
Abstract
Background:
Family caregivers make end-of-life (EOL) decisions for persons with severe dementia (PWSDs). It is not known whether the family caregivers’ goals change over time.
Objective:
Assess caregivers’ EOL care goal for PWSDs and change in these goals over time.
Methods:
Using a prospective cohort of 215 caregivers of PWSDs, we assessed the proportion of caregivers whose EOL care goal for PWSDs changed between two consecutive time points. Mixed effects multinomial regression models assessed factors associated with caregivers’ EOL care goals for PWSD (maximal, moderate, minimal life extension); and change in EOL care goal from previous time point.
Results:
At baseline, 20% of the caregivers had a goal of maximal life extension for their PWSD, and 59% changed their EOL care goal at least once over a period of 16 months. Caregivers of PWSDs with lower quality of life (RR: 1.15, CI: 1.06, 1.24), who expected shorter life expectancy for PWSDs (RR: 10.34, CI: 2.14, 49.99) and who had an advance care planning discussion (RR: 3.52, CI: 1.11, 11.18) were more likely to have a goal of minimal life extension for PWSD. Caregivers with higher anticipatory grief (RR: 0.96, CI: 0.93,1) were more likely to have a goal of maximal life extension. Change in PWSDs’ quality of life and change in caregivers’ anticipatory grief were associated with change in caregivers’ EOL care goals.
Conclusion:
Caregivers’ EOL care goals for PWSDs change over time with change in PWSD and caregiver related factors. Findings have implications regarding how health care providers can engage with caregivers.
Keywords
INTRODUCTION
Dementia is a major cause of death worldwide [1]. It is estimated that there were 1.62 million deaths due to dementia globally in 2019 [2]. To provide patient-centered care, it is recommended that end-of-life (EOL) care should be aligned with patients’ wishes [3]. However, this is difficult to achieve in the context of dementia as persons with severe dementia (PWSDs) are unable to make or verbalize their own EOL care decisions [4–6]. Their EOL care decisions are thus made by their family caregivers, who may be unaware of PWSDs’ EOL care goals for themselves [7, 8]. It is thus relevant to understand caregivers’ EOL care goals for PWSDs and the factors associated with these goals.
Our previous work with patients with advanced cancer and heart failure has shown that patients’ goals and preferences for EOL care change over time based on what they are experiencing at that point in time, e.g., their quality of life, mood, and current understanding of prognosis [9–11]. If caregivers’ EOL care goals too change over time, then it suggests that these goals may not be well-formulated, potentially leading to decisional regret [6, 7], depression, and anxiety [6, 13] among caregivers after the EOL decisions are made. However, there is a dearth of literature assessing caregivers’ EOL care goals [14] as well as change in their EOL care goals [15].
Therefore, in this study, we first aimed to assess caregivers’ EOL care goals for PWSDs and the factors associated with these goals. As health care cost is a major concern for seriously ill patients in many countries [16], we assessed the trade-off between caregiver’s goals for life-extending treatments versus healthcare cost for these treatments. Our measure captures caregivers’ goal of extending PWSDs’ life even if it comes at a high cost.
Second, we aimed to assess the extent to which caregivers’ EOL care goals for PWSDs change over time. Based on previous literature among PWSDs, other seriously ill patients, older adults and their caregivers, we hypothesized that caregivers who had participated in an advance care planning (ACP) discussion [17, 18], with greater financial burden [19, 20], whose PWSDs’ quality of life was poorer [21, 22], who spent more time in caregiving [23, 24] and adult child caregivers [25] will be less likely to want maximal life extension for PWSDs. On the other hand, caregivers who are more satisfied with PWSDs’ quality of care [26], experiencing anticipatory grief [27, 28] and those who believe PWSDs have a better prognosis [10, 30] will be more likely to want maximal life extension for PWSDs. We also hypothesized that the change in time-varying factors, including change in PWSDs’ quality of life, caregiver financial burden, caregiver satisfaction with PWSDs’ quality of care and caregiver anticipatory grief will be associated with a change in caregivers’ EOL care goal for PWSDs.
