
Abstract
China has proposed medical couplet body to alleviate residents’ difficulties in seeking medical treatment, and the future development ability of medical couplet body has gradually become a research interest. On the basis of prospect theory, this study constructs a comprehensive evaluation index system with qualitative and quantitative indexes, clear hierarchy, and diverse attribute characteristics. The development ability of medical couplet body is also comprehensively and systematically evaluated. In addition, the evidential reasoning method is proposed on the basis of the equivalent transformation of prospect value. Furthermore, the validity and feasibility of the model are proven through experiments, and the influence of decision makers’ risk attitude on the evaluation results is discussed.
Introduction
China’s economic development has become rapid since its reform and opening up, thus accelerating the country’s urbanization process. This development has greatly improved people’s material standard of living. During this period, China’s medical and health undertakings have also advanced, thereby achieving remarkable results [5,28,17,16, 5,28,17,16]. For example, the average life expectancy of Chinese citizens has been raised from 68 years in the early stage of reform and opening up to 76 years in 2018. China has also gradually improved its medical and health personnel training, medical infrastructure construction, and coverage rate of medical institutions. However, the rapid aging of China’s population and people’s increasing attention to health have resulted in an urgent medical reform because previous medical and health services have been proven insufficient to meet residents’ needs [24]. In 2009, the government began the medical and health system reform in the country to respond to the medical and health resource shortage caused by “medical care,” “hospital,” and “operation” fields [14,4, 14,4]. This reform aimed at developing a multi-channel, multi-form medical fundraising, which was gradually established with public ownership as the main body, and private ownership coexists. A new pattern of fundraising was formed, such as a multi-channel arrangement to run medical facilities. However, this design has not been proven effective in meeting residents’ demand to visit a doctor. Thus, to complete the medical resource integration and allow the utilization of medical resources, China devised a new medical reform program in 2013 and proposed the concept of medical association referred to as “couplet of medical.” The medical couplet body mainly refers to the integration of medical resources by gathering different fields and levels of hospitals to constitute a medical association [13]. This consortium is centered on large- and medium-sized hospitals in which communities, villages, and town hospitals are connected to the local medical institutions at the grassroots level between large- and medium-sized hospitals. Moreover, primary care grading diagnosis and two-way referral, namely, “ailments” and “common disease” are provided in the grassroots medical units, whereas “serious illnesses” and “incurable diseases” are treated in large- and medium-sized hospitals.
Experts from both hospitals are responsible for regularly visiting grassroots medical institutions to make rational allocation of limited medical resources in the area; to fully mobilize all medical resources to meet the different needs of varying patients; and ultimately, to form a convenient, fair, scientific, and standardized integrated medical service mode. The couplet of China is currently in the medical building development period. In general, the country is still in the exploration and test phase. The establishment of a medical couplet body involves many units, and its complexity involves wide range, large-scale, and 3D engineering. Therefore, the construction of a medical couplet body not only allocates medical pressure but also improves the medical security system and accelerates the development of medical-level important patterns. And with the continuous deepening of the construction process of medical couplet body, its advance work still faces many difficulties. The most important one is the lack of reasonable and effective evaluation mechanism or methods. They will lead to a series of problems in the construction of medical couplet body, such as such as inconsistent construction standards and lack of scientific evaluation methods. And the evaluation of medical couplet body has many advantages: (1) It can further promote the smooth construction and implementation of medical couplet body. (2) In response to the national call on the evaluation of medical couplet body, it provides a theoretical basis for the implementation of the performance management and comprehensive evaluation of medical couple. (3) It is conducive to the horizontal comparison between medical couplet body, and provides a reference for improvement direction of construction of medical couplet body. In addition, it can effectively improve the enthusiasm of construction personnel. Thus, an evaluation of the couplet of medical development ability is important to promote its rapid and orderly development. The future will also become one of the important indicators of the couplet of medical development.
At present, the couplet of medical research is still in the exploration of a new stage concept. It mainly concentrates on the analysis of the formation and advancement of medical couplet body, definition, basic results, operation mode, and operation mechanism. To aid the development of the couplet of medical evaluation and research problems, such as less construction direction, this study focuses on the comprehensive development ability and construction of the couplet of medical evaluation standard research, which mainly uses prospect theory for the decision-making process in traditional evidence reasoning methods. First, the process of evidential reasoning (ER) entails the transformation of the original evaluation framework into a common framework, which is usually converted according to the invariance of utility before and after the conversion. However, in the actual decision-making process, expected utility theory may change, whereas prospect theory makes an uncertainty consistent with the actual decision-making needs. Second, prospect theory includes the influence of psychological factors of decision makers in the research scope. Finally, the transformation of the original recognition framework based on prospect value can obtain the evaluation value of each scheme on the basis of the data information itself, without knowing the evaluation standard of the index in advance. Therefore, this study employs the prospect value method to evaluate the development ability of medical couplet body.
The structure of this paper is as follows: Section 2 introduces the relevant literature. Section 3 describes the concepts of ER and prospect theory. Section 4 presents the evaluation model of the development ability of medical couplet body. Section 5 discusses the experimental analysis. Section 6 provides the conclusion and prospect.
