
Abstract
Background:
Hallucinations in Alzheimer’s disease (AD) have been linked to more severe cognitive and functional decline. However, research on visual hallucinations (VH), the most common type of hallucinations in AD, is limited.
Objective:
To investigate the cognitive and cerebral macrostructural and metabolic features associated with VH in AD.
Methods:
Twenty-four AD patients with VH, 24 with no VH (NVH), and 24 cognitively normal (CN) matched controls were selected from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database. Differences in regional gray matter (GM) volumes and cognitive performance were investigated with whole brain voxel-based morphometry analyses of MRI structural brain scans, and analyses of neuropsychological tests. Glucose metabolic changes were explored in a sub-sample of patients who had FDG-PET scans available.
Results:
More severe visuoconstructive and attentional deficits were found in AD VH compared with NVH. GM atrophy and hypometabolism were detected in occipital and temporal areas in VH patients in comparison with CN. On the other hand, NVH patients had atrophy and hypometabolism mainly in temporal areas. No differences in GM volume and glucose metabolism were found in the direct comparison between AD VH and NVH.
Conclusion:
In addition to the pattern of brain abnormalities typical of AD, occipital alterations were observed in patients with VH compared with CN. More severe visuoconstructive and attentional deficits were found in AD VH when directly compared with NVH, and might contribute to the emergence of VH in AD.
INTRODUCTION
Although cognitive impairment represents the core feature of Alzheimer’s disease (AD), neuropsychiatric symptoms are also common, affect negatively patients’ and caregivers’ quality of life, and are associated with early institutionalization [1, 2]. Hallucinations are observed in a minority of patients with AD, with a prevalence of 13% on average [3], and they have been related to more severe and rapid cognitive impairment [4]. Visual and auditory hallucinations appear to be the most common forms of hallucination in AD, although they can be found in any sensory modality [3, 4]. VH in AD have been associated with older age, impaired visual acuity, and more severe dementia [5–7]. VH have been identified as the most specific clinical symptom differentiating dementia with Lewy bodies (DLB) from AD in the early stages, and as the only feature suggesting the presence of Lewy bodies (LBs) in cases with mixed AD/LB pathology [8–10].
Hallucinations and delusions have often been investigated together in AD, given their high comorbidity [11]. Studying psychosis in AD as a unitary phenomenon, however, may introduce interpretative issues on symptom-specific neural and cognitive processes that may vary between different psychotic manifestations. In particular, although some studies suggested that visual hallucination may present often with misidentification delusions [12, 13], investigations into the neural alterations that may either underlie both hallucinations and delusions or contribute to them individually are lacking. One study comparing two patients with AD and VH and two patients with paranoid delusions with five patients without psychosis found brain hypometabolism in lateral prefrontal and medio-temporal areas in both patient groups with psychosis, but parietal hypometabolism only in the group with VH [14]. Moreover, the neural correlates of misidentification delusions appear to be still not completely understood, since the few studies available have shown hypometabolism in orbito-frontal and cingulate regions [15] and greater medial temporal lobe atrophy [16] associated with this symptom.
These few and heterogeneous findings suggest a clear need for studies that include carefully characterized groups of patients with AD presenting with specific psychotic symptoms to investigate hallucinations and delusions separately, but also hallucinations in different sensory modalities. Evidence reporting neuropsychological features associated with hallucinations in AD is very limited, and even less for VH. Most studies did not differentiate between sensory modalities, providing, therefore, only partial knowledge of hallucinatory phenomena in this disease. Indeed, recent revisions of both research [13] and clinical criteria [17] for psychosis in neurocognitive disorders have advocated for the distinction of specific psychotic symptoms (e.g., hallucinations in different sensory modalities) in order to advance the understanding of the possible specific causes and treatments. El Haj et al. [4] proposed that hallucinations in AD are the result of a complex interaction between state markers, such as psychological distress and iatrogenic factors, and trait markers, including neurological, sensory, and cognitive deficits. In terms of specific cognitive deficits associated with hallucinations, the authors suggested a prominent role of dysfunctional inhibitory mechanisms of irrelevant memories, memory suppression and response inhibition [4, 19]. A study focusing specifically on VH in AD reported associations with more severe impairments in executive functioning, verbal, visuospatial, and semantic memory, as well as more severe global cognitive impairment [20]. Chiu et al. [6] examined the core features of DLB symptomatology in AD patients with VH, who had higher rates of REM sleep behavior disorder (RBD), cognitive fluctuations, severe neuroleptic sensitivity, and other neuropsychiatric and psychotic symptoms when compared with patients without VH. Hallucinating patients were said to have more severe global cognitive impairment, but the use of only screening tests limited the investigation of more specific cognitive features [6]. Studies detailing the cognitive profile of AD patients with VH are still lacking, as well as those investigating the neural processes involved, suggesting a need for further research. Only a few studies have explored the structural and functional brain features associated with hallucinations in AD, and even less have focused on the visual modality. Some studies reported evidence of brain alterations in the occipital lobe in patients with VH, including smaller occipital/whole brain ratio [21] and higher occipital periventricular hyperintensities scores [22], while other findings suggest a frontal, parietal, and temporal involvement [14], although sample sizes were rather small. In a longitudinal study, Donovan et al. [23] investigated changes in cortical thickness over time in a cohort of 812 participants, including patients with AD dementia, mild cognitive impairment, and cognitive normal individuals from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database. The authors found that lower baseline supramarginal cortical thickness predicted the worsening of hallucinations over time, but not reduced thickness of occipital, frontal, and superior parietal cortices [23]. Other studies on hallucinations found frontal and insular hypometabolism and gray matter (GM) loss, and parietal hypoperfusion [24, 25].
The present study explored trait-related neurocognitive and brain features associated with VH in AD using neuropsychological testing, voxel-based morphometry (VBM) analyses of structural magnetic resonance imaging (MRI) scans, and 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET). We hypothesized that VH in AD might be associated with cognitive and neural alterations that could possibly resemble those observed in DLB [8, 26], and expected an involvement of visual perception and attention deficits, in line with the Perception and Attention Deficit (PAD) model of VH [27], and underlying disrupted neural circuits, as contributing factors to VH in AD. We hypothesized occipital and occipito-temporal volumetric brain abnormalities in hallucinating patients, underlying visual perception impairments, and frontal/subcortical atrophy, sustaining attention deficits [28]. Finally, we expected occipital hypometabolism [26], in line with the hypothesis suggesting a DLB-like profile in AD with VH.
METHODS
Study participants and clinical assessment
Data used for this study were obtained from the ADNI database (adni.loni.usc.edu)2 and associated material. All data contained in the ADNI database are anonymized and publicly available. Approval for secondary analyses of this dataset was granted by the Research Committee of Brunel University of London (reference number 30422-TISS-Jul/2021- 33453-2).