METHODS
Setting
The study was conducted in Singapore, a rapidly aging country in South-East Asia. The prevalence of dementia is about 10% among older adults in the country [31]. Most people with dementia including PWSDs are cared for at home by their families, with the government policies too promoting ‘aging in place’ [32–35]. Consistent with Confucian values of filial piety, adult children take care for their older parents and make medical decisions for them [36, 37]. As a result, uptake of advance care planning remains low, further increasing the burden of decision making for caregivers [38, 39].
Study design and participants
We used data from PISCES (Panel study Investigating Status of Cognitively impaired Elderly in Singapore), a prospective cohort of 215 primary informal caregivers of community-dwelling PWSDs in Singapore. Following written consent, the study recruited patients (between May 2018 and March 2021) who met inclusion criteria of having a diagnosis of dementia with Functional Assessment Staging Test stage 6c or higher. Inclusion criteria for caregivers included being 21 years or above, Singapore citizen or permanent resident, being a family member and primary decision maker for PWSD, meeting the PWSD at least once a week and having intact cognition. Eligible caregivers were recruited from memory/geriatrics clinics and general medicine wards of seven major public restructured hospitals in Singapore, six home care foundations and two hospices. Healthcare providers at each site identified and approached eligible participants to take part in the study. Further details of the study protocol are published [40]. The study was approved by the Institutional Review Board at SingHealth and National University of Singapore.
Study variables
The caregivers were surveyed at baseline and every four months. We used data from five waves- baseline, 4, 8, 12, and 16 months.
Outcome variable
Caregivers’ goal for PWSDs’ EOL care: We asked caregivers about their treatment preferences for the PWSDs if they were to be hospitalized. Caregivers responded on scale of 1 to 9, with 1 representing ‘extend life as much as possible at high cost’ and 9 representing ‘no life extension at less cost’. Based on distribution of responses (Supplementary Appendix 1), we categorized the outcome measure as maximal (1–4), moderate (5), and minimal (6–9) life extension. We have used the same measure with other patient groups, and have found it to be associated with patients’ health carespending [41].
Change in caregivers’ goal for PWSDs’ EOL care from previous time-point: was assessed by comparing caregivers’ goal between two successive time points for which data was available. The dependent variable is thus the change in EOL care goal between 0 to 4 months, 4 to 8 months, 8 to 12 months, and 12 to 16 months. We categorized change in EOL care goal as: 1) no change in goal, 2) change in goal towards reduced life extension, 3) change in goal towards increased life extension.
Independent variables
PWSDs’ quality of life: was assessed using Quality of Life in Dementia (QUALID) [42], a composite measure of eleven items assessing PWSDs’ engagement with basic activities over the last week. Each item was scored from 1 to 5 and summed to create a total score ranging from 11 to 55, higher values signifying lower quality of life.
PWSDs’ EOL discussions: Caregivers were asked if PWSD had discussed their EOL care goal/preference with any family member (yes/no).
Caregivers’ satisfaction with PWSDs’ care: was assessed using a ten item scale, Satisfaction with Care at the End-of-Life in Dementia [43]; total score ranged from 10 to 40 and a higher score indicated greater satisfaction.
Caregivers’ anticipatory grief: was assessed using an 18-item Marwit-Meuser Caregiver Grief Inventory-Short form [44] (range: 18–90); higher score indicated greater grief.
Caregivers’ financial burden: was assessed based on caregivers’ response (strongly disagree to strongly agree) to two statements - “it is difficult to pay for the health expenses of the patient” and “caring for patient puts a financial strain on me”. Higher score indicated higher financial burden for the caregiver.
Caregivers’ ACP discussions: Caregivers were asked if they (or any other caregiver) had signed an ACP for the PWSD.
Caregivers’ expected life expectancy for PWSD: Caregivers were asked to indicate PWSDs’ current age and expected age of death. Expected life expectancy was calculated as the difference between the two and categorized as not reported (=1); 0 to 5 years (=2); 6 to 10 years (=3); more than 10 years (=4).
