
Abstract
Specific sleep characteristics have been associated with cognitive decline, Alzheimer’s disease, and related dementias; however, studies examining the association between multidimensional sleep (a more comprehensive integration of sleep parameters) and cognitive decline are lacking. Among 2,811 older men without dementia, those with none, 1-2, and 3–5 “poor” self-reported sleep health dimensions had an adjusted 10-year change score of global cognition (3MS) of 2.9, 4.0 and 3.5 points (p-trend = 0.05), and in executive function (Trails B) completion time of 36.7, 42.7, and 46.7 seconds (p-trend < 0.01), respectively. In conclusion, a multidimensional measure of sleep health was associated with greater cognitive decline.
INTRODUCTION
Increasing evidence suggests that individual sleep disturbances evaluated objectively such as extreme sleep duration, poor sleep quality, and disrupted circadian rhythms are associated with poor cognition and risk of developing Alzheimer’s disease and related dementias in older adults [1–4]. However, objective assessment of sleep can be challenging and difficult to scale in large population studies, while self-reported measures have the advantage of being practical in real-world settings. Additionally, most studies have only looked at a global sleep score (ex. PSQI) or have focused on the effects of specific sleep characteristics or disorders, failing to capture the multidimensional nature of sleep [5]. To address this gap, the concept of “sleep health” has emerged, emphasizing multiple dimensions of sleep and their interrelationships to improve overall health and functioning [5]. A simple, and easily quantifiable, aggregate measure of self-reported sleep health has been developed, including characteristics representing sleep satisfaction, alertness, timing, efficiency, and duration [5], and has been shown to be closely related to health outcomes in older adults including physical functioning and frailty, depression, and mortality [6–9]. Among these studies, two have examined a gradient effect, and found that an increased number of poor sleep health dimensions (SHD) was associated with higher risk of depression and mortality [8, 9]. However, to our knowledge, no study has investigated the association between this multidimensional measure of sleep health and cognitive outcomes in older adults, and whether more poor SHD are related to a more significant cognitive decline remain unknown. Hence, in this study, we aimed to examine the longitudinal association between a multidimensional sleep health assessment and subsequent cognitive decline over 10–12 years in community-dwelling older men without dementia.
METHODS
In this original study, we examined men enrolled in an ancillary study to the Osteoporotic Fractures in Men Study (MrOS), the MrOS Sleep Study [10, 11]. Briefly, during the MrOS baseline examination (2000–2002), 5,994 community-dwelling men (≥65 years old) were recruited at six clinical centers in the United States. To participate, men needed to be able to walk without assistance and must not have had a bilateral hip replacement. Among them, 3,135 underwent a comprehensive sleep assessment between 2003 and 2005 (Sleep Visit 1). We excluded 188 men with incomplete data of significant cognitive impairment (Modified Mini-Mental State Examination (3MS) score < 80 or taking medication for dementia) at Sleep Visit 1, and 136 men lacking follow-up data, leading to a final sample of 2,811 participants with multiple cognitive assessments over 10–12 years (Supplementary Figure 1). All men provided written informed consent and the study was approved by the Institutional Review Board at each site.
Sleep characteristics over the past year were self-reported and were categorized as “good” or “poor” based on the five sleep dimensions of the Satisfaction, Alertness, Timing, Efficiency, and Duration (SATED) scale [5]. Poor Satisfaction was defined as getting fewer hours of sleep than needed to feel rested. Poor Alertness was assessed by excessive daytime sleepiness and was defined by the standard cutoff score of > 10 on the Epworth Sleepiness Scale [12, 13]. Poor Timing was assessed by mid-sleep time, which is calculated as the midpoint of the in-bed interval. Mid-sleep time was categorized based on octiles, and the first and eighth octiles were combined to define the “poor timing” dimension as extreme chronotypes have been linked to poor cognitive outcomes [14, 15]. Since efficiency was defined as the ease of falling asleep and returning to sleep, here we used sleep latency as a measure of efficiency. Poor Latency was defined as reporting taking 30 min or more to fall asleep. Participants who reported a sleep duration of < 7 h or > 8 h were classified as having a Poor Duration. A multidimensional measure of sleep health was derived by summing the number of “poor” dimensions, with total scores ranging from 0 to 5 and higher scores indicating poorer sleep health. The scores were categorized, according to the number of poor sleep health dimensions, into two categories (≥1 versus 0) and three categories (0, 1-2, 3–5) to decipher a potential dose-response effect.
