
Abstract
Background:
The relationship between cataracts and Alzheimer’s disease (AD) has been reported in recent observational studies. However, it is still unclear whether a causal effect of cataracts on AD or reverse causation exists.
Objective:
To explore the association between cataracts and AD genetically, we performed a bidirectional two-sample Mendelian randomization study.
Methods:
We obtained genetic instrumental variables related to cataracts and AD from recently published genome-wide association studies (GWASs). SNP-outcome associations for AD were obtained from a GWAS with 111,326 cases and 677,663 controls. SNP-outcome associations for cataracts were drawn from two sources: a GWAS with 67,844 cases and 517,399 controls and the FinnGen consortium (42,843 cases and 262,698 controls). Inverse variance weighted (IVW) was used as the primary method for Mendelian randomization (MR) analyses.
Results:
No genetic evidence suggested that cataracts were associated with the risk of AD (IVW odds ratio =1.04, 95% confidence interval: 0.98-1.10, p=0.199). In contrast, an effect of genetically determined AD on a decreased risk of cataract was observed with suggestive evidence (IVW odds ratio =0.96, 95% confidence interval: 0.93-0.99, p=0.004). However, this result might be distorted by survival bias.
Conclusion:
Genetically determined cataracts were not related to AD, as demonstrated by our study. In contrast, there was suggestive evidence that AD might prevent cataract development, but there might be potential survival bias. To define the exact association between the two diseases, more prospective research and studies on the pathogenesis are needed.
INTRODUCTION
Alzheimer’s disease (AD) is the most prevalent form of dementia and the fifth most common cause of death among people over 65 years, which begins with mild memory loss and possibly leads to the loss of conversation ability and response to environment-responding ability. Thus, AD can seriously affect one’s daily activities [1]. In 2020, Alzheimer’s Disease International estimated that approximately 50 million people suffer from dementia worldwide, and this number is projected to triple by 2050 [2, 3]. This results in large economic costs to those afflicted. AD treatment cost approximately $305 billion by 2020, increasing to more than $1 trillion as the population ages [4]. It is essential to identify risk factors or markers for the early stage of AD to prevent or halt disease progression.
In the elderly, visual impairment and low cognition are very common. Many studies have indicated that visual impairment may lead to cognitive problems [5–10]. It was reported that cataracts, the leading cause of blindness worldwide and which are caused by clouding of the lens in the eyes [11], were associated with an increased risk of AD [12–16]. A cohort study conducted by Lee et al. [14] determined that cataract extraction was significantly associated with lower risk of dementia development. This pioneering research may bring new methods to slow down or prevent age-related dementia. However, there were inconsistent findings in the literature [16–18]. For instance, a randomized controlled trial in 2006 suggested no cognitive benefits of cataract surgery in cognitively normal adults [16]. Moreover, the association between cataract and AD risk may be influenced by other confounders, including age, stroke, heart disease, diabetes, and depression. Patients with cataracts and these other conditions are more likely to develop AD [8]. It is still unclear whether cataract surgeries protect against AD.
Mendelian randomization (MR) is a method that uses genetic variation, typically single-nucleotide polymorphisms (SNPs), as instrumental variables to assess the causal relationship between the exposure and the outcome. A genetic variant must satisfy the following assumptions to be used for the causal effect estimation: i) the SNP is associated with the exposure (the relevance assumption), ii) the SNP is independent of common causes of the outcome (the independent assumption), and iii) the SNP affects the outcome only through the exposure (the exclusion restriction assumption) (Fig. 1). It can reduce bias in observational studies, such as reverse causation and residual confounding. MR is also a considerable tool when the exposure of interest is expensive or difficult to measure [19–21].
