
Abstract
Until 300,000 years ago, ancestors of modern humans ubiquitously carried the apolipoprotein E (APOE) ɛ4/ɛ4 genotype, when the ɛ3 allele mutated from the ancestral ɛ4, which elevates the risk of Alzheimer’s disease. Modern humans living today predominantly carry the ɛ3 allele, which provides protection against heart disease and dementia in long-lived populations. The ancestral ɛ4 allele has been highly preserved in isolated populations in tropical and Arctic regions with high pathogen burdens, e.g., helminths. Early humans experienced serious enteric infections that exerted evolutionary selection pressure, and factors that mitigate infant and childhood mortality from enteric infections also exert selection pressure. Some bacteria can exploit the host’s defensive inflammatory response to colonize and invade the host. Pathogen-induced inflammation associated with infant and childhood diarrhea can damage the gut wall long after the invading organisms are no longer present. Inflammation not only resides in the mucosal wall, but also induces systemic inflammation. Baseline systemic inflammation is lower in ɛ4 carriers, yet ɛ4 carriers display a stronger host inflammatory response that reduces pathogen burdens, increasing infant and early childhood survival. Evolutionary selection of the ɛ3 allele likely occurred after humans moved into temperate zones with lower pathogen burdens, unrelated to protection from Alzheimer’s disease.
THE APOLIPOPROTEIN ɛ3 ALLELE EVOLUTIONARILY OUTCOMPETED THE ɛ4 ALLELE
There are three common alleles of the apolipoprotein (APOE) gene, i.e., APOE ɛ2, APOE ɛ3, and APOE ɛ4 [1]. In the general United States (US) population, the ɛ4 allele prevalence is approximately 25.5%, constituted by a small portion of ɛ4 homozygous individuals (2% of the US population) with a larger proportion being ɛ3/ɛ4 (22%) and ɛ2/ɛ4 heterozygous (1.5%) [2]. Until 300,000 years ago, ancestors of modern humans were ubiquitously ɛ4/ɛ4, and then the ɛ3 allele mutated from the ancestral ɛ4 allele [3]. The ɛ3 allele displayed a competitive survival advantage sufficiently robust to result in the current predominance of the APOE ɛ3 gene, with a presence in approximately 96% of the US population with more than 60% being homozygous ɛ3/ɛ3. One thought was that the ɛ3 was successful because of its protection against atherosclerotic heart disease, memory loss, and dementia in progressively older age ranges [4]. Similarly, the ɛ2 allele mutated from the ɛ3 allele about 200,000 years ago, but this protective allele has remained relatively rare, with the homozygous ɛ2/ɛ2 variant less than 1%, and ɛ2/ɛ3 heterozygosity occurring in about 11% of the population. The failure of the ɛ2 allele to compete successfully against the ɛ3 allele is not surprising given that its benefit on longevity and cognition [5], and protection from AD pathology [6, 7] does not contribute to survivability until an advanced age well after the average life expectancy, particularly of hunter gatherer populations. In addition, possession of the ɛ2 allele is associated with elevated triglyceride levels, which can increase heart disease risk in middle-aged individuals, and predispose to certain infections that can occur in younger age groups [8, 9].
Possession of one ɛ4 allele increases the risk of developing AD by 3 to 4-fold, and possession of two ɛ4 alleles increases risk by 15-fold, as compared with the ɛ3/ɛ3 genotype, with a large part of the variation being related to substantially earlier age of onset. Over 60% of patients with “non-familial” AD carry the ɛ4 allele [4, 10, 11]. This profound difference in AD risk is a consequence of conformational changes resulting from minor differences in the sequences of the APOE alleles. The three isoforms of APOE differ in amino acid sequence at only amino acid positions 112 and 158: the APOE ɛ2 allele has cysteine at both positions; the APOE ɛ4 allele has arginine at both positions and the APOE ɛ3 allele has cysteine at 112 and arginine at 158 [12, 13].
ɛ4 ALLELE PREVALENCE IS HIGHER IN AREAS WITH GREATER PATHOGEN BURDENS
The prevalence of the ancestral apolipoprotein ɛ4 allele is highest in hunter-gatherer populations residing in the high pathogen environments of the tropics or Arctic zones [14]. Tropical populations with a high prevalence of ɛ4 carriers include the San people in Southern Africa [15], pigmies in the Congo [16], sub-Saharan tribes including the Fon, Zairians, and Tutsi [16], New Guineans [17], Malaysian and Australian aborigines [18], and the Sami of northern Scandinavia. In addition, the population frequency of the ɛ4 allele decreases and the ɛ3 allele increases when moving from southern to northern latitudes [18–21], until reaching the sub-Arctic and Arctic zones where the ɛ4 allele begins to increase in frequency again [14].