Literature review
Medical couplet body is an association wherein public hospitals of different types and levels in a certain region join together to form a medical community. Its goals are to achieve information sharing and share responsibilities and interests among involved parties. Harris et al. [7] suggested that the continuous nursing work of general practitioners and hospitals should be integrated with community hospitals in the fields of health promotion and public health, so that information between hospitals and community hospitals can be shared. Patients can also have additional choices in inpatient care and other aspects. Pelikan et al. [19] analyzed the concept and development of health-promoting hospitals and believed that circular medicine in such hospitals can become one of the advancement directions of hospital quality. In the context of the state of Missouri, Beatty et al. [3] suggested that a nonprofit hospital in collaboration with local health authorities based on the community hospital need assessment is essential because mortality regional medical resources seem to be decreasing, thus strengthening cooperation among healthcare providers is advantageous for a reasonable distribution of medical and financial resources.Medrano et al.[18] introduce Savana, an AI-enabled system based on Natural Language Processing (NLP) and Neural Networks, capable of, for instance, the automatic expansion of medical terminologies, thus enabling the re-use of information expressed in natural language in clinical reports. However, most recent studies on hospital association are based on the basic research of medical association, and the overall evaluation of medical association is seldom analyzed.
ER method is an uncertainty reasoning method, which can rationally deal with evaluation problems in many cases, such as the existence of unknown and uncertain information. Yang et al. [27] used ER method to deal with uncertainty in maritime safety assessment and management. They proposed a new computational aggregation method by using ER method, which can retain the original characteristics of multiple attributes with various information types. Moreover, Zhang et al. [29] proposed a complete e-commerce security assessment model and method through ER method and proved that this model is beneficial when solving decision-making problems, especially in the aspect of e-commerce security assessment. Kong et al. [12] also evaluated medical quality by employing ER method, and the results revealed that multiple indicators can be summarized by this method to obtain the comprehensive hospital nursing quality assessment. However, most research on evidence-based reasoning methods seldom consider the psychological factors of decision makers [25].
Prospect theory was initially proposed by Kahneman and Tversky [10]. It analyzes the decision-making problem of people from the perspective of behavioral psychology and considers psychological factors when making decisions. The core content of prospect theory is whether people can always remain rational when making decisions, especially in the face of future uncertain factors. Kahneman and Tversky [10] indicated that people often make systematic mistakes and deviate from the optimal behavior assumption model of economics, thus people cannot always be rational when making decisions. Liu et al. [15] proposed a multi-attribute decision-making method on the basis of prospect theory, which is used to analyze the form of interval probability and uncertain language variables. Attema et al. [2] believed that the prospect theory of quantitative assessment in the field of health has a certain decision-making effect.Khiat et al.[11] consider that each decision maker is assimilated to an agent that has a decision-making autonomy, in which he interacts with other agents in the debate through a negotiation process in order to reach an acceptable compromise. Zhou et al. [30] evaluated the risk of drivers’ path selection on the basis of prospect theory. They suggested that prospect theory is more consistent with human behavior characteristics than traditional economic theories. Zhou et al. [30] also provided a reference to understand individuals’ attitude toward risks and uncertainties.Adrian et al.[1] identify and analyze the affecting factors and elements of BDA implementation and to propose a conceptual model for effective decision-making through BDA implementation assessment.
However, these studies cannot perform the multi-attribute evaluation of multi-factor integrated information and uncertainty reasoning.
Basic theory
ER theory
ER was initially proposed by Dempster [6]. He used multi-value mapping to obtain the upper and lower bounds of probability. Shafer [20] promoted and developed ER, and thus alternatively called Dempster-Shafer theory. The evidential reasoning approach has been applied to solve many assessment problems such as engineering design, safety assessment [26]. Evidence theory focuses on the large system of decomposition-coordination thought, which involves decision theory and utility function, theory of artificial intelligence, the combination of evidence theory, and the ambiguous mathematics theory from multiple disciplines. Evidence theory is suitable for processing and comprehensively understanding unknown and uncertain fuzzy information about multi-attribute decision-making problems. ER is based on evidence theory, which is a method suitable for dealing with uncertainty.
When dealing with the impact evaluation of different schemes on many factors, ER method allows a scheme to have different evaluation levels for a factor, which is more compatible with people’s habit of knowing things and thus ensures an authentic reflection of the initial information. Simultaneously, the recursive algorithm of ER is adopted to synthesize the result of impact level recognition, which preserves the uncertainty of the initial information, thereby proving that the evaluation result is scientific and reasonable.
ER has the following advantages: (1) ER has a solid mathematical theoretical foundation. (2) ER can simultaneously fuse multiple types of indexes, including uncertain evaluation indexes such as such as fuzzy number, interval number, interval belief structure, and determined evaluation indexes such as fixed value and language evaluation. (3) ER has a good applicability to deal with complex uncertain problems.
Basic principles of prospect theory
Prospect theory describes and predicts people’s behavior during the risk decision-making process. This definition is inconsistent with the traditional expected value theory and expected utility theory. People’s risk preference behavior is inconsistent when dealing with gain and loss, thus they become risk seeking in the face of “loss,” whereas they show risk aversion in the face of “gain.” Establishing and changing reference points affect people’s feelings of gain and loss and decision making.
