
Abstract
Background:
Several studies have examined association between vitamin D levels in serum and cognition, but little is known of vitamin D levels in cerebrospinal fluid (CSF) and association with Alzheimer’s disease (AD).
Objective:
In this cross-sectional, explorative study we investigated possible associations of vitamin D in CSF with biomarkers for AD, amyloid-β, tau protein/phosphorylated tau protein in CSF, and with the cytokines IL-6, IL-8, and TNF-α in CSF in patients with cognitive impairment and cognitively healthy controls.
Methods:
We included 100 outpatients ≥65 years referred for assessment of cognitive impairment and 76 age- and sex-matched cognitively healthy controls. Levels of 25-hydroxyvitamin D (25(OH)D), amyloid-β, tau protein and phosphorylated tau protein, as well as IL-6, IL-8, and TNF-α, were analyzed in CSF in both groups.
Results:
Higher levels of 25(OH)D in CSF in all groups together were associated with lower levels of tau protein (p = 0.01) and phosphorylated tau protein (p = 0.005). We found no association between 25(OH)D levels in CSF and pathological levels of amyloid-β in CSF nor levels of IL-6 or TNF-α in CSF. Higher levels of 25(OH)D in CSF were associated with higher levels of IL-8 in CSF (p = 0.002). However, vitamin D explained only 6% of variance in IL-8. There was no significant difference between the patient groups and the control group regarding the association between 25(OH)D in CSF and any of the three cytokines in CSF.
Conclusion:
Participants with higher CSF levels of 25(OH)D exhibited reduced CSF levels of tau protein and phosphorylated tau protein.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is a multifactorial neurologic disorder caused by progressive damage of neurons. The neuropathological hallmarks of the disease are an extracellular accumulation of amyloid-β and neuritic plaques and the formation of neurofibrillary tangles (NFT) caused by abnormal phosphorylation of tau proteins [1]. The diagnosis of AD dementia is based on clinical criteria [2]. Cerebrospinal fluid (CSF) analysis is not necessary for the diagnosis of AD dementia, but might be supportive, showing pathologically decreased levels of amyloid-β and increased levels of tau protein and tau phosphorylated at threonine 181 (hereafter called phosphorylated tau protein) [3].
Polymerization of amyloid-β proteins has been considered the main risk factor for initiation and progression of AD, described as the amyloid cascade hypothesis [4]. Therefore, vast research efforts in the last decades have focused on therapies for amyloid reduction, so far without clinical success [5]. Alternative hypotheses suggest that the accumulation of amyloid-β plaques could merely be a response to other harmful neuronal stimuli and not the cause of the disease [5], but this is yet to be confirmed.
Research on anti-tau therapies has increased considerably. Tau pathology, compared to accumulation of amyloid-β plaques, is shown to have a better correlation with cognitive deficits in AD patients [6]. Pathological tau levels are associated with higher severity and longer duration of AD [7]. However, studies focusing on tau-targeting therapies have so far not shown positive results [8], but the attempts continue, especially in the field of immunotherapy [4].
Adaptive immune systems have been suggested to be preventive of the pathogenesis of AD via modulation of microglial activity [9] and neuroinflammation is thus an important potential target for clinical AD studies [10]. Pro-inflammatory cytokines have been suggested to increase the accumulation of amyloid-β in the brain [11]. Over-activated microglia in AD are also shown to increase pro-inflammatory cytokines, the most studied being interleukin-1 (IL-1), IL-6, and tumor necrosis factor alpha (TNF-α) [12]. IL-8, a member of the CXC chemokine family, is another pro-inflammatory cytokine that acts as a signaling factor for recruitment of neutrophils to sites of damage and across the blood-brain barrier [13]. The chemotactic response is associated with brain inflammation, but could also exert neuroprotective effects [14].