Cognitive function was assessed using two cognitive tests administrated by trained staff: the 3MS and the Trail Making Test–Part B (Trails B). The 3MS is a global measurement of cognition, with components for orientation, concentration, language, praxis, and immediate and delayed memory. Scores range from 0 to 100, with higher scores representing better cognitive function [16]. Trails B is a timed test that measures attention, sequencing, visual scanning, and executive function [17]. Participants are given 300 s to complete the test, and higher completion times represent worse cognitive function. In addition to Sleep Visit 1, four repeated cognitive tests were implemented (n = 2,740 in 2005–2006, n = 2,489 in 2007–2009, n = 1,019 in 2009–2012, and n = 1,226 in 2014–2016).
Participants also completed examinations and questionnaires at Sleep Visit 1, including information about demographics, body mass index (BMI), smoking and alcohol use, physical activity [18], depressive symptoms [19], medical history, and medication use [20] (Supplementary Material).
Participant characteristics were first compared by presence of poor SHD using chi-square tests for categorical variables, t-tests for normally distributed continuous variables, and Wilcoxon rank sum tests for skewed continuous data. Random effects models were used to examine the association between multidimensional poor sleep health and change in cognitive function over the follow-up (Supplementary Material) [21]. Cube and log transformations were performed on 3MS and Trails B respectively to improve the normality of the distributions, and the results were back-transformed to the original scale. Covariates for model adjustment were selected based on potential biological plausibility. Models were minimally adjusted for age, race, and clinic site. These models were further adjusted by potentially confounding factors (education, BMI, smoking, alcohol use, physical activity, depressive symptoms, benzodiazepine or sleep medication use, history of diabetes mellitus, hypertension, stroke, cardiovascular disease, and Parkinson’s disease). Statistical tests were two-sided, and analyses were performed using SAS version 9.4 (SAS Institute Inc, Cary, NC).
RESULTS
Among the 2,811 participants (mean age, 76.0±5.3 years), 33.7% did not report any poor SHD, 54.5% reported 1 to 2 poor SHD, and 11.8% reported three or more poor SHD. Of the individual dimensions, 18.1% of the participants had Poor Satisfaction, 12.3% suffered from Poor Alertness, 24.6% had Poor Timing, 20.9% had Poor Latency, and 38.6% had Poor Duration. Men with at least one poor SHD were more likely to be nonwhite, to smoke and drink alcohol, had less education and physical activity, had higher BMI, and more depressive symptoms. They were also more likely to have a history of diabetes mellitus, stroke, and cardiovascular disease, and to take benzodiazepines and sleep medications (Table 1).
Baseline characteristics by presence of poor sleep health dimensions in older men (n = 2,811)
SD, standard deviation. *Cardiovascular disease includes myocardial infarction, angina, and congestive heart failure.
The mean 3MS score and Trails B completion time at the initial assessment were 93.6±5.5 points and 117.2±50.7 s, respectively. Men with at least one poor SHD had lower cognition (93.4±4.5 points and 119.9±52.3 s) compared to those without any (94.1±4.4 points and 111.9±47.1 s). Repeat cognitive tests were performed at up to 4 follow-up timepoints (Supplementary Figure 1). As estimated by the adjusted random effects models, over 10 years, 3MS score decreased by 3.9 points and Trails B completion time increased by 43.5 s for those with at least one poor SHD compared to those with none (2.9-points decrease and 36.8-s increase, respectively) (Table 2). Figure 1 shows estimated changes in 3MS and Trails B by number of poor SHD. The adjusted changes in 3MS scores were 2.9, 4.0 and 3.5 points (p-trend = 0.05), and in Trails B completion times were 36.7, 42.7, and 46.7 s (p-trend < 0.01), for those with none, 1-2, and 3-5 “poor” SHD, respectively. When individual SHD were examined, Poor Latency was associated with a decrease in 3MS score after multivariable adjustment (4.5-point and 3.3-point decrease for “poor” and “good” categories, respectively; Table 2), whereas Poor Timing was associated with an increase in Trails B completion time (48.7-s and 40.0-s increase for “poor” and “good” categories, respectively; Table 2).