From the ADNI cohort, a systematic search for patients with VH was undertaken and participants for whom the following data were available were screened further: T1-weighted MRI scan, Neuropsychiatric Inventory (NPI), Mini-Mental State Examination (MMSE) and a comprehensive neuropsychological assessment. Scores were retrieved for the following tests: Trail Making test (TMT), Prose Memory test, Rey Auditory Verbal Learning test (RAVLT), Category Fluency test, Clock Drawing test (CDT) (drawing and copy), Boston Naming test. A detailed description of the clinical protocol, neuropsychiatric and neuropsychological assessments is available at http://adni.loni.usc.edu/methods. Data collected within a 6-month period were retrieved for each participant. For patients with data collected at two different time points, the earliest visit was chosen. Consistent with most studies investigating hallucinations in neurodegeneration, we explored trait-related features associated with VH, and differentiated hallucinating and non-hallucinating patients based on whether VH were among the reported clinical features [29]. The presence of VH was assessed with the NPI sub-section for VH, namely by answering the question “Does [P] describe seeing things not seen by others or behave as if he/she is seeing things not seen by others (people, animals, lights, etc.)?” with yes/no. Patients in the NVH group had a “no” answer to this question in all assessments available in the ADNI database. Patients were assigned to the VH group if they had a “yes” answer to the relevant question at least in one of the available assessments, suggesting the presence of this symptom as a trait-related feature characterizing their clinical phenotype. In case of visits at multiple time points, the first assessment when patients had a record of the presence of VH was chosen. Six patients were reported as experiencing VH at 2 (n = 3) and 3 (n = 3) visits. Eight patients presented a fluctuating VH status, with 1 (n = 3), 2 (n = 4), or 4 (n = 1) follow-up visits without VH, and 11 patients did not have a follow-up assessment after the first visit when VH were recorded. Of the 24 selected patients with VH, 12 also presented hallucinations in other sensory modalities, namely auditory (n = 8), tactile (n = 3) hallucinations, and a combination of visual, auditory, and tactile hallucinations (n = 1). Five patients (2 with VH only, 2 with VH and auditory hallucinations, and 1 with VH and tactile hallucinations) were also reported talking with people who were not present. Six participants had mild cognitive impairment (MCI) due to suspected AD (including two who had progressed to dementia one year after the assessment selected for this study), and 18 patients with a diagnosis of AD dementia. Subsequently, a group of 24 AD patients with no hallucinations in any sensory modality was selected to match the VH group for age, gender, years of education, MMSE and NPI total score minus the NPI hallucination sub-score. Six participants had MCI due to suspected AD (one of whom progressed to dementia three years after the assessment selected for this study), and 18 had a diagnosis of dementia due to AD. A group of matched cognitively normal (CN) participants (n = 24), with no neuropsychiatric symptoms (NPI total score equal to zero) was also identified. Data for all participants (n = 72) were part of ADNI 2 (n = 68) and ADNI 3 (n = 4).
A second sub-study included a sub-sample of patients with VH with FDG-PET available (n = 11). Six out of 11 patients with VH also presented other types of hallucinations, specifically auditory (n = 4), and tactile (n = 2). Additionally, 3 patients (1 with VH only, 1 with VH and auditory hallucinations, and 1 with VH and tactile hallucinations) were reported talking with people who were not present. Three patients had MCI due to suspected AD (of whom two progressed to dementia within a 6 to 12-month period), and 8 were diagnosed with AD dementia. A group of 11 patients with MCI (n = 2) and dementia (n = 9) due to AD with no hallucinations and a group of 11 CN with FDG-PET available were then selected to match the one with VH. Additionally, in order to explore brain metabolism in the overall group of AD patients irrespectively of hallucination status (n = 22), a group of matched CN participants (n = 22) with FDG-PET available was identified.
Statistical analyses
Differences in demographic, clinical, and neuropsychological measures between patients’ groups were assessed using IBM SPSS Statistics 22. The following tests were used as appropriate: one-way ANOVA and independent sample t-test for numerical normally distributed variables, and Mann-Whitney U and Independent-samples Kruskal-Wallis for non-normally distributed variables. The Fisher’s Exact Test was used for categorical variables. Bonferroni correction was used as a statistical method for multiple-comparison correction (statistical significance reached with a p value <α/n, where α is equal to the p value for each comparison (p = 0.05) and n the number of comparisons).
MRI and FDG-PET imaging and analyses
MRI acquisition protocols are available at http://adni.loni.usc.edu/methods. VBM pre-processing and statistical analyses were carried out using the Statistical Parametric Mapping (SPM) 12 software (Wellcome Centre for Human Neuroimaging, London, UK), running on MATLAB R2014a, version 8.3 (The MathWorks, Icn, Natick, MA). Structural MRI data were manually reoriented to the Anterior Commissure-Posterior Commissure line, segmented into GM, white matter (WM), and cerebrospinal fluid (CSF), spatially normalized to the Montreal Neurological Institute (MNI) space, modulated and smoothed using a full width half maximum (FWHM) 8 mm isotropic Gaussian kernel. Total GM, WM, and CSF volumes were determined from each image in native space using the MATLAB ‘get_totals’ script http://www0.cs.ucl.ac.uk/staff/g.ridgway/vbm/get_totals.m. Total intracranial volume (TIV) was calculated by summing GM, WM, and CSF total volumes for each patient. A GLM analysis with TIV and age as covariates of no interest was carried out to explore pair-wise between-group differences: VH versus NVH, VH versus CN, NVH versus CN. A confirmatory analysis was carried out selecting only patients with VH but no hallucinations in other sensory modalities (n = 12) and matched participants in the NVH and CN groups. Relative threshold masking of 0.2 was applied for GM map analysis. Cluster-forming significance thresholds were p < 0.05 FWE-corrected for the full analysis, and p < 0.0001 for the VH-only sub-study, and the cluster-level threshold was p < 0.05 FWE-corrected for multiple comparisons. MNI coordinates were converted into Talairach coordinates using GingerALE, version 2.3.6 http://www.brainmap.org/ale/, and brain region labels were determined with the Talairach Client, version 2.4.3 http://www.talairach.org/client.html.