As AD is a multifactorial neurodegenerative disease, vitamin D might be an important agent to consider in the search of modifiable risk factors for disease development. The effect of vitamin D on the central nervous system (CNS) has been studied extensively in recent decades, as it has been suggested that vitamin D might have neuroprotective properties [15]. Observational studies have shown associations between serum vitamin D deficiency and all-cause dementia and AD [16], although results have been heterogeneous [17]. There are several theories on how vitamin D might exert positive effects on cognition. One is that vitamin D facilitates clearance of amyloid-β and stimulation of amyloid-β phagocytosis, as shown in animal studies [18]. Another theory is that vitamin D reduces tau phosphorylation, an effect also shown in animal studies [19]. As elevated levels of cytokines contribute to the immune response and thus exacerbate AD pathology [20], an anti-inflammatory effect of vitamin D has been suggested as a modulatory factor via this pathway [21]. To the best of our knowledge, there have so far been no human studies exploring vitamin D in human brain in association with AD biomarkers and inflammatory cytokines.
The study aim
We recently found evidence that participants with positive AD core biomarkers have low CSF levels of 25(OH)D, despite normal serum levels [22], which supports the theories of the local effect of vitamin D in the brain. Gezen-Ak et al. have presented a hypothesis that amyloid-β might disrupt the function of vitamin D in the brain, even if the systemic level of vitamin D is sufficient, suggesting the term “inefficient utilization of vitamin D” [23].
In this study, we aimed to further explore the relationship between intrathecal vitamin D and amyloid-β, tau protein and phosphorylated tau protein, as well as three cytokines in CSF.
MATERIALS AND METHODS
Study participants
Participants 65 years and older were included in the study. All participants were screened with cognitive tests and underwent a lumbar puncture. For the patient group, 100 patients were included from the Norwegian registry for patients assessed for cognitive symptoms (NorCog) [24] between 2011 and 2020. The registry includes patients with subjective cognitive impairment (SCI), mild cognitive impairment (MCI), and dementia.
Dementia was diagnosed according to the ICD-10 criteria. Clinical AD MCI or AD dementia were diagnosed according to National Institute on Aging (NIA) at National Institutes of Health (NIH) and the Alzheimer’s Association published revised guidelines [2, 25]. MCI was diagnosed according to the Winblad criteria for MCI [26].
The patient group was divided into two subcategories: patients without clinical AD symptomatology (MCI and dementia, primarily vascular etiology and other types) (31%), hereafter called the non-AD group, and patients with clinical AD (MCI and dementia) symptomatology (68%), hereafter called the AD group. One patient with SCI was excluded from sub-analyses.
For the control group, 76 cognitively healthy participants were recruited among orthopedic patients planned for elective hip or knee joint replacement surgery under spinal anesthesia at Lovisenberg Diaconal Hospital. They had no subjective cognitive symptoms and were included if MMSE-NR3 ≥27/30, Clock Drawing Test ≥3/5 points and Trail Making Test A and B was better than two standard deviations below the expected score adjusted for age and education. Controls were included between 2018 and 2020.
Ethical considerations
The study was approved by The Regional Committee for Medical and Health Research Ethics (reference 2016/888/REK Sør-øst C). Participants in the patient group gave informed written consent for inclusion in NorCog. Participants in the control group gave informed written consent for their participation.
Biochemical procedures
Blood and CSF samples were collected within a maximum interval of three days in individual patients and controls and all samples were transferred to storage tubes immediately after centrifugation and stored at –80°C until analysis.
CSF levels of amyloid-β, tau protein, and phosphorylated tau protein were analyzed consecutively for patients and simultaneously for controls at the Department of Interdisciplinary Laboratory Medicine and Medical Biochemistry, Akershus University Hospital. The analysis method and recommended cut-off values for amyloid-β changed several times during the inclusion period of the present study. Until October 2020, the samples for amyloid-β were analyzed by enzyme-linked immunosorbent assays using the Innotest kit (Innogenetics, Ghent, Belgium). After October 2020, ElectroChemiLuminescense ImmunoAssay (ECLIA) from Cobas e 602 (Roche Diagnostics) was utilized. In 2021, the cut-off values were changed again due to the transition to Sarstedt tubes (referent values > 1100 ng/L) [27]. For tau protein and phosphorylated tau protein, the cut-off values were changed once during the inclusion period, in 2021, after transition to Sarstedt tubes. The reference values for tau protein were changed from < 500 to < 300 ng/L and for phosphorylated tau from < 80 to < 27 ng/L.
The results of the analysis were therefore dichotomized into pathological and non-pathological. As for tau protein and phosphorylated tau protein, the same principle of dichotomization into pathological and non-pathological was applied, but we also analyzed them as continuous variables controlling for the changes in the method (see Statistics section for details).
