
Abstract
Background:
Emerging evidence suggests that age-related changes in cerebral health may be sensitive to vascular risk modifiers, such as physical activity and sleep.
Objective:
We examine whether cardiorespiratory fitness modifies the association of obstructive sleep apnea (OSA) severity with MRI-assessed measures of cerebral structure and perfusion.
Methods:
Using data from a cross-sectional sample of participants (n = 129, 51% female, age range 49.6-85.3 years) in the Wisconsin Sleep Cohort study, we estimated linear models of MRI-assessed total and regional gray matter (GM) and white matter (WM) volumes, WM hyperintensity (WMH:ICV ratio), total lesion volume, and arterial spin labeling (ASL) cerebral blood flow (CBF), using an estimated measure of cardiorespiratory fitness (CRF) and OSA severity as predictors. Participants’ sleep was assessed using overnight in-laboratory polysomnography, and OSA severity was measured using the apnea-hypopnea index (AHI), or the mean number of recorded apnea and hypopnea events per hour of sleep. The mean±SD time difference between PSG data collection and MRI data collection was 1.7±1.5 years (range: [0, 4.9 years]).
Results:
OSA severity was associated with reduced total GM volume (β=-0.064; SE = 0.023; p = 0.007), greater total WM lesion volume (interaction p = 0.023), and greater WMHs (interaction p = 0.017) in less-fit subjects. Perfusion models revealed significant differences in the association of AHI and regional CBF between fitness groups (interaction ps < 0.05).
Conclusion:
This work provides new evidence for the protective role of cardiorespiratory fitness against the deleterious effects of OSA on brain aging in late-middle age to older adults.
Keywords
INTRODUCTION
Emerging evidence suggests that age-related changes in cerebral structure and perfusion— hallmark features of Alzheimer’s disease (AD) [1–4]— may be sensitive to vascular risk modifiers such as physical exercise and sleep [5–8].
Cardiorespiratory fitness, a measure of exercise-induced oxygen delivery and utilization [9], has been positively associated with brain structure and function [6, 10, 11], particularly in regions associated with age-related cognitive decline such as the hippocampus [11, 12].
In contrast, the incomplete modulation of cardiovascular and respiratory control during sleep, a defining feature of obstructive sleep apnea (OSA) [13], has been linked to gray matter (GM) and white matter (WM) atrophy from intermittent hypoxia-induced alterations in cerebral blood flow (CBF) [14].
This study examines whether cardiorespiratory fitness (CRF), indexed by a reported non-exercise cardiorespiratory fitness measure [11, 15], modifies the association of OSA severity with magnetic resonance imaging (MRI)-assessed measures of GM and WM integrity and arterial spin labeling (ASL) perfusion in a sample of cognitively normal late-middle age participants from the Wisconsin Sleep Cohort (WSC).
METHODS
Participants
This study features n = 129 participants from the WSC study, a longitudinal population-based study of OSA whose cohort includes cognitively healthy, late-middle-aged adults who were between the ages of 30 and 60 years at study entry [16].
Participants in the study were administered a survey of sleep habits, health, and demographics; 72% of subjects responded to this survey. From these respondents, a stratified random sample of 2,884 people (excluding pregnant persons and individuals with recent airway cancer, airway surgery, or decompensated cardiopulmonary disease) were selected and invited to participate in overnight in-laboratory polysomnography (PSG) studies that were repeated approximately every four years. Of those invited to participate, 1,543 WSC subjects gave successful PSG recordings; a subset of 134 individuals participated in neuroimaging protocols. Five of these participants were excluded due to CPAP use at the time of PSG recording; thus, n = 129 participants were the subject of this work.
MRI imaging and PSG assessments were not always collected at the same visit. If PSG data was not collected at the same visit at the MRI data, PSG data from the visit closest in time (and always prior) to the MRI visit was used as a proxy. Visits were limited to being at most 5 years apart. The mean±SD time difference between PSG data collection and MRI data collection was 1.7±1.5 years (range: [0, 4.9 years]). Physical activity responses were available for almost all participants. Four participants were missing questionnaire data concomitant with their time of MRI acquisition; for these participants, we used physical activity data obtained from a prior study visit.
All study procedures were approved by the University of Wisconsin-Madison Institutional Review Board, and each subject provided informed consent prior to participation.