All FDG-PET images had been quality controlled by the ADNI PET core team, and pre-processed to harmonize images from different scanners [30]. Details on PET acquisition and pre-processing are described at http://adni.loni.usc.edu/methods/pet-analysis-method/pet-analysis. Pre-processed FDG-PET images underwent additional processing steps using SPM12. Firstly, each image was co-registered to the corresponding structural MRI scan and resliced using a trilinear interpolation. The output images were inspected visually to check for the accuracy of this process. Co-registered images were then affine registered into the MNI space using the International Consortium for Brain Mapping (ICBM) standard template available in SPM, with 16 non-linear iterations and non-linear regularization set to 1. Images were resliced by means of a trilinear interpolation and no modulation was applied. Within this step, an FDG-PET template developed for patients with dementia was used, available for download as an extension of SPM at https://www.fil.ion.ucl.ac.uk/spm/ext [31]. Images were also intensity normalized to reduce the effect of inter-individual differences in brain metabolism by using the cerebellum as reference region. To do so, an area in the superior cerebellum, including the vermis, as identified by Rasmussen et al. [32] was used, including the following Automated Anatomical Labelling (AAL) atlas regions: cerebellum III, IV, V, VI, and the whole vermis. Firstly, a mask based on these regions was created with the WFU PickAtlas toolbox, and the signal was extracted for each participant using the MarsBaR (MARSeille Boîte À Région d’Intérêt) toolbox. Then, the entire FDG-PET image for each participant was intensity normalized to the cerebellar region of interest (ROI) mean signal using the SPM12 ImCalc tool. Finally, the images were smoothed using a FWHM 8 mm isotropic Gaussian kernel. All pre-processed images were then used for between-group comparisons of hallucinating and non-hallucinating patients, with TIV and age as covariates of no interest. Similarly, an additional confirmatory sub-group analysis was carried out focusing on patients with hallucinations in the visual modality only (n = 5). Cluster-forming significance levels were set at p < 0.001 for all analyses (except for the GM map comparisons between AD groups and CN, for which an FWE-corrected cluster-forming threshold p < 0.05 was used) and the cluster-level significance threshold was set at p < 0.05 FWE-corrected for multiple comparisons. Further analyses were run comparing AD sub-groups and CN participants, reported in the Supplementary Material. Since hallucinations manifest especially in later disease stages, all voxel-based analyses were replicated by excluding patients with MCI; these analyses are also reported in the Supplementary Material.
Additionally, we carried out some post hoc analyses adopting a region-of-interest (ROI) approach. For these additional analyses, 14 ROIs (7 right-sided and 7 left-sided) in occipito-temporal areas that appeared to be more significantly affected in the AD VH group were selected, namely: the calcarine cortex, the cuneus, the inferior, middle and superior occipital gyri, the fusiform and lingual gyri. Additionally, we also selected 4 control regions more affected by AD pathological changes, i.e., left and right hippocampi and posterior cingulate cortices. The AAL atlas 2 [33] was used to identify these ROIs and create the binary masks to extract GM volumes and values of FDG-PET signal for all of the participants. ANOVA was used to compare both GM volumes and values of FDG-PET signal across participant groups. Correlations between GM volume and metabolism were also investigated for each ROI in the three separate groups (11 VH, 11 NVH, and 11 CN) and in the whole sample of participants with PET images irrespectively of diagnosis (n = 33).
Biomarkers
Low levels of CSF Amyloid-β 1-42 (Aβ1 - 42) have been associated with cerebral Aβ deposition and represent a valid in vivo biomarker of AD pathology [34, 35]. Thus, we checked whether CSF Aβ1 - 42 and/or florbetapir (18F-AV45) PET scans were available for all the participants. Methodology has been described in detail elsewhere [10, 36]. CSF Aβ1 - 42 was considered abnormal at a cut-off of 977 pg/mL or below [37], while florbetapir PET images were considered abnormal with a standardized uptake value ratio (SUVR) above the cut-off of 1.11 [36].
Additionally, we also extracted data on CSF levels of phosphorylated tau (p-tau), a biomarker of fibrillary tau pathology [35]. Values of the p-tau/Aβ1 - 42 ratio above the cut-off of 0.025 were considered abnormal [37]. Biomarker data closest in time to the date of MRI/FDG-PET assessments wereincluded.
Post hoc neuropathological diagnosis checking
Since VH have been found to be a strong predictor of LB pathology at autopsy, we checked post hoc the neuropathological status of AD patients included in the present cohort. Methodology has been described in detail elsewhere [10].
RESULTS
Demographic, neuropsychiatric, and neuropsychological findings
AD patients with and without VH, and CN did not significantly differ in age, gender, and years of education. Post hoc analyses (Dunn’s pairwise test) on the MMSE scores revealed differences between both AD sub-groups and CN (p < 0.001), but not between AD VH and NVH (p = 1.00). Some patients presented tremor (3 VH and 2 NVH), gait abnormalities (4 VH and 1 NVH), and one patient without VH presented both. Detailed demographic and clinical features are reported in Table 1. Moreover, no significant differences were observed in pharmacological treatments between patient groups (Supplementary Material).
Demographic, clinical and volumetric characteristics of AD patients with and without VH and CN. Mean and SD are reported for each variable unless otherwise specified
AD, Alzheimer’s disease; CN, cognitively normal; CSF, cerebrospinal fluid; GM, gray matter; NPI, neuropsychiatric inventory; NVH, no visual hallucinations; VH, visual hallucinations; WM, white matter. aOne-way ANOVA; bIndependent-samples Kruskal-Wallis test; cMann-Whitney U test; dFisher’s Exact Test.
Independent-sample Kruskal-Wallis tests, comparing AD VH, NVH, and CN, yielded significant results in all neuropsychological measures (p≤0.001). Post hoc analyses (Bonferroni adjusted p-values from Dunn’s pairwise tests) are reported in Table 2. In the direct comparison between AD VH and NVH, significant differences were only detected on the CDT - copy, a measure of visuoconstructive abilities, and on both parts of the TMT, a test of visuo-spatial attention and executive function, but these differences were not statistically significant after applying Bonferroni correction for multiple comparisons across neuropsychological tests (significance threshold at p < 0.005). However, when compared with the CN, only hallucinating patients showed statistically significant deficits in the CDT - copy (Table 2 and Fig. 1).
Differences in neuropsychological tests between AD VH, AD NVH and CN (Kruskal-Wallis test). Bonferroni adjusted p-values from Dunn’s pairwise tests (post hoc comparisons) are reported
AD, Alzheimer’s disease; BNT, Boston naming test; CN, cognitively normal; CFT, category fluency test; HC, healthy controls; M, memory; NVH, no VH; s, seconds; RAVLT, Rey Auditory Verbal Learning Test; SD, standard deviation; TMT, Trail Making Test; VH, visual hallucinations.
