
Abstract
Background:
Apolipoproteins and cortical morphology are closely associated with memory complaints, and both may contribute to the development of Alzheimer’s disease.
Objective:
To examine whether apolipoprotein B (ApoB), apolipoprotein A-1 (ApoA1), and their ratio (ApoB/ApoA1) are associated with cortical morphology in patients with memory complaints.
Methods:
Ninety-seven patients underwent neuropsychological testing, measurements of ApoB, ApoA1, ApoB/ApoA1, plasma Alzheimer’s biomarker, apolipoprotein E (ApoE) genotyping, and 3T structural magnetic resonance imaging (sMRI) scans. Based on sMRI scanning locations, patients were categorized into the University of Electronic Science and Technology (UESTC) and the Fourth People’s Hospital of Chengdu (FPHC). The Computational Anatomy Toolbox within Statistical Parametric Mapping was used to calculate each patient’s cortical morphology index based on sMRI data. The cortical morphology index and apolipoproteins were also analyzed.
Results:
Significant positive correlations were found between ApoB and sulcal depth in the lateral occipital cortex among the UESTC, the FPHC, and the total sample groups, and negative correlations were observed between sulcal depth in the lateral occipital cortex and the scores of the Shape Trails Test Part A and B. In the FPHC group, the scores of the Montreal Cognitive Assessment Basic, delayed recall of the Auditory Verbal Learning Test, Animal Fluency Test and Boston Naming Test were positively correlated with the sulcal depth.
Conclusions:
ApoB is associated with the sulcal depth in the lateral occipital cortex, potentially relating to speed/executive function in individuals with memory complaints.
INTRODUCTION
Alzheimer’s disease (AD) is a progressive neurodegenerative disorder that encompasses six clinical stages, including subjective cognitive decline (SCD) and mild cognitive impairment (MCI) as stages two and three, respectively. 1 Patients with SCD perceive cognitive decline without demonstrating objective, measurable cognitive impairment. 2 This phenomenon occurs in the preclinical stage of AD. 3 Conversely, individuals with MCI exhibit noticeable cognitive impairment, though their activities of daily living remain relatively unaffected.4,5, 4,5 Memory complaints, prevalent in the general population, often precede observable reduction in cognitive abilities and augment the risk of developing AD.3,6, 3,6 Consequently, identifying reliable biomarkers and indicators in patients expressing memory complaints is imperative for the timely diagnosis, prevention, and treatment of AD.
Lower plasma levels of amyloid-β 42 (Aβ42) and 40 (Aβ40) are predictive of dementia,7–9 and plasma Aβ42/Aβ40 ratios are correlated with prospective cognitive decline. 10 Additionally, plasma AD biomarkers, such as phosphorylated tau (p-tau) and neurofilament light chain (NfL), can predict cognitive decline and brain atrophy.11–14 Among apolipoproteins, apolipoprotein B (ApoB), apolipoprotein A-1 (ApoA1), and their ratio (ApoB/ApoA1) are reportedly closely related to cognitive function deterioration and may influence the etiology of MCI and AD.15,16, 15,16 For instance, a recent study demonstrated that cerebrospinal fluid ApoB increased in AD and correlated with t-tau and p-tau in pre-symptomatic individuals. 17 Prior research suggested that serum ApoB could have a protective effect in the preclinical stage of AD and possibly serve as a potential blood biomarker in patients with memory complaints. 18 Moreover, another study found that the top quartile of ApoB and ApoB/ApoA1 values was linked to a higher risk of dementia, while that of ApoA1 was associated with a lower risk. 19 Overexpression of ApoA1 has been shown to effectively suppress age-induced decline in memory and learning abilities. 20 Serum ApoB levels have been found to be significantly elevated in patients with AD. 20 Furthermore, the ApoB/ApoA1 ratio can reflect not only the balance of liver cholesterol transport but also the balance between atherogenic particles and anti-atherosclerotic particles, thus serving as a precise index for assessing lipid metabolism disorders. 21 Research indicates that ApoB/ApoA1 and ApoB values are linked to ischemic myocardial disease, and the accelerated cognitive decline related to ApoB may be associated with atherothrombotic characteristics, microvascular dysfunction and subsequent hypoperfusion of ischemic clinical or subclinical cerebrovascular disease,21,22, 21,22 showing that ApoB may act as an intermediate factor in accelerating cognitive decline and ensuing dementia. 23 Together, these findings suggest that the examination of atherogenic lipoproteins, such as ApoA1 and ApoB, and the ratio of ApoB/ApoA1, has significant relevance in the study, auxiliary treatment, and diagnosis of cognitive disorders and overall cognitive health.