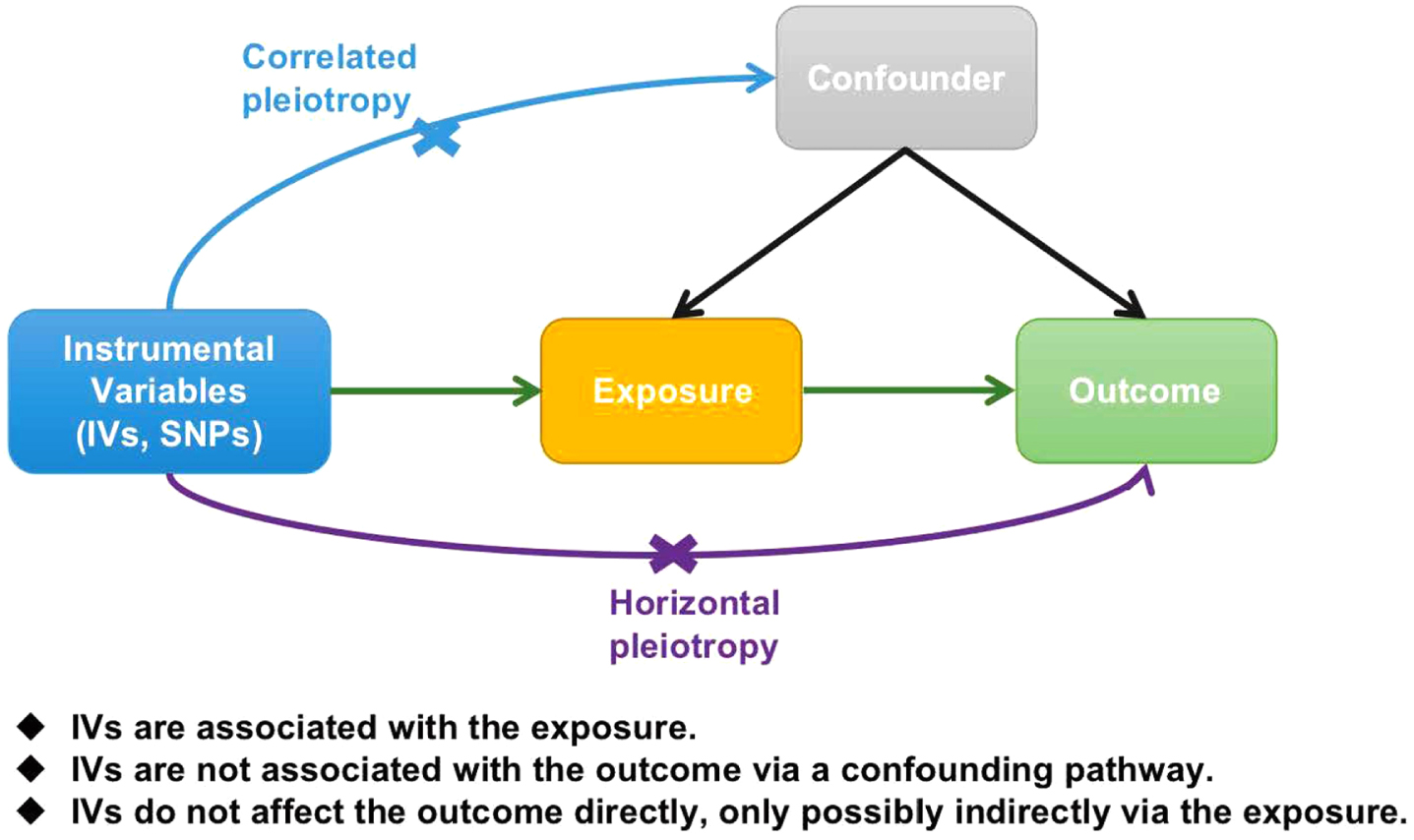
Mendelian randomization model. The fundamental conditions for a genetic variant to satisfy to be an IV are summarized as the picture shows. SNPs, single nucleotide polymorphisms; IVs, instrumental variables.
In order to test hypotheses about causal directions and influences of these two age-related diseases and to address the issues Lee et al. raised, we applied bidirectional two-sample MR using summary statistics from large-scale genome-wide association studies (GWASs) of cataracts and AD.