The following equation focuses on the calculation of prospect value. Foreground theory posits that during an uncertain and risky decision-making process, the decision is represented by prospect value V, which is determined by two functions, namely, value function v (Δx) and decision weight function π (p).
(1) Value function v (Δx)
The specific form of value function is as follows:
Δx represents a profit and loss value, that is, the difference between the real value and the reference point. If Δx ⩾ 0, then it represents a gain. If Δx < 0, then it indicates a loss. The loss function is steeper than the gain function, thus decision makers are often sensitive to loss. Moreover, α and β are risk attitude coefficients, 0 < α< 1, 0 < β< 1, thus the higher the two values are, the riskier the decision makers’ attitude is. λ refers to the risk aversion coefficient. Generally, the larger λ is, the more inclined decision makers are to risk aversion. The value function is illustrated in Fig. 1.

Value function.
(2) Decision weight function π (p)
The specific form of decision weight function is as follows:
p represents the probability of the result, whereas γ and δ represent the attitude coefficient of gain and loss, respectively, thus reflecting the degree of convexity of the function.
Prospect theory has the following advantages: (1) It has in-depth discussion on the influence of psychological factors in the decision-making process, and has a better explanation and description of the actual decision-making behavior. (2) According to this theory, when people face uncertain and risky decision-making environment, the theory holds that decision results will be influenced by people’s risk attitudes and subjective judgment criteria. So it is more scientific to make decisions using prospect instead of utility.
The release of the guideline on the development of medical couplet body has led to the launch of relevant pilot works in various provinces across China, and certain preliminary experiences and models have been formed. However, the evaluation on the development ability of medical couplet body faces many difficulties. To solve these problems, this chapter proposes a relatively complete and scientific evaluation index system. ER method, which considers the transformation of recognition framework, is also proposed to construct the evaluation model of the development ability of medical couplet body. This method is mainly divided into three parts, as illustrated in Fig. 2. When applying ER to multi-attribute decision analysis problems, we usually define a recognition framework, which is an expression of all possible results for evaluation. Because different attributes have different recognition frameworks, it is necessary to form a public recognition framework to integrate different attributes and obtain the final evaluation result of each evaluation object. And the contributions of this framework are as follows: (1) In the process of transforming the original evaluation framework into the public recognition framework, ER is usually transformed according to the invariance of the utility before and after the transformation, while the prospect theory corrects the expected utility theory and is more in line with people’s actual decisions. (2) Prospect theory considers the psychological factors of decision makers and can study the influence of decision makers’ risk attitude on decision making. (3) The last is to convert the original identification framework based on the prospect value without knowing the evaluation criteria of indicators in advance.
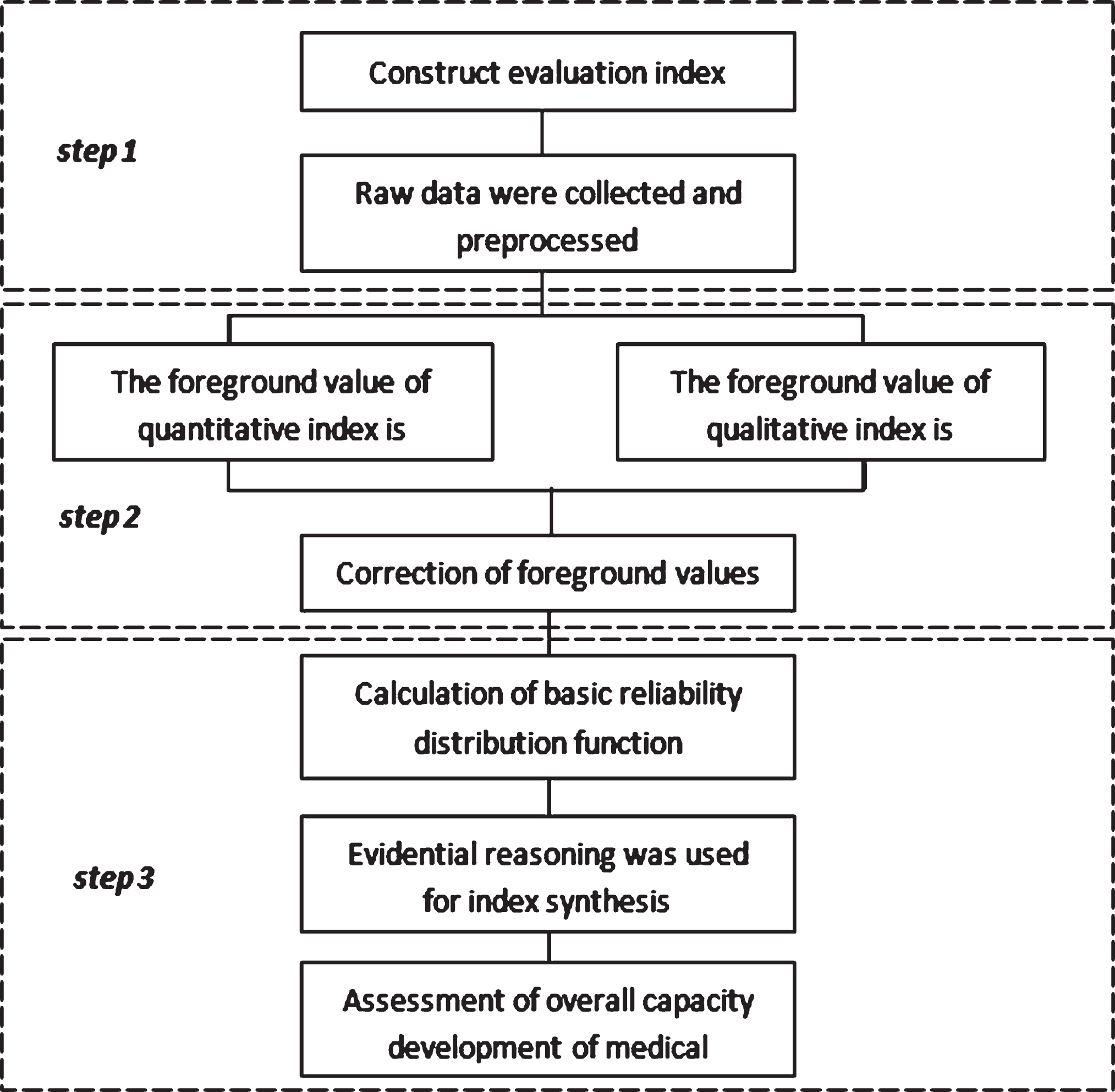
Procedure of medical association evaluation method based on an improved ER method.