Four cytokines, IL-6, TNF-α, Interferon gamma (IFN-γ), and IL-8, in CSF were analyzed at Vitas AS laboratory in Oslo, using the Multiplex Human Cytokine (4-Plex), a quantitative ELISA-based chemiluminescent assay.
IFN-γ levels were not detectable in CSF. TNF-α values were under the lower limit of detection in 31 participants (18%). IL-6 and IL-8 were detectable in all participants.
25(OH)D levels in both serum and CSF were analyzed by liquid chromatography double mass spectrometry (LC-MS/MS). For CSF analysis, ultraperformance liquid chromatography-tandem mass spectrometry (UPLC-MS/MS) was applied. Of the 176 measured values for 25(OH)D in CSF, 17 were under the lower limit of detection. Serum analysis was performed at Oslo University Hospital, and CSF was analyzed at Vitas AS laboratory.
Covariates
The following potential confounders were chosen: age, gender, season of blood collection (unless the vitamin D was taken at the same time as other serum and CSF samples or cognitive tests), education (years), smoking (non-smoker, previous smoker, current smoker), alcohol consumption (non-drinker, occasional drinker [≤3 drinks/week], moderate to heavy drinker [> 4 drinks/week or previous alcohol abuse]), vascular risk factors (heart disease, cerebrovascular disease, hypertension or diabetes mellitus).
Statistics
Characteristics of patients and controls were presented as means, minimum and maximum values, and standard deviations (SDs) or frequencies and percentages and compared by independent samples t-test or χ2-test, as appropriate. Associations between vitamin D in CSF and biomarkers, cytokines and diagnosis were assessed by tobit regression models. For CSF to serum 25(OH)D ratio, linear regression models were used. Furthermore, the associations between cytokines and vitamin D in CSF and between cytokines and diagnosis were assessed by linear regression models. To assess the differences between the diagnostic groups with respect to association between vitamin D in CSF and cytokines, interaction between diagnosis and cytokines was included. A significant interaction would imply that the differences between the groups regarding the association between vitamin D and cytokines are significant. All models were adjusted for pre-chosen confounders. The models with tau protein and phosphorylated tau protein as continuous covariates were in addition adjusted for (factor accounting for) the change in method. All tests were two-sided and the results with p-values below 0.05 were considered statistically significant. The analyses were performed using SPSS v27 and Stata v16 statistical software.
RESULTS
Mean age in both the patient group and the control group was 71 (SD 5) years. As shown in Table 1, mean serum 25(OH)D level in serum was 75 nmol/l (SD 32) in the patient group and 83 nmol/l (SD 24) in the control group. There was no statistical difference between the mean serum levels of 25(OH)D in the patient and control groups. We did not have complete data on vitamin D supplementation in the patient group. Out of 36 participants in the patient group that had available data, 19 % used vitamin D supplementation. In the control group, 13 % used vitamin D supplements.
Descriptive characteristics of the patient and control groups
1 χ2-test; 2independent samples t-test. SCI, subjective cognitive impairment; MCI, mild cognitive impairment; AD, Alzheimer’s disease; CSF, cerebrospinal fluid; LLOD, the lower limit of detection.
As shown in our previous article [22], vitamin D levels in CSF were significantly lower in patients in the AD group compared to patients in the non-AD group or to the control group, despite normal 25(OH)D serum levels in all groups. Most of the participants in the present material were considered to be vitamin D sufficient, defined as 25(OH)D > 50 nmol/l.
One participant in the control group had a short post-operative delirium, likely due to use of opioids. No other participants in the control group experienced delirium after hip or knee replacement operation.
Core biomarkers for AD and vitamin D
As the diagnosis of AD was made on clinical criteria, not all patients with final AD diagnosis had pathological levels of core biomarkers for AD (amyloid-β, tau protein, and phosphorylated tau protein) [28]. As shown in Supplementary Table 1, all three biomarkers were pathological in 65% of patients with AD dementia and AD-MCI, and in 3% of patients with non-AD dementia and MCI. Pathological core biomarkers of AD were also found in the control group, as presented in Table 1. One person in the control group had pathological levels of all three core biomarkers for AD. This is in accordance to previous reports in healthy elderly [29].
