
Abstract
The aim of this study is to determine if there is an association between atrial arrhythmias and brain amyloid-β (Aβ), measured on florbetapir (FBP) PET. 346 nondemented participants from the Atherosclerosis Risk in Communities study underwent FBP-PET, 185 also wore Zio® XT Patch. The associations between global cortical Aβ (> 1.2 standardized uptake value ratio) and history of atrial fibrillation, zio-defined atrial tachycardia and premature atrial contractions, each, were evaluated. Among nondemented community-dwelling older adults, we did not find an association between atrial arrhythmias and Aβ. Other brain pathology may underlie the association described between atrial arrhythmias and cognition.
INTRODUCTION
Atrial fibrillation (AF) has been suggested as an independent cardiovascular risk factor for accelerated cognitive impairment and dementia [1]. The mechanisms for this remain unclear; whether AF-related ischemic stroke, silent infarction, hypoperfusion, inflammation, or some combination therein directly contributes to brain morphologic changes remains to be determined [2]. AF as a diagnostic entity is also dynamic, and there are increased calls to consider AF along a spectrum, rather than as a binary entity [3]. The presence of other atrial arrhythmias such as premature atrial contractions (PACs) or the amount of time one has atrial tachycardias (AT) could also be important given they represent another measure of atrial dysfunction, or an intermediary to AF and might provide additional information. We recently reported from the Atherosclerosis Risk in Communities (ARIC) study that compared to individuals with minimal PACs (< 1%), those with frequent PACs (> 5%) had lower executive function, lower global cognitive function, and higher odds of dementia or mild cognitive after multivariable adjustment, including adjusting for stroke [4]. Additionally, PACs have been associated not only with AF, but also with mortality [5].
A prevalent form of dementia is Alzheimer’s disease (AD), with AD classically defined pathologically by the presence of amyloid-β plaques (Aβ) and neurofibrillary tangles [6]. One way to evaluate potential mechanisms by which atrial arrhythmias might impact cognition and increase dementia risk is to consider specific markers of disease processes that impact cognition. Nuclear imaging tracers that bind to Aβ now allow quantitative measurement of AD-specific pathology.
Although demonstrating an association between atrial arrhythmias and an imaging marker of brain amyloid does not rule out other mechanisms connecting the two (including shared, confounding risk factors), evidence of elevated brain amyloid in individuals with atrial arrhythmias would emphasize importance of treatment and prevention of atrial arrhythmias. The aim of this study is to evaluate, among nondemented individuals in the ARIC-PET study who underwent cerebral Aβ imaging (florbetapir PET), the association between prevalent AF and other atrial arrhythmias and Aβ deposition. We hypothesize that global cortical Aβ will be elevated in individuals with AF, those with frequent PACs and those with a higher AT burden.
METHODS
ARIC is a community-based cohort study whose methods have been described in detail elsewhere [7]. In addition to the parent ARIC study, the ARIC Neurocognitive study enrolled patients for detailed cognitive assessments and magnetic resonance imaging, of whom 346 non-demented individuals (cognitively normal, and mild cognitive impairment (N = 86)) were recruited to undergo florbetapir positron emission tomography (PET) imaging, in the ARIC-PET ancillary study (2011–2013, concurrent with ARIC visit 5) [8]. A total of 4,003 participants attended visit 6 (2016-2017) and were invited to wear a Zio® XT Patch for 14 days, of whom 185 consenting participants overlapped with ARIC-PET (Fig. 1). Full details regarding the Zio® protocol have been previously described [9]. All ARIC participants who attended visit 6 were eligible to wear a Zio® XT Patch unless they already had an implantable cardiac device or had a history of allergic reactions to skin adhesive.
