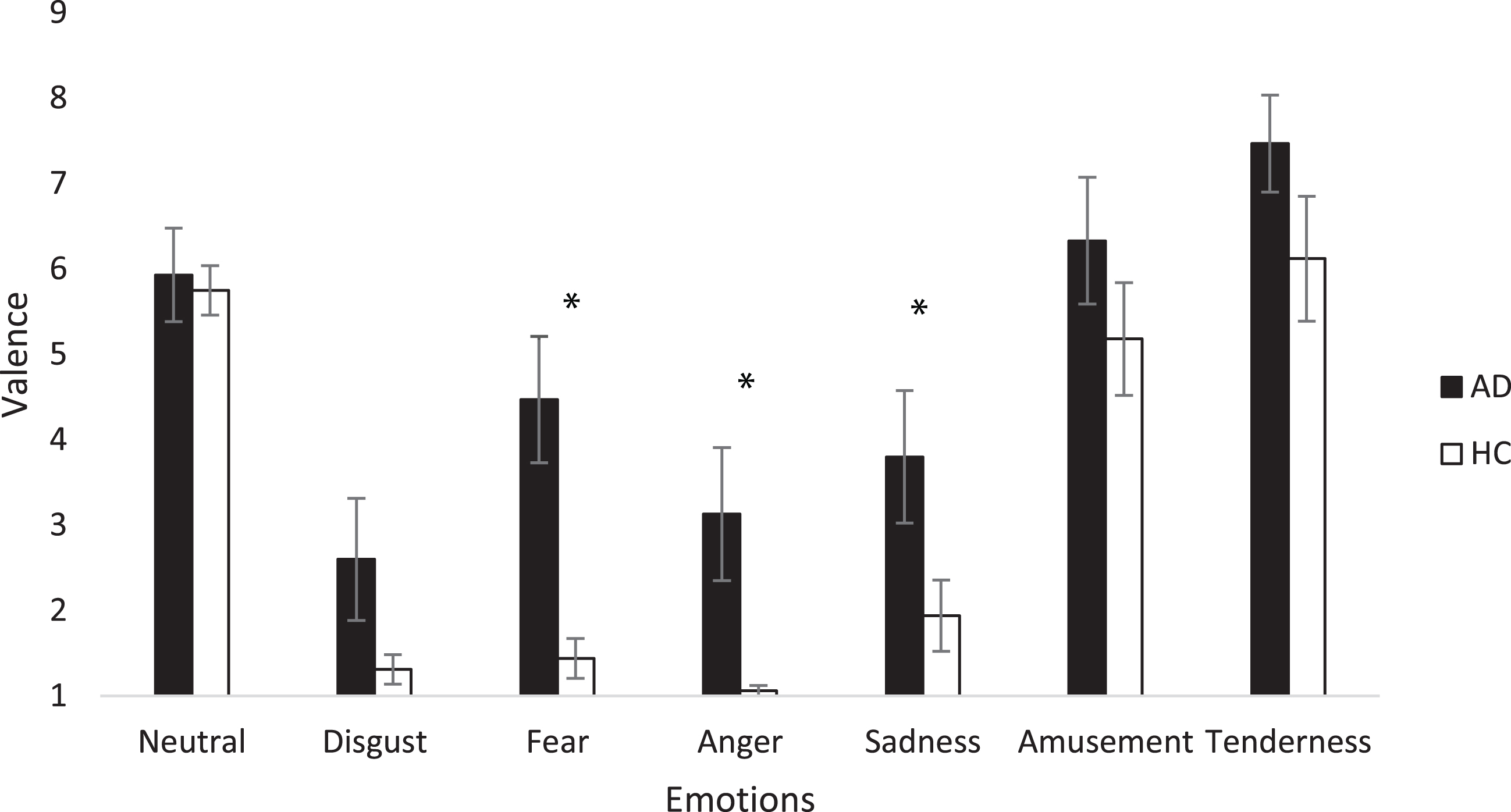
Emotional valence scores by film condition and group. Participant-level means on baseline and emotional target categories. Error bars depict standard error (SE) values. AD, Alzheimer disease; HC, healthy comparison group. *p < 0.05.
