
Abstract
Background:
Depression has been suggested to be a cause of reversible cognitive impairment but also a risk factor for neurodegenerative disease. Studies suggest that depression prevalence may be high in early onset dementia, particularly Alzheimer’s disease, but this has not been systematically assessed in a biomarker-validated clinical dementia cohort to date.
Objective:
To examine the prevalence, features, and association with amyloid pathology of lifetime depressive symptoms in a memory clinic cohort meeting appropriate use criteria for amyloid PET imaging.
Methods:
We included 300 patients from a single-center memory clinic cohort that received diagnostic biomarker evaluation with amyloid PET imaging according to appropriate use criteria. History of lifetime depressive symptoms was retrospectively assessed through structured review of clinical correspondence.
Results:
One hundred forty-two (47%) patients had a history of significant depressive symptoms (‘D+’). Of these, 89% had ongoing symptoms and 60% were on antidepressants at the time of presentation to our Clinic. Depressive symptoms were equally highly prevalent in the amyloid-positive and the heterogeneous group of amyloid-negative patients.
Conclusion:
Approximately half of patients who meet appropriate use criteria for amyloid PET have a history of depressive symptoms. We suggest that depression is an important feature of both neurodegenerative and non-neurodegenerative cognitive impairment and may contribute to the diagnostic uncertainty behind referral to amyloid PET.
Keywords
INTRODUCTION
Depressive symptoms and cognitive impairment are closely linked to each other: depression can be the cause of potentially reversible cognitive decline [1] and patients with neurodegenerative diseases often experience depressive symptoms at an early stage [2]. While a large body of evidence suggests that a link may exist between depression and Alzheimer’s disease (AD), it is still unclear whether affective symptoms represents a risk factor [3], a prodromal feature [4], or both [5]. Elevated amyloid-β (Aβ) deposition has been proposed as one of the possible mechanisms mediating this association, with studies showing that patients with a history of depression have higher levels of Aβ [6]. However, other studies have reported no [7] or negative [8] association between Aβ and depression.
Disentangling the relationship between depression and AD at an individual level is central for the optimal diagnosis and management of patients with suspected cognitive decline. AD and depression share some clinical features that can make the differential diagnosis challenging on clinical and behavioral grounds alone [9]. This has even greater implications in patients presenting with atypical clinical features, such as inconsistent patterns of cognitive impairment, young age of onset (<65 years) or multiple comorbidities, which are more likely to lead to diagnostic delays and misdiagnoses [10, 11]. Despite the potential clinical relevance, there are insufficient data on the occurrence of depressive symptoms in this clinical population. Previous studies have shown that the prevalence of neuropsychiatric symptoms is higher in clinical cohorts than in the general population [12]. However, most of these did not include systematic biomarker evaluation [13, 14], and very few of them examined both ongoing symptoms and previous history of depression [15].
In the clinical setting, patients with atypical patterns of cognitive impairment, young age of onset, and diagnostic uncertainty are potential candidates for biomarker assessment with amyloid PET [16] or cerebrospinal fluid examination for neurodegenerative biomarkers [17]. While there is a vast body of literature concerning the impact of these investigations on the diagnosis and management of this clinical population [18, 19], only few studies have systematically examined the presenting clinical features contributing to diagnostic uncertainty [20], with little or no focus on depressive symptoms.
At Imperial College Healthcare NHS Trust Memory Centre (Imperial Memory Centre, IMC) (London, United Kingdom), we have established the Imperial Amyloid PET Cohort (Imperial APC), one of the largest single-center memory clinic cohorts in Europe for the diagnostic use of biomarker assessment with clinical Amyloid PET Imaging (API) [18, 21]. In this retrospective study, we examined the prevalence of lifetime depressive symptoms and its association with AD pathology in the clinical population of patients meeting appropriate use criteria for API [16].
METHODS
Subjects
We included 300 patients from the Imperial Amyloid PET Cohort who were referred for amyloid PET imaging between March 2014 and February 2021 as part of their diagnostic investigations. Patients were not included if they had not received clinical follow-up in our center or their clinical correspondence was not available for review. As part of their clinical workup, all patients referred to the service were assessed by one of five dementia experts and decision to perform amyloid PET was made after review by a Cognitive Neuroradiology Multidisciplinary Team. The decision to carry out scanning was based on the Amyloid Imaging Taskforce’s appropriate use criteria, meaning that all patients had objective cognitive impairment which was potentially secondary to AD pathology, but diagnostic uncertainty remained after comprehensive evaluation [16]. 18F-florbetapir was used as the PET tracer until December 2017 when it was replaced with 18F-florbetaben due to its manufacture cessation in the UK. Amyloid-PET images were visually rated as ‘positive’ (Aβ-pos) or ‘negative’ (Aβ-neg) according to manufacturers’ guidelines by an experienced nuclear medicine radiologist using greyscale images and the cerebellum as the reference region.