Each of the ancient populations noted above experiences a significant burden of infectious disease including infestation from a variety of parasites endemic to the tropics or equatorial zones [22–24], or helminths found in the Arctic zone [25–32]. In contrast with other ancient peoples who live in hot weather climates, the Sami are descended from nomadic peoples who had inhabited northern Scandinavia for thousands of years [33]. The case of the ancient Sami people suggests that it is the parasite burden rather than the climate itself or latitude that is the critical factor in the persistence of the ɛ4 allele. The Sami people have a very high ɛ4 frequency of 0.31, a level equivalent to that seen in current descendants of ancient tropical populations [34]. From several thousand to a few hundred years ago, the Sami hunted reindeer (domesticated caribou) and kept them in small numbers as pack and decoy animals [33]. For only a comparatively short time of their residency across northern Scandinavia, probably the past few hundred years, the Sami transitioned from nomadic hunting to reindeer herding.
The diet of the ancient nomadic Sami people can be extrapolated from dietary histories provided by current Sami peoples, some of whom are still nomadic. The ancestral Sami probably relied upon five main sources of protein: all edible parts of the reindeer including the blood; all edible parts of the moose; a cold freshwater fish related to salmon and trout called the arctic char; a freshwater fish related to salmon called the whitefish; and Kalix roe, i.e., the eggs of the saltwater vendace fish native to Bothian Bay on the coast between Sweden and Finland. Of these five protein sources, reindeer were and are the most important by far [35]. Throughout their circumpolar distribution, reindeer are known to be infected by several parasites including Brucellosis, foot rot, warble and bot flies, and gastrointestinal roundworms. Reindeer are frequently infected with Brucella suis biotype 4. Humans can become infected by eating or handling uncooked infected meat, milk, etc. The ancient Sami people would have been exposed to Brucellosis and other infectious organisms [36].
INFANT AND CHILDHOOD MORTALITY IS VERY HIGH IN HUNTER-GATHERERS
The San people of Southern Africa are the most ancient extant human population identified and studied [37–40]. The San people of this region had a population of several million until about 1,500 years ago when competition from cattle herders began pressuring the population downward [41] to its current levels of approximately 100,000 [42]. Twenty percent of San infants die within their first year, most commonly from gastrointestinal infections. Fifty percent of San children die before the age of 15 [41]. Also, adult San have a short average lifespan of only 45–50 years, with only 10% of the San population surviving past age 60 [41].
The high infant mortality rate in the San population is observed in other hunter-gatherer populations. Overall, infant mortality is over 30 times greater among hunter-gatherers than in the United States [43]. Early childhood mortality is over 100 times greater in hunter-gatherer populations than in the United States. On the average, only 57% of children survive to age 15 years in hunter-gatherer populations [43]. If a hunter-gatherer child reaches the age of 15, there is a 64% chance that he or she will live to or past the age of 45 [43].
ENTERIC INFECTIONS IN ɛ4 CARRIERS
Oria et al. [44] measured the degree of Giardia infections in stool samples in Brazilian children living in shantytowns. Carriers of the ɛ4 allele had fewer Giardia infections [44]. The high bacterial count in the normal human gut results in an overall load of approximately one gram of endotoxin. The vast majority of this one gram does not access the bloodstream as only 100 ng of endotoxin injected intravenously induces inflammatory activation of the blood, somatic organs, and brain. As compared with APOE ɛ3 carriers, APOE ɛ4 carriers produce a stronger innate immune response when challenged by lipopolysaccharide (LPS). This result has been duplicated in APOE ɛ4 mice [45].