As demonstrated in Table 2, there was no significant difference between participants with pathological levels of amyloid-β in CSF and participants with non-pathological levels of amyloid-β in CSF regarding 25(OH)D levels in CSF or CSF/Serum 25(OH)D ratio.
Associations between biomarkers for AD and vitamin D in CSF (N = 176)
*Models are adjusted for age, sex, education (in years), alcohol consumption, smoking habits and vascular risk factors. **Results of tobit regression analysis. ***Results of linear regression analysis. RC, regression coefficient.
Lower levels of vitamin D (both 25(OH)D in CSF and CSF/Serum 25(OH)D ratio) were associated with pathological levels of tau protein (p = 0.008 and p = 0.02, respectively) and phosphorylated tau protein (p = 0.02 and p = 0.02, respectively).
As shown in Table 3, the associations were still significant in models with continuous tau protein and phosphorylated tau protein. Increasing levels of 25(OH)D in CSF were significantly associated with lower levels of tau protein (p = 0.01) and phosphorylated tau protein (p = 0.005) in adjusted models. The unadjusted associations are illustrated in Fig. 1.
Associations between tau protein/phosphorylated tau protein and vitamin D in CSF** (N = 173)
*Models are adjusted for age, sex, education (in years), alcohol consumption, smoking habits, vascular risk factors and method used for tau-protein analysis. **Results of tobit regression analysis.
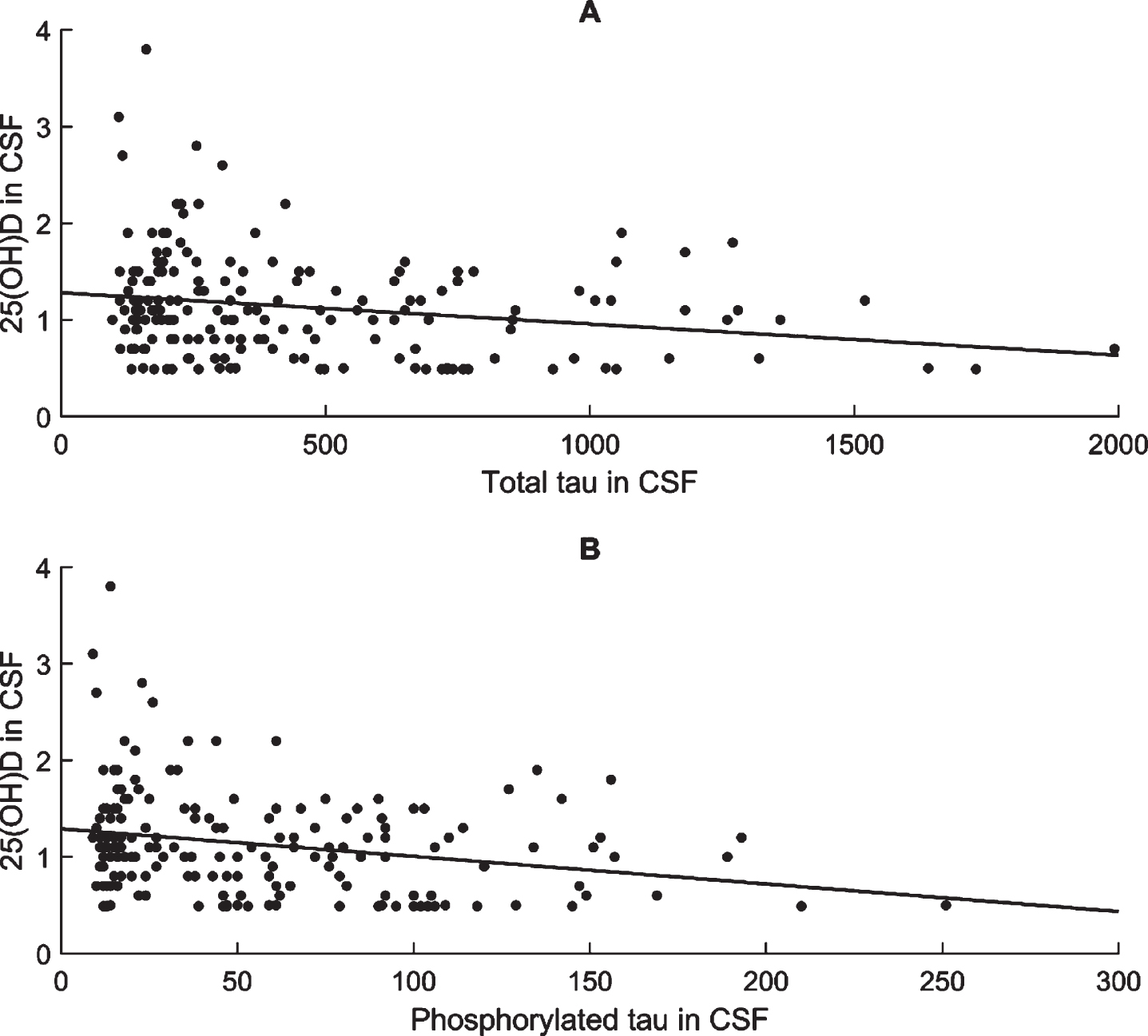
Associations between 25(OH)D in CSF and total tau and phosphorylated tau levels in CSF. 25(OH)D in nmol/L and Total tau and Phosphorylated tau in ng/L.