Cortical thickness, assessed through T1-weighted structural magnetic resonance imaging (sMRI), is a valuable biomarker for predicting or facilitating early dementia diagnosis. Initial years of clinical symptom onset may witness detectable reductions in cortical thickness. 24 Prior studies have indicated significant thinning in the anterior cingulate and superior temporal regions compared to other brain areas in patients with MCI, 25 with a notable decrease also observed in the left lateral occipital domain. 26 Sulcal depth significantly decreases with age. 27 It emerges as a promising metric for early AD detection, demonstrating significant variation between patients with mild and severe disease, suggesting its potential as a crucial indicator of disease severity. 28 Research has identified significant differences in the parietal-occipital fissure and intraparietal sulcal regions as individuals progress from HC to MCI to AD; moreover, patients with posterior cortical atrophy exhibited more pronounced parieto-occipital sulcal widening than typical AD.29,30, 29,30 In both MCI and AD, the sulcal depth decreases during disease progression from healthy individuals to MCI and from MCI to AD.31,32, 31,32 Furthermore, research has revealed that individuals with AD presented an increased degree of folding of the insular cortex, which is specifically linked to improved memory function and semantic fluency. 33 In individuals with subjective cognitive complaints, the entorhinal and the para-hippocampal gyrus were associated with higher memory complaint scores. 34 Language was related to the temporal regions and the supramarginal gyrus sulcal depth, executive function was correlated with the medial temporal gyrus and supramarginal gyrus sulcal depth, 35 and a significant correlation between processing speed and superior temporal sulcus was observed in older adults. 28
The abovementioned morphological indices contribute valuable insights into neuroanatomical research on individuals with memory complaints. Furthermore, a study showed that ApoB negatively correlates with occipital periventricular hyperintensity. 36 Lower grey matter and cortical volume reductions have been found to be associated with a larger percentage increase in ApoA1 levels. 37 However, to the best of our knowledge, few studies have combined ApoB, ApoA1, ApoB/ApoA1, plasma AD biomarkers, cortical surface morphology, and cognitive performance analyses in individuals with memory complaints.
Therefore, this study examined whether the determination of the plasma ApoB, ApoA1, the ratio ApoB/ApoA1 is cognitively and neurologically correlated with memory complaints patients. Considering the impact of these neurological and cognitive functions, we hypothesized that plasma apolipoprotein levels are associated with surface morphometry and cortical morphology are correlated with cognitive performance or plasma AD biomarkers in patients with memory complaints.
MATERIALS AND METHODS
Participants
Ninety-seven participants reporting memory complaints, including SCD and MCI, were included in this study. 38 They underwent sMRI scans in the University of Electronic Science and Technology in Chengdu (UESTC, 42 patients) or in the Fourth People’s Hospital of Chengdu (FPHC, 55 patients). All participants voluntarily participated in standardized clinical assessments and physical examinations, none of them had previously received intervention. They underwent history taking, blood sampling and serial neuropsychological assessments. The inclusion criteria were as follows: 1) right-handedness; 2) no medication for hyperlipidemia diseases; 3) no contraindications for MRI; 4) the identification of SCD followed a specialized diagnostic framework 3 as follows: i) individuals reporting continuous subjective cognitive decline rather than other domains of cognition for at least 6 months, activities of daily living were not restricted and were not associated with acute events; ii) none showed displaying objective cognitive impairment or met the criteria for MCI or dementia; iii) individuals expressed SCD-related concerns and felt worse than their peers through structured interviews with physicians; iv) cognitive decline confirmed by another informant; 5) MCI was identified using the Jak/Bondi criterion 39 as follows: i) necessitated individuals to have at least two impaired test scores in one cognitive domain (memory, language, or speed/executive function) falling more than one standard deviation below the age-adjusted normative mean; ii) impaired scores one standard deviation below the age-adjusted standardized mean in each of the three cognitive domains.
Exclusion criteria were as follows: 1) major depressive disorder, bipolar disorder, schizophrenia, or other psychiatric disorders; 2) other nervous system diseases that cause cognitive decline (such as cerebrovascular disease, cerebral infarction, brain tumor, Parkinson’s disease, encephalitis or epilepsy); 3) other diseases that may lead to cognitive decline (such as thyroid dysfunction, severe anemia, syphilis or HIV); 4) any other systemic illness or uncertainty that prevented the completion of the project.
The use of lipid-lowering agents may be associated with a reduced risk of dementia in individuals aged <80 years. 40 As our participants were in a subclinical healthy stage and the average level of apolipoprotein was within the clinically normal range, we examined the absence of any use of hyperlipidemic drugs. Demographics, clinical information, and biomarkers are listed in Table 1, and chi-square test, independent samples t-test and Kolmogorov-Smirnov test were performed to assess the differences between the UESTC and FPHC groups. This study was approved by the Ethics Committee of the Fourth People’s Hospital of Chengdu, and written informed consent was obtained from all participants. Figure 1 presents the overall research flow.
Demographic, clinical information and biomarkers
Analysis of differences between UESTC and FPHC groups, ◊Chi-Square test, # Independent samples t-test, others use the Kolmogorov-Smirnov test, *p < 0.05, **p < 0.0001. Selected demographic data of the study participants are presented as mean±standard deviation or n (%). UESTC, the University of Electronic Science and Technology in Chengdu; FPHC, the Fourth People’s Hospital of Chengdu; SCD, MCI (%), Subjective cognitive decline, Mild cognitive impairment (%); MRI scanners, magnetic resonance imaging scanners; MMSE, Mini-Mental State Examination; MoCA-B, Montreal Cognitive Assessment-Basic; AVLT-DR, Auditory Verbal Learning Test, Delayed Recall; STT-A/STT-B, The Shape Trail Test Part A or B; AFT, Animal Fluency Test; BNT, Boston Naming Test; Aβ40, amyloid β-protein 40; Aβ42/Aβ40, amyloid β-protein 42/40; Tau, tau protein; p-tau181, phosphorylated tau181; NfL, neurofilament light chain.