In humans, vitamin D deficiency has been associated with increased risk of respiratory infections, Clostridium difficile infection of the GI tract, and bacterial sepsis. Ryz et al. (2015) [46] employed a mouse model to study the mechanism of vitamin D3 on susceptibility to enteric infection with Citrobacter rodentium (C. rodentium). This enteropathogenic bacteria can cause a self-limiting colitis in mice. Vitamin D3 deficiency in mice increased intestinal inflammation that killed some of the normal gut flora thereby allowing C. rodentium to overgrow and cause colitis. If the mice receive a relatively high dose of vitamin D3, the action of Th17 T-cells can be inhibited. In this murine model, too little or too much vitamin D3 can promote gut inflammation and increase susceptibility to enteric infection via C. rodentium. Huebbe et al. [47] demonstrated higher 25(OH)D (vitamin D) levels in APOE ɛ4 targeted replacement mice as compared with APOE ɛ3 and ɛ2 mice. A similar allele association in elevation in vitamin D levels was observed in a small group of human research subjects (N = 93; p < 0.072), and in a larger general population sample (N = 699; p < 0.003).
Toll-like receptors (TLRs) are membrane-spanning receptors expressed on macrophages and dendritic cells. TLRs recognize specific proteins derived from bacteria. Gale et al. [48] showed that whole blood from healthy ɛ3/ɛ4 carriers stimulated by TLR2, TLR4, and TLR5 ligands induced more pro-inflammatory cytokine secretion than whole blood from ɛ3/ɛ3 carriers. In addition, following intravenous injection of LPS, ɛ3/ɛ4 carriers experienced higher hyperthermia and plasma TNFα, and earlier IL-6 release than ɛ3/ɛ3 carriers. Taken together, these results suggest a more robust innate immune response in humans who possess at least one copy of the ɛ4 allele.
In a murine model that produced mice homozygous for either APOE ɛ2, ɛ3, or ɛ4, allele status was associated with significant differences in the composition of the gut biome. The relative abundance of Erysipelotrichia (bacteria of the phylum Bacillota) was associated with APOE ɛ4 status, a finding also seen in humans [49]. In a similar murine model, APOE ɛ4 status was associated with a relative abundance of bacteria from the Lactobacillaceae family. This finding might be of clinical significance as an increase in Lactobacillus has been associated with localized acidification via lactic acid and hydrogen peroxide secretion. The acidic microenvironment is thought to reduce colonization by pathogenic bacteria including Cryptosporidium, and fungal infections [50].
APOE affects inflammatory processes in murine models of infection concomitant with malnutrition. Azevedo et al. [51] examined the role of APOE alleles in genetic strains of mice developed to model the effects of gut inflammation in a malnourished host. Mice were fed a low protein diet and infected with Cryptosporidium parvum (C. parvum). Transgenic APOE ɛ4/ɛ4 mice had less weight loss than either transgenic ɛ3/ɛ3 or wild-type mice, showed an accelerated pace of bacterial killing, and displayed better intestinal villi. APOE ɛ4 contributes to a regulated cytokine response in C. parvum infected, transgenic ɛ4/ɛ4 mice characterized by increased ileal L-arginine selective cationic protein transporter (CAT-1), arginase-1 (possible marker of ileal recovery), and TLR9 transcripts. TLR9 binds bacterial and viral DNA thereby eliciting signaling cascades leading to release of pro-inflammatory cytokines. These data suggest that the ɛ4 allele resists infection with C. parvum and assists in intestinal normalization post-infection.
The normal function of the inflammatory arm of the innate immune system is to combat infection and tissue injury [52]. Pathogens use many different defense mechanisms to aid in their invasion of their hosts [53], one of which is the hijacking of host inflammation to facilitate invasion and colonization [54]. The first demonstration of this facet of pathogen defense was reported in 1966 by Gray and Killenger [55]. They showed that Listeria monocytogenes invades macrophages recruited to the site of infection and travels inside the macrophages to distant tissues. Shigella recruit neutrophils across the epithelium, rupturing the epithelial barrier, thereby trading off some degree of neutrophilic killing of the Shigella for enhanced entry of the surviving bacteria into the host [56]. The pro-inflammatory cytokines interferon-γ and TNF-α can disrupt tight junctions between cells thereby increasing intercellular permeability [57].
Helicobacter pylori (H. pylori) uses gastric epithelial inflammation to establish long-term colonization [58]. Although H. pylori elicits a strong inflammatory response, the bacteria dampen host immune responses to facilitate chronic colonization of the stomach. CD4+ helper T cells are the most important T cell subtype involved in responses to H. pylori infection, with contributions from Th1 and Th17 cells, and regulatory T cells. H. pylori predominately elicits the production of Th1-type cytokines induced by IL-12 release by neutrophils and monocytes. H. pylori releases virulence factors that inhibit antigen presentation to T cells, block T cell proliferation, and suppress Th1 responses. Therefore, although H. pylori raises a strong innate immune response with attendant chronic inflammation, its immunosuppressive abilities facilitate bacterial persistence and long-term residence in the gastric mucosa [59].