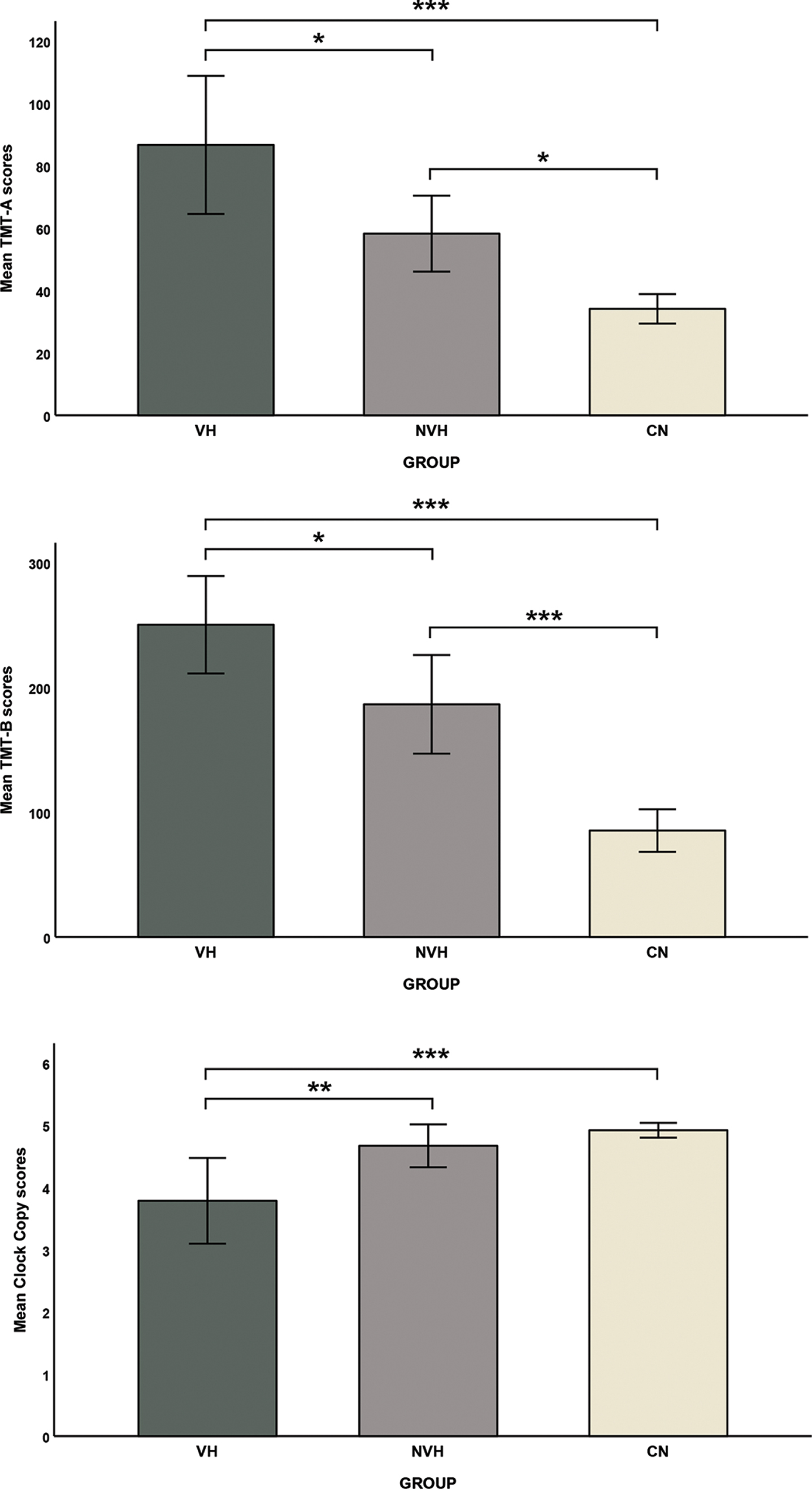
Differences between AD VH, AD NVH, and CN on the Trail Making Test –part A and B and the Clock Drawing test - copy. *p < 0.05, **p < 0.01, ***p < 0.001 (surviving Bonferroni correction).
Whole brain VBM findings
Whole brain VBM analysis of GM yielded no significant results between AD patients with and without VH. When compared with CN, analysis of both patient sub-groups revealed regions of lower GM volume (Tables 3 and 4 and Fig. 2).
Regions of lower gray matter volume in AD VH patients compared with CN (FWE-corrected cluster-level threshold of p < 0.05 with TIV and age as covariates of no interest, k > 20)
AD, Alzheimer’s disease; CN, cognitively normal; BA, Brodmann area; L, left; R, right; VH, visual hallucinations; TIV, total intracranial volume; k, cluster-extent based threshold; acluster-level FWE corrected p value.
Regions of reduced gray matter volume in AD NVH patients compared with CN (FWE-corrected cluster-level threshold of p < 0.05 with TIV and age as covariates of no interest, k > 20)
AD, Alzheimer’s disease; CN, cognitively normal; BA, Brodmann area; L, left; R, right; NVH, no visual hallucinations; TIV, total intracranial volume; k, cluster-extent based threshold; acluster-level FWE corrected p value.