METHODS
We performed bidirectional two-sample MR studies of cataracts and AD (Fig. 2). All the procedures were consistent with the Strengthening the Reporting of Observational Studies in Epidemiology Using Mendelian Randomization (STROBE-MR) guidelines.

Flowchart of the studies design of Mendelian randomization analysis for the association between cataracts and AD. The flowcharts showed the progress of our study. The sources of GWASs databases, selections of IVs, and methods applied for MR analyses and sensitivity analyses were all presented clearly. a) Study design of Mendelian randomization analysis for cataract on AD; b) study design of Mendelian randomization analysis for AD on cataract. GWAS, genome-wide association study; SNP, single nucleotide polymorphism; LD, linkage disequilibrium; AD, Alzheimer’s disease; IVW, inverse variance weighted method.
Datasets and selection of the genetic instrumental variables
Summary statistics for cataracts were obtained from a multiethnic GWAS meta-analysis by Choquet et al. [22] This GWAS included 67,844 cataract cases and 517,399 controls from the Genetic Epidemiology Research in Adult Health and Aging (GERA) and the UK Biobank (UKB), in which the analyses were adjusted for age, sex, and ancestry principal components (PCs) [22]. They identified SNPs associated with the risk of developing cataracts at a significance threshold of 5.0 × 10-8.
Summary statistics for AD were obtained from a two-stage GWAS of European ancestry by the European Alzheimer & Dementia Biobank (EADB) consortium [23], which included a total of 111,326 clinically diagnosed or “proxy” AD cases and 677,663 controls. The stage I participants of this GWAS came from EADB, GR@ACE, European Alzheimer’s Disease Initiative, Genetic and Environmental Risk in AD/Defining Genetic, Polygenic, and Environmental Risk for Alzheimer’s Disease, DemGene, Bonn, the Rotterdam study, the Copenhagen City Heart Study study, the Neocodex–Murcia study, and the UKB, while the stage II participants came from the Alzheimer’s Disease Genetics Consortium, Cohorts for Heart and Aging Research in Genomic Epidemiology, and FinnGen consortia. SNPs were considered to be associated with the development of AD at a significance level of 5.0×10-8 in the stage I and II meta-analyses.
Genome-wide significant (p <5.0×10-8) SNPs were selected as genetic instrumental variables. In addition, we performed linkage disequilibrium clumping (LD) and pruned SNPs in LD (r2 >0.001) within a window of 10000 kb. The SNPs with the lowest p value were retained. We also looked up the SNPs in Phenoscanner (A database of human genotype-phenotype associations, http://www.phenoscanner.medschl.cam.ac.uk/) [24, 25] and GWAS Catalog (The NHGRI-EBI Catalog of human genome-wide association studies, https://www.ebi.ac.uk/gwas/) [26]. SNPs associated with other traits (p <5.0×10-8) that may affect our results were eliminated. We calculated the F-statistic of each SNP using the formula F = (beta/se)2 [27]. SNPs with an F-statistic <10 were considered weak genetic instrumental variables.
Datasets of SNP-outcome associations
The SNP-outcome associations for AD were obtained from the two-stage GWAS by the EADB consortium described above [23]. The SNP-outcome associations for cataracts were drawn from two sources: the GERA and UKB GWAS by Choquet et al. [22] (described above) and the R7 release of the FinnGen consortium [28]. In the FinnGen consortium, cataract cases were identified by an ICD-10 code of H25, and the numbers of cases and controls were 42,843 and 262,698, respectively. The genetic associations were adjusted for age, sex, 10 genetic PCs, and genotyping batch.
Power calculation
We calculated the statistical power through an online power calculator for MR analysis (https://shiny.cnsgenomics.com/mRnd/), where the alpha level was set to 0.05. The proportion of variance explained (PVE) was required in the power calculation, and we calculated the PVE using the formula PVE = varSigma(beta2/(beta2 + se2 × N)), where beta and se are the beta and se coefficients of each SNP and N represents the sample size [29].