Salmonella typhimurium (S. typhimurium) can invade the GI tract and cause diarrhea and acute intestinal inflammation eliciting a neutrophilic infiltrate. These bacteria enter and survive in mucosal macrophages residing in intestinal epithelium. In the inflamed gut, the growth of S. typhimurium is enhanced as other microbes are outcompeted. The mechanism underlying Salmonella overgrowth in intestinal inflammation is unclear. A possible mechanism is the reaction of inflammation-associated activated oxygen species with thiosulfate naturally resident in the gut to form tetrathionate, a respiratory electron acceptor. Tetrathionate allows S. typhimurium to utilize respiration and outcompete other gut microbes reliant on anerobic fermentation [60].
Several lines of evidence suggest that some pathogens use host inflammation to kill competitor pathogens. Brown et al. [25] have modeled the growth kinetics of how a particular pathogen can trigger host inflammation to the detriment of competitor pathogens. In humans, S. typhimurium induces a self-limiting gastroenteritis. Due to the similarity between human and porcine S. typhimurium-induced gastroenteritis, Chirullo et al. [61] used piglets to model Salmonellosis. These authors showed that wild-type strain S. typhimurium (STM14028) can employ host inflammation to enhance an active infection. STM14028 efficiently colonizes in vitro porcine monocytes-macrophages and intestinal columnar epithelial (IPEC-J2) cells. If the cells are pre-treated with pro-inflammatory LPS, the degree of STM14028 colonization increases. If an LPS antagonist is used to inhibit the pro-inflammatory effect of LPS, the increased colonization is inhibited. In the in vivo arm of the Chirullo et al. [68] experiment, the pathogenicity of STM14028 in the presence and absence of inflammation was examined. When pro-inflammatory LPS is co-administered with S. typhimurium via the intraperitoneal (i.p.) route to piglets, at four hours post-infection both body temperature and blood cytokine levels are increased, consistent with the induction of acute inflammation. As compared with i.p. injection with S. typhimurium alone, co-administration of the bacteria with LPS showed a significant increase in colonization of tonsils, cecum, and spleen [61]. Also, Salmonella might derive nutrients from the inflammatory mucosa to stimulate growth. In addition, a gut wall highly colonized with different strains of bacteria represents a colonization barrier to new bacterial strain infection [62, 63]. Inflammation can kill a significant number of the bacterial strains colonizing the gut wall thereby facilitating the entry of a new infective bacterial strain [64]. Antibiotic treatment can illustrate this principle when normal gut flora are killed thereby facilitating the growth of more harmful strains, e.g. Clostridium difficile [65].
DAMAGE FROM PATHOGEN-INDUCED INFLAMMATION TO PEDIATRIC GUT STRUCTURE AND FUNCTION
Damage to the small bowel associated with pediatric diarrhea has a complex etiology [66]. Overgrowth of the normal microbiome of the gut by anaerobic bacteria such as Veillonella and Bacteroides species, predisposes to intestinal mucosal injury [67]. These and other strains of anaerobic bacteria chemically modify the primary bile acids cholic and chenodeoxycholic acid and convert them into deoxycholic and lithocholic acid, which are highly damaging to the jejunal mucosa. In the bowel lumen, deoxycholic and lithocholic acid induce water and sodium glucose malabsorption, increase intestinal permeability, and facilitate entry of intact and therefore potentially allergenic macromolecules. Dietary fats are solubilized in mixed micelles, which are disrupted by deoxycholic and lithocholic acid, leading to abnormal fecal excretion of dietary fats [66]. In rural West African children, enteropathy from chronic diarrhea has been shown to be mediated by T cells [68]. The pathological increase in intestinal permeability associated with chronic pediatric diarrhea has also been shown to cause endotoxemia, wherein LPS from intestinal bacteria enter the bloodstream. The presence of endotoxin (LPS) in the bloodstream leads to systemic inflammation [69]. While diarrhea initiates the enteropathy, post-initiation the enteropathy only co-exists with infant diarrhea for 10% of the time [70]. Once initiated, the enteropathy appears to perpetuate itself presumably via antigens passing from the intestinal lumen and into the mucosa where T-cell stimulation elicits further damage to the tissue [68].