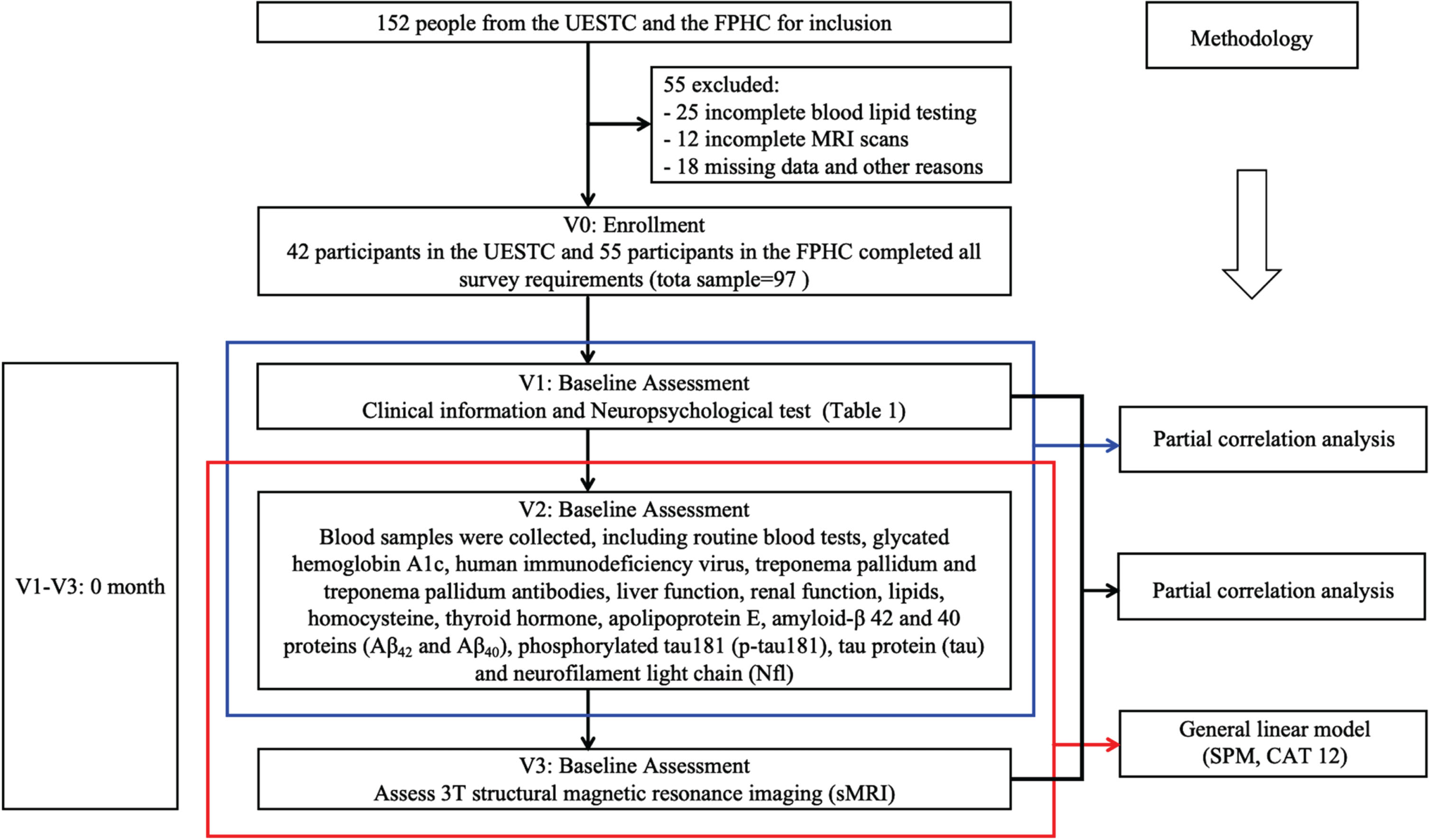
Flowchart of the overall research. V0: V1: Initial visit. V2: Second visit. V3: Third visit.
Neuropsychological assessment
Cognitive function was evaluated using a set of neuropsychological clinical tests. 38 The tests, including the Mini-Mental State Examination (MMSE), the Montreal Cognitive Assessment Basic (MoCA-B), the Auditory Verbal Learning Test (AVLT), the Animal Fluency Test (AFT), the Boston Naming Test (BNT), and the Shape Trail Test A (STT-A) and B (STT-B), assessed memory, language, and speed/executive functions to gauge symptoms in participants reporting memory complaints. Results are summarized in Table 1.
ApoB, ApoA1, ApoB/ApoA1 measurement
Participants were instructed to fast for at least 8 hours preceding blood sampling. Whole blood was collected in a non-heparinized anticoagulant tube, with a minimum of 400 microliters promptly transferred to the testing laboratory. In instances of delay, samples were refrigerated at 4°C and tested within one week to circumvent repeated freezing. For the UESTC group, fasting venous serum samples were procured, and ApoB levels were measured using an Atellica IM1600 analyzer (Siemens Healthineers, Erlangen, Germany). 38 The minimum detection concentration for ApoB was 0.43 mg/ml. The FPHC group utilized an AU680 automatic biochemical analyzer to measure ApoB levels; the lowest detection concentration was 0.16 mg/ml. Apart from ApoB measurement, ApoA1 levels were also assessed, with minimum detection concentrations of 1.01 mg/ml and 0.89 mg/ml for the UESTC and FPHC groups, respectively.
APOE genotyping measurement
Blood samples for ApoE genotyping were preserved at –80°C using ethylenediaminetetraacetic acid as an anticoagulant to avoid repeated freezing and thawing. The ApoE genotyping analysis was conducted at Zhuhai Sinochips Bioscience Co., Ltd., Guangdong, China. The ApoE genotype detection kit implemented polymerase chain reaction (PCR) to amplify specific gene fragments, targeting two ApoE polymorphism sites (codons 112 and 158). The PCR procedure involved initial denaturation at 95°C for 15 min, followed by 45 cycles of amplification at 94°C for 30 s and 65°C for 45 s. The PCR products were subsequently hybridized into a gene chip, and the data were analyzed using a microarray reporting system.