MR analysis
We conducted bidirectional two-sample MR with the “TwoSampleMR” R package (https://mrcieu.github.io/TwoSampleMR/, R version 3.6.3). The genetic instrumental variables were extracted from the outcome summary statistics and were harmonized. During harmonization, we used effect allele frequencies to resolve the ambiguities of palindromic SNPs, i.e., SNPs with A/T or G/C alleles, for which the reference strands were unknown. The main analysis used for the MR is inverse variance weighted (IVW), which is the most efficient method if all genetic instrumental variables are valid [30]. Since the effect of AD on cataract was estimated using two sources of cataract summary statistics, we meta-analyzed the IVW results with Stata (version 16.0, Stata Corporation, College Station, TX) software. In addition, we performed weighted median, weight mode, and MR–Egger to assess the robustness and potential pleiotropic effects. The weighted median method is consistent even if up to 50% of the weights were contributed by invalid genetic instrumental variables [31]. The weighted mode method clusters genetic instrumental variables based on their similarity, and the causal effect is estimated using the cluster with the largest weight [32]. The weighted mode method is robust if the instrumental variables contributing to the cluster with the largest weight are valid [32]. The MR–Egger method can detect directional horizontal pleiotropy and make causal inferences that are not subject to pleiotropy, although it compromises power [33]. Moreover, leave-one-out analysis was performed by excluding one SNP and estimating the causal effect with the remaining SNPs to assess whether the causal inference was driven by a single SNP. Furthermore, we performed the MR pleiotropy residual sum and outlier test (MR-PRESSO) to detect outliers of genetic instrumental variables and estimate causal effects after removing outliers via the “MRPRESSO” R package [34].
RESULTS
Effect of cataracts on Alzheimer’s disease
Thirty-five SNPs were applied as genetic instrumental variables for cataracts (Supplementary Table 2). The F statistics ranged from 29.9 to 273.6 (Supplementary Table 1). MR analysis showed that there was no significant effect of genetically determined cataracts on the risk of AD (IVW: OR=1.04, 95% CI=0.98-1.10, p = 0.199; Figs. 3a, 4a, Supplementary Table 5). The results of the sensitivity analyses were similar to those of the main analysis (Table 1). There was no heterogeneity observed with the Cochran Q-test (Supplementary Figure 3). No pleiotropy was found by the MR-PRESSO global test and MR–Egger intercept. Leave-one-out plots suggested that the validity of inference did not depend on certain extreme SNPs (Supplementary Figure 2).
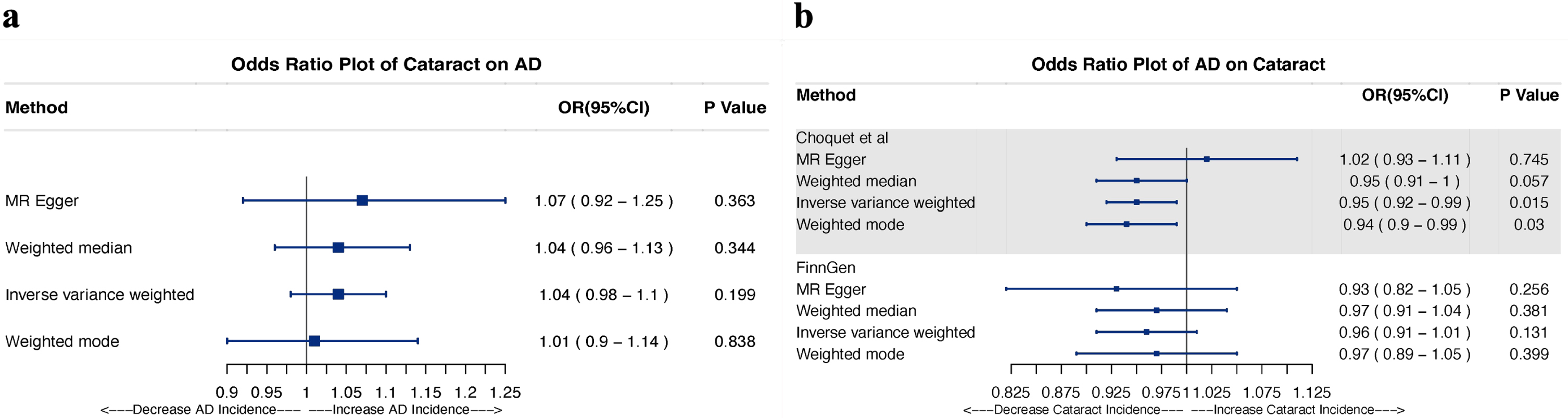
Association between genetically determined cataracts and AD. Odds ratio for the association between genetically predicted cataracts and AD. Four methods, including IVW, Weighted Median, MR Egger, and Weighted Mode, were used for the analyses. a) Odds ratio plot showing the effect of cataracts on AD; b) Odds ratio plot showing the effect of AD on cataracts. OR, odds ratio; CI, confidence interval; MR?Egger, Mendelian randomization-Egger; AD, Alzheimer’s disease.