ENTERIC INFECTIONS ARE A MAJOR CAUSE OF MORTALITY AND MORBIDITY IN HUNTER-GATHERER INFANTS AND CHILDREN
In surviving hunter-gatherer and extant pre-industrial populations, enteric infections represent a major cause of mortality and morbidity in infants and children. For example, gastrointestinal infections are responsible for the majority of the 20% infant mortality rate seen in San People [41]. Although data on infant mortality due to enteric infection in ancestral hunter-gatherers are not available, today one in nine child deaths worldwide are due to diarrheal disease [71], the vast majority of which occur in less developed countries. Enteric infections are not only endemic in tropical and warm climates but are also endemic in hunter gatherer populations in the Arctic [72]. In 1959, Gordon and Babbott [73] reviewed the causes and frequency of acute intestinal infection in the Arctic. In Alaska, parasites were found in 62 of 227 residents in the Kuskokwim delta. In 1958, Fournelle et al. [74] examined 1,680 Alaskan Inuits and reported an infection rate of 40% for protozoa and 12% for helminths. Most of the helminths observed by Fournelle et al. [74] were diphyllobothriasis tapeworms found in raw or undercooked fish. Enteric infection rates were very high in Greenland, with 78 per cent of 274 Inuits examined having parasites with protozoa infection being about six times more common than helminth infection [73].
Early humans experienced enteric infections that have exerted a significant degree of evolutionary selection pressure [22]. Fumagalli et al. [22] calculated that the evolutionary pressure imposed by parasitic worms (helminths) on human genes has been stronger than pressure due to viral, protozoa, or bacterial agents. Based on results from Dunne and Cooke [75], Fumagalli et al. [22] have postulated that helminths evolve slower than unicellular/viral agents and have complex life cycles thereby resulting in relatively stable geographic distributions. Further, helminths and humans evolved on similar timescales that facilitated co-evolutionary interaction between the human host and parasite. Faster evolving species like viruses might not exert the same, or as long-lasting, selective pressure as helminths toward inducing change in ɛ4 allele frequencies [22].
In 1961, HJ Heinz published a study on parasitical infections in ancient San people adult males who at that time were still living in the Kalahari Desert according to their ancestral lifestyle [76]. In 220 stool samples studied, the only pathogen found was the hookworm Necator americanus, as the many different species of parasitical worms that afflict other sub-Saharan African tribes are not able to survive in the arid conditions of the Kalahari [76]. Hookworm infections are more persistent than many other pathogens because of their ability to co-exist with the host by inhibiting the immune system. The Kalahari Desert is relatively wet from November to March. A San tribesman infected during this wet period during which hookworms can live outside of a host can continue to carry the hookworm infection into the dry season from April to October.
Loukas and Prociv [77] have reviewed immune responses to hookworms. In their review, these authors noted that protective immunity to hookworms does not develop in humans so that prolonged infections occur in all age groups. Both the larval stage and adult hookworms elicit a type 2 T-helper type immune response characterized by activated mast cells in gut mucosa, elevated serum IgE levels and eosinophils [77]. The lack of protective immunity against hookworm is consistent with the dry season infection rate of 26%, and wet season hookworm infection rate of 89.5% (17 out of 19 San men) observed by Heinz [76]. High hookworm infection rates in San adults implies that infants and children also experienced significant infection rates as infection is acquired by invasion of the infective larval stages through the skin [78].
Children and adults can display differential immune responses to the same enteric pathogen. Shigella is a bacterium that can cause enteritis that is usually more serious in children than in adults. Raqib et al. [79] showed that children with shigellosis have persistent activation of the innate immune response in the post-acute infection convalescent phase. The persistence of immune activation indicates delayed elimination of Shigella antigens in children [79].
APOE ɛ4 PROTECTS COGNITION IN PEDIATRIC ENTERIC INFECTIONS
Several large epidemiology studies have reported a relationship between elevations in systemic markers of inflammation and declines in cognition [80]. Inflammatory markers have suggested a pro-inflammatory state in cognitive decline including CD40 ligand, C-Reactive Protein (CRP), IL-6, soluble intracellular adhesion molecule-1, monocyte chemoattractant protein-1, myeloperoxidase, osteoprotegerin (OPG), P-selectin, TNF-α, and TNF receptor. Microglial cells are thought to play an important role in modulating neuroinflammatory processes related to the development of Alzheimer’s disease [80].