Plasma biomarkers of AD
Plasma samples were preserved at –80°C before testing and analysis to avoid repeated freeze-thaw cycles. Preparation involved fully thawing the EDTA plasma sample, placing it on ice, thoroughly mixing it, and subjecting it to 10000 cycles× g. Plasma components were transported to Hangzhou G-Bio Biotechnology Co., Ltd. on dry ice. The Simoa HD-X platform (Quanterix Company, USA) was used to perform the automated analysis of plasma Aβ42, Aβ40, total tau, and NfL according to the instrument and reagent kit instructions. Board-certified investigators blinded to the clinical data executed all measurements.
MRI data acquisition
Participants were instructed to relax, close their eyes, lie flat, and minimize head and body movements. Foam pads and earplugs were used to reduce scanner noise and motion artifacts. For the UESTC group, a GE 3.0T MR750 scanner captured high-resolution three-dimensional (3D) T1-weighted MRI images with MRI parameters as previously described: 38 repetition time (TR) = 5.956 ms, echo time (TE) = 1.964 ms, inversion time (TI) = 450 ms, flip angle = 9°, the field of view (FOV) = 256×256 mm2, slice thickness = 1.0 mm, voxel size = 1×1×1 mm3, and scan time = 239 s. For the FPHC group, high-resolution three-dimensional sagittal T1-weighted images of the entire brain were obtained using a Siemens Skyra 3.0 T (MAGNETOM) MR brain 32-channel phased array coil. The scanning parameters were as follows: TR = 2,300 ms, TE = 2.32 ms, field of view = 224 mm×224 mm, matrix = 240×240, and layer thickness = 0.9 mm.
Surface-based morphometry analysis
The images were preprocessed using the Computational Anatomy Toolbox 12 software 41 (CAT12, http://www.neuro.unijena.de/cat/, version 12.8) in conjunction with Statistical Parametric Mapping 12 (SPM12, http://www.fil.ion.ucl.ac.uk/spm/software/spm12/, version 7771) running on MATLAB (R2014a). The CAT12 toolbox contains a processing pipeline for surface-based morphometry (SBM), which includes established new algorithms for extracting geometric surfaces, 42 allowing for the calculation of multiple morphological measures, including cortical thickness and sulcal depth.
All DICOM images were converted to the NifTI format, visually inspected for motion or other artifacts using MRIcron software (http://people.cas.sc.edu/rorden/mricron/index.html), and preprocessed with bias-field inhomogeneity correction. The CAT12 toolbox then uses tissue segmentation to estimate grey matter, white matter, and cerebrospinal fluid on T1-weighted images. The adjacency relationship described by white matter distance is then used to project the local extremum to other gray matter voxels, the values are equivalent to cortical thickness values. This method also includes partial volume correction, sulcal blurring, and assessment of sulcal asymmetry without the need for reconstructed sulcal. 42 Topological corrections are formed through spherical harmonics. Interparticipant analyses included algorithms for spherical mapping of cortical surfaces. 43 Then, DARTEL algorithm was applied diffeomorphic anatomical registration to the spherical registration surface for normalization. 44 The CAT12 toolbox was used to estimate cortical thickness and sulcal data. 42 In addition to cortical thickness indices, local sulcal depth indices were extracted based on absolute mean curvature, 45 which was calculated based on the Euclidean distance between the central surface of the cortex and its convex hull. 46 The central cortical surface were created respectively for two hemispheres. Finally, cortical thickness and sulcal depth were separately resampled and smoothed using a Gaussian kernel with half-maximum widths of 15 and 20 mm, respectively.
Statistical analyses
Correlation analysis between ApoB, ApoA1, ApoB/ApoA1, plasma AD biomarkers and cognitive performance
Using the IBM ® SPSS ® 27.0., we performed partial correlation analysis in which the correlation between ApoB, ApoA1, ApoB/ApoA1, plasma AD biomarkers and cognitive performance subtests was evaluated while controlling for age, sex, education, and ApoE (Supplementary Tables 1 and 2).
Neuroimaging statistical analysis
Vertex-based analysis of ApoB, ApoA1, ApoB/ApoA1 related maps of sulcal depth and cortical thickness were conducted separately for the three groups using the general linear model approach implemented in SPM12, using age, sex, education, and ApoE as covariates. In the total sample group, the difference in MRI scanners (“UESTC = 1, FPHC = 2”) was added as a covariate to account for the difference in MRI scanners. There were 6 models in the total sample, 6 models in the UESTC, 6 models in the FPHC, 18 models in the three groups. The independent variables of each model were ApoB, ApoA1 and ApoB/ApoA1, the predictive factors were sulcal depth and cortical thickness, and the covariates were age, sex, education, and ApoE (the total sample: age, sex, education, ApoE and MRI scanners). For plasma biomarkers of AD, we also performed general linear model each correlating plasma biomarkers of AD with cortical thickness and sulcal depth, respectively (Supplementary Tables 3 and 4). Then, biomarkers that were significantly associated with sulcal depth and cortical thickness were included as covariates in the model of ApoB, ApoA1, and ApoB/ApoA1 with sulcal depth and cortical thickness in the three groups to be analyzed again, to eliminate possible influence of biomarkers on the results (Supplementary Tables 5 and 6). We used threshold-free cluster enhancement (TFCE) 47 with 100 permutations to identify the cluster significance that were significantly associated with ApoB, ApoA1, ApoB/ApoA1, plasma AD biomarkers at p < 0.05 after correcting for multiple comparisons across space using Family-wise error (FWE) correction. The anatomical locations of the significant clusters were determined with reference to the multi-modal analyses of sMRI images from the HCP multimodal parcellation (HCP MMP 1.0) cortical atlas. 48 We used the age to group the sulcal depth values of three groups of people (5-year group) and took the average sulcal depth values of each group for heterogeneity analysis. The results showed few heterogeneity problems among the three groups (Supplementary Figure 1).