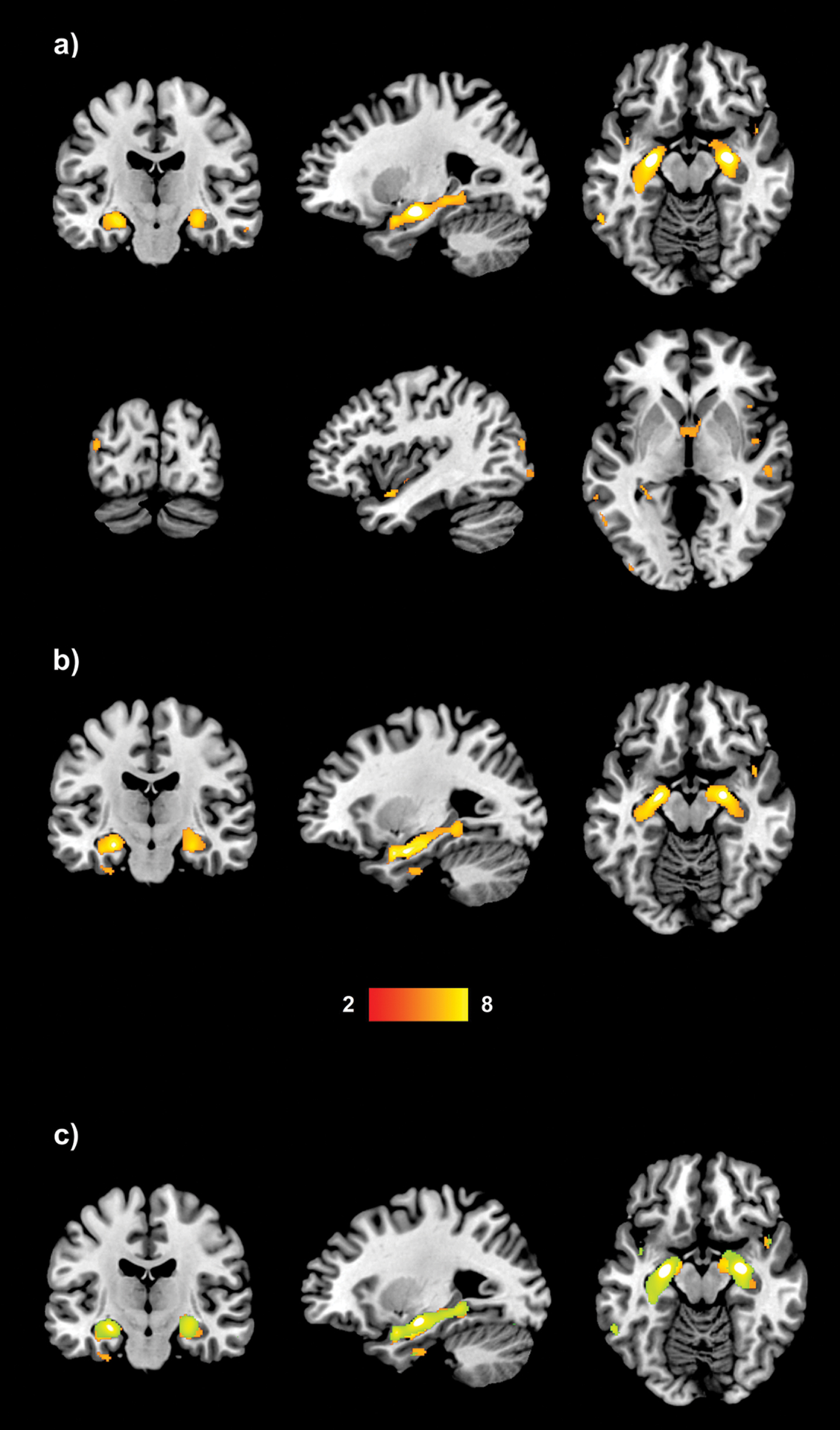
Regions of reduced GM volume in a) AD VH and b) AD NVH compared with CN (the color bar indicates the z scores with the cluster-level threshold of p < 0.05 FWE-corrected for multiple comparisons, with TIV and age as covariates of no interest); and c) regions of overlapping GM loss in VH and NVH patients (yellow), NVH only (red) and VH (green).
Overlapping regions of GM loss were located in medial and lateral temporal regions, namely the parahippocampal gyrus and middle temporal gyrus bilaterally, left inferior temporal gyrus, right superior temporal gyrus (Fig. 2). Other common areas of reduced GM volume were the following: thalamus and insula bilaterally, and right caudate nucleus, inferior frontal and supramarginal gyri. Additional regions of reduced GM were detected in VH patients in the bilateral middle occipital gyri and in the right anterior cingulate. Decreased volume in temporal regions in patients with no VH extended to the left superior temporal gyrus and uncus. Moreover, they presented GM loss in left parietal regions.
Sub-group analyses restricted to patients with hallucinations in the visual modality only showed similar results. In fact, when compared with CN, the two patient groups presented with divergent patterns of atrophy: mainly in bilateral posterior temporo-occipital and parietal regions for AD VH and in temporal, parietal and frontal areas for the AD NVH (Supplementary Material). Similar results emerged when analyses were restricted only to patients with a diagnosis of dementia excluding those with MCI (Supplementary Material).
PET findings
Demographic, clinical, and neuropsychological feature details of this sub-sample of participants, and results of FDG-PET analyses comparing AD patients and CN are reported in the Supplementary Material. No regional differences in brain metabolism were found between AD VH and AD NVH groups. However, when patient groups were compared with CN, the AD VH sub-group showed hypometabolism in bilateral posterior occipito-temporal cortices, in the posterior cingulate, precuneus and cerebellar areas, while the AD NVH presented with hypometabolism in bilateral inferior and medio-temporal areas only (Table 5 and Fig. 3).
Regions of hypometabolism in AD patients with and without VH independently compared with CN (FWE-corrected cluster-level threshold of p < 0.05 with TIV and age as covariates of no interest)
AD, Alzheimer’s disease; BA, Brodmann area; CN, cognitively normal; L, left; R, right; TIV, total intracranial volume; VH, visual hallucinations; TIV, total intracranial volume; acluster-level FWE corrected p value.
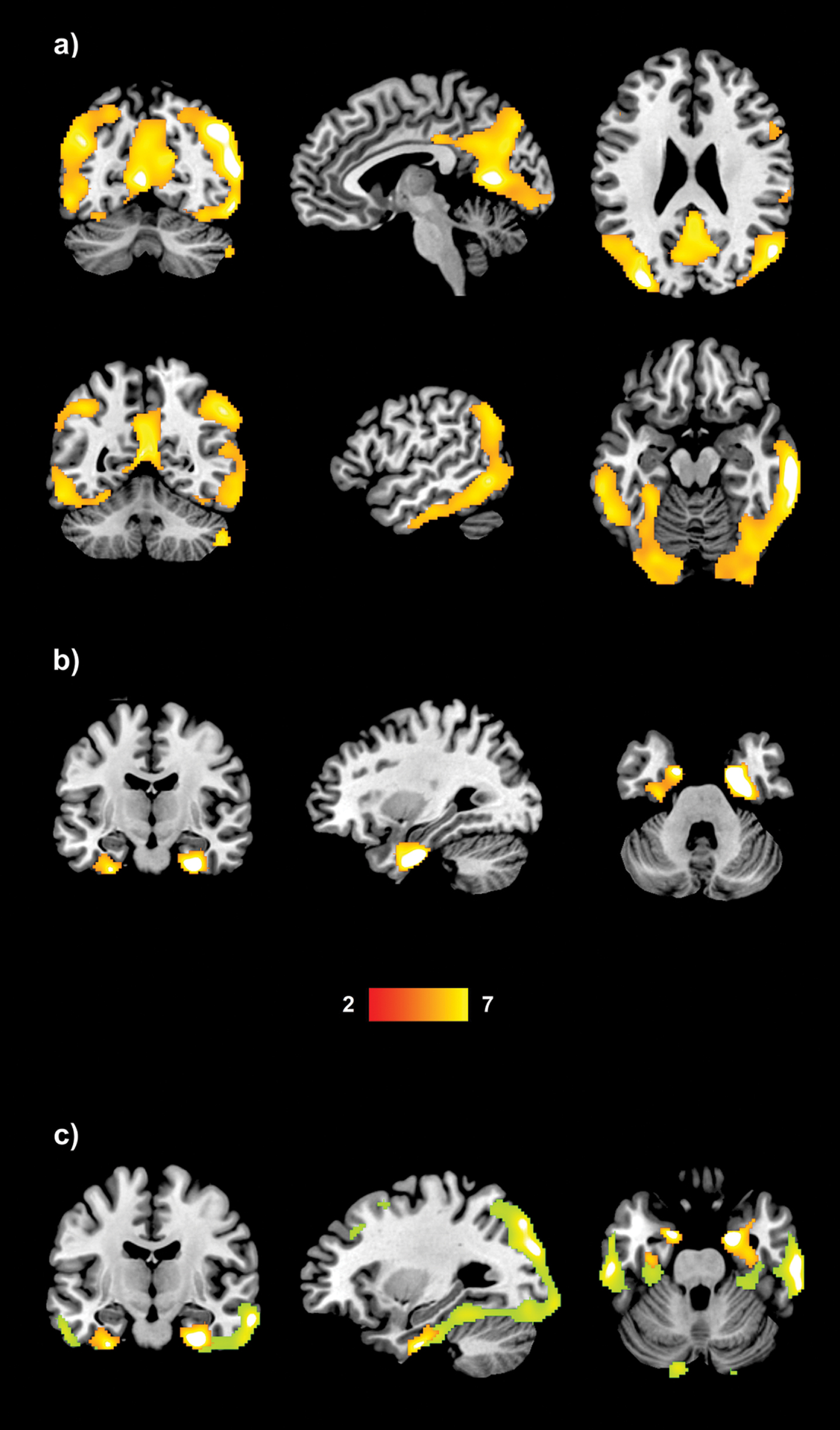
Regions of hypometabolism in a) AD VH and b) AD NVH when compared with CN (the color bar indicates the z scores with the cluster-level threshold of p < 0.05 FWE-corrected for multiple comparisons, with TIV and age as covariates of no interest); and c) regions of non-overlapping hypometabolism in NVH (red) and VH patients (green).
Confirmatory sub-group analyses of the patients with only VH showed that AD VH had widespread hypometabolism, when compared with CN, in left-lateralized occipito-temporal regions. No differences were found between AD NVH and CN (Supplementary Material). Similar results emerged from the analyses restricted to patients with a diagnosis of dementia only (Supplementary Material).
Post hoc ROI findings
No significant differences in ROI GM volumes were found between patient groups, while the VH group showed more consistent and severe GM volume loss in most occipital areas compared with the CN group (Supplementary Table 8). Both patient groups showed hippocampal atrophy, while GM reductions in the posterior cingulate cortex were significant only in the NVH versus CN comparison. FDG-PET ROI analyses, instead, showed that the VH group presented with hypometabolism in occipital (bilateral calcarine and cuneus) and occipito-temporal (left lingual gyrus) when compared with the NVH group (Supplementary Table 8). Hypometabolism was also observed in all the other occipital ROIs in the VH versus CN contrast only. Moreover, although no significant differences were observed between patient groups, the NVH group showed more severe hypometabolism in both hippocampi and the right posterior cingulate when compared with the CN group.
Additionally, a significant association (surviving correction for multiple comparisons) between GM volume and metabolism was found for both hippocampi. These findings were significant when the whole sample was investigated, while they were not replicated in the three separate groups (Supplementary Table 9).
Biomarkers
In both sub-studies, most patients and CN had biomarkers data available (Supplementary Material). In the MRI sub-study, both patient sub-groups had lower CSF Aβ1 - 42 and higher p-tau levels, as well as higher florbetapir uptake values than CN. No significant differences were found between patient sub-groups. The proportion of patients with positive biomarkers for AD pathology (A + T+) was significantly higher than in the CN group, but no significant differences were observed between patients with and without VH.