Scatter plots of MR analyses between cataract and AD. The x-axes represent the genetic instrument associations with exposure, and the y-axes represent genetic instrument associations with outcome. The slope of each line corresponds to the estimated MR effect of each method. a) Scatter plot of MR analyses for cataract (Choquet et al.) on AD (Bellenguez et al.), b) Scatter plot of MR analyses for AD (Bellenguez et al.) on cataract (Choquet et al.); c) Scatter plot of MR analyses for AD (Bellenguez et al.) on cataract (Finngen). SNPs, single nucleotide polymorphisms; IVW, inverse variance-weighted; MR?Egger, Mendelian randomization-Egger; AD, Alzheimer’s disease.
Sensitivity analyses of the association between genetically determined cataract and AD. Three tests, including Heterogeneity test, MR PRESSO and Pleiotropy test were used for sensitivity analyses
IVW, inverse variance weighted; MR PRESSO, MR Pleiotropy RESidual Sum and Outlier; Q, Cochran’s Q statistics; OR, odds ratio; CI, confidence interval; AD, Alzheimer’s disease.
Effect of Alzheimer’s disease on cataracts
Eighty-three SNPs were reported to be associated with AD and related dementias in the research of Bellenguez’s team. We sorted 51 SNPs and 52 SNPs (Supplementary Tables 3 and 4), which were used as IVs to assess causal relationships in observational data sourced from Choquet’s study and the Finngen consortium, respectively. No weak instruments were used for F statistics calculated over 10 (Supplementary Tables 1, 3, and 4). Four MR methods, including IVW, MR–Egger, weighted median and weighted mode, were performed to estimate the causal effect in each outcome GWAS.
The MR analysis supported an effect of genetically determined AD on the risk of cataracts in the outcome database from Bellenguez. However, no significant effect was observed between genetically determined AD and cataracts in the FinnGen consortium (Figs. 3B, 4B, 4C, Supplementary Table 5). We discovered an effect of genetically determined AD on the decreased risk of cataracts after combining these two databases in the meta-analysis using a random effects model (Fig. 5). The results of the sensitivity analyses are shown in Table 1 and Supplementary Figure 3. Heterogeneity was detected by Cochran’s Q statistics. The MR-PRESSO global test revealed pleiotropic outliers in Choquet’s study; however, after correcting for outliers, the results were similar to those in IVW. No pleiotropic effect was detected by MR–Egger intercept. As a result of leave-one-out sensitivity analysis, no single SNP strongly violated the overall AD effect on cataracts (Supplementary Figure 2).

Effect of genetically determined AD on risk of cataract. We combined the estimated ORs from an inverse-variance weighted analysis of the two databases using multiplicative random meta-analyses. OR, odds ratio; CI, confidence interval; AD, Alzheimer’s disease.
DISCUSSION
As the leading cause of dementia, AD is a global health issue with huge societal and individual implications [35]. Therefore, identifying effective markers and strategies for preventing AD will have a significant impact on population health. A recent study found that nonsurgical cataract patients were at an increased risk of AD, but the risks could be reversed by cataract surgery [13, 14].