Correlation analysis between cortical shape index and cognitive performance
For each region of interest, the HCP multimodal parcellation (HCP MMP 1.0 cortical atlas) 48 was used to extract the values of average thickness or sulcal depth from the surface meshes for the subregions, respectively, which were significant with ApoB, ApoA1, or ApoB/ApoA1 at the vertex level. Then, using the IBM ® SPSS ® 27.0., partial correlation analysis was performed between values for sulcal depth or cortical thickness from the surface meshes in sub-regions and cognitive performance, respectively. In the UESTC and FPHC groups, ApoE, age, sex, and education were accounted for as covariates, while in the total sample group, MRI scanners (“UESTC = 1, FPHC = 2”), ApoE, age, sex, and education were included as nuisance factors. Statistical significance was set at p < 0.05.
RESULTS
ApoB, ApoA1, ApoB/ApoA1 and cortical shapes
Significant positive correlations were found between ApoB and the sulcal depth of the left lateral occipital cortex in the total sample group (p < 0.0001) (Fig. 2A). A significant positive correlation was also observed between ApoB and the sulcal depth of the left lateral occipital cortex in the UESTC group (p < 0.0001) (Fig. 2B) at corrected thresholds p < 0.05 (TFCE, FWE-corrected). At uncorrected thresholds p < 0.003 (TFCE, uncorrected), a significant positive correlation was found between ApoB and the sulcal depth of the right lateral occipital cortex in the FPHC group (p = 0.001) (Fig. 2C). A summary of these findings is presented in Tables 2–4. However, no significant relationships were discovered between ApoA1, ApoB/ApoA1, and sulcal depth, or between any of the apolipoproteins and cortical thickness in any group.
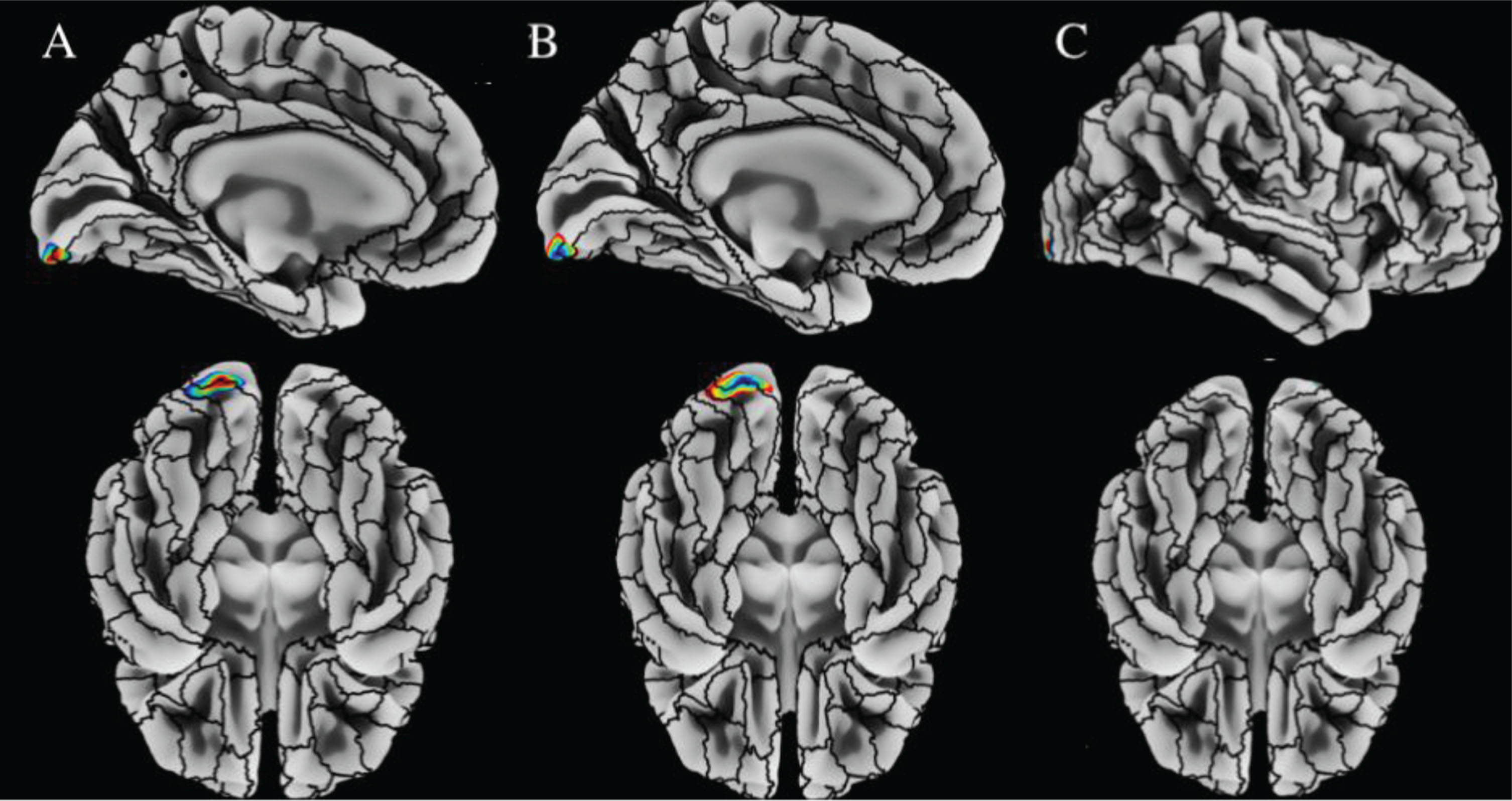
A) Positive correlations between ApoB and sulcal depth values in the left lateral occipital based on vertex-based analyses in the total sample group. The whole brain’s underlay used sulcal depth, and the atlas border used overlay HCP Multi-Modal Parcellation. The threshold was set at p < 0.05 (TFCE, FWE-corrected), controlling for age, sex, education, ApoE, and MRI scanners. B) Positive correlations between ApoB and sulcal depth values in the left lateral occipital based on vertex-based analyses in the UESTC group. The whole brain’s underlay used sulcal depth, and the atlas border used overlay HCP Multi-Modal Parcellation. The threshold was set at p < 0.05 (TFCE, FWE-corrected), controlling for age, sex, education and ApoE. C) Positive correlations between ApoB and sulcal depth values in the right lateral occipital based on vertex-based analyses in the FPHC group. The whole brain’s underlay used sulcal depth, and the atlas border used overlay HCP Multi-Modal Parcellation. The threshold was set at p < 0.003 (TFCE, uncorrected), controlling for age, sex, education, and ApoE. Significant regions are identified using SBM, which was projected onto the left and right lateral surfaces of the standard central brain. Tables 2–4 provide details on the regions. No significant correlations were observed for ApoA1 and ApoB/ApoA1 levels.