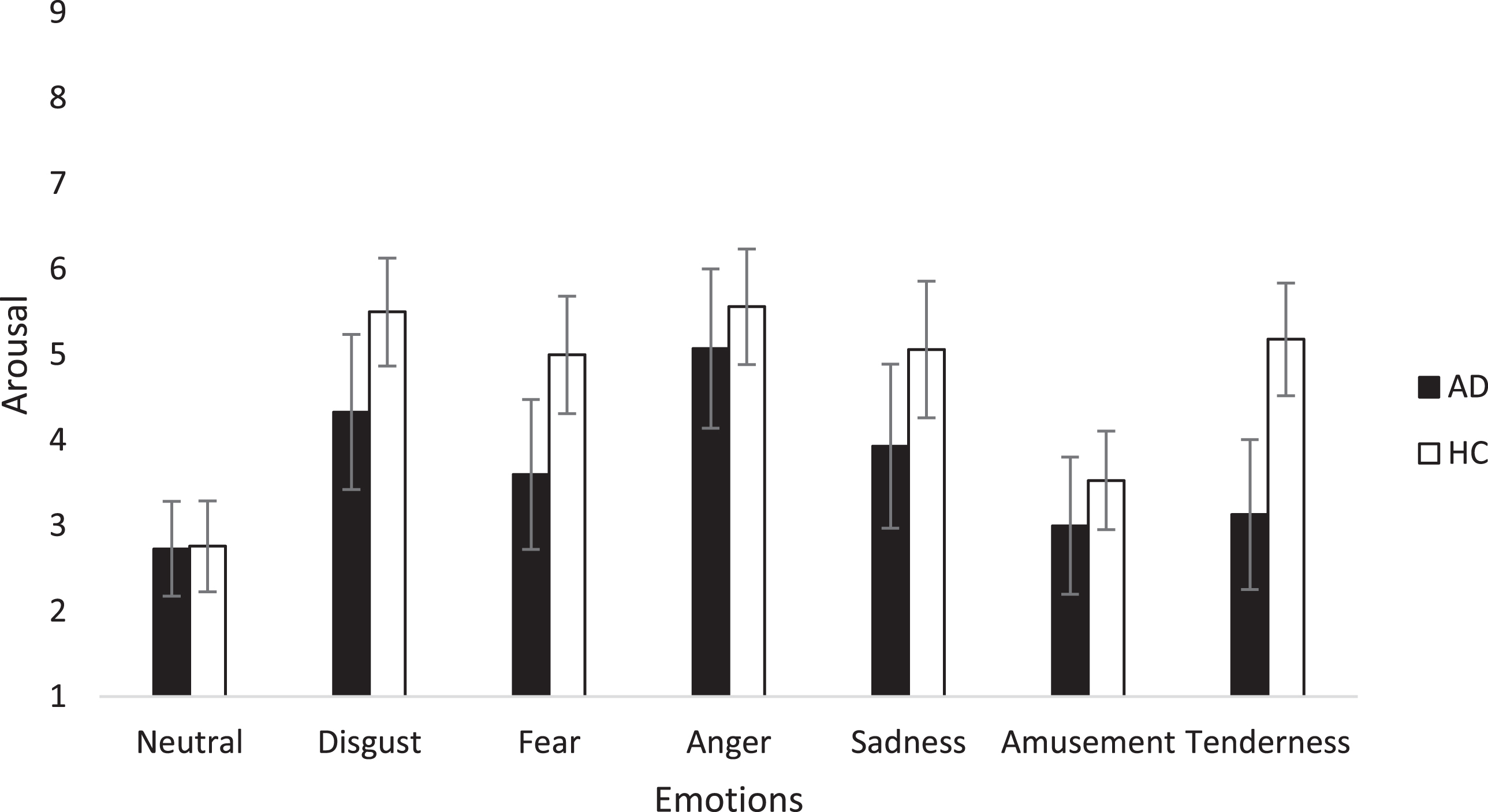
Emotional arousal scores by film condition and group. Participant-level means on baseline and emotional target categories. Error bars depict standard error (SE) values. AD, Alzheimer disease; HC, healthy comparison group. *p < 05.