The Apnea-Hypopnea Index and OSA Severity Assessment
OSA severity was measured in-laboratory by PSG. Eighteen-channel PSG was performed at the University of Wisconsin Clinical Research Unit in accordance with established protocols [17]. PSG included electroencephalography, electrooculography, and electromyography. Breathing events were measured by oxyhemoglobin saturation (pulse oximetry, Ohmeda Biox 3740, Englewood, CO), respiratory inductance plethysmography (Respitrace; Ambulatory Monitoring, Ardsley, NY), and nasal and oral airflow (ProTec thermocouples; Hendersonville, TN). PSG recordings were segmented into 30-s epochs and scored for sleep stage, apnea, and hypopnea events by trained technicians and reviewed using standard criteria [17]. Apnea events were defined by the cessation of both nasal and oral airflow for at least 10 s. Hypopnea events were defined as a discernible reduction in breathing concomitant with a reduction in oxyhemoglobin saturation of 4% or greater [18, 19]. OSA severity was measured using the base 10 logarithm of the apnea-hypopnea index (AHI), or ‘log10(AHI+1)’ where the AHI was defined as the mean number of recorded apnea and hypopnea events per hour of sleep. In accordance with prior works [20], AHI was categorized according to established thresholds of OSA severity: minimal OSA (AHI < 5), mild OSA (AHI: 5–14.9), and moderate/severe OSA (AHI≥15).
Non-exercise cardiorespiratory fitness (CRF)
The CRF measure used in this study is based on the expression reported in a seminal study by Jurca et al., where their non-exercise estimate of cardiorespiratory fitness was found to be highly correlated with maximal oxygen consumption measured during graded exercise testing (0.76≤r≤0.81) within three large, independent cohorts [15]:
where sex was a binary index (male = 1, female = 0), body mass index (BMI) was calculated by laboratory-assessed weight in kilograms divided by height in meters squared, and resting heart rate was measured at the PSG measurement from the ECG channel during a five-minute, pre-sleep quiet resting phase for PSG calibration. The ‘Physically Active’ index was characterized as adequate (≥150 min/week=1) or inadequate (<150 min/week=0) weekly physical activity as assessed by a modified version of the Paffenbarger Physical Activity Questionnaire [36] which quantified participants’ usual frequency, intensity, duration, and type of regular and recreational physical activity. As such, the summative CRF index is a unitless estimate representative of standard metabolic equivalents (METs). In the present sample, male subjects had a median CRF of 8.0, while the median CRF for female participants was 4.5. All reported statistical analyses were stratified by these sex-specific CRF levels.
MRI assessment
MRI assessment was performed using a General Electric 3.0 Tesla Discovery MR750 (Waukesha, WI) system with an eight-channel head coil and parallel imaging (ASSET). A T1-weighted volume was acquired in the axial plane with a 3D fast spoiled gradient-echo (FSPGR) sequence using the following parameters: TI = 450 ms; TR = 8.1 ms; TE = 3.2 ms; flip angle = 12°; acquisition matrix = 256×256×156 mm, FOV = 260 mm; and slice thickness = 1.0 mm. In addition, a T2-weighted fluid attenuated inversion recovery (FLAIR) sequence was acquired in the sagittal plane using the following parameters: TI = 1868 ms; TR = 6000 ms; TE = 123 ms; flip angle = 90°; acquisition matrix = 256×256×100 mm, FOV = 256 mm; slice thickness = 2.0 mm, which yielded a voxel resolution of 1 mm×1 mm×2 mm.
FreeSurfer image analysis suite version 5.1.0 (http://surfer.nmr.mgh.harvard.edu/) was used to derive WM and GM volumes from T1 images, as described in prior works [21]. The open-source Lesion Segmentation Tool (LST) version 1.2.3 was used to calculate the total volume of WM lesions [22]; in this toolbox, LST seeds lesions based on spatial and intensity probabilities from T1 images and hyperintense outliers on T2 FLAIR images. ICV was calculated using the reverse brain masking method [23], and WM hyperintensity was obtained by dividing WM lesion volume by ICV to obtain a ratio of lesion-to-cranial volume (WMH:ICV) [24].