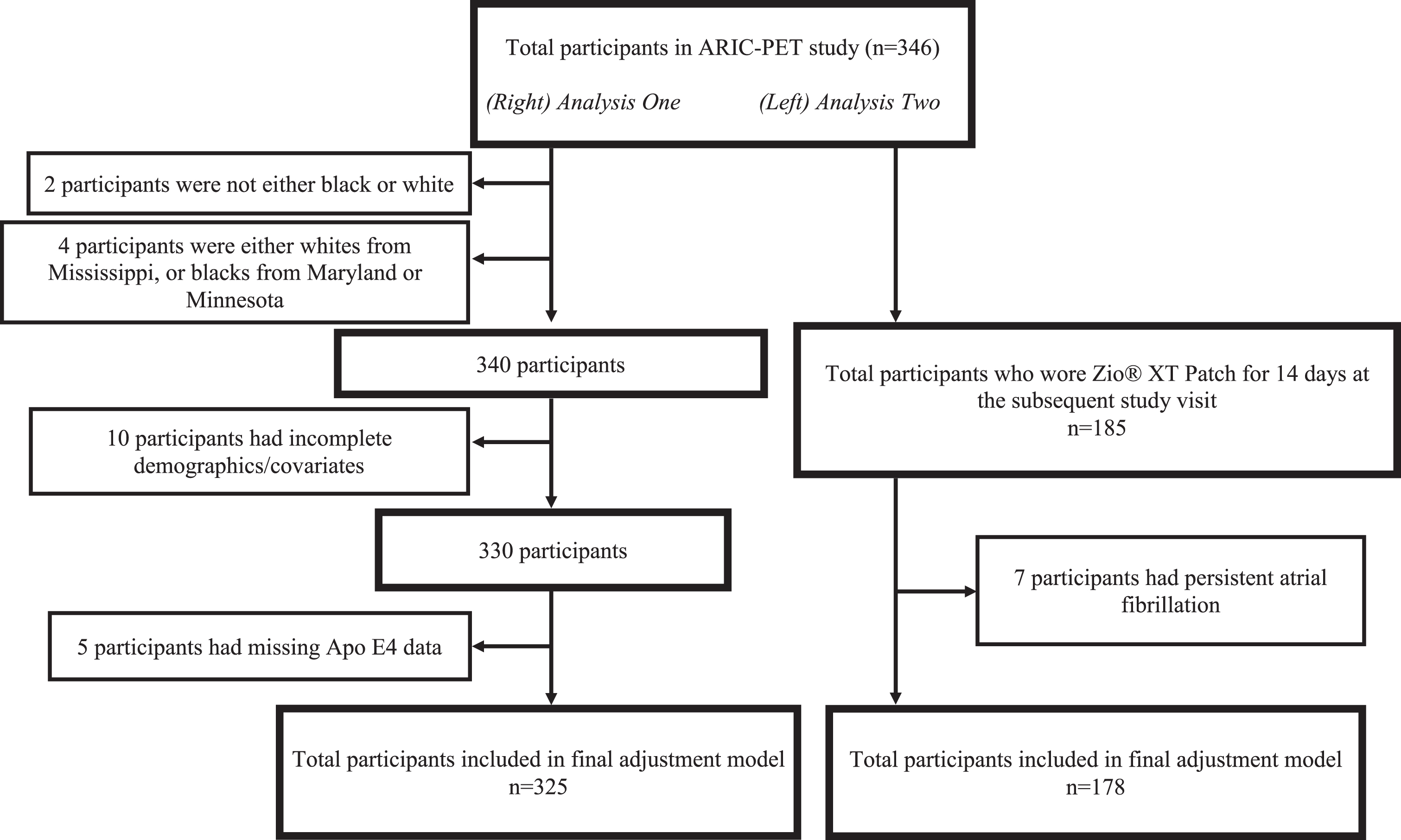
Flow diagram of study participants demonstrating overlap between analyses, and reasons for study exclusion.
Atrial arrhythmias
AF was defined as prevalent AF up to the end of visit 5 (2011–2013). Adjudication of AF has been previously described and was determined using 12-lead ECG reports, and International Classification of Disease diagnosis codes for AF in prior hospitalizations [10]. AT and PAC frequency measures were derived from the Zio® XT Patch. Number of PACs was calculated based on the number of isolated, couplet, and triplet PAC per day utilizing the following equation: PAC count per day = # isolated PAC + 2×(# couplet PAC) +3×(# triple PAC). PAC frequency was defined as the percent of heart beats that were PACs. AT, which is defined by narrow complex tachycardia > 4 beats with a rate > 100 bpm, was analyzed as the number of episodes per day. When considering PACs, participants with persistent AF were excluded because it is not possible to measure PAC frequency in this setting.