The positive correlation of sulcal depth in the left lateral occipital cortex and ApoB in the total sample group
Overview of significant positive correlation of sulcal depth in the left lateral occipital cortex and ApoB in total sample group of 97 cases of memory complaints. Atlas labeling was performed according to the HCP Multi-Modal Parcellation atlas. 48 The threshold was set at p < 0.05 (TFCE, FWE-corrected), controlling for age, sex, education, ApoE and MRI scanners. T values (p < 0.05, FWE-corrected at peak level). V1, V2, and V3: lateral occipital.
The positive correlation of sulcal depth in the left lateral occipital cortex and ApoB in the UESTC group
Overview of significant positive correlation of sulcal depth in the left lateral occipital cortex and ApoB in the UESTC group of 42 cases of memory complaints. Atlas labeling was performed according to the HCP Multi-Modal Parcellation atlas. 48 The threshold was set at p < 0.05 (TFCE, FWE-corrected), controlling for age, sex, education and ApoE. T values (p < 0.05, FWE-corrected at peak level). V1, V2, and V3: lateral occipital.
The positive correlation of sulcal depth in the right lateral occipital cortex and ApoB in the FPHC group
Overview of significant positive correlation of sulcal depth in the right lateral occipital cortex and ApoB in the FPHC group of 55 cases of memory complaints. Atlas labeling was performed according to the HCP Multi-Modal Parcellation atlas. 48 The threshold was set at p < 0.003 (TFCE, uncorrected), controlling for age, sex, education and ApoE. T values (p < 0.003, uncorrected at peak level). V1: lateral occipital, V2: middle temporal.
Cognitive performance and the sulcal depth index
According to the HCP MMP 1.0 atlas, the mean sulcal depth of the lateral occipital region was negatively associated with STT-A and STT-B in the total sample group, the UESTC group, and the FPHC group, respectively (β= –0.364, p < 0.0001; β= –0.364, p = 0.024; β= –0.395, p = 0.005 for STT-A and β= –0.259, p = 0.013; β= –0.329, p = 0.044; β= –0.430, p = 0.002 for STT-B) (Fig. 3A, B).

A) A significant negative correlation exists between the sulcal depth of the lateral occipital and STT-A(s) across all groups. B) A significant negative correlation exists between the sulcal depth of the lateral occipital and STT-B(s) across all groups. These results were complemented by an examination of the whole lateral occipital using the HCP Multi-Modal Parcellation atlas parcellation. The total sample group was adjusted for baseline age, education, sex, ApoE, and MRI scanners. The UESTC and FPHC groups were adjusted for baseline age, education, sex, and ApoE, p < 0.05.
In the FPHC group, the sulcal depth in the lateral occipital cortex was positively correlated with the MoCA-B (β= 0.343, p = 0.017), AVLT-DR (β= 0.291, p = 0.045), AFT (β= 0.405, p = 0.004), and BNT (β= 0.408, p = 0.004). The results are summarized in Table 5. However, we found no significant relationship between other cognitive performance metrics and sulcal depth or cortical thickness.
The associations between sulcal depth of lateral occipital and cognitions in three groups
*p < 0.05, **p < 0.0001. Partial correlation analysis was used to assess the differences in cognitions between the total sample group, the UESTC group and the FPHC group. The total sample group was adjusted for baseline age, education, sex, ApoE, and MRI scanners. The UESTC and FPHC groups were adjusted for baseline age, education, sex, and ApoE. UESTC, the University of Electronic Science and Technology in Chengdu; FPHC, the Fourth People’s Hospital of Chengdu; MMSE, Mini-Mental State Examination; MoCA-B, Montreal Cognitive Assessment-Basic; AVLT-DR, Auditory Verbal Learning Test, Delayed Recall; STT_A/STT_B, The Shape Trail Test Part A or B; AFT, Animal Fluency Test; BNT, Boston Naming Test.