Finally, resting CBF assessments were made using a background-suppressed pseudo-continuous ASL (pcASL) [25] protocol, featuring a 3D fast spin echo spiral sequence that utilizes a stack of variable-density spiral four ms-readout and eight interleaves. Scan parameters were TR = 6000 ms; TE = 21 ms; FOV = 240×240×160 mm; slice thickness = 4 mm no gap; matrix size = 128×128; NEX = 3; and labeling RF amplitude = 0.24 mG. Multi-slice spin labeling was implemented using a single coil that eliminates off-resonance errors [26]. The pcASL scan involved three acquisitions, each consisting of a control image subtracted from a labeled image. The protocol also included a fluid-suppressed proton density (PD) acquisition with the same imaging sequence and image slab location as pcASL, but without RF labeling preparation for CBF flow quantitation and image registration. To reduce CBF assessment variability, participants fasted for a minimum of four hours prior to their scan from food, tobacco, caffeine, and medications with vasomodulatory properties. There was an error with the ASL scan equipment/calibration that resulted in unusable data for 27 participants.
Statistical analyses
To test whether CRF modified the association between OSA severity and MRI-measured cerebrovascular health outcomes, we estimated multiple linear regression models under the single-moderation framework depicted in Fig. 1.

Moderation analysis framework for the present study.
Results from these models were first assessed for between-group differences in MRI outcomes across the sex-specific median split for CRF, thus testing the effect of OSA severity within the ‘more fit’ versus ‘less fit’ strata. Post hoc conditional effects analyses were likewise performed for each outcome to test for significant interaction effects between OSA severity and CRF in predicting neuroimaging outcomes. Sensitivity analyses were also performed using alternative cut points to define ‘more fit’ and ‘less fit’ groups, but there were no meaningful changes in findings from prior median-split models. As such, we only present findings from analyses that featured sex-specific median cut points for estimated CRF.
RESULTS
Background characteristics
The n = 129 participants in this study had a mean (SD) age of 67.5 (7.9) years old; 51% were female, and 96% white. Mean (SD) AHI was 16.5 (13.7) events/hour, and n = 26 (20%) had minimal OSA (AHI < 5), n = 48 (37%) had mild OSA (AHI: 5–14.9), and n = 55 (43%) had moderate to severe OSA (AHI≥15). The mean (SD), [range] CRF level was 6.3 (2.3), [0–10.7]. Table 1 details additional demographic characteristics of study participants grouped by median CRF.
Demographic characteristics of participants
†This study included one Asian, two Black, and two Hispanic/Latinx participants.
MRI volumetrics
As shown in Table 2, among less fit individuals, a tenfold increase in AHI was associated with a significantly lower total GM volume (p = 0.007); there was a similar, but non-significant, association within the more fit group (p = 0.11). Regional GM models found no significant between-group differences in the hippocampus or amygdala.
Results from MRI volumetrics models stratified by median CRF. Beta-coefficients represent estimated increments (positive coefficients) or decrements (negative coefficients) in volumes associated with a 10-fold increase in the AHI (e.g., 30 versus 3 events/h)
Predictor: OSA severity (tenfold increase in AHI, ‘log 10 (AHI + 1) ’; no CPAP use). Moderator: median CRF (‘less fit’ versus ‘more fit’). Covariates: age, sex, BMI, education (‘some college’), hypertensive (BP > 140/90 or medication use). Significance: **p < 0.01, *p < 0.05.
Likewise, there were no significant differences in total WM volume, WMHs, or total lesion volume between CRF groups.
As an additional post hoc analysis of CRF’s modifying influence on the association between OSA severity and MRI volumetrics, conditional effects analyses were performed [37]. Figure 2 shows the results from this assessment, illustrating significant crossover interaction effects with their respective p-values— OSA severity was more strongly associated with both total lesion and WMH loads in less fit compared to more fit persons (interaction p = 0.023 and p = 0.017, respectively).

Conditional effects models stratified by median CRF illustrating the relationship between OSA and: i) total WM lesion volume, and ii) WMH:ICV ratio.
ASL perfusion
While there were no significant effects of OSA on CBF within either more fit or less fit subgroups, conditional effects analyses revealed significant crossover interaction effects. As shown in Fig. 3, these analyses revealed significantly different associations between OSA and regional CBF by fitness status for the following regions: angular gyrus, middle frontal cortex, and superior frontal gyrus, as well as paradoxically lower CBF in the anterior cingulate gyrus and hippocampus in more fit individuals (interaction ps < 0.05).