Ethics permission was granted by the Camden and Kings Cross UK Research Ethics Committee (REC number 20/LO/0442) in June 2020.
Assessment of depressive symptoms
All patients had a comprehensive clinical assessment, including medical history review, patient and caregiver interview, neurological examination, and assessment of ongoing cognitive problems, in addition to structural brain imaging. The clinical letters and results of all investigations are stored electronically within the Imperial College Healthcare NHS Trust’s electronic patient record, allowing us to investigate retrospectively whether patients referred to our Clinic had a history of previous or ongoing depressive symptoms. In this study, we performed a structured review of all patients’ clinical notes and correspondence, as well as referral letters, neuropsychological reports, and results of previous external investigations when available. Here we refer to depressive symptoms as any signs of low mood throughout the individual’s lifespan (previous or ongoing) that were severe enough to be discussed in the clinical notes by the referring clinician and/or dementia expert. Ambiguous cases were discussed with the clinical and research teams. Patients were classified as ‘D+’ when depressive symptoms were reported in the diagnosis list or in the text of a clinician’s notes and if the onset preceded presentation to our Clinic. The subgroup of D+ patients whose depressive symptoms were described by the clinician as ongoing at the first IMC visit were classified as ‘D+ ongoing’. When available, we also extracted from clinical reports the age of onset of depressive symptoms, whether these required psychological and/or pharmacological treatment, and the relative antidepressant category. Patients without any evidence of a history of depressive symptoms were classified as ‘D–’, along with those patients whose clinical notes suggested that depressive symptoms appeared at follow-up visits rather than at presentation. If depressive symptoms were recorded at the first but not at follow-up visits, patients were categorized as ‘D+ ’ as long as there was clear evidence that the onset preceded presentation to our Centre. This conservative approach ensured exclusion of those patients whose symptoms might have resulted from a reaction to the cognitive impairment experienced. Lastly, we also recorded if patients had symptoms of anxiety that preceded or were ongoing at the first visit to our Centre.
Diagnostic categorization
Within the clinical setting and in line with appropriate use criteria [16], a positive amyloid PET scan is highly suggestive of underlying AD. On the other hand, a negative amyloid PET essentially excludes a diagnosis of AD but does not further clarify the underlying cause of cognitive impairment. Where possible, we retrospectively classified amyloid-negative patients as ‘stable/non-neurodegenerative’ or ‘progressive/other-neurodegenerative’ as described elsewhere [20]. The ‘stable’ group included patients for which the results of cognitive investigations and clinical follow-ups were suggestive of a non-neurodegenerative cause of cognitive impairment, which was of either indeterminate or psychological nature. The ‘progressive’ group included patients with clear evidence of clinical progression, defined as decline in cognition and/or independent functioning, over clinical follow-ups due to an underlying neurodegenerative process. Within this group, we also recorded the final clinical diagnosis reported by the dementia expert in the clinical correspondence.
Statistical analysis
Patients were grouped on the basis of amyloid PET results (Aβ-pos versus Aβ-neg) or depressive symptoms (D+ versus D–) and, where relevant, analyses were repeated on the subgroup of D+ patients with ongoing symptoms (D+ ongoing versus D–). We compared the demographic and clinical characteristics between groups using independent t-test for continuous variables and Pearson’s χ2 test for categorical variables. The association between amyloid PET results and depressive symptoms was investigated using Pearson’s χ2 test. In the D+ group, we used Mann-Whitney U test and Pearson’s χ2 test to respectively investigate the association of amyloid PET results with age of onset of depressive symptoms and pharmacological treatment. In the Aβ-neg group, we investigated whether a history of depressive symptoms was associated with the final diagnosis (stable non-neurodegenerative vs progressive other-neurodegenerative) using Pearson’s χ2 test.
Data availability
Data not provided in the article are available upon reasonable request.
RESULTS
Group-level demographic information is provided in Table 1. Patients were referred from general neurology clinics (37%), GP practices (34%), external memory clinics (13%), mental health clinics (2%) or other practices (14%).