DISCUSSION
To the best of our knowledge, this study is the first to explore the relationship between ApoB, ApoA1, ApoB/ApoA1, plasma AD biomarkers and cortical morphology. The result revealed that ApoB was positively associated with sulcal depth in the lateral occipital cortex and independent of the association with biomarkers. Furthermore, a negative correlation between the sulcal depth of the lateral occipital area and STT-A and STT-B scores was observed in all groups, suggesting a positive relationship between ApoB and sulcal depth of the lateral occipital cortex in individuals with memory complaints and that sulcal depth in this area correlates positively with speed/executive function.
ApoB-related surface shapes in participants with memory complaints
Recently, there has been growing evidence of cognitive ability in individuals with memory complaints, particularly with ApoB levels.15,19, 15,19 Additionally, research has indicated that plasma ApoB levels were suggestive of atherogenic potential and atherosclerotic changes. 18 A Mendelian randomization study suggested ApoB as the main characteristic connecting lipoprotein to heart disease and stroke risk. 49 The well-documented connection between cardiovascular risk factors and faster AD conversion, 22 along with the dysregulation of ApoB homeostasis and its relation to AD, further reinforces ApoB level as an early AD risk factor. Interestingly, the cognition tied to ApoB might be associated with atherothrombotic traits and microvascular dysfunction. 15
Our study revealed a positive correlation between ApoB levels and sulcal depth in the lateral occipital region in individuals with memory complaints. This indicates that ApoB may be associated with atherothrombotic traits and cortical structure (Tables 2–4) in the memory complaints population. ApoB in cerebrospinal fluid samples has emerged as a valuable marker for pathological cognition, highlighting the importance of considering apolipoproteins in clinical practice. 17 Grey matter atrophy in the left precentral gyrus and left insular cortex of patients with occipital periventricular hyperintensity is reportedly associated with ApoB levels. 50 Moreover, grey matter and cortical volume were associated with ApoA1 levels. 37 However, data on the association between sulcal depth and ApoB levels in individuals with memory complaints remain lacking. Studies have reported that cortical thickness is negatively correlated with plasma concentrations of Aβ40, Aβ42, and p-tau. 51 Higher tau levels were associated with greater cortical thickness changes in AD patients with higher genomewide polygenic risk scores. 52 Moreover, cerebrospinal fluid Aβ, tau, and p-tau have different correlations with cortical thickness and brain structural atrophy in preclinical AD patients.53,54, 53,54 In our research, Aβ42/Aβ40 and ptau-181 were positively associated with sulcal depth in the left temporal cortex and the left frontal cortex, respectively. No significant correlations were found between plasma biomarkers of AD and sulcal depth and cortical thickness in the UESTC group. Moreover, Aβ42/Aβ40 and ptau-181 were not significant for the correlation between ApoB and sulcal depth in the lateral occipital cortex. Sulcal depth is known to be affected by age, sex, and ApoE.27,55,56, 27,55,56 Nevertheless, our study results are less likely to be attributed to variations in age, sex, and ApoE, as we meticulously controlled for these variables in our analyses. Consequently, we posit that the sulcal depth within the lateral occipital cortex in individuals with memory complaints may be associated with ApoB levels.
Previous studies on the relationship between ApoA1 and AD have yielded modest and conflicting results.57,58, 57,58 In the present study, no association was observed between ApoA1 or ApoB/ApoA1 and sulcal depth and cortical thickness in patients with memory complaints. It is beneficial to explore the interaction of ApoA1 and ApoB/ApoA1 with other binding partners to elucidate their roles in AD and related diseases. 59
ApoB-related sulcal depth of lateral occipital cortex and cognitive function
Previous research has established that ApoB, a protein associated with cerebrovascular diseases, 22 may accelerate cognitive decline and subsequent dementia. 23 ApoB linked with atherothrombosis, and ischemic diseases of large and small vessels were associated with cognition, even in AD.15,60, 15,60 Furthermore, changes in cognitive function in older adults have been found to positively correlate with the complexity of cerebral sulcal folds. 61 Studies have revealed that individuals with AD exhibit an elevated degree of folding in the insular cortex, which is specifically linked to improved memory function and enhanced semantic fluency. 33 Language and executive function were correlated with the sulcal depth in the temporal region, medial temporal gyrus and supramarginal gyrus, 35 and processing speed was correlated with superior temporal sulcal in older adults. 28 Our study detected a subtle positive association between the sulcal depth of the lateral occipital cortex and ApoB (Tables 2–4). The sulcal depth of the lateral occipital cortex positively correlates with speed/executive function in individuals with memory complaints. In the FPHC group, the sulcal depth of the lateral occipital cortex is positively correlated with global cognitive function, delayed recall function and language function (Table 5).
Previous research findings have demonstrated a positive relationship between sulcal depth in the left cap and cognitive function in Parkinson’s disease. 62 Sulcal morphology in specific regions is significantly positively correlated with most cognitive domains in older adults, including attention, language, and executive function. 28 The sulcal curvature and depth of MCI or AD patients are smaller than those of healthy individuals, 31 and sulcal depth in the temporal and frontal lobes was positively correlated with executive and language function in older adults with memory complaints. 28 In individuals with mild AD, a decline in MMSE scores was observed in conjunction with an increase in the width of all individual sulcal depths studied, except for the intraparietal sulcal depth. 63 In our study, we found the sulcal depth of the lateral occipital cortex was positively associated with speed/executive function in memory complaints individuals. Based on these findings, we proposed a positive correlation between ApoB and sulcal depth in the lateral occipital region, and sulcal depth was positively related with speed/executive function in individuals with memory complaints.