Similar results emerged from the FDG-PET sub-study: while no differences were found between patient sub-groups, the CN group had higher CSF Aβ1 - 42 and lower CSF p-tau levels and florbetapir uptake values than patients with AD and VH. The number of patients with positive biomarkers was also higher than in the CN group, but there were no significant differences between patient sub-groups.
Neuropathological diagnosis
Results of neuropathological examinations were available only for four patients in the MRI sub-study (two with and two without VH), three of whom also had FDG-PET assessment (two with and one without VH). Gross findings included moderate cortical atrophy in the two patients with VH, one of whom also had mild hippocampal atrophy, while the other one had hypopigmentation in both the locus coeruleus and the substantia nigra. No gross findings were reported in the two cases without VH, apart from mild atherosclerosis of the circle of Willis in one case.
Microscopic findings confirmed that all four patients had a primary neuropathological diagnosis of AD, with homogeneous pathology across all cases (Thal phase 4 and Braak stage V). They all presented with frequent cortical neuritic plaques and cerebral amyloid angiopathy was reported to be moderate in one non-hallucinating patient and mild in two patients (one with and one without VH).
All patients had mild arteriolosclerosis mainly as mineralization of blood vessels, observed in both patients without VH and in the patient with VH. The latter also presented with mild acute/subacute microinfarcts and with remote ischemic foci in the hippocampus (CA1 region).
LB pathology was present in the amygdala of one patient without VH, while TDP-43 immunoreactive inclusions were observed in both hallucinating patients in the amygdala and the entorhinal/inferior temporal cortex (both cases), the hippocampus (one case), and the neocortex (one case). Mild neuronal loss in the substantia nigra was also observed in both cases without VH and the patient with VH. Moreover, one of the hallucinating patients had pathological changes in WM. Hippocampal sclerosis and frontotemporal lobar degeneration with tauopathy was not present in any of the 4 patients.
DISCUSSION
The first aim of the present study was to explore the neuropsychological correlates associated with VH in a sample of participants with MCI and dementia due to AD. In the direct comparison between patients with and without VH, the CDT - copy (assessing visuoconstructive abilities) and both parts of the TMT (assessing visuospatial attention and executive functioning) suggested more severe deficits in the AD VH group. Interestingly, non-hallucinating patients performed similarly to CN controls on the CDT - copy, suggesting that a combination of more severe visuoconstructive and visuospatial attention impairments may be associated with the clinical manifestation of VH. Lower scores on the Rey figure copy, assessing visuoconstructive abilities, have been detected previously in association with VH in hallucinating Parkinson’s disease (PD) and DLB patients [38–41], and other studies identified visual perception impairments in patients with VH in PD and DLB [42–44]. Deficits in visual attention in PD and DLB patients with VH have also been reported [28, 46]. These findings, together, are in line with the PAD model that proposes that VH result from the combination of visual perception and attention impairments [27]. In the present study, however, none of the cognitive tests can be considered a pure measure of visuoperceptive abilities. In fact, the CDT - copy is a visuoconstructive task that relies on spatial attention, executive functioning, motor planning skills and constructive praxis, in addition to visuoperceptive abilities, and this should be considered while interpreting the results of the present study. This limitation is, however, due to the relatively restricted cognitive assessments available within the ADNI database. Therefore, the involvement of other cognitive functions cannot be completely ruled out, including cognitive domains that are not assessed by the neuropsychological battery used in ADNI. Moreover, measures of visual attention (e.g., TMT-A or digit cancellation), and visuoconstruction (e.g., CDT –copy or Rey figure copy) were partially different from previous studies investigating VH in DLB [28, 45] and might capture different aspects of analogous cognitive functions. Moreover, VH tend to be less severe and complex in AD compared with DLB. Differential patterns of phenomenological features, as well as different clinical diagnoses, might reflect distinct underlying neurocognitive and biological processes.