Sample characteristics
Aβ, amyloid-β; D+, with history of depression; D–, without history of depression; AD, Alzheimer’s disease; MCI, mild cognitive impairment; DLB, dementia with Lewy bodies.
Depression prevalence and features
One-hundred-and-forty-two (47%) patients had a history of significant depressive symptoms and were classified as ‘D+’ (Fig. 1). These patients did not differ from those without history of depression (D–) in age (mean±SD: D+ 66.71±8.95 years, D–67.66±9.29 years, t (298) = –0.89 p = 0.37) or sex (% female: D+ 47.2%, D–43.7%, χ2 (1) = 0.372 p = 0.54). Of the 142 D+ patients, a total of 126 (89%) were classified as ‘D+ongoing’, meaning that clinical evaluation at the time of the first visit to our Centre highlighted ongoing depressive symptoms. This was further corroborated by the finding that, at the first IMC visit, pharmacological treatment for depression was ongoing for 78 (62%) patients and prescribed to 19 (15%) patients (Fig. 2A). Additional information on the types of antidepressants is provided in Fig. 2B; antidepressants that were prescribed to treat medical conditions other than depression (e.g., amitriptyline for migraine) were not considered. The subgroup of patients with ongoing depressive symptoms did not differ from D–patients in age (mean±SD: D+ ongoing 66.8±8.83 years, D–67.66±9.29 years, t (282) = –0.8 p = 0.42) or sex (% female: D+ ongoing 44.4% D–43.7%, χ2 (1) = 0.017, p = 0.896). Information regarding the age of onset was available for 91 (64%) D+ patients: depressive symptoms started between 18 and 45 years for 18.7%, between 46 and 65 years for 52.7% and between 66 and 85 years for 28.6%, with an overall mean age of onset of 58.03 (±13.18) years. Thus, in the ‘D+ongoing’ group, the onset of depressive symptoms preceded amyloid PET scanning by 7.61±8.74 years. In the ‘D+not-ongoing’ group (n = 16), depressive symptoms were last active within 5 years from presentation to our Clinic for 9 (56%) patients, between 6 