The lateral occipital cortex, a critical area for visual processing, plays pivotal roles in visuospatial processing, distance and depth perception, color determination, and executive function. Additionally, it participates in scene perception and context analysis.64,65, 64,65 Consequently, disturbances in occipital signaling have been associated with cognitive deficits and intellectual disability. 66 Liu et al. suggested a negative correlation between sulcal morphology in the left superior temporal sulcus and executive function in older individuals. 28 Furthermore, compelling evidence demonstrates a positive correlation between the complexity of cerebral sulcal folds and various cognitive domains, including processing speed, language, and executive function. 61 Our study demonstrated that speed/executive function in patients with memory complaints may be linked to sulcal depth in the lateral occipital cortex. As the severity of AD escalates, the overall sulcal index seems to decrease. 67 Moreover, the connection between cognitive functions, apolipoproteins, and cortical morphology may be influenced by genetic factors. Indeed, ApoE ɛ4 carriers exhibit age-related structural-functional associations and may rely on the integrity of multiple compensatory brain systems to maintain their cognitive abilities.68,69, 68,69 Therefore, we added ApoE as a covariate to eliminate its effect in the analysis of cortical morphology in the three groups.
Nevertheless, through the analysis of the cortical thickness and cognitive function, we have not found a connection, although a cross-sectional study of older adults with subjective cognitive impairment and MCI proposed that occipital cortex thinning is related to memory impairment. 24 This inconsistency in findings could stem from the fact that cortical thickness measurements tend to reflect the later stages of the disease, 70 and sulcal depth may be a more sensitive measure for detecting imminent brain changes that lead to objective cognitive dysfunction. 62 Moreover, we found the plasma AD biomarkers did not correlate with the cerebral cortex’s morphology or with ApoB, ApoA1, and ApoB/ApoA1.
Our study incorporated data on both traditional and non-traditional cardiovascular risk factors potentially reducing cognitive ability and accelerating AD, suggesting that ApoB is associated with cortical morphology via a vascular mechanism in the memory-complaint population 49 and with sulcal depth in the lateral occipital cortex, independent of biomarkers. Sulcal depth in the lateral occipital cortex was also associated with global cognitive function, speed/executive function and language function in individuals with memory complaints. Importantly, our study examined plasma biomarkers of AD for association with cortical morphology, adjusted for potential ApoE influences, and had a more comprehensive domain of cognitive testing. ApoB is still within the normal range, has been associated with sulcal depth of occipital cortex change, therefore, in preclinical AD may need to pay close attention to ApoB, provide a basis for early prevention and treatment of AD.
Limitations
This study has some limitations. First, a more comprehensive exploration of all pertinent polymorphisms within genome-wide association study lipid-associated genes might enhance our ability to elucidate the efficacy and potential causal attributes of apolipoproteins, plasma AD biomarkers, and cortical morphological indicators. Second, since our participants were all Asians with memory complaints, the findings may be subject to limited generalizability related to ethnicity and non-patient populations. Third, it is important to note that subjective memory complaints are not only a trait evident in preclinical AD but can be identified in adults in their 40 s. Furthermore, since the groups exhibited meaningful distinctions in certain characteristics and considering our relatively limited sample size, we refrained from conducting additional subgroup analyses to explore the variations between the groups. The sample size may influence the reported group differences that, although not statistically significant, may still hold practical significance. The total sample group for AD plasma biomarkers was 90, whereas apolipoproteins had a total of 97. Therefore, we recommend expanding the sample size, conducting further longitudinal follow-up investigations and establishing MCI or AD control groups to fully validate apolipoproteins, AD biomarkers, cortical morphology correlations and ascertain their applicability to specific populations. Finally, the combined use of software such as BrainVISA and Freesurfer to calculate the cortical morphological parameters may provide additional clarity and validation of the results.
Conclusion
Our study explored the association between ApoB, cortical morphology of the lateral occipital cortex, cognitive function, and apolipoproteins, as well as plasma AD biomarkers in patients reporting memory complaints. Consequently, ApoB could potentially serve as a beneficial biomarker for sulcal depth and a target for lipid modification therapy. Routine lipid testing and lipid management should be incorporated into strategies aimed at dementia prevention and risk reduction. Moreover, sulcal depth could function as a surrogate marker to assess the efficacy of future disease management strategies.
Ongoing efforts to identify modifiable risk factors related to sulcal depth may facilitate healthy cognitive aging and contribute to the development of new preventative strategies for dementia. Sulcal depth measurements obtained using the SBM method, an imaging modality that automatically and comprehensively extracts anatomical brain data, are relevant to precision medicine and should be incorporated in large-scale clinical projects, such as human brain projects or brain initiatives.
AUTHORS CONTRIBUTIONS
Jiayu Wang (Data curation; Formal analysis; Methodology; Writing – original draft); Lisi Xu (Data curation); Xuemei Chen (Data curation); Jiajing Wu (Data curation); Yu Chen (Conceptualization; Data curation); Ziqian Feng (Data curation); Li Dong (Project administration); Dezhong Yao (Project administration); Qingyan Cai (Supervision); Wei Jian (Supervision); Hongyi Li (Data curation); MingJun Duan (Conceptualization; Investigation; Writing – review & editing); Ziqi Wang (Funding acquisition; Methodology; Software; Supervision; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank Wenbin Wu’s team from the Hospital of Chengdu University of Traditional Chinese Medicine for collecting the blood samples.
FUNDING
This study was supported by the National Natural Science Foundation of China (No.82201628), the Chengdu Municipal Bureau of Science and Technology Innovation R&D Project (No.2022-YF05-01883-SN), the MOST 2030 Brain Project (Grant No.2022ZD0208500), and the Natural Science Foundation of Sichuan Province (2022NSFSC1398).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available upon reasonable request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.