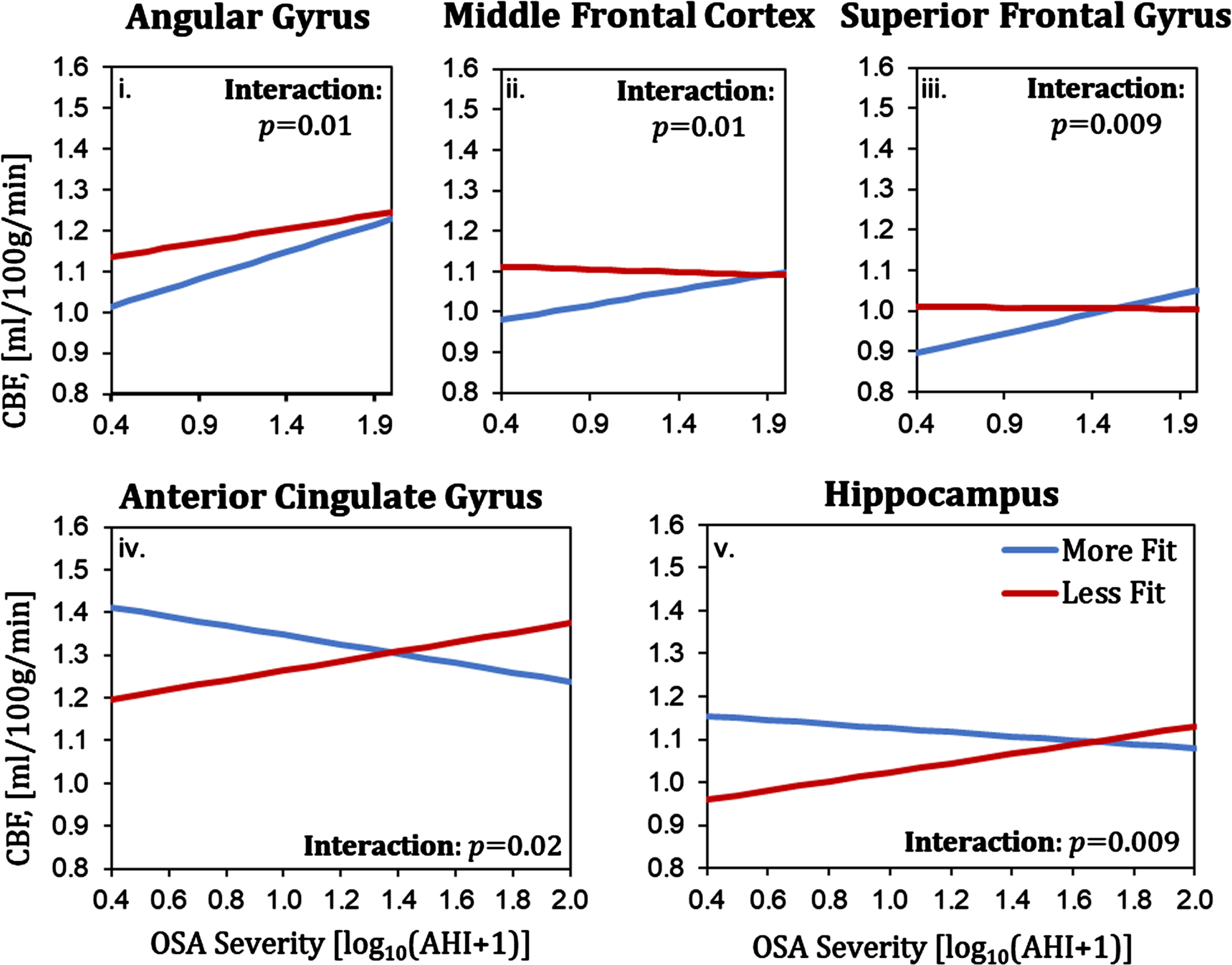
ASL perfusion results: associations between OSA and regional CBF by fitness level.
DISCUSSION
This work provides supporting evidence that cardiorespiratory fitness may attenuate the deleterious effects of OSA on cerebral structure and perfusion in late-middle age to older adults. We likewise highlight important relationships between brain health and modifiable behavioral factors— namely sleep and fitness— that have the potential to help maintain or improve brain integrity with age. These findings are novel given that, to our knowledge, no prior studies have tested the modifying effect of a validated, non-exercise estimate of cardiorespiratory fitness in this regard, particularly using an array of core MRI-based measures of brain integrity.