This chapter refers to the data issued by the National Health and Family Planning Commission < Opinions on the performance evaluation indicators of medical institutions > Issued by the leading group for deepening medical reform in Nanjing < Opinions on the performance evaluation indicators of medical institutions > and< “China model” in the world view –practice exploration and management innovation of medical couplet body model > Discussion on the evaluation index system of medical association. In addition, the evaluation index system is constructed by considering the components of the development ability of medical association and the principles of index construction from the management operation, medical services, medical resources, social benefit of the four first-level indicators, management structure, members of units, and information dissemination level. In the business level, 13 secondary indicators, such as organization structure, management system, three armor hospitals, and 40 grassroots medical institutions, are provided to build three-level indicators, including the qualitative index of the regional health planning commission organization. Third-party evaluation experts are responsible for the qualitative evaluation, whereas quantitative indicators can be obtained on the basis of the actual statistic. The specific construction situation is illustrated in Appendix 1.
Calculation and correction of prospect value
Different types of indicators according to different methods are used to explore value calculation. Subsequently, the future value of each index is obtained depending on whether a couplet of medical prospects selects indexes of the construction of value correction. Finally, the prospect of the adjusted value for normalization is determined for the subsequent reliability calculation of distribution function and basic synthesis. Moreover, prospect theory is discussed from the psychological perspective in the face of the actual decision making. Under uncertainty, adjusting the application of expected utility theory is insufficient, thus revealing people’s irrational psychological factors during the decision-making process. Multi-attribute decision making, which has been used in several studies, was employed. Comprehensive evaluation was also conducted on this part, which explores the index system by using all kinds of index value calculation and correction.
(1) Calculation of the prospect value of quantitative indicators.
Suppose
Among them
After obtaining the value function of the quantitative indicator, the value of the decision weight function must be calculated. The formula can be calculated as follows:
Finally, the prospect value of the quantitative indicator may be from
(2) Calculation of the prospect value of qualitative index
In the evaluation index system of the development ability of medical association, different types of index prospect values have different methods for data processing. Therefore, the type of index is important for the calculation of prospect value. Prospect theory requires quantitative data, thus the data of qualitative indicators must be preprocessed and transformed into quantitative data. Assuming that
Hn,irepresent the sample values of
where
The profit and loss values of the quantitative index can be calculated using Formula (4). For qualitative indicators,
Which
The analysis reveals that two income indexes of interval value Hn,iand If If If If If If
The calculation method of the profit and loss values of the given income-type index suggests that the profit and loss values of income- and cost-type indices can be obtained. The calculation results are shown in Tables 1 and 2.
Gain and loss for all possible cases (benefit criteria)
Gain and loss for all possible cases (cost criteria)
After obtaining the qualitative index of the profit and loss values, the qualitative indicators from the prospect of a possible level value formula
(3) Correction of prospect value
The evaluation index system of the development ability of medical couplet body results in “extremely large” income-type indicators, such as the number of grade A hospitals and the total number of medical technicians among others. “Extremely small” cost indicators, such as the incidence of medical disputes, the rate of patient complaints, and the average length of hospital stay before elective surgery, are also obtained. In addition to these quantitative indicators, qualitative indicators, such as information platform construction situation and the identity of the couplet of medical staff, also exist. Therefore, each index of each dimension and scale is not unified, and the indexes cannot be compared. This result causes inconvenience to the comparison of the couplet of medical development ability. To avoid the effects of dimension and order of magnitude difference, a dimensionless processing evaluation index must be constructed. This index is a prerequisite for the realization of index integration, which can have an impact on subsequent evaluation and research. Therefore, the extreme value processing method is employed to conduct dimensionless processing for the comprehensive prospect value obtained from the determined types of indicators of each sample, as indicated in the following formula:
e i refers to the qualitative or quantitative indicators in the evaluation index system of the development ability of medical couplet body, whereas max{ V (e i ) } refers to the maximum value in the comprehensive prospect value of this index. min{ V (e i ) } comprehensive outlook refers to the index value of the minimum value, whereas V (e i ) and V (e i ) * (0 ⩽ V (e i ) * ⩽ 1) are the values before and after the dimensionless comprehensive prospect value of the index, respectively.