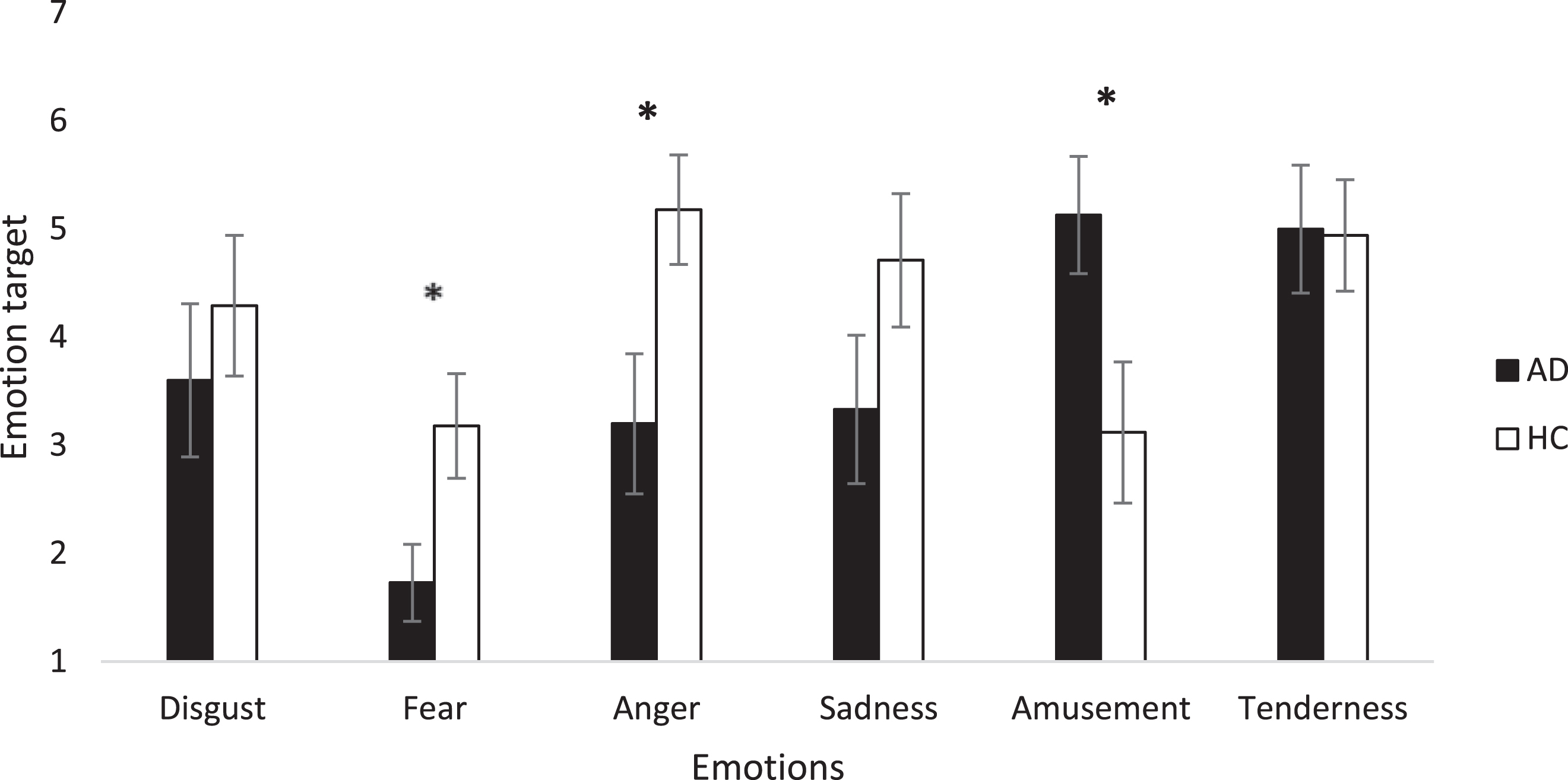
Emotional targets scores by film condition and group. Participant-level means on baseline and emotional target categories. Error bars depict standard error (SE) values. AD, Alzheimer disease; HC, healthy comparison group. *p < 0.05.
Ability to identify the target emotions
As regards the ability of the two groups to identify the emotional targets, Table 3 shows that the positive emotions were more easily identified than the negative emotions in the case of both the HC and the AD group. In this sense, the negative film clip stimuli elicited a more mixed emotional experience than the positive emotion clips.