Oria et al. [44, 81, 82] have shown that possession of the ɛ4 allele protects against long-term cognitive deficits associated with severe diarrhea in Brazilian shanty-town children. The children were tested for verbal fluency according to the NEPSY Developmental Neuropsychological Assessment booklet. Coding test performance was evaluated using paired associated symbol recall (ages 8–16 years) in the standard WISC-111 protocol. To measure the child’s ability to plan and to inhibit impulsive responses the children were administered Elithorn mazes (ages 8–16 years). The cognitive protection might be related to a greater availability of cholesterol to the developing brain in ɛ4 carriers. In glial cells, APOE ɛ4 knockout mice display an increased activity of the arginine cationic transporter thereby increasing nitric oxide levels. It can be postulated that the enterocytes lining the intestines of APOE ɛ4 positive humans might also experience elevated nitric oxide levels which could enhance intestinal immunity [82].
Escherichia coli is the bacterial pathogen most commonly associated with endemic forms of childhood diarrhea [83], although several other pathogens are also common including Norovirus GII, shiga toxin-producing Escherichia coli (STEC), Giardia, and Sapovirus [24]. Trumble et al. [84] studied Amazonian Amerindians with high parasite burdens and found that the ɛ4 allele is associated with improved cognitive function. In human populations not stratified by APOE allelic type, parasite infections have been shown to impair cognitive function [85–87]. Eosinophil counts rise in response to parasitic infections [88]. In homozygous ɛ3/ɛ3 carriers, higher eosinophil counts were associated with poor performance on all cognitive tests [84]. Adults who possessed at least one ɛ4 allele (ɛ3/ɛ4 or ɛ4/ɛ4) and having high eosinophil counts indicating high levels of parasite infection demonstrated superior cognitive performance as compared with non-carriers. Despite similar environmental exposure to parasites, ɛ4 carriers had significantly lower eosinophil counts than did non-carriers.
The Tsimane are an indigenous tribe of the lowland Bolivian Amazon. Despite high levels of infection and inflammation, they do not tend to develop arterial aging and cardiovascular disease. A clinical evaluation of 983 Tsimané women reported that 70% were infected with the parasitic roundworm Ascaris lumbricoides, which is believed to increase fertility by suppressing the immune system [89]. In a previous study on the Tsimane [90], serum CRP levels were 60% higher in ɛ3/ɛ3 carriers than in ɛ4 carriers. These authors suggested that the elevated serum CRP levels indicate a higher parasite burden in the ɛ3 homozygotes [90]. Figure 1 summarizes some of the complex interactions among possession of the ɛ4 allele and the immune system.

Interaction of ɛ4 allele with the immune system.
SYSTEMIC INFLAMMATION IN POPULATIONS NOT INFECTED BY PARASITES IS RELATED TO APOE GENOTYPE (ɛ4 CARRIERS < ɛ3 CARRIERS < ɛ2 CARRIERS)
CRP is a ring-shaped (annular) protein synthesized in the liver and composed of five subunits (pentameric). CRP plasma concentration increases in response to inflammation [91]. CRP production is stimulated by IL-6 [92]. Hubacek et al. [93] analyzed data from a large population sample of randomly selected individuals from seven Czech towns. Their analysis included data on 2,886 males and 3,344 females from the HAPIEE (Health, Alcohol, and Psychosocial factors In Eastern Europe) study. In both males and females, the lowest levels of plasma high sensitivity CRP were measured in the carriers of the ɛ4/ɛ4 and ɛ4/ɛ3 genotypes. As expected, two-thirds of the study subjects were ɛ3/ɛ3, i.e., the most common genotype. In this group, the median (interquartile range, IQR) concentration of high sensitivity CRP was 1.13 mg/l (IQR, 0.56–2.33) in men and 1.23 mg/l (IQR, 0.61–2.65) in women. In carriers of the ɛ4 allele, the high sensitivity CRP level in males was 0.72 mg/l (IQR, 0.61–0.86) and 0.72 mg/l (IQR, 0.61–0.85) in females. The differences between the ɛ4 non-carrier and ɛ4 carrier groups were statistically significant (p < 0.001). Adjustment for age, sex, history of cardiovascular disease, or cardiovascular risk factors did not affect the result.