Cardiorespiratory fitness has been shown to improve cardiovascular function and cerebrovascular health through a host of underlying mechanisms. In contrast, since OSA has been independently associated with decreasing ventricular function [27], adverse cardiac remodeling [28], and risk for vascular dementia [29], it is compelling to hypothesize that the observed protective effect of CRF may be mediated by changes across a spectrum of factors that confer cerebrovascular health. Indeed, a large body of work, including observational and intervention studies, has shown that physical activity is beneficial for maintaining cardiovascular function [35] and that habitual physical activity improves cognitive function and delays the pathophysiological cascade of AD. For example, a study by Erickson et al. demonstrated that aerobic training leads to increased hippocampal volume [30], a notion further reflected by findings on augmented hippocampal angiogenesis/neurogenesis [31] and perfusion [32] following structured aerobic training. Interrogating these mechanisms further in future works could clarify factors that explain the modifying effect of fitness on OSA severity.
While the relationship between CRF and favorable changes in GM and WM volumetrics are in agreement with extant literature, our findings showing lower CBF in the anterior cingulate and hippocampus in more fit participants is interesting as it may be somewhat counterintuitive. While fitness may indeed confer increased CBF to these regions, the response to OSA could reflect an adaption response, i.e., that for less fit individuals, intermittent hypoxia may trigger a compensatory response leading to increased CBF in regions sensitive to the transient loss of oxygen. Further work is needed to explore these underlying mechanisms.
A key limitation of the present study is its cross-sectional and observational design; in lacking a prospective framework, the associations we report here should not be interpreted as causal. Likewise, our findings may be confounded by unmeasured variables related to the outcomes tested. Furthermore, as noted previously, the study cohort is 96% White; therefore, our findings may not be generalizable to individuals from other racial or ethnic groups.
The severity of OSA in the present sample was representative of the general population, meaning that few participants had severe OSA (e.g., AHI > 30), which therefore limited our observation of OSA effects to primarily mild to moderate cases. A high percentage of participants were taking blood pressure medications at study entry; this may have unintentionally affected interactions between OSA and unmeasured fitness-dependent cerebrovascular changes.
While objective measures of CRF are described in literature, non-exercise indices such as our equation adapted from Jurca et al. are often utilized instead [15]. However, one limitation of the Jurca estimate comes from its dichotomous characterization of 150 weekly minutes of moderate physical activity, which limits the measure’s sensitivity to differences across the full spectrum of weekly exercise. Another potential limitation from this estimation stems from its use of self-reported physical activity— a method which may be vulnerable to measurement bias from faulty recall or social desirability [33]. However, our estimate of CRF was not based entirely (or even primarily) on this assessment, as the measure incorporated objective measures of both body size (height and weight in BMI) and resting heart rate. Furthermore, purely objective measures of physical fitness (such as graded exercise testing) may be unsuitable for individuals of advanced age; for example, measuring fitness via peak oxygen consumption during graded exercise has been shown to significantly underestimate cardiorespiratory fitness in advanced age [34].
Altogether, this work shows that cardiorespiratory fitness may attenuate the deleterious effects of sleep apnea on cerebral structure and perfusion in late-middle age to older adults. These findings motivate multiple prospective directions for future research in this regard; examples include: (a) interrogating the underlying mechanisms behind the moderating effect of CRF, perhaps through testing key factors related to cerebrovascular health; (b) isolating the effects of severe OSA (AHI≥30) to further explore the interaction with CRF at the highest OSA severity level; and (c) exploring longitudinal OSA data using linear mixed-models to test whether our observed moderating influence of CRF is indeed causal. Constructing a robust evidence base in this regard could further support the investigation of cerebrovascular risk modifiers as prospective targets for clinical intervention against deleterious age-related changes in brain health.
Footnotes
ACKNOWLEDGMENTS
Wisconsin ADRC is funded through the NIH National Institute on Aging and combines academic, clinical, and research expertise from the University of Wisconsin School of Medicine and Public Health and the Geriatric Research, Education, and Clinical Center (GRECC) of the William S. Middleton Memorial Veterans Hospital. For more information: www.adrc.wisc.edu.
FUNDING
This work was supported by United States National Institutes of Health grants R01AG062167, R01AG058680, R01HL62252, 1R01AG036838, and 1UL1RR025011.
CONFLICT OF INTEREST
Dr. Plante has served as a consultant for Teva Pharmaceuticals Australia, a consultant for Harmony Biosciences, and consultant/medical advisory board member for Jazz Pharmaceuticals. All other authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.