After the dimensionless treatment, the prospect value of the sample index is normalized to the interval of [0, 1]. Subsequently, the prospect value must be modified according to whether the index is a required index of the medical association’s rigid assessment index or an optional index of additional score assessment item. The specific correction method is presented in the following formula.
For required indicators:
For optional indicators:
where
The modified prospect value suggested that the basic reliability distribution function of each index of each sample should be calculated, and the index was synthesized according to the analytical algorithm of ER. The comprehensive evaluation results of each medical association sample were also obtained. Finally, the results were further analyzed.
Assume that the comprehensive evaluation result of attribute e_i after being converted to the public identification framework is as follows:
is analysis implies that the initial reliability distribution function of all indexes in the indicator system of each sample can be calculated.
Experiment description
The evaluation index system of the development ability of medical couplet body has been established, and an improved ER method has been proposed to analyze such an ability. In this paper, the emphasis is on the improved method rather than the actual data, so the data used in the experiment in this paper is a simulation example. And five medical associations (a1, a2, a3, a4, a5) are included in this experiment. After a period of construction and development, the medical associations are found to have different degrees of advancement in the four aspects of “management operation,” “medical service,” “medical resources,” and “social benefits.” The development level, development focus, and improvement direction of each medical couplet body are analyzed in detail through the pattern of medical couplet body evaluation. Moreover, the application prospect of the index system and evaluation method are clarified. The influence of decision makers’ risk attitude on the decision result is investigated by adjusting the parameters that influence decision makers’ risk attitude.