As for structural brain alterations, we expected volumetric differences in occipital and occipito-temporal brain regions in AD with VH. No differences were identified in the direct comparison between hallucinating and non-hallucinating patients, probably because the two sub-groups had very similar levels of disease severity, as suggested by the analysis of CSF and PET biomarkers for Aβ and tau pathology and subtle regional symptom related differences insufficient to survive statistical thresholding. Consistently, our voxel-wise PET analysis showed no differences in the direct comparison between AD patients with and without VH. Post hoc ROI analyses revealed hypometabolism in the occipital lobe in AD patients with VH compared with those without, mainly in primary visual areas and in the cuneus bilaterally. These results, however, did not survive correction for multiple comparisons and thus, they must be interpreted with caution. Indeed, a degree of occipital hypometabolism emerged only when patients with VH were compared with controls, while a similar comparison of patients without hallucinations and controls revealed hypometabolism in bilateral medio-temporal areas. No FDG-PET investigation has previously focused on VH in AD. Other PET and SPECT studies that have explored hallucinations in AD have reported conflicting results, including frontal altered glucose metabolism and reduced parietal blood flow [14, 25]. Contrasting findings may be due to methodological and clinical differences between studies, including those not distinguishing between hallucinations in different sensory modalities [14, 25]. Occipital/occipito-temporal atrophy has been related to VH in previous studies of patients with AD and PD, and hypometabolism/hypoperfusion in these regions was found in hallucinating patients with PD and DLB [21, 48]. In the present study, although the results of the independent comparisons of both AD sub-groups with CN participants seem to suggest a trend of divergent structural and metabolic alterations in VH and NVH patients (i.e., primarily occipital and temporal in VH and temporal in NVH), we detected no significant differences in the direct comparison between patients with and without VH contrary to our hypothesis. Similar findings emerged also when analyses were restricted only to patients with a diagnosis of dementia. Lack of significant results in the direct patient subgroups comparisons, therefore, suggests either that there are no detectable differences in brain structure and metabolism between AD VH and NVH or that any local symptom related differences might be subtle and insufficient to survive statistical thresholding in small samples. In fact, the small sample size may have affected our findings due to lack of statistical power, especially when comparing regional glucose metabolism, where the sub-groups were very small (AD VH, n = 11; AD NVH, n = 11). Future studies with increased statistical power may be more informative on whether there are specific differences in GM volume and glucose metabolism between AD VH and NVH, although collection of a bigger sample is complicated by the fact that this symptom is rare in AD. In addition, the chosen imaging modalities might have not been suitable to clarify the mechanisms at the basis of VH in AD. There is evidence that altered functional connectivity, detected using resting-state functional MRI (fMRI), may be related to VH in patients with PD and DLB, especially in the default mode network (DMN) [49–51]. According to Shine et al. [52], VH in PD would be facilitated by the presence of disrupted engagement of attention networks, including overactivity of the DMN. Similar mechanisms may underlie hallucinatory phenomena in AD. Notably, altered DMN connectivity has also been related to delusions in AD [53]. Resting-state fMRI studies may be more clearly informative about the dysfunctional organization of large-scale networks contributing to VH in AD, providing greater mechanistic insight than the sole investigation of structural and metabolic alterations.
The findings of the present study highlight the presence of cognitive changes in AD patients with VH similar to those usually observed in DLB. DLB and PD dementia may be defined as visuoperceptive, attentional, and executive dementias, as opposed to the more severe memory deficits observed in AD [54, 55]. In addition, occipital hypometabolism/perfusion is among the supportive biomarkers for the diagnosis of DLB [26]. Thus, the more severe deficits in visuoconstruction (CDT –copy), visuospatial attention (TMT-A) and executive functioning (TMT-B), as well as the more pronounced occipital hypometabolism in patients with AD and VH resemble the alterations usually observed in DLB, irrespectively of the presence of VH. In this study, patients with VH presented a pattern of abnormalities typical of AD, including temporal atrophy, and parietal and temporal hypometabolism. In addition, all the patients with VH who underwent either CSF or PET assessments, i.e., 22 out of 24 patients, had at least one positive biomarker of AD. Moreover, no differences in posterior cingulate metabolism (i.e., cingulate island sign) were found between patients with and without VH (Supplementary Material). Rates and types of eye diseases (primarily cataracts and decreased eyesight) were also very similar across groups (4 CN, 3 AD NVH, and 3 AD VH), thus ruling out a possible role of visual problems as the main cause of VH. Overall, these findings support a diagnosis of AD for the patients with VH included in the present study, who do not appear to be clinically defined DLB cases misdiagnosed as AD, although a possible comorbid synuclein and amyloid neuropathology cannot be ruled out. In a previous study, Chiu et al. [6] demonstrated the presence of DLB core features in AD patients with VH and the authors speculated that among AD patients with VH a high proportion could have LB-associated pathological changes. The present findings, although limited by the lack of neuropathological data, complement those reported by Chiu et al. [6], by showing visuoperceptive/visuoconstructive deficits in hallucinating AD patients, a pattern of deficits usually distinctive of DLB [26]. A previous study on an ADNI series of 22 autopsies found that all 4 patients with AD and hallucinations had concomitant diffused LB pathology, although the sensory modality of the hallucinatory phenomena was not specified [10]. In our study, none of the hallucinating patients with available neuropathological examination (n = 2) had concomitant LB pathology. Instead, TDP-43 proteinopathy was found in the medial temporal lobe of both VH patients, and vascular damage in one case, consistently with a previous study pointing at non-AD pathological changes as risk factors for psychotic symptoms in AD [56]. In the current study, autopsy was available for very few patients, only two with VH, making it difficult to draw any firm conclusions. However, VH have also been reported in pure AD cases. In fact, Thomas et al. [8] found that three out of 19 patients with autopsy-confirmed pure AD had VH that were, however, less complex than those usually observed in DLB. This finding suggests that the phenomenological features of VH may be very informative in investigating their underlying cognitive and neural mechanisms that may differ in relation to complexity and severity of the symptoms, and might also reflect different patterns of underlying neuropathological features. Given the limited neuropathological data available, it is difficult to draw firm conclusions on the specific neuropathological features related to VH in our sample. Thus, VH in AD may be due to a combination of pathologies, including AD and non-AD neuropathological changes, as well as LB-related pathology, although this hypothesis could not be tested by the present study.