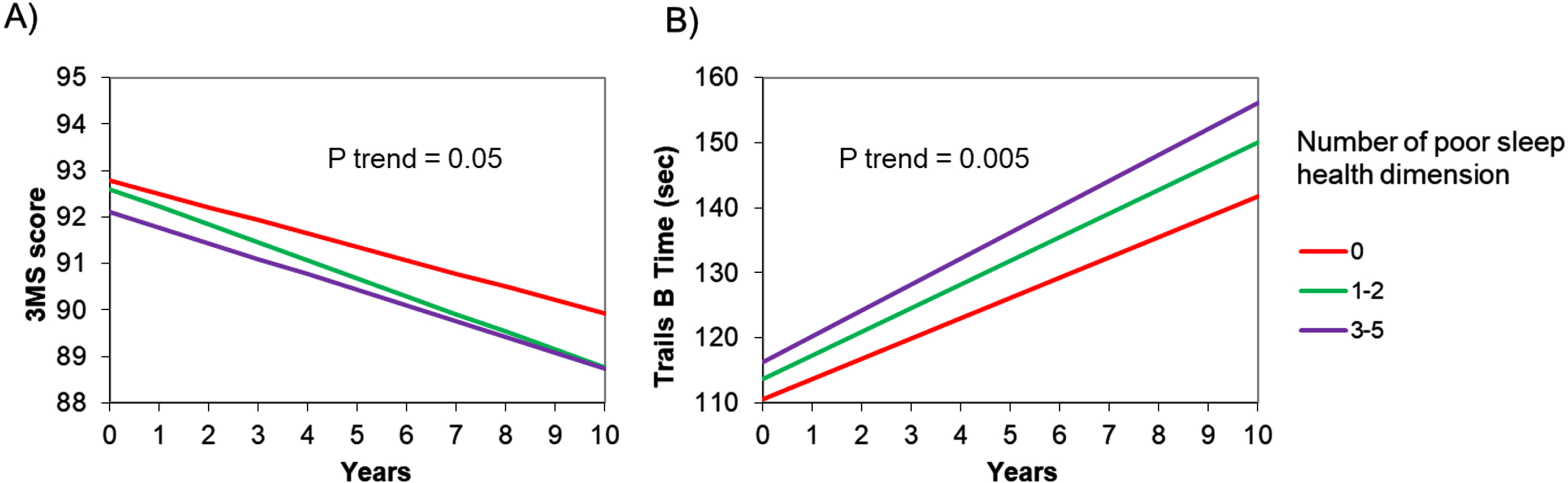
Changes in cognitive functions over 10 years by number of poor sleep health dimensions (n = 2,811). 3MS, Modified Mini-Mental State Examination; Trails B, Trail Making Test –Part B. Panel A represents the estimated change in 3MS score over 10 years by number of poor sleep health dimensions. Panel B represents the estimated change in Trails B test time over 10 years by number of poor sleep health dimensions. Adjusted for age, race, clinic site, education, body mass index, smoking, alcohol use, physical activity, depressive symptoms, benzodiazepine or sleep medication use, history of diabetes mellitus, hypertension, stroke, cardiovascular disease, and Parkinson’s disease.
Changes in cognitive test scores by multidimensional poor sleep health and its dimensions (n = 2,811)
3MS, Modified Mini-Mental State Examination; Trails B, Trail Making Test –Part B. p-value for the beta coefficient of sleep health predictor*time. Change in cognition is presented as average change per year, calculated using the coefficients derived from the random-effects models (beta coefficient for time + beta coefficient for sleep health predictor*time). Model 1: Adjusted for age, race, and clinic site. Model 2: Model 1 + education, body mass index, smoking, alcohol use, physical activity, depressive symptoms, benzodiazepine or sleep medication use, history of diabetes mellitus, hypertension, stroke, cardiovascular disease, and Parkinson’s disease.
DISCUSSION
Among older community-dwelling men without dementia, having a higher number of poor self-reported SHD was associated with greater cognitive decline, especially on executive function, after consideration of a number of potential confounders. Analyses of individual SHD suggested that Poor Latency was associated with a greater decline in global cognition, whereas Poor Timing was related to a greater decline in executive function.