To avoid the influence of index weight on the treatment mechanism of compulsory and optional indexes, the index weight of each level in the evaluation index system of the development ability of medical couplet body is obtained using the method of average distribution. This experiment aims to comprehensively evaluate medical couplet body through the proposed evaluation index system and evaluation method, which makes the comparison of different medical consortia with quantitative methods feasible. Through the analysis of the experimental results, this paper can find the key points in the construction of medical couplet body, promote the further development of each medical couplet body, and ultimately improve the overall performance of the national medical level. And the value of the risk attitude coefficients α and β (α=β) for the value function in prospect theory is set to 0.2, 0.5 and 0.8 respectively, which are used to investigate the influence of decision makers’ attitude on decision-making results. Other parameters are calculated by Tversky and Kahneman [21, 22] by conducting several empirical experiments: λ = 2.26; if Δx ≧ 0, the value of δ is 0.61. If Δx<0, the value of δ is 0.69. Moreover, the original recognition framework for five medical associations and the unified basic belief assignment for each indictor which is transformed from raw data by the improved ER method in our paper is showed in Appendix 2 and 3, respectively.
The basic reliability distribution function suggests that after transforming each index, they are synthesized step by step by using the analytical algorithm of ER. The comprehensive evaluation results of the second-level index, first-level index, and even the overall development level of medical couplet body are obtained.
Result analysis
Experimental results
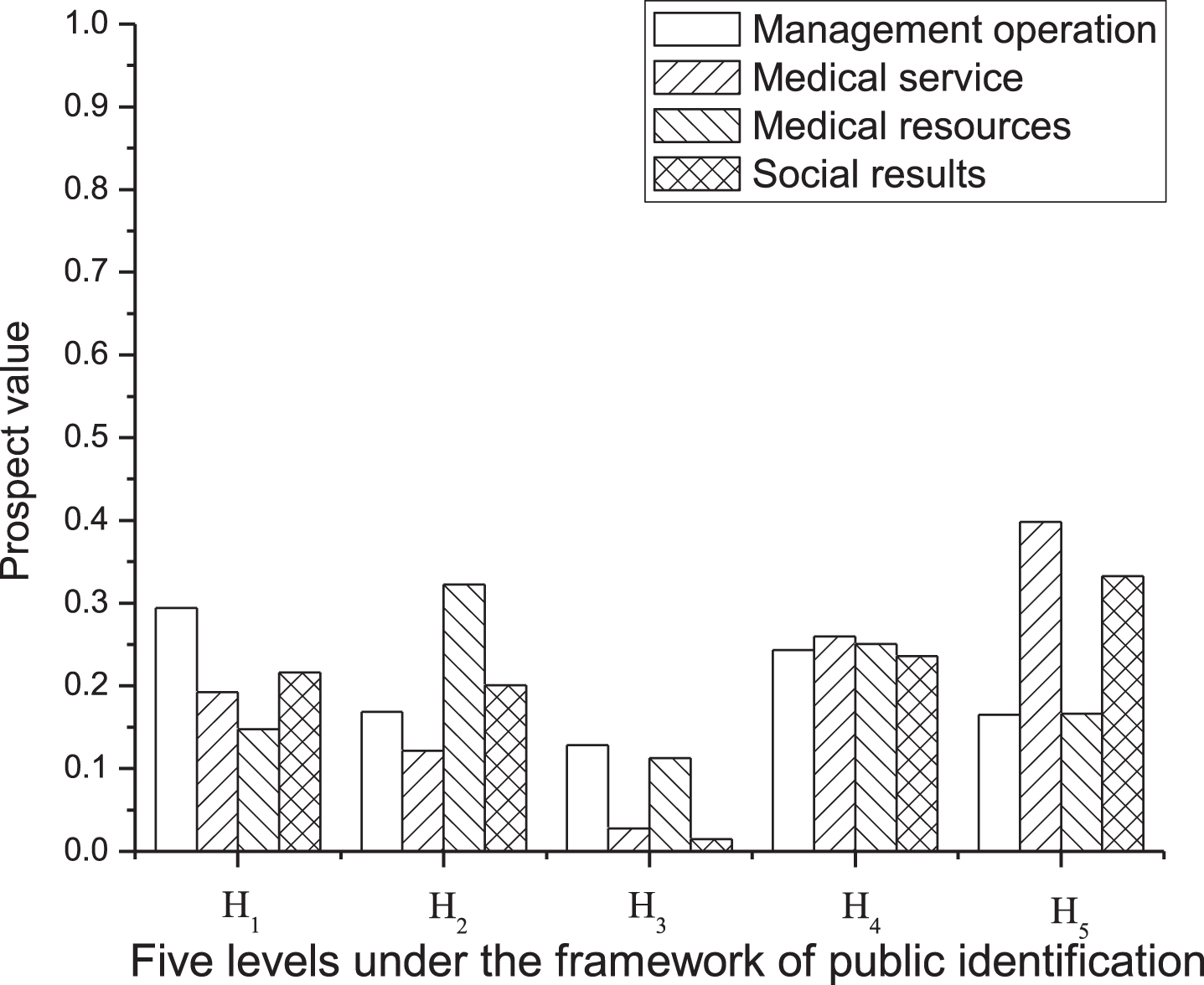
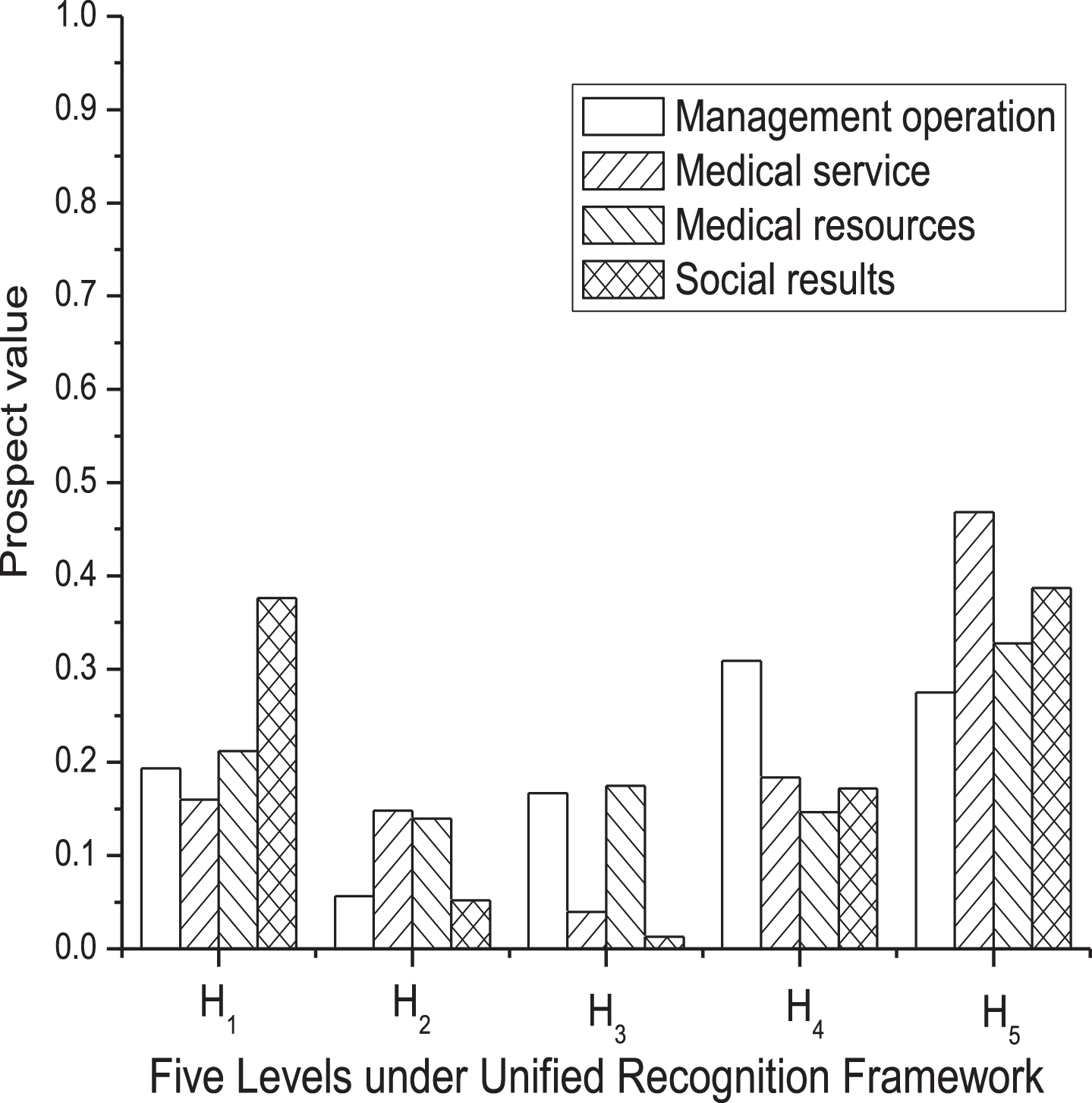
This chapter proposes the couplet of medical development capability assessment method of the index of the couplet of five medical raw data to calculate the coefficient of decision weighting function of risk attitude. First, set α=β=0.5 and obtain all the normalized index and prospect adjusted values. The prospect and optional index values are then selected as illustrated in Figs. 3 and 4.