Caregivers’ relation to PWSDs: was categorized as spouse (=1), adult child (=2), and others (=3) (son/daughter-in-law, sibling, friend etc.).
Time spent in caregiving: Caregivers were asked to indicate on a typical care day in the last 30 days, the number of hours they spent in assisting the PWSD in Activities of Daily Living (toilet visits, eating, dressing etc) and Instrumental Activities of Daily Living (shopping, food preparation, housekeeping etc). Values ranged from 0–16 hours.
Statistical analysis
We first described the proportion of caregivers whose EOL care goal for PWSD changed from the previous survey and from baseline. Our model has repeated measures, i.e., each individual has one or more responses over time, which may not be independent from each other. To account for this, we ran mixed effects multinomial regression models with caregiver ID as the random effect. By doing this, we controlled for the random effects of each caregiver. For computational simplicity, we assumed a shared covariance structure, i.e., there is one variance that is estimated for the j-1 equations (j is the number of outcomes) in the model and there is no covariance. We ran this model for the following two outcomes.
Our first outcome was caregivers’ EOL care goal for PWSDs (maximal life-extension, moderate life-extension, minimal life extension). Independent variables in the model included PWSDs’ quality of life, PWSDs’ EOL discussions, caregivers’ satisfaction with PWSDs’ care, caregivers’ anticipatory grief, caregivers’ financial burden, caregivers’ ACP discussions, caregivers’ expected life expectancy for PWSD, time spent in caregiving and caregivers’ relation to PWSDs. Control variables include PWSDs’ sex and age.
Our second outcome was change in caregivers’ EOL care goal for PWSDs (no change in goal, change in goal towards reduced life extension, change in goal towards increased life extension). Independent variables in the model included change in PWSDs’ quality of life from previous time point, change in satisfaction with care from previous time point, change in financial burden from previous time point, change in anticipatory grief from previous time point and caregiver’s relation to PWSD. Control variables included PWSDs’ sex and age. This analysis was restricted to caregivers who responded to at least two consecutive surveys.
RESULTS
At baseline, we surveyed 215 caregivers of PWSDs. Their median age was 58 years [IQR: 52–63] and were mostly females (69%), Chinese (79%), and spouse (13%)/child (75%) (Table 1). Out of these, 181, 149, 143, and 124 caregivers answered follow-up surveys at 4, 8, 12 and 16 months respectively (Supplementary Figure 1). Of the 215 caregivers, 191 (89%) answered at least two surveys.
Baseline sample characteristics of caregivers (N = 215)
Shapiro-Wilks test was conducted to assess normality of all continuous variables. All variables were non-normal. IQR, inter quartile range; PWSD, persons with severe dementia.
At baseline, moderate life extension was the most preferred option among caregivers (40%), and maximal life extension was the least preferred option (20%). The proportion of caregivers opting for maximal life extension reduced with time (Supplementary Figure 2). By one year, 51.6% of the caregivers had changed their EOL care goal at least one time since baseline and by 16 months (end of study duration), 58.6% of the caregivers had changed their EOL care goal at least one time since baseline (Supplementary Table 2). Of the latter, 31.9% changed their EOL care goal once, 15.2% twice, 9.4% thrice and 2.1% four times. At each time point, around 29 to 36% changed their EOL care goal from the previous time point (Fig. 1).