Although no previous studies have investigated the relationship between multidimensional sleep health and cognitive aging, our results are consistent with prior literature linking multidimensional sleep health to adverse health outcomes such as physical impairment, depression, and mortality in community-dwelling older adults [6–9]. We contribute to the literature by showing that increment in the number of poor SHD is associated with greater cognitive decline over 10 years even after accounting for covariates. Our findings are also in line with other studies reporting associations between specific sleep characteristics and cognitive decline [22–24]. More precisely, we found that only Poor Latency was associated with global cognition when studying individual SHD. In the literature, mixed findings have been reported on the relationship between sleep latency and cognition [5, 25–29]. Our study highlights the importance of studying sleep latency together with other dimensions of sleep health. For executive function, an association was found with Poor Timing only, which corroborates a growing body of research suggesting circadian dysfunctions as markers of neurodegenerative diseases [30].
We found that the increased number of poor sleep health dimensions was a stronger predictor of decline in executive function than global cognition. This result is consistent with prior research showing that the prefrontal cortex area, an important structure for executive function [31], may be particularly vulnerable to sleep disturbances [32, 33]. Several biological mechanisms underlying the relationship between sleep and cognitive aging have been proposed. Indeed, poor sleep alters the clearance process via the glymphatic system, leading to the accumulation of amyloid-β which is implicated in the neurodegenerative process of Alzheimer’s disease [34]. It has also been linked with an increased risk of cardiovascular diseases and risk factors [35–37], all of which are known to be associated with an increased risk of cognitive decline and dementia [38, 39]. Finally, poor sleep could be an early marker of dementia, caused by the degeneration of neurons that promote wakefulness and sleep [40].
Overall, these results highlight the fact that considering individual SHD separately may underestimate the effects of sleep on cognition, reinforcing the importance of examining sleep in its multidimensional aspect. The SATED scale is a simple measure and easy to assess on a large scale, making it a promising tool at the population level to evaluate sleep health as an early marker of cognitive decline in late life. If poor multidimensional sleep health is confirmed to be a risk factor for dementia, interventions to improve sleep health may provide new opportunities for slowing down cognitive decline or reducing the risk of dementia in older adults.
Strengths of this study include a population of community-dwelling older men who were not selected based on sleep problems or cognitive function, its longitudinal design with a 10-year follow-up with high retention, a multidimensional measure of sleep health, and the consideration of a large number of possible confounders including information about demographics, lifestyle, comorbidities, and medication. Some limitations also need to be acknowledged. Generalizability of the results may be limited for women, non-White, and younger populations because this study involves mainly White older men. Sleep measures were self-reported which can lead to a lack of accuracy in responses; however, validated measures such as the Epworth Sleepiness Scale were used. The cognitive battery of tests was somewhat limited. Future longitudinal studies are needed to examine objective measures of multidimensional sleep health and cognitive decline in older adults. Finally, this is an observational study, and therefore causal relationship between multidimensional sleep health and cognitive decline cannot be assumed.
In summary, a multidimensional measure of sleep health was significantly associated with long-term decline in both global cognition and executive function among community-dwelling older men without dementia. Sleep health as a simple, self-reported measure might be a valuable risk marker of future cognitive decline in late life.
Footnotes
ACKNOWLEDGMENTS
The authors thank the study staff and all the men who participated in MrOS Sleep Study.
FUNDING
Y.L. is supported by National Institute on Aging (NIA) 1R00AG056598. K.Y. is supported in part by (NIA) R35AG071916. The MrOS Study is supported by National Institutes of Health funding. The following institutes provided support: the National Institute on Aging (NIA), the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), the National Center for Advancing Translational Sciences (NCATS), and NIH Roadmap for Medical Research under the following grant numbers: U01 AG027810, U01 AG042124, U01 AG042139, U01 AG042140, U01 AG042143, U01 AG042145, U01 AG042168, U01 AR066160, R01 AG066671, and UL1 TR002369). The National Heart, Lung, and Blood Institute (NHLBI) provided funding for the MrOS Sleep ancillary study “Outcomes of Sleep Disorders in Older Men” under the following grant numbers: R01 HL071194, R01 HL070848, R01 HL070847, R01 HL070842, R01 HL070841, R01 HL070837, R01 HL070838, and R01 HL070839.
CONFLICT OF INTEREST
Y.L is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.