Kahri et al. [94] have also reported a statistically significant inverse relationship between possession of the ɛ4 allele and plasma high sensitivity CRP levels. This group measured the concentrations of serum high sensitivity CRP, soluble vascular cell adhesion molecule-1 (sVCAM-1), soluble intercellular adhesion molecule-1 (sICAM-1), and soluble E-selectin in 211 subjects from Finnish families with low high density lipoprotein (HDL) and in 157 normolipidemic subjects. Subjects carrying the ɛ4 allele in both the low-HDL subgroup (p < 0.05) and the normolipidemic subgroup (p < 0.01) had lower concentrations of serum high sensitivity CRP than subjects without the ɛ4 allele.
By conducting a large Korean study Yun et al. [95] validated that the inverse association between the ɛ4 allele and CRP was not limited to European populations. This group evaluated the association of the APOE genotype with serum CRP levels and white blood cell count in two large Korean population-based studies. The subjects analyzed were enrolled in the Dong-gu study and the Namwon Study. In the Dong-gu Study, 8,893 (3,525 men and 5,368 women) subjects ≥ aged 50 years from the Dong-gu district of Gwangju Metropolitan City in South Korea were evaluated. In the Namwon Study, 10,032 (3,909 men and 6,123 women) subjects from the Namwon city of Jeollabuk do province in South Korea were analyzed. The polymerase chain reaction-restriction fragment length polymorphism method was used to identify APOE genotypes. After adjusting for age, sex, body mass index, smoking, diabetes, hypertension, and serum lipids, multivariable linear regression analysis was performed to evaluate the relationships among APOE genotypes and CRP levels and white blood cell count. White blood cell count did not differ among APOE genotypes. In the Dong-gu Study, ɛ4 heterozygotes (ɛ3/ɛ4) and ɛ4 homozygotes (ɛ4/ɛ4) had significantly lower CRP levels as compared with the ɛ3/ɛ3 genotype, i.e., 0.50 mg/L versus 0.67 mg/L for the heterozygotes and 0.37 mg/L versus 0.67 mg/L for the homozygotes. In the Namwon Study, the ɛ4 heterozygotes and the ɛ4 homozygotes also had significantly lower CRP levels as compared with the ɛ3/ɛ3 genotype, i.e., 0.47 mg/L versus 0.66 mg/L for the heterozygotes and 0.45 mg/L versus 0.66 mg/L for the homozygotes.
CONCLUSIONS
The kinetics of the transition from the ubiquitous ancestral ɛ4/ɛ4 allelic distribution to the current 25.5% (23.5% % heterozygous; 2% homozygous) ɛ4 prevalence in primarily European derived populations is unknown [2]. There is consensus that humans first evolved in Africa, with recent evidence supporting the coincidental evolution of geographically subdivided populations across Africa [96, 97]. Modern humans diverged from pre-human hominins 260,000 to 350,000 years ago [98]. The most recent evidence suggests that the vast majority of modern humans living today are descended from a population that migrated from southern Africa to eastern Africa about 70,000 years ago, and then traveled beyond the continent from East Africa approximately 60,000 years ago [39]. At the time humans migrated from southern Africa to eastern Africa, the area was hot and humid as it is today [99].
A strong host innate immune response capable of killing bacteria soon after infection is advantageous for infant and early childhood survival via reduction in pathogen burden and associated immune responses. Despite lower baseline levels of inflammation, ɛ4 carriers display enhanced innate immune responses [48]. The robust innate immune response seen in extant pre-industrial populations provides a parsimonious explanation for the persistence of the ɛ4 allele (Fig. 2). A significant body of evidence suggests that an important normal function of the ɛ4 allele was to reduce the morbidity and mortality from enteric infections in infants and children among hunter-gatherer populations. From this perspective, the ancestral ɛ4 allele is not defective as compared with the now more common ɛ3 allele but is rather an adaptation to mankind’s ancestral high-pathogen environment, still experienced by selected tropical and arctic modern human populations.