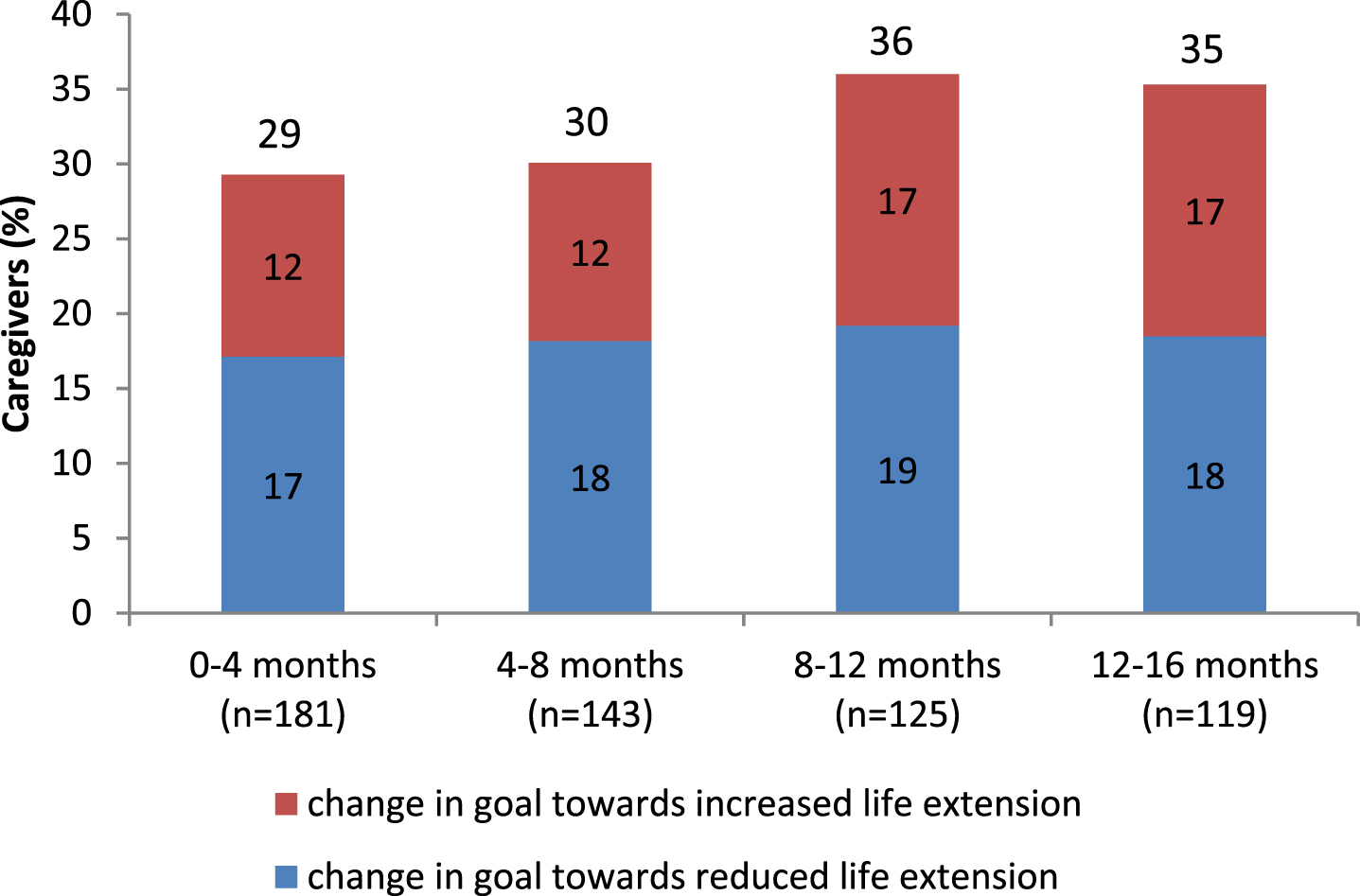
Proportion of caregivers who changed end-of-life care goal for persons with severe dementia from previous time point. *n is the number of people who answered survey n and n-1 (Supplementary Table 1/column 2).