Cytokines and vitamin D, and cytokines and core biomarkers for AD and diagnostic groups
Descriptive statistics for IL-6, IL-8, and TNF-α and their associations with vitamin D levels in CSF are shown in Table 4. Higher levels of 25(OH)D and higher values of CSF/Serum 25(OH)D ratio were associated with higher levels of IL-8 in CSF (p = 0.002 and p = 0.001, respectively). However, as evident in the scatterplot in Fig. 2, which illustrates the unadjusted association between vitamin D in CSF and IL-8, vitamin D explains little of the variation in IL-8 (about 6 %). In the adjusted model, there were no significant associations between levels of IL-6 or TNF-α and 25(OH)D levels in CSF.
Associations between cytokines in CSF and vitamin D in CSF as well as cytokines in CSF and pathological levels of amyloid-β, tau protein and phosphorylated tau protein in CSF (N = 176)
*Models are adjusted for age, sex, education (in years), alcohol consumption, smoking habits, and vascular risk factors. **Results of tobit regression analysis. ***Results of linear regression analysis.

Association between 25(OH)D in CSF and IL-8 levels in CSF. 25(OH)D in nmol/L and IL-8 in pg/mL.
Mean values of each cytokine by disease subgroup are presented in Supplementary Table 2. Column graphs with individual values for 25(OH)D in CSF by subgroups and scatterplot showing relation between 25(OH)D and IL-8 in CSF are presented in Supplementary Figure 1. Supplementary Figure 2 presents column graphs with individual values for CSF amyloid-β, tau, and phosphorylated tau protein by subgroups and correlation graph for CSF 25(OH)D and amyloid-β, tau, and phosphorylated tau protein.
Pathological levels of amyloid-β, tau protein, and phosphorylated tau protein in CSF were significantly associated with higher levels of TNF-α in CSF in adjusted models (p = 0.005, p = 0.04, and p = 0.05, respectively).
As shown in Table 5, there was no significant difference between the patient groups and the control group regarding the association between 25(OH)D in CSF and any of the three cytokine levels in CSF.
Association between cytokines in CSF and vitamin D in CSF with diagnosis as a main covariate, N = 173
*Models are adjusted for age, sex, education (in years), alcohol consumption, smoking habits, and vascular risk factors. **Results of tobit regression analysis.
In Table 6, we present the linear regression model assessing the association between the three cytokines and the three diagnostic groups. Patients in the AD group had significantly higher levels of TNF-α (p = 0.01) compared to the control group.
Associations between diagnosis and cytokines in CSF (N = 176)
*Models are adjusted for age, sex, education (in years), alcohol consumption, smoking habits, and vascular risk factors. **Results of tobit regression analysis.
DISCUSSION
The present study assessed associations between CSF levels of 25(OH)D and selected cytokines and core CSF biomarkers for AD in patients with cognitive impairment and a cognitively healthy control group. Our results show that higher levels of vitamin D in CSF are associated with lower levels of both total tau and phosphorylated tau protein in CSF. Further, the results show that higher levels of vitamin D in CSF are associated with higher levels of IL-8 in CSF, but vitamin D does not seem to explain much of the variation in IL-8.