Emotional reactivity differences to discrete emotions identification between AD and HC adults
In
DISCUSSION
This study examined the differences in negative and positive emotional reactivity between a group of healthy older adults and a group of patients with mild to moderate AD. Participants with mild to moderate AD showed difficulties in the induction of three negative emotions compared to their HC counterparts, showing a different emotion reactivity. In the case of positive emotional induction, the participants with mild to moderate AD showed higher levels of the emotional target of amusement.
The analysis of negative emotions revealed that the participants with AD showed higher levels of valence than HC participants in the fear, anger, and sadness stimuli. Moreover, they showed lower fear than the HC group in the fear target, and lower anger than HC group in the anger target. In line with previous research using film clips, the level of subjective reactivity in AD patients was reduced for the dimensions of fear [3] and sadness [37]. The difficulty patients with AD have in identifying or experiencing negative emotions has been evidenced in the literature. In fact, a recent systematic review showed that the most difficult emotions to recognize for these patients are anger and sadness and the easiest is happiness [9]. Over the last ten years, the emotions have been extensively studied using facial expressions. However, there has been little research using film clips. Regarding the facial expression method, there are robust findings to suggest that negative emotions may be more difficult to identify than positive ones. Our results suggest that emotional reactivity through film induction yields similar findings. Disgust was the only negative emotion which showed no differences between the AD and HC groups. This seems to indicate that, as with facial expression recognition, the ability to react to disgust is preserved in mild AD. Previous studies suggest that preservation of disgust could be attributable to the relative preservation of the basal ganglia in AD [38, 39]. It would be necessary to test the specific neuropathological information of the participants with AD in the future. In the same line, it has been suggested that the nature of emotional experience in older persons is more complex and mixed than in younger adults [40]. The present study reveals greater emotional co-occurrence in response to the negative clips compared to the positive clips in both the older HC and AD older participants.
Concerning our exploration of positive emotions, the reactivity of positive emotions is relatively intact, and a certain degree of positive bias can be observed. Specifically, AD participants showed higher levels of amusement-to-amusement target, although there were no differences in reactivity to the tenderness target. This differential influence in positive emotions has been found in other studies [21, 22]. This reveals that positive emotions should be considered independently. A review of the literature shows that happiness is typically used as the only positive target in mood induction procedures. However, discrete positive emotions need to be studied because each one has a different developmental role.
Previous research has suggested that these emotions are more intact in AD and therefore show normal reactivity. However, this may depend on the stimuli presented. For example, the amusement scenes often include a laugh track without understanding of the narrative being required [3].
The present study highlights the consideration of both discrete and dimensional perspectives on emotion. The results confirmed that AD and HC older adults present different patterns of reactivity to emotional stimuli. They showed differences in valence and discrete emotions tests, but the differences were not the same in the two measures. Considering affective valence, the reactivity of AD participants was lower to the fear, sadness, and anger targets, and there were no differences in case of the positive targets. However, considering the discrete emotions model, the reactivity of AD participants was higher to the amusement target and lower to the anger and fear targets. Our findings show that considering dimensions and discrete models of emotions can enhance the understanding of the emotional system in older people with and without cognitive impairment.
Related to the discrepancies observed between negative and positive emotions suggest that several factors may be influencing the results. First, negative information has a greater psychological impact than positive information [41], requires more attention, and is more accurately recognized [42]. As this study suggests, this differential form of processing emotions is also present when cognitive impairment appears, with negative emotions being the most difficult to identify [43–46]. A potential explanation for this is that although the negative clip induction is more powerful than the positive clip induction [47], negative stimuli require the mobilization of a greater number of cognitive processes [42, 43]. Second, cognitive processing is a crucial element of emotion, understood from a multidimensional perspective. The results of the present study highlight that people with mild to moderate AD already present impairment in memory tasks, such as encoding, temporal orientation, semantic memory and recall, and these involve executive functioning skills, such as the use of strategies for learning, susceptibility to interference, recognition and the learning curve [48]. Third, the loss of cognitive abilities can lead to a reduction in the ability to experience negative emotions. The amygdala is one of the main structures involved in emotional recognition and, specifically, in facial recognition [49]. Furthermore, it is one of the areas affected in the early stages of AD [50, 51]. The similarity of results when using different methods (facial expressions and film clips) suggests that the involvement of the amygdala in emotional identification and reactivity involves strong links between cognition and emotion. On the other hand, the effect on executive functioning skills of participants with AD and their emotional responses to the clips could indicate that executive functions, in addition to being important in the recognition of facial expressions, are also key for the identification and reactivity of the emotions one experiences [52]. Finally, patients with AD are less flexible in their ability to regulate emotions, and it is possible they excessively suppress negative emotions, but this is not the case with socially acceptable emotions [8, 53].