Some limitations need acknowledging. Firstly, the sample size was reasonably small, suggesting a need for additional imaging studies aimed at clarifying the neural substrates of this symptom that is, however, rather rare in AD. Pathological data were available only for four patients, providing limited insight into the underlying neuropathological processes of VH in AD, but still this limited evidence might be useful in future meta-analytical reviews. This paucity of evidence highlights the need for further neuropathological studies that might contribute to clarifying the mechanisms underlying VH in AD and might test whether VH in this disease are the phenomenological outcome of a combination of pathologies. Moreover, neuropsychological assessment was limited to tests available in the ADNI cohort. Thus, some cognitive processes previously associated with hallucinations in AD, such as memory suppression, as proposed by El Haj et al. [4], could not be tested. Moreover, since the NPI was used, no information on the phenomenology of VH was included, and this may differ between conditions. Thus, it was not possible to know whether the reported visual hallucinations were complex or simple, and whether the patients also had illusions or other visual misperceptions. In addition, the NPI refers to changes in neuropsychiatric symptoms over the previous month, and thus the presence of hallucinations outside this time window cannot be completely ruled out. All patients in the NVH group, however, did not present any type of hallucinations in all the available assessments in the ADNI database. The limited time frame of the NPI assessment and the lack of other clinical records has also limited the full application of the revised criteria for diagnosis of psychosis in neurocognitive disorders [13, 17]. However, to the best of our knowledge, all patients in the VH group developed this symptom after receiving a diagnosis of neurocognitive disorder and had not been previously affected by psychiatric disorders with psychotic features, ruling out, therefore, potential etiologies for hallucinations alternative to neurodegeneration.
Given the high comorbidity of psychotic symptoms in AD, including hallucinations in different sensory modalities, it is difficult to differentiate completely the brain features underpinning these symptoms taken separately. Previous studies have investigated the brain correlates of hallucinations in AD without specifying the sensory modality [24, 25]. Other studies focusing on VH had rather small sample size (considerably smaller than the present study), and no information regarding the presence of hallucinations in other sensory modalities in addition to VH was reported [21, 22]. However, it should be noted that, in our sample, of the 24 patients with VH, 12 also presented hallucinations in other sensory modalities. Although half of the patients also presented hallucinations in other sensory modalities, all the individuals in the VH group were characterized by the presence of visual hallucinatory phenomena. In addition, 8 patients presented a fluctuating VH status, and did not present VH in at least one follow-up visit, while it was not possible to verify the presence of VH at follow-up for 11 patients. However, the presence of VH at one of the available assessments suggests that this symptom was part of their clinical phenotype. The lack of data in the ADNI database about disease duration prevented us from fully characterizing our patient samples also on the basis of this variable. However, disease duration may not be directly associated with severity of either neural damage or symptoms. It has been shown that in autopsy confirmed AD with no concomitant α-synuclein pathology and AD with LBs limited to the amygdala, an earlier VH onset was associated with greater limbic and cortical neurofibrillary tangle (NFT) density [57]. However, the same study reported no differences in Braak NFT stage between patients with and without hallucinations [57]. Although hallucinations are mainly observed in advanced disease stages in patients with AD [58], multiple genetic [59–61], personality [62], and environmental factors [63] may increase the risk of hallucination in some patients independently of disease duration or disease stage, a combination of factors that may also explain the occurrence of VH in some patients with MCI. Another limitation is that FDG-PET was available only for 11 out of the 24 AD patients with hallucination.
To our knowledge, this is the first whole brain VBM and FDG-PET study of VH in AD, a symptom that appears to be rare in AD, considering the limited number of patients experiencing VH within all the ADNI cohorts. In addition to a pattern of disease-specific abnormalities, we found more severe visuoconstructive and attention impairments in association with VH. We did not find, however, significant regional differences in GM volume and glucose metabolism in the direct comparison between patients with and without VH, but only a differential pattern of differences when each group was independently compared with cognitively healthy controls. Future multimodal neuroimaging studies with bigger sample sizes may increase our knowledge on the functional and structural brain differences contributing to the development of this symptom in AD. VH are severe and disabling symptoms, often distressing, that have been associated with increased likelihood of institutionalization and a poor response to treatment [64, 65]. Nevertheless, there is currently no effective targeted treatment, problem that is worsen further by the lack of evidence-based interventions [66, 67]. In this context, a wider knowledge of the pathophysiology underlying VH, as well as the detection of disease and symptom-specific biomarkers, might aid current research on the treatment of this symptom, by developing new targets and assessing the efficacy of existing interventions.
Footnotes
ACKNOWLEDGMENTS
Data collection and sharing for this project was funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health ![]() . The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
. The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
A.C. was supported by the “Department of excellence 2018-2022” initiative of the Italian Ministry of education (MIUR) awarded to the Department of Neuroscience - University of Padua.
The ADNI was launched in 2003 as a public-private partnership, led by Principal Investigator Michael W. Weiner, MD. The primary goal of ADNI has been to test whether serial MRI, PET, other biological markers, and clinical and neuropsychological assessment can be combined to measure the progression of mild cognitive impairment and early AD. The development and use of optimized methods have the purpose of identifying specific biomarkers of AD progression to improve its diagnosis, and to aid the development of new treatments and the assessment of their efficacy [68]. Further details and up-to-date information are available at ![]() . ADNI inclusion and exclusion criteria are stated in the procedure manuals and clinical protocols available at http://adni.loni.usc.edu/methods/documents. Written informed consent was obtained from all ADNI participants, and study protocols were approved by each participating site’s institutional review board. All methods were carried out in accordance with the relevant guidelines and regulations. For research governance and compliance with ethical standards and informed consent please consult the ADNI website at http://www.adni-info.org
. ADNI inclusion and exclusion criteria are stated in the procedure manuals and clinical protocols available at http://adni.loni.usc.edu/methods/documents. Written informed consent was obtained from all ADNI participants, and study protocols were approved by each participating site’s institutional review board. All methods were carried out in accordance with the relevant guidelines and regulations. For research governance and compliance with ethical standards and informed consent please consult the ADNI website at http://www.adni-info.org