Core biomarkers for AD and vitamin D
To the best of our knowledge, we are the first group to examine associations between CSF 25(OH)D and core CSF biomarkers for AD. We did not find any association between levels of 25(OH)D in CSF and pathologic CSF levels of amyloid-β in the present study.
Animal studies have shown that vitamin D might increase amyloid-β phagocytosis and decrease amyloid-β formation [30–32]. However, human studies have found conflicting results [33]. One study did not find any association between serum levels of 25(OH)D and cerebral amyloid-β in older adults [34], while other studies found a significant association between 25(OH)D levels in serum and lesser amyloid burden in CSF [35, 36].
Fan et al. proposed that optimal vitamin D levels may reduce oxidative stress, synaptic degeneration and neuronal loss that reduces tau phosphorylation, and thus results in better cognitive performance [37]. Several research groups have suggested that vitamin D also influences tau hyperphosphorylation-related mechanisms in humans [23, 39], but the human data are limited.
Cytokines and vitamin D
We found no significant differences between the two patient groups and the control group regarding the association between the three cytokines examined and 25(OH)D in CSF.
IL-8, also called CXCL8, is a chemotactic factor produced by several cells that attracts, among others, T-cells and neutrophils in response to injury. It is also involved in intracellular calcium mobilization [40]. IL-8 is found to be increased in brain injury, suggesting intrathecal production [41]. Patients with AD have previously been found to have significantly lower CSF levels of IL-8 compared to controls [42]. The same association was found for IL-6 [43] and TNF-α [44]. Higher levels of 25(OH)D in CSF were associated with higher levels of IL-8. However, vitamin D explained only about 6% of the variance in IL-8. Because of this, we chose not to emphasize the findings, as we did not find any significant association between levels of 25(OH)D in CSF and levels of IL-6 and TNF-α. Further, we did not find any association between IL-8 or IL-6 levels and AD pathology in CSF (pathological levels of amyloid-β, tau protein and phosphorylated tau protein).
As expected, we did find that participants with AD symptomatology in CSF had significantly higher levels of TNF-α in CSF [45], but this did not seem to be mediated by lower levels of intrathecal vitamin D, according to our results.
Our results do not support the hypothesis that vitamin D reduces the levels of pro-inflammatory cytokines [46, 47] in human brain tissue, nor that it reduces the amyloid burden [18] in a population that is considered, for the most part, to be serum vitamin D sufficient. It is possible that the results would be different in populations with a higher prevalence of vitamin D deficiency. Vitamin D might contribute to lower tau phosphorylation and thus protect cognitive function from the harmful effect of hyperphosphorylation. The observed association between vitamin D and tau in this study warrants further investigation.
Study strengths and limitations
We examined a relatively large number of participants with CSF analysis of 25(OH)D, cytokines, and core biomarkers for AD in CSF and included a cognitively healthy control group. Further, we adjusted the models for several potential confounders. The application of the LC-MS/MS method, the only method validated for 25(OH)D analysis in CSF [48], is also considered a study strength.
The results of amyloid-β in CSF were dichotomized as normal or pathological due to several changes in the analytic methods, which might have limited the validity of the analysis. The data on body mass index were incomplete in our material and therefore we chose to exclude this variable from the analysis. We did not have the available data on all the factors that might influence vitamin D levels such as time spent outside, medication history, diet, and relevant comorbidities. Even though other potentially confounding variables identified in previous studies were adjusted for, residual confounding cannot be ruled out.
Conclusion
We have shown an association between increased levels of 25(OH)D in CSF and reduced levels of tau protein and phosphorylated tau protein in CSF. This should be further explored in clinical intervention studies, e.g., in population with AD MCI, to determine whether vitamin D supplementation— and what dose— can increase its intrathecal levels, reduce tau protein and phosphorylated tau protein and have a positive effect on cognition.
Footnotes
ACKNOWLEDGMENTS
This study was funded by Lovisenberg Diaconal Hospital. The authors would like to thank the anesthesiologists, orthopedic surgeons, and nurses at Lovisenberg Diaconal Hospital, as well as bioengineers at the Unger Vetlesens Institute for their help with data collection and excellent cooperation on this project. We would also like to thank the Norwegian registry of patients assessed for cognitive symptoms (NorCog) for providing access to patient and caregiver data and biological material.