and 10 years for 3 (19%) patients and over 10 years for 2 (13%) patients; this information was not available for the remaining 2 (13%) patients. For 63% of the D+ sample (n = 90), we were able to determine the approximate duration of depressive symptoms which was on average 8±11 years (median: 5 years). A total of 33 (23%) D+ patients had received psychological input for depression. Sixty-five (44.8%) D+ patients reported concomitant symptoms of anxiety compared with 20 (12.7%) in the D–group.
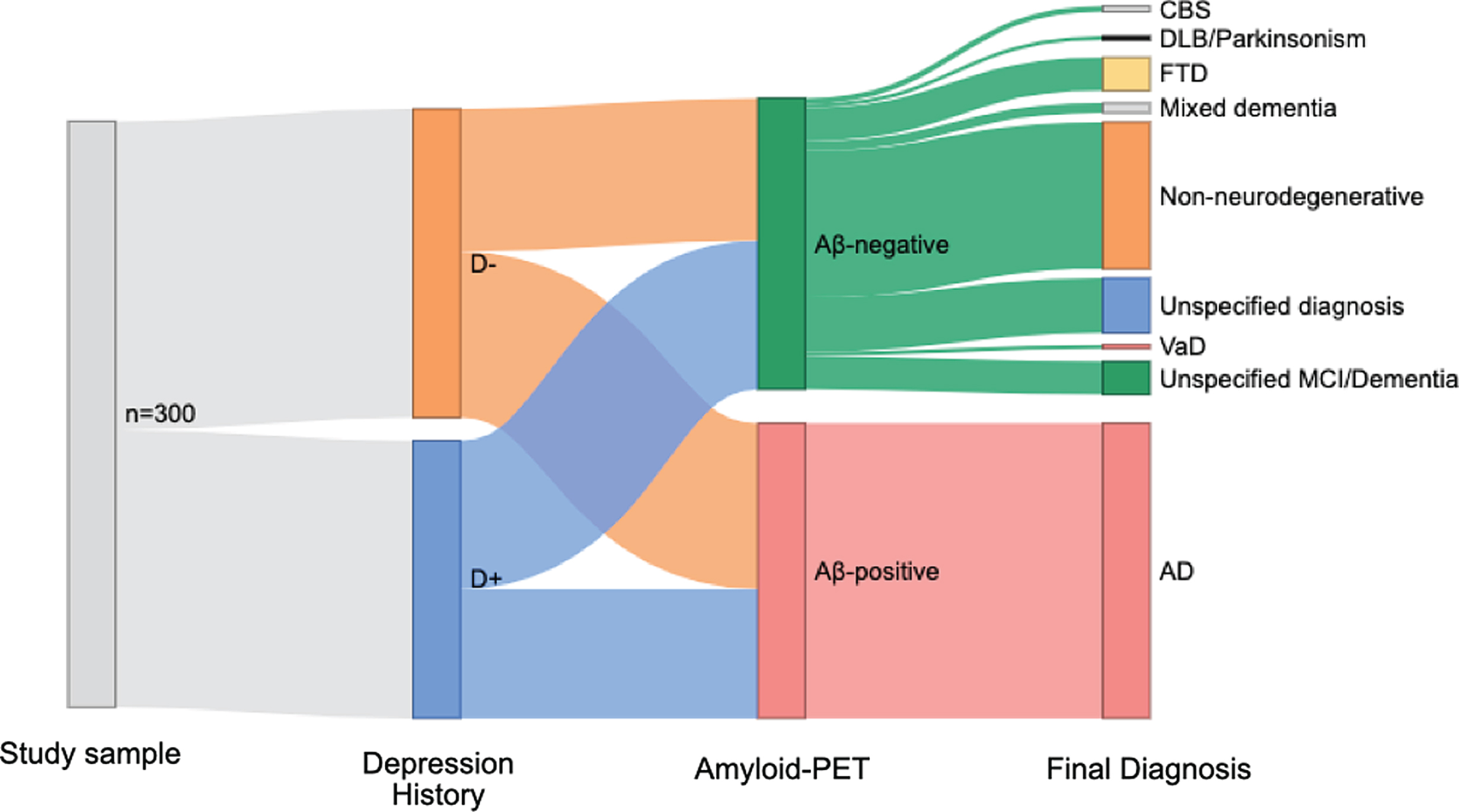
A Sankey diagram showing the distribution of study sample (n = 300) according to depression history, amyloid PET results, and final clinical diagnosis. Aβ, amyloid-β; D+, with history of depression; D–, without history of depression; CBS, corticobasal syndrome; DLB, dementia with Lewy bodies; FTD, frontotemporal dementia; VaD, vascular dementia; MCI, mild cognitive impairment; AD, Alzheimer’s disease.
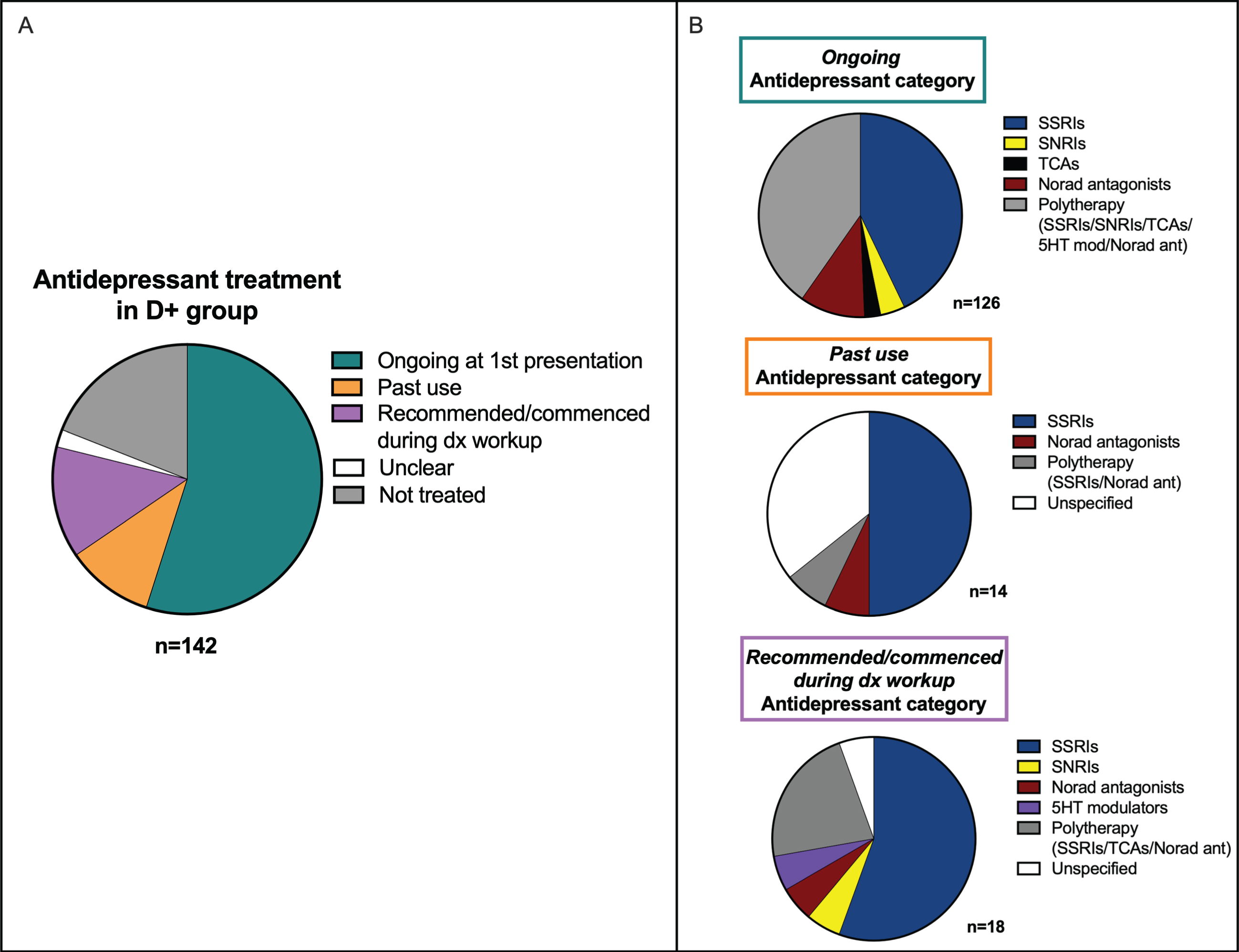
A) Description of antidepressant usage in the D+ group. B) Breakdown of antidepressant categories according to whether treatment was ongoing, preceded or followed the first visit to our Centre. D+, with history of depression; D–, without history of depression; SSRIs, selective serotonin reuptake inhibitors; SNRIs, serotonin and norepinephrine reuptake inhibitors; TCAs, Tricyclic antidepressants; Norad, noradrenergic; 5HT, serotoninergic receptors.
Depression and amyloid-PET results
Amyloid-positive and amyloid-negative patients were comparable for age (mean±SD: Aβ-pos 67.59±8.37 years, Aβ-neg 66.83±9.85 years, t (298) = 0.72 p = 0.47) but not for sex (% F: Aβ-pos 53.6% Aβ-neg 36.9%, χ2 (1) = 8.47 p = 0.004), with a higher proportion of females in the positive group. Amyloid-PET positivity was not associated with a history of depressive symptoms (Aβ-pos 43.7% Aβ-neg 51.01%, χ2 (1) = 1.6, p = 0.21) (Fig. 1), regardless of whether these were ongoing at presentation to our Centre (χ2 (1) = 