Factors associated with caregivers’ EOL care goal for PWSDs (Table 2)
Caregivers reporting greater satisfaction with care received by PWSDs (RR: 0.87, CI: 0.77, 0.97; RR: 0.85, CI: 0.76, 0.96), and higher anticipatory grief (RR: 0.96, CI: 0.93, 1; RR: 0.96, CI: 0.93, 1) were less likely to have a goal for minimal or moderate life extension (versus maximal life extension). Caregivers of PWSDs with lower quality of life were more likely to have a goal of minimal life extension (RR: 1.15, CI: 1.06, 1.24) or moderate life extension (RR: 1.11, CI: 1.02, 1.20) (versus maximal life extension). Similarly, compared to caregivers whose expected life expectancy for their PWSD was over 10 years, those with less than 5 years (RR: 10.34, CI: 2.14, 49.99) and 6–10 years (RR: 18.02, CI: 3.69, 87.90) of expected life expectancy were more likely to have a goal of minimal life extension or moderate life extension (versus maximal life extension). Caregivers who had participated in an ACP discussion (RR: 3.52, CI: 1.11, 11.18) were also more likely to have a goal of minimal life extension compared to maximal life-extension. Contrary to hypothesis, we did not find any significant association of caregivers’ financial burden and caregiver-PWSD relationship with caregivers’ EOL care goal for PWSDs.
Factors associated with caregivers’ end-of-life care goals for person with severe dementia (PWSD) (N = 778)
RRR, relative risk ratio; CI, confidence interval; PWSD, persons with severe dementia; ACP, advance care planning; AD, Advance directive; EOL, End-of-life. Regression is controlled for age and sex *p < 0.10, **p < 0.05, ***p < 0.01.
Factors associated with change in caregivers’ EOL care goal for PWSDs from previous time point (Table 3)
Caregivers whose PWSDs’ quality of life had decreased from previous time point (RR: 1.06, CI: 1.01, 1.10) were more likely to change their EOL care goal towards reduced life extension. Caregivers who experienced an increase in anticipatory grief from the previous time point (RR: 0.97, CI: 0.94, 1) were less likely to change their EOL care goal towards reduced life extension.
Factors associated with change in caregivers’ end-of-life care goals for person with severe dementia (PWSD) (N = 539)
RRR, relative risk ratio; CI, confidence interval; PWSD, persons with severe dementia; Regression is controlled for age and sex. *p < 0.10, **p < 0.05, ***p < 0.01.
DISCUSSION
The study results highlighted the variation in caregivers’ EOL care goals for PWSDs and that 59% of the caregivers changed their EOL care goal over time during a study duration of 16 months. Results suggest that most caregivers’ EOL care goals for PWSDs may not be well-formulated, and may vary with their experiences with PWSDs’ illness and their reaction to it at that point in time. This has implications for caregivers’ EOL decision making for PWSDs.
Our results showed that several factors are associated with caregivers’ EOL care goals for PWSDs. Caregivers of PWSDs with lower quality of life, caregivers whose expected life expectancy of PWSDs was lower and caregivers who had an ACP discussion favoured minimal life extension for PWSD. Previous studies among other caregivers of PWSDs and of patients with other illnesses have also shown that caregivers and physicians who perceive patients’ quality of life and prognosis to be poor were less likely to prefer aggressive life extending treatments for patients [21, 45]. Caregivers may feel that life-extending treatments may reduce PWSDs’ quality of life even further, enhancing their suffering. Past evidence also suggests that optimism about patient’s prognosis is associated with greater preference for life extension [10, 30] and that caregivers who participate in ACP and EOL discussions have a more accurate understanding of patient’s prognosis and preferences [17, 18]. Despite the plausible benefits of these discussions, caregivers’ participation in ACP remains low with only 15% of caregivers in our sample having participated in ACP.
Caregivers who were satisfied with care received were more likely to favour maximal life extension for the PWSD. Past evidence shows that EOL care goals are associated with both good and bad care experiences, and satisfaction with care [26]. Similarly, caregivers who experienced higher anticipatory grief were more likely to favour maximal life extension for the PWSD. As caregivers’ intensity of grief increases, caregivers threatened with the impending loss of PWSDs may intensify their attachment behaviours [27, 28], and thus be more willing to use life extending treatments for PWSDs. Our previous work has also shown that many caregivers prefer to use life extending treatments due to fear of losing the PWSD [46].