Florbetapir PET
Radioisotope (florbetapir (FBP) was administered at the three enrolling sites with a butterfly needle for the 20 min (4×5 min) uptake scan, with image acquisition between 50–70 min. The Johns Hopkins University Department of Radiology, Section of High Resolution Brain PET imaging core reviewed all scans for image quality and conducted measurements of standardized uptake value ratios (SUVRs) as has been previously reported [11]. The primary unit for analysis was a weighted average of 9 brain regions (orbitofrontal, prefrontal, superior frontal cortices, lateral temporal, parietal and occipital lobes, precuneus, anterior and posterior cingulates) which were used to define a global cortical measure of aggregated Aβ. Elevated FBP was defined as SUVR > 1.2, the sample median, due to the highly skewed distribution of the data.
Covariates
Covariates were defined at the 5th study visit, with the exception of race, sex, and education level which were defined at ARIC baseline. Hypertension was defined as systolic blood pressure≥140 mm Hg, diastolic blood pressure≥90 mm Hg, or antihypertensive medication use. Diabetes mellitus was defined as a Hemoglobin A1C≥6.5%. Low density lipoprotein (LDL) was analyzed continuously (mg/dL), as was body mass index (BMI; kg/m2). Race was self-reported (black or white, non-black/white participants excluded, Fig. 1), as was smoking status and level of educational attainment. APOE alleles were considered for participants who gave consent for genetic data use, with alleles collapsed into a binary variable for the presence or absence of at least one APOE ɛ4 allele.
Statistical methods
For continuous variables, means and standard deviations are reported, and for categorical variables, frequencies are reported. Using multivariable logistic regression, we modeled the association of cerebral amyloid (SUVR > 1.2) with prevalent AF (Analysis One) and 1) presence of AT, 2) number of AT episodes, 3) percent time with PAC and 4) per one standard deviation increase in PAC (Analysis Two), each in separate models with adjustment for confounders. The nested adjustment models were as follows: Model 1-center*race, education (> high school graduation), sex and age, Model 2-Model 1 + BMI, current smoker, hypertension, diabetes mellitus, LDL, Model 3-Model 2 + APOE ɛ4 allele. All statistical analyses were performed using Stata v14.1. Two-sided p < 0.05 was considered statistically significant.
RESULTS
Three hundred thirty participants met inclusion criteria (325 permitted APOE ɛ4 usage), of whom 185 participants also wore Zio® XT Patch at the next study visit (Fig. 1). Eighteen participants of the overall cohort had prevalent AF, and 157 had AT. Participants has a mean age of 76 years (range 71–81 years), and the majority were White (57%), hypertensive (72%), female (57%), and not currently smoking. There were significant differences in age and diabetes among those who wore a Zio® XT Patch compared to those who did not (Table 1). All of the participants with Zio® XT Patch had PACs (N = 185), of whom 7 had persistent AF, and were therefore excluded from the PAC analysis (N = 178).
Participant demographics, comparing Zio® XT Patch wearers to non-wearers*
*χ2 was used to compare categorical variables and ANOVA for continuous variables. All values are mean (SD) unless otherwise noted. Hypertension defined as systolic > 140 mmHg, or diastolic > 90 mmHg, or use of hypertension medication. Diabetes defined as a hemoglobin A1C≥6.5%. Two-sided p < 0.05 was considered statistically significant.
There was no association found between prevalent AF and global cortical cerebral amyloid as measured by FBP PET (OR 0.67, 95% CI 0.23–1.97, Model 3, Table 2, Fig. 1-Analysis One). There was also no association between FBP SUVR among participants who had AT (OR 1.42, 95% CI 0.60–3.39, Model 3, Table 4, Fig. 1-Analysis Two) or between the number of AT episodes and FBP PET measured cerebral amyloid. When considering PACs, there was a suggestion of an increased odds of SUVR > 1.2 among those participants with per 1% increase time with PACs (OR 1.10, 95% CI 0.91–1.34, Model 3, Fig. 1-Analysis Two) and higher frequency of PACs (OR per 1 SD increase 1.18, 95% CI 0.84–1.66, Model 3, Fig. 1-Analysis Two) as measured by the Zio® XT Patch, but again not statistically significant.