2.45, p = 0.12). That is, patients with evidence of previous or ongoing symptoms of depression were not more or less likely to show increased levels of Aβ deposition. In the D+ group, the mean age of onset of depressive symptoms did not differ significantly between Aβ-pos (mean±SD: 59.1±12.3 years) and Aβ-neg (mean±SD: 57.12±13.96 years) patients (U = –933.5 p = 0.45). Moreover, whether D+ patients had ongoing, past or no pharmacological treatment for depression was not associated with amyloid PET results (χ2 (2) = 2.25 p = 0.32).
Depression, amyloid-β, and clinical diagnosis
All Aβ-pos patients (n = 151) received a clinical diagnosis of AD or mild cognitive impairment due to AD in line with the NIA-AA criteria [22, 23]. Aβ-neg patients (n = 149), instead, formed a more heterogenous group, with 50.3% of patients diagnosed with stable non-neurodegenerative conditions, 30.9% with progressive other-neurodegenerative conditions, and 18.8% with indeterminate diagnoses. Further details on the diagnostic categories can be found in Table 1. Aβ-neg patients with a history of depression were not more likely to be diagnosed with non-neurodegenerative (54.7%) than with other-neurodegenerative (41.3%) conditions (χ2 (1) = 2.04 p = 0.15) (Table 1), and this held true when limiting the analysis to the ‘D+ ongoing’ group (χ2 (1) = 2.85 p = 0.09).
DISCUSSION
In this study we aimed to determine the prevalence of previous and ongoing depressive symptoms in a single-center memory clinic cohort of patients who had undergone diagnostic biomarker investigation for AD. Retrospective review of clinical correspondence showed that just under half (47%) of the 300 patients referred for amyloid PET scanning in our Centre between 2014 and 2021 had suffered from clinically significant depressive symptoms; most of these had ongoing symptoms at the time of the first visit to our Clinic (89%), and a considerable proportion of them were receiving pharmacological treatment for depression (62%).