Normalized and modified prospect values of mandatory indicators.
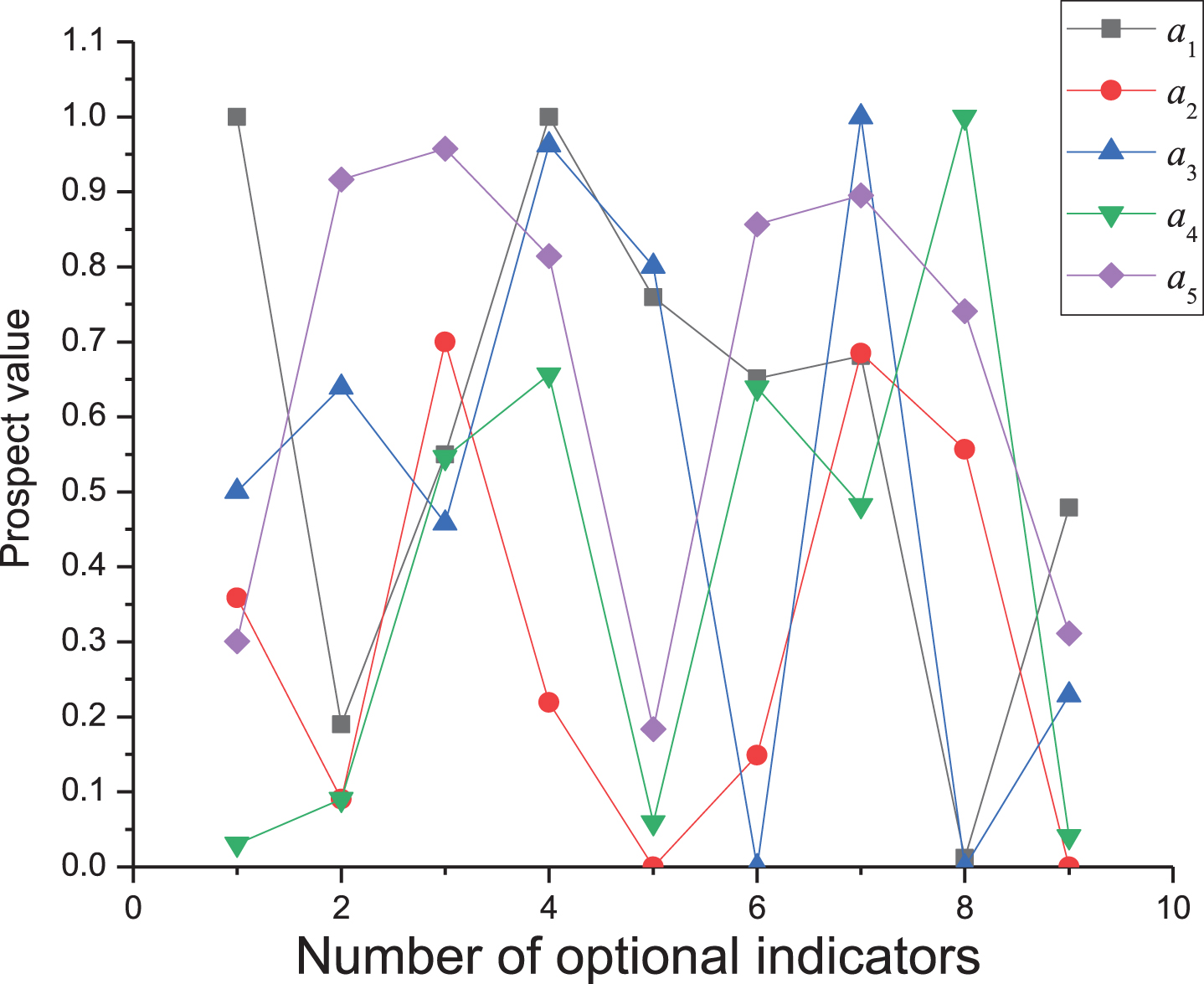
Normalized and modified prospect values of optional indicators.
Figs. 3 and 4 illustrates that the experimental results are consistent with the original intention of the required and optional indexes in the evaluation index system after their prospect values are adjusted by the correction mechanism. The evaluation index system has two purposes to distinguish between mandatory and optional indexes. First, the required index is the basic requirement for the construction of medical couplet body. If the index does not reach the average level, then the construction and development of medical couplet body is affected to a large extent. Many “minimum values” are reflected in the change of the prospect index value. Second, optional index is first considered with other indexes belonging to secondary indicators. The selected index must be average; otherwise, optional index must be analyzed and is also better than average. If the optional index for the cure of the couplet of development level evaluation has certain enhancement function and no index is better than average, then optional indicators must not be adjusted. If any other compulsory indicator belongs to the same second-level indicator with the optional indicator that does not reach the average level, no matter how well the optional measures perform, the third-level index under the second-level index performs poorly. Therefore, the overall evaluation of this optional index on the development level of medical association is not only “plus points” but also “minus points,” whereas the change of the prospect value of the index is “polarization.”