Along the same lines as the works of Bohn and colleagues [13, 14], which show a certain effect of positivity in AD patients, the findings of this study lead us to consider whether they fit the classic models of aging, such as the Socioemotional Selectivity Theory (SST) [54] and the Dynamic Integration Theory (DIT) [55]. SST considers the tendency of older people to prioritize the achievement of emotional gratification, to inhibit negative information and to show a relative preference towards positive information (positivity effect). It is possible that emotional dimensions are important for advanced age, even when cognitive functions decline. In the present study, AD participants showed higher levels of amusement emotion. Like the recent study of Bohn and colleagues [13], it is feasible to consider that cognitive impairment is not a barrier to socioemotional selectivity. Furthermore, DIT postulates that the decline in cognitive resources, characteristic of aging, is resolved by optimization strategies that bias or distort information in a positive direction. The results of the present study suggest that these strategies could be intensified when AD causes deterioration of cognitive resources, and not simply due to the course of age. Because the results of this research have suggested a first approach to the subject on AD and the possible links with these models of emotional aging, it would be necessary for future research to focus on the study of this hypothesis.
The results of the present study could guide future research and clinical practice. The study shows that audiovisual stimuli (multimodal method) may facilitate emotional understanding in dementia. The more emotional the information clues, the easier an event is to understand. Therefore, films are an effective method of inducing emotions in people with dementia. Past research also has indicated the importance of using participant-selected music (from late adolescence and early adulthood) to elicit strong emotions [56], and suggests that familiar music may play a greater role in prompting the recall of self-defining memories for individuals with dementia than it does for healthy older adults. Future research should create audiovisual catalogues for AD patients. Additionally, interventions with positive film clips should be used as a clinical strategy to improve mood in this population, with positive clips being recalled with greater intensity. Patients with cognitive impairment might benefit from mood induction beyond simply recalling events that triggered the emotion, as they could experience prolonged affective mood states despite not recalling the stimulus that generated the emotion [37, 57].
This study also has some limitations that should be mentioned. First, the findings may have been influenced by having a relatively small sample. In this sense, it is worth noting this is an exploratory study, the aim of which was to enhance the understanding of emotional reactivity in AD patients and the effectiveness of film clips as an MIP in such individuals. The sample size and the type of study performed do not allow us to establish relationships between the different variables, such as neuropsychological tests and values of emotional reactivity. Given that the emotional response system is complex, to assess emotional induction through movie clips, it would be of great interest to have different neurophysiological correlates involved in the emotional response considered. Furthermore, it would be useful to include a global measure of cognitive functioning that could allow us to relate general cognitive functioning to the scores obtained in response to the different emotional targets, and to analyze the existence of differences according to the different levels of arousal produced by the stimuli. Second, gender may influence the intensity of some discrete emotional experiences, due, for example, to the social acceptability of emotional events [58]. Future studies should consider gender equity in the participants.
Third, watching film clips can place a high cognitive demand on patients with AD and can affect the understanding of stimuli. Further research should examine how the emotional response is affected in individuals who are at other stages of the disease or even with other types of dementia, such as frontotemporal dementia. Emotional reactivity in AD is a promising line of research. Future studies should explore whether the positive effects on AD observed here are also produced by other stimuli or other cognitive processes. Research also needs to focus on examining whether individuals with non-Alzheimer’s type dementia are also biased toward positive information in cognitive processes.
Footnotes
ACKNOWLEDGMENTS
We are grateful to our participants for their contributions to this study.
This study has been supported by the Castilla-La Mancha Department of Education, Culture and Sports and the European Regional Development Fund under SPBLY/19/180501/000181 grant and the Spanish Ministerio de Ciencia, Innovación y Universidades (Spain) under PID2019-103956RB-I00 grant.