Other studies have previously shown a higher occurrence of depressive symptoms in clinical cohorts with cognitive impairment than in the general population [2]. For example, in a large UK study on community dwelling older adults, 19% had consulted a doctor regarding depressive symptoms at least once in their life and 8.7% had ongoing clinical depression [24]. Although direct comparison is made difficult by methodological differences, the prevalence found in our study was considerably higher than that seen in other memory clinic cohorts. A previous study on a heterogeneous group of young-onset dementia (YOD) patients reported that 17.6% had a history of previous depressive episodes and 19.9% had been on antidepressants [25]. In another study, where assessment of depressive symptoms was based on patient’s account and clinical notes, 38.6% of 88 YOD patients had a history of depression [11]. In a general memory clinic population, instead, history of depression and antidepressant use were respectively 19.7% and 15.7% [15]; however, the method used to evaluate depression history was not described in this study.
Our other key finding was that history of depressive symptoms was equally highly prevalent in patients with and without AD pathology. A total of 43.7% amyloid-positive and 51.01% amyloid-negative patients had a history of depressive symptoms. To the best of our knowledge, this is the first study to assess history of depressive symptoms in a ‘real-world’ memory clinic cohort with persistent diagnostic uncertainty and consequent biomarker evaluation.
Within the heterogenous group of amyloid-negative patients, history of depression was not more strongly associated with a stable or progressive underlying condition. Of the amyloid-negative patients, 50.3% were diagnosed with a stable non-neurodegenerative condition, a subset of which would have been likely to have functional etiology [26, 27]. In the stable amyloid-negative group, depressive symptoms may be associated with increased awareness of cognitive failures, consequently leading to seek medical consultation. Studies on subjective cognitive impairment have shown that patients with a history of medical help-seeking behavior had lower amyloid and higher depressive symptoms [28], and that feelings of worse cognitive performance were not predicted by amyloid positivity in younger individuals [29]. Although patients undergoing amyloid PET in our Clinic do have some degree of objective impairment by definition [16], a similar mechanism to that seen in subjective cognitive impairment may apply to the stable amyloid-negative group.
On the other hand, the high occurrence of depressive symptoms in both the amyloid-positive and the progressive amyloid-negative groups in later life suggests that affective symptoms are frequently part of the prodromal phase of neurodegenerative diseases. Another possibility is that depressive symptoms may lead to earlier onset of cognitive decline in these patients by depleting cognitive reserve [30]. Further studies are needed to disentangle the nature of the links between neurodegeneration, depression, and amyloid in this clinical population.
The results of this work have important clinical implications. Firstly, as concomitant depression has been associated with worse prognosis of AD [31], regular active screening for depression in this setting may identify an additional therapeutic target [32]. Secondly, at the diagnostic level, depression may be one of the key reasons behind diagnostic uncertainty leading to biomarker testing. Our findings highlighted that depression was not more strongly associated with a positive or a negative scan result in this group, further corroborating the importance of biomarker assessment for the differential diagnosis [9, 33]. This is illustrated by two example cases in Figs. 3 4.