Multivariable logistic regression of elevated global cortical cerebral amyloid by florbetapir PET (SUVR > 1.2) by prevalent atrial fibrillation (Analysis One N = 330) or specified Zio® XT Patch independent variable (Analysis Two N = 185, *178)
*Seven participants in persistent AF dropped from PAC analysis (N = 178); one standard deviation represents 1.74% Adjustment models: Model 1: Age (years), sex, race, education; Model 2: Model 1 + body mass index (kg/m2), current smoker, low density lipoprotein (mg/dL), diabetes (hemoglobin A1C≥6.5%), hypertensive (systolic blood pressure > 140 mmHg, or diastolic blood pressure > 90 mmHg, or use of hypertension medication), Model 3: Model 2 + APOE ɛ4 allele.
DISCUSSION
Among nondemented community-dwelling older adults, we did not find an association between atrial arrhythmias and an imaging marker of elevated cerebral Aβ. Although the literature supporting an association between AF and dementia is robust, data explaining the cause or etiology of this association are scarce. Prior work has suggested an increased risk of both AD-type dementia and vascular contributions to cognitive impairment and dementia [12], with some suggesting a higher risk of AD than other types [13], although pathologic studies demonstrate an overlap in the underlying neuropathology between the two entities.
In our study, we examined a pathologic precursor of AD, specifically Aβ as measured using FBP PET. We did not find a significant association of AF with Aβ, but we may have failed to detect an association due to power (prevalent AF cases, N = 18). It may be that such a small number of AF cases would have inflated type 1 error; however, we did not find an association and therefore did not risk stating a false positive conclusion. We also acknowledge that there may be a selection bias in who enrolled in the ARIC PET ancillary study, or the ARIC Zio-XT ancillary study, such as a survivor bias, or that those who would have developed global cortical Aβ did not survive to enroll in the study. Specifically, the population was by inclusion criteria nondemented. It also may be that we failed to capture all AF cases by only having 14 days of Zio-XT monitoring, versus long-term implantable cardiac monitoring, but this reflects real world clinical practice, and therefore we still believe our results are meaningful.
It is possible that the pathologic precursor to AD that is being captured in our analysis is not sufficient to describe the neurologic underpinnings at play in the development of cognitive decline or ultimate dementia in people with PACs, AT, or AF. As mentioned previously, there is an increased awareness of the presence of mixed dementia, with the typically considered AD pathology co-occurring with the presence of more traditionally considered vascular pathology. FBP PET is a powerful imaging tool but would not account for the full spectrum of pathologies that might underlie the known association between the AF spectrum and cognition. It has also been suggested that these pathologies play different roles in the development of cognitive decline at different ages, and given that our participants were older adults, these associations may have been different in a younger cohort.
In conclusion, we did not find an association between atrial arrhythmias and the presence of an imaging marker (FBP PET) of cerebral Aβ, a pathological precursor for AD. Over the past decades, there have been increasing data regarding a relationship between AF and cognitive decline or dementia, but many questions remain regarding the pathologic underpinnings of this association. We suggest that development of more sensitive diagnostic markers, as well as advanced imaging techniques that can account for a more complete pathologic profile, will help capture those AF-spectrum patients at risk for cognitive impairment and the underlying mechanistic cause.
Footnotes
ACKNOWLEDGMENTS
The authors thank the staff and participants of the ARIC study for their important contributions.
The Atherosclerosis Risk in Communities Study is carried out as a collaborative study supported by NHLBI contracts (HHSN268201700001I, HHSN268201700002I, HHSN268201700003I HHSN268201700005I, HHSN268201700004I). The ARIC-PET study is funded by the NIA (R01AG040282, previously to RG). Avid Radiopharmaceuticals provided the florbetapir isotope for the study, but had no role in the study design or interpretation of results. Dr. Johansen receives funding from the NINDS (K23NS112459); Dr. Gottesman received prior funding from the NIA (K24AG052573). Dr. Alonso receives funding from the NIH (K24HL148521, P30AG066511). Dr. Chen receives funding from the NIH (R01HL126637, R01HL141288, and K24HL155813)
iRHYTHM (the manufacturer of Zio©XT) did not contribute any funding nor to analysis or drafting of the manuscript in any way.
This article was prepared while Dr. Rebecca Gottesman was employed at the Johns Hopkins University School of Medicine. The opinions expressed in this article are the author’s own and do not reflect the view of the National Institutes of Health, the Department of Health and Human Services, or the United States Government.