Researchers have also claimed that amyloid-β serves as a link between cataracts and AD, while these proteins found in the lens may indicate preclinical AD [36–38]. Despite the association between cataracts and AD, the possibility of using cataract-related proteins as biomarkers for the early detection of this disease remains controversial [17, 39]. Our study aimed to explore the bidirectional causal relationship between cataracts and AD using MR analysis.
To the best of our knowledge, our study was the first MR analysis to examine the potential relationships between cataracts and AD. Most of the previous studies in the field of cataract and AD were observational, which might be confounded by potential biases and reverse causation. MR analysis is designed to avoid these biases. Additionally, we obtained SNPs related to cataract or AD from recently published large GWASs. Our study provided novel insight into the association between cataracts and AD.
Our analyses suggested no effect of genetically determined cataracts on the risk of AD. Other studies investigating the relationship between cataracts and the risk of dementia yielded similar results [8]. Researchers hypothesized that the association between cataract and dementia risk might be partially mediated by a connection between cataract and other conditions associated with dementia risks such as stroke, heart disease, diabetes, and depression. Patients with cataracts and these other conditions are at higher risk of developing dementia than those with cataracts alone [8]. Grodstein et al. found no relation between cataracts and either low scores (RR = 0.99; 95% CI = 0.87-1.13) or a substantial decline from baseline to the second interview (RR = 1.08; CI = 0.93-1.25) of cognitive tests, and they concluded that cognitive function was unrelated to cataract extraction in females [18]. A randomized controlled trial conducted in Australia found that cataract surgery does not significantly influence neuropsychological test performance [16]. However, recent studies suggested that cataract extraction might be a protective action against AD based on their finding that cataract is a promising modifiable risk factor for AD [12, 13]. These researchers also admitted that participants who underwent cataract surgery might pay close attention to their health condition, so they were healthier and at lower risk of dementia because of healthy bias. Another challenging issue is immortal time bias which probably lead to overestimation of the outcome event rate in the unexposed group, under estimation of the event rate in the exposed group, or both [14, 41]. Therefore, more prospective research and studies on the pathogenesis are needed.
In the reverse analysis, we provided suggestive evidence [42] that AD may decrease the risk of cataract, while we did not find any relevant observational studies about the effect of AD on cataract. We supposed that there might be survival bias in the study. It has been reported survival bias may distort results in MR studies in the elderly [43–45]. AD increases mortality rates [46], and participants who died early of AD were less likely to develop cataract. This bias would have consequences as misinterpretation of correlation, or seeing a cause-and-effect relationship where there is not one. Therefore, further studies need to apply proper statistical approaches to alleviate this and other types of selection bias.
Limitations of our study should be acknowledged. First, the data related to AD are mostly derived from European ancestry. Our findings should not be directly generalized to other ethnic groups. Second, we detected heterogeneity in the reverse analysis. Caution should be taken in the interpretation of both the heterogeneity results and the MR investigation. The statistical power may still be insufficient to detect an effect of cataracts on AD in a single GWAS dataset (Supplementary Figure 4), although we analyzed the latest and largest databases, such as UKBB, FinnGen, and EADB. Finally, in the cataract GWAS, cases were defined as participants with a self-reported cataract operation (F20004 code 1435) or/and a hospital record including a diagnosis code (ICD-10: H25 or H26) [22]. As a result, we were also unable to distinguish the effect of surgery on AD in our study. Our paper left some directions for future studies.
Conclusion
Our study indicated that genetically determined cataracts are not associated with the risk of AD. The reverse MR analysis suggested that AD might be associated with a decreased risk of cataract. Whether cataract extraction is taken as a protective measure for AD still needs further study.
Footnotes
ACKNOWLEDGMENTS
Thank you for all investigators and instructions for making their GWAS data publicly available.
FUNDING
This work was supported by the Foundation of Health Commission of Sichuan Province (21PJ023) and China Postdoctoral Science Foundation (2022M710101).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
All data that support the findings of this study are available in the supplementary material of this article and referenced publications.