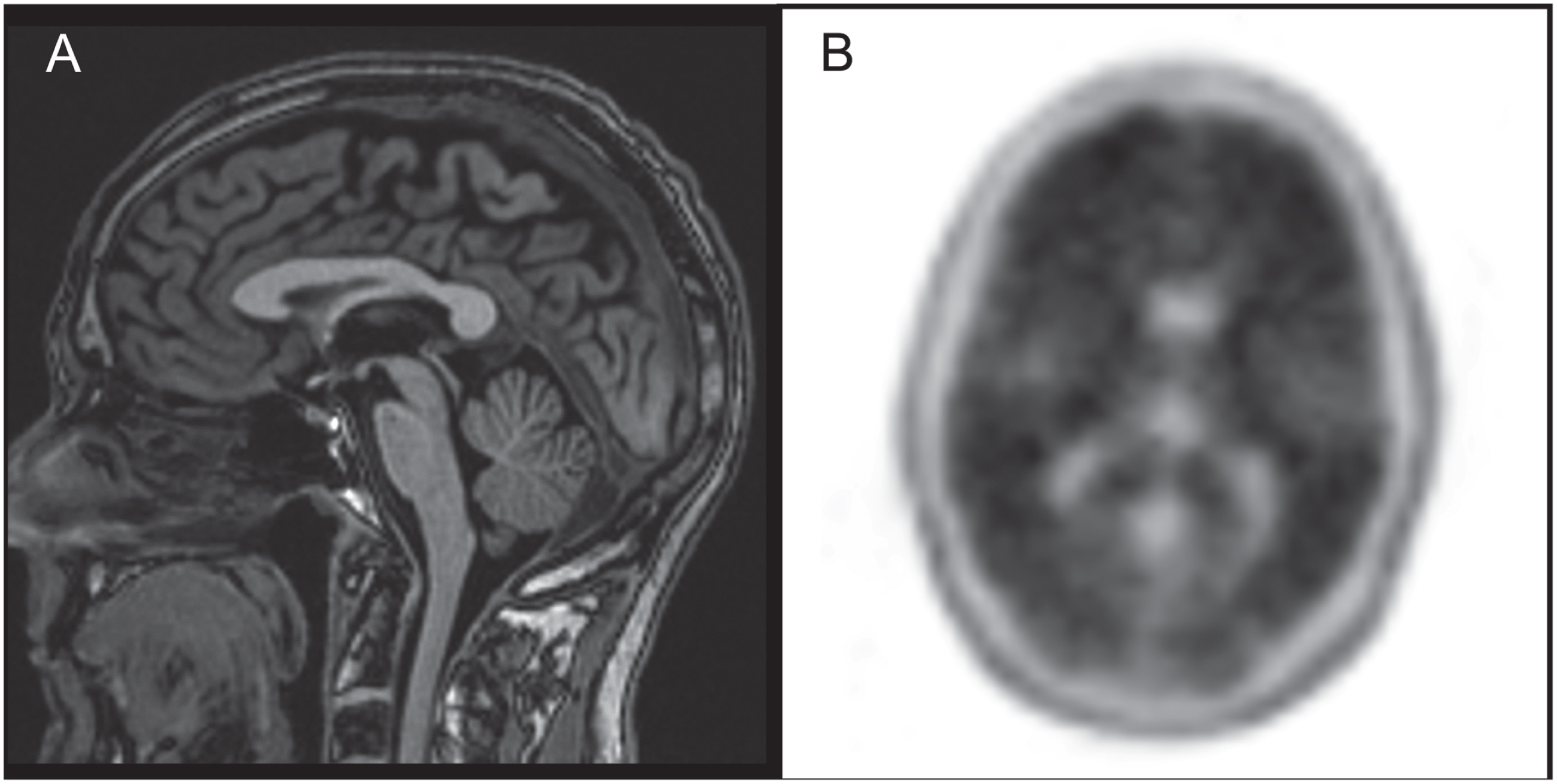
A man in his 50s presented with a 3-year history of memory problems and depressive symptoms. MRI scan (A) was reported to show mild hippocampal atrophy and previous cerebrospinal fluid revealed normal tau and slightly low Aβ (ratio: 0.96). Depression was indicated as the most likely cause of impairment and API was requested to rule out AD. API was strongly positive (B), indicating underlying AD. Patient was prescribed cholinesterase inhibitors and referred to the clinical trials unit. (Images courtesy of Dr. Zarni Win and Dr. Anastassia Gontsarova).