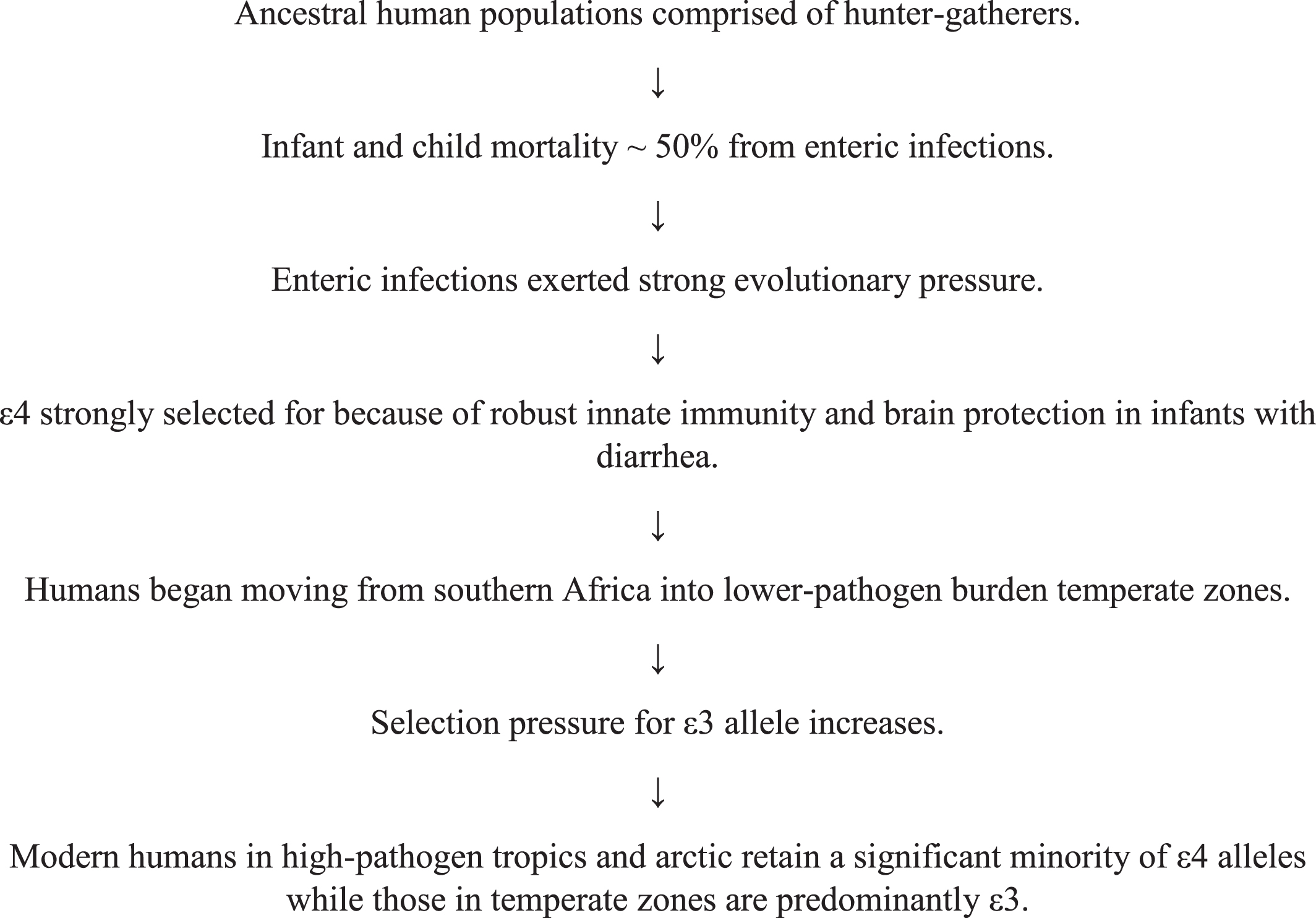
Persistence of the ɛ4 allele in high-pathogen environments.
Concomitantly, a major question is what is the factor explaining the success of the ɛ3 allele related to migration to temperate climates with a lower pathogen burden? While the advantage of the ɛ3 allele for lowering cardiovascular disease and AD in elderly individuals may be significant [4], this possibility needs further anthropological study, as additional factors might have also contributed to the rapid success of the ɛ3 allele [100], including unexplained burdens of the ɛ4 allele. The weight-of-the-evidence suggests that the ɛ4 allele represents a case of antagonistic pleiotropy wherein natural selection originally favored the allele because it increased fitness and fertility early in life, although ɛ4 increases the risk of AD later in life [4, 11, 101]. However, this primal allele may have yet other disadvantages in temperate climates and more recent human evolution. The more robust systemic inflammatory response in ɛ4 carriers is consistent with the observation that neuroinflammation might play a significant role in initiation or exacerbation of AD pathology. Further research on the possible relationship between systemic innate immunity and immune/inflammatory responses in the brain is warranted.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgements to report.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
J. Wesson Ashford is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
Carr J. Smith has no conflict of interest to report.