During the study duration of 16 months, about 59% of the caregivers changed their EOL care goal for the PWSD at least once since baseline. This is consistent with our previous work reporting that patients’ preferences change over time and that these preferences vary with patients’ experiences, e.g., quality of life and mood at that point in time [9–11]. The current study highlights, that caregivers too experience the same phenomenon, and that change in caregivers’ EOL goals is associated with change in PWSDs’ quality of life and change in their own anticipatory grief.
Our results have clinical implications. In the context of severe dementia, the burden of making decisions for PWSDs falls on their family caregiver. However, this has been shown to be an emotionally challenging task [6], made even more burdensome due to caregivers not being aware of PWSDs’ own preferences and goals for themselves. As a result, caregivers’ decisions for PWSDs are guided by their own goals [47], often resulting in aggressive EOL treatments for PWSDs [4, 48] and decisional regret [6, 7], depression and anxiety [6, 13] among caregivers. Our findings can guide health care providers during ACP and EOL discussions in helping caregivers make informed decisions for PWSDs.
First, as caregivers’ EOL goals change over time, ACP discussions should be a continuous process rather than a one-time intervention. Second, we found that caregivers’ goals for PWSDs and change in these goals are associated with PWSDs’ quality of life as well as their own emotions at that point in time (e.g., anticipatory grief). Evidence show that many patients also want their caregivers to adjust their care goals for them based on changing circumstances [49]. However, when caregivers experience heightened emotions, this can impede their rational decision making. Thus, health care providers should first support the caregivers by helping them cope and come to terms with the impending loss of their loved one. Effectively managing these emotions can make it easier for health care providers to engage in EOL discussions with caregivers. Lastly, about 25% of caregivers in our sample, expected the PWSD to live more than 5 years. Studies show that median survival after a diagnosis of dementia is 3.7 years, though it varies by sex and age at diagnosis [50]. Similar optimism in predicting patients’ life expectancy has previously been reported among caregivers, physicians, and patients themselves [51–53]. Our results show that, caregivers whose expected life expectancy for the PWSD is lower have a lower preference for life extension. This highlights the importance of discussing prognosis so that caregivers can have a more realistic understanding of PWSDs’ life-expectancy, and thus make more informed decisions.
The main strength of our study is our longitudinal dataset enabling us to capture caregivers’ EOL goals for PWSDs every four months over a period of 16 months. We used validated scales to measure variables such as quality of life, anticipatory grief, and satisfaction with care. Our study also has limitations. First, there was attrition in our sample over time due to death of PWSDs and loss to follow up of their caregivers. Second, the question assessing caregivers’ EOL care goal for PWSD may not exactly mirror the conversations between caregivers and health care providers, and thus the generalizability of our study results to these conversations needs to be explored. Third, caregiving duration may be an important factor affecting caregivers’ EOL care goals for PWSDs but we did not have access to this data. Lastly, our results may not generalize to settings where treatment costs are not a major concern.
In conclusion, our results showed that caregivers’ EOL goals for PWSDs changed over time with change in PWSDs’ quality of life and caregivers’ own anticipatory grief, expected life expectancy of PWSD and satisfaction with PWSDs’ care. Our findings suggest that ACP and EOL discussions with caregivers should be a continuous process rather than a one-time intervention, and that managing caregivers’ emotions and optimism regarding PWSDs’ prognosis, can enable health care providers to help caregivers make more informed decisions for PWSDs.
Footnotes
ACKNOWLEDGMENTS
We would like to thank the team involved at each site for their assistance in the recruitment and screening of study participants, and our team of data collectors (Lien Centre for Palliative Care) for their contributions to the study.
FUNDING
This work was supported by funding from National Medical Research Council’s Health Services Research Grant (NMRC/HSRG/0081/2017), COVID-19 Top-up Grant (COVID19TUG21-0031) and Lien Centre for Palliative Care Research Award (LCPC Grant: LCPC-IN21-0001).
CONFLICT OF INTEREST
We have no conflict of interest to disclose and we have not received any financial consideration from any person or organization to support the preparation, analysis, results or discussion of this paper.
DATA AVAILABILITY
The data supporting the findings of this study are available on reasonable request from the corresponding author.