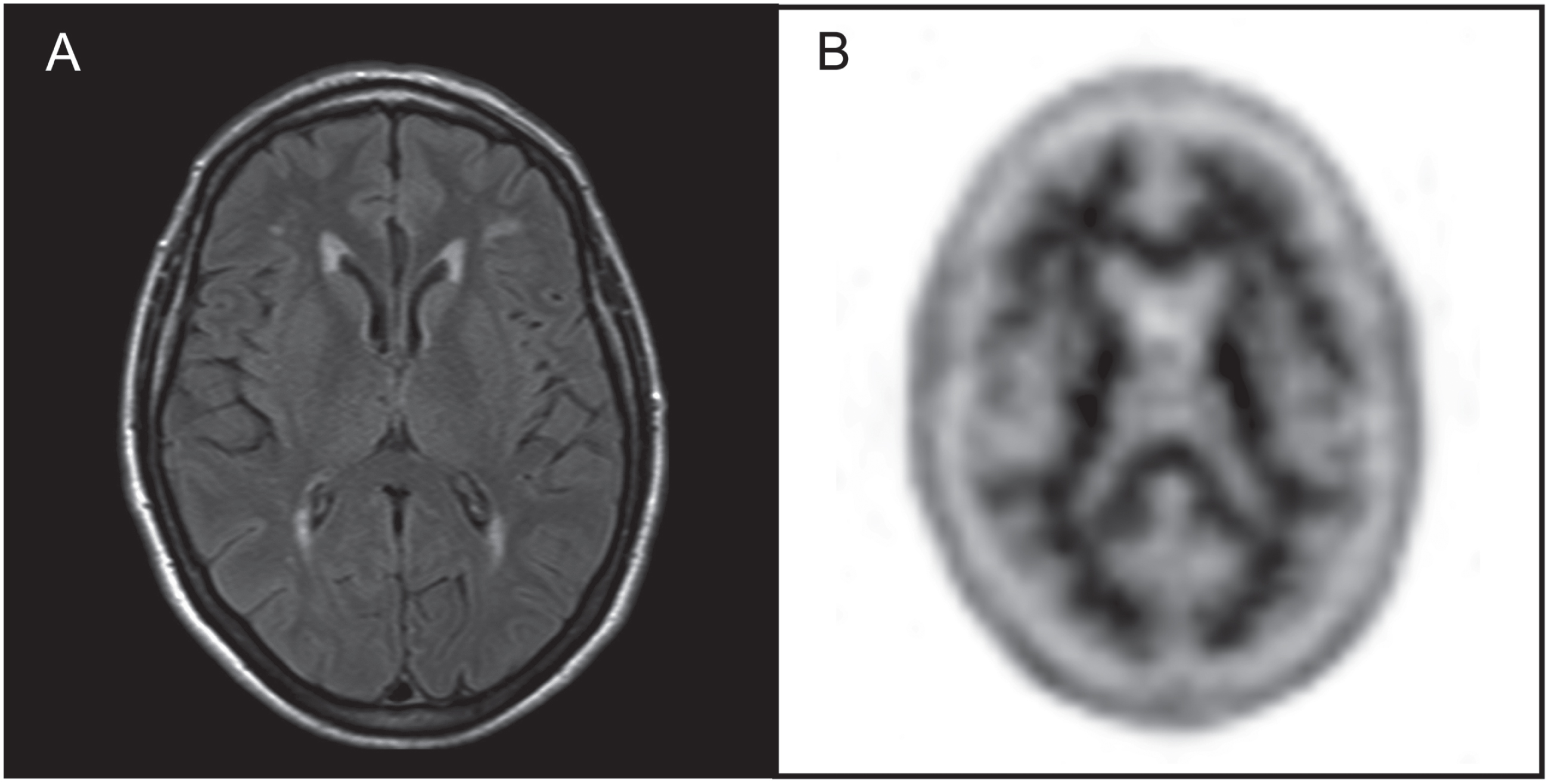
A lady in her late 60s presented with a 4-year history of episodic memory difficulties, with episodes of spatial disorientation and reduction in her activities of daily living. She also had a 11-year history of depression treated with Mirtazapine. Cognitive screening highlighted cognitive under functioning (Mini-Mental State Examination score: 24) and the MRI was reported as showing static confluent white matter changes (A). API was requested to investigate the possibility of underlying AD pathology. API was clearly negative (B), excluding a diagnosis of AD. Patient was referred for psychological input to treat ongoing depressive symptoms. (Images courtesy of Dr. Zarni Win and Dr. Anastassia Gontsarova).
Our study presents some limitations. As depressive symptoms were evaluated retrospectively, a history of depression may not have always been recorded in the clinical correspondence. Similarly, symptoms may have been more likely to be reported if ongoing at the time of evaluation. However, these scenarios would in fact underestimate depression prevalence. Furthermore, we could not categorize patients according to the types of depressive disorder. Future studies should evaluate whether specific subtypes of depression are particularly associated with AD pathology. Finally, self-reported depression scores were not available for review; however, these usually do not assess lifetime history of depressive symptoms and their one-off administration in the clinical setting could capture an emotional reaction to the diagnostic workup itself. Nevertheless, the regular administration of affective questionnaires across memory clinic visits should be considered to assess the longitudinal trajectories of depressive symptoms and their association with patterns of cognitive functioning.
Conclusions
This is the first study to evaluate depressive symptomatology in patients routinely referred for clinical amyloid PET. Our findings provide robust evidence for a high prevalence of depression in both amyloid-positive and amyloid-negative patients meeting appropriate use criteria for biomarker assessment, highlighting the importance of gaining a greater understanding into the clinical features of this group and their role at the diagnostic stage.