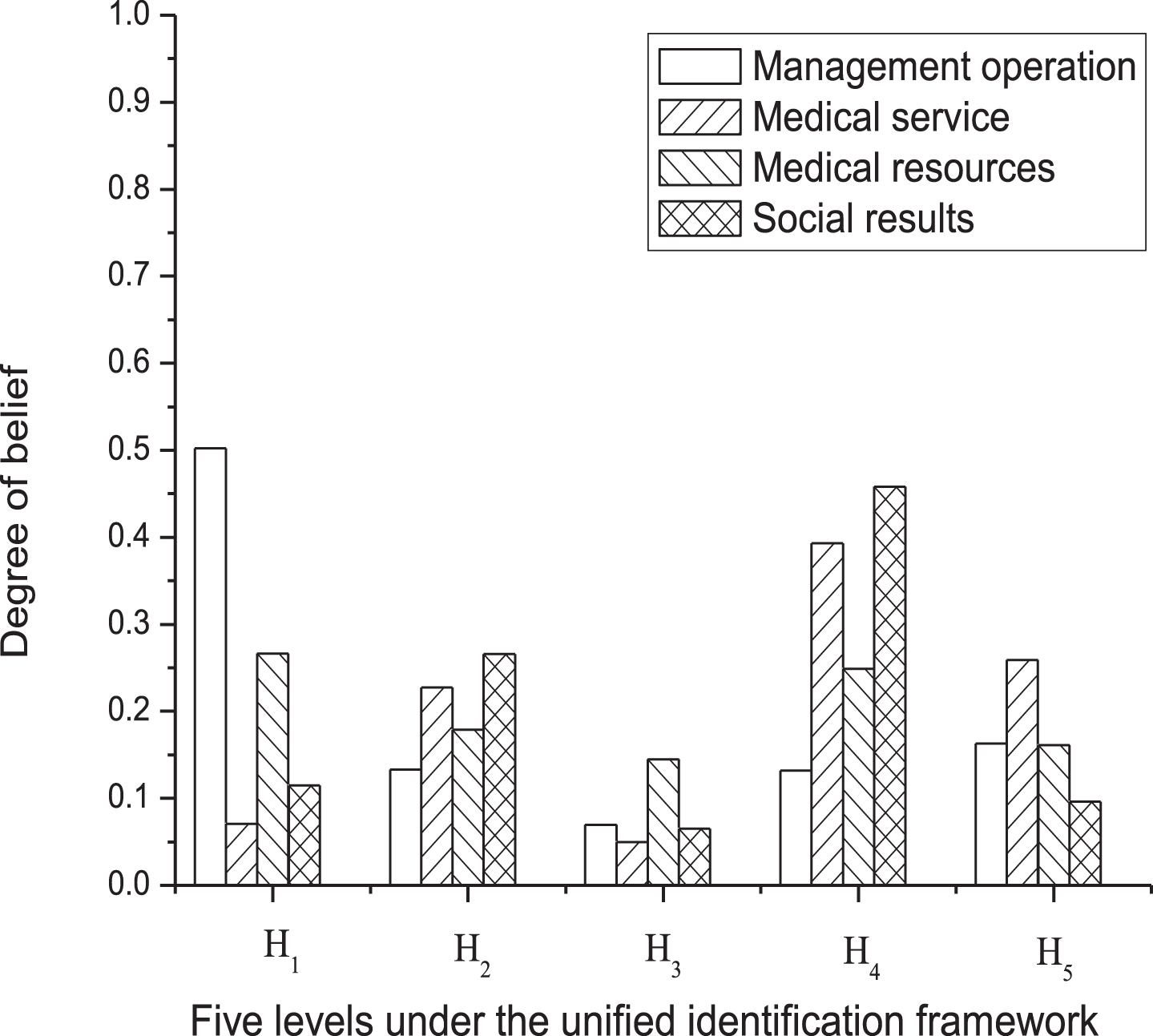
Figure 5 shows that medical couplet body a1 has high confidence in H4 and H5, whereas the confidence in other grades is relatively average at a low level. Medical couplet body a5 has high confidence on the H4 level but low confidence on other levels. Therefore, a1 and a5 are generally in a good development level. a2 and a4 show the phenomenon of “polarization” in the confidence of each grade, that is, the confidence of the middle grade is low, whereas that of the two sides is high. Thus, the development level of both medical associations fluctuates greatly in the evaluation level. However, a2 confidence is inclined to a low level in general, whereas a4 confidence is relatively average on low and high levels. The size and confidence of prospect value defined on each level under the unified identification framework indicate that the sequencing of the five medical associations at the development level can be calculated, as presented in the line diagram in Fig. 5. From top to bottom, medical couplet body a1 has the best development, whereas medical couplet body a2 has the least development. Medical consortia a5, a3, and a4 rank second, third, and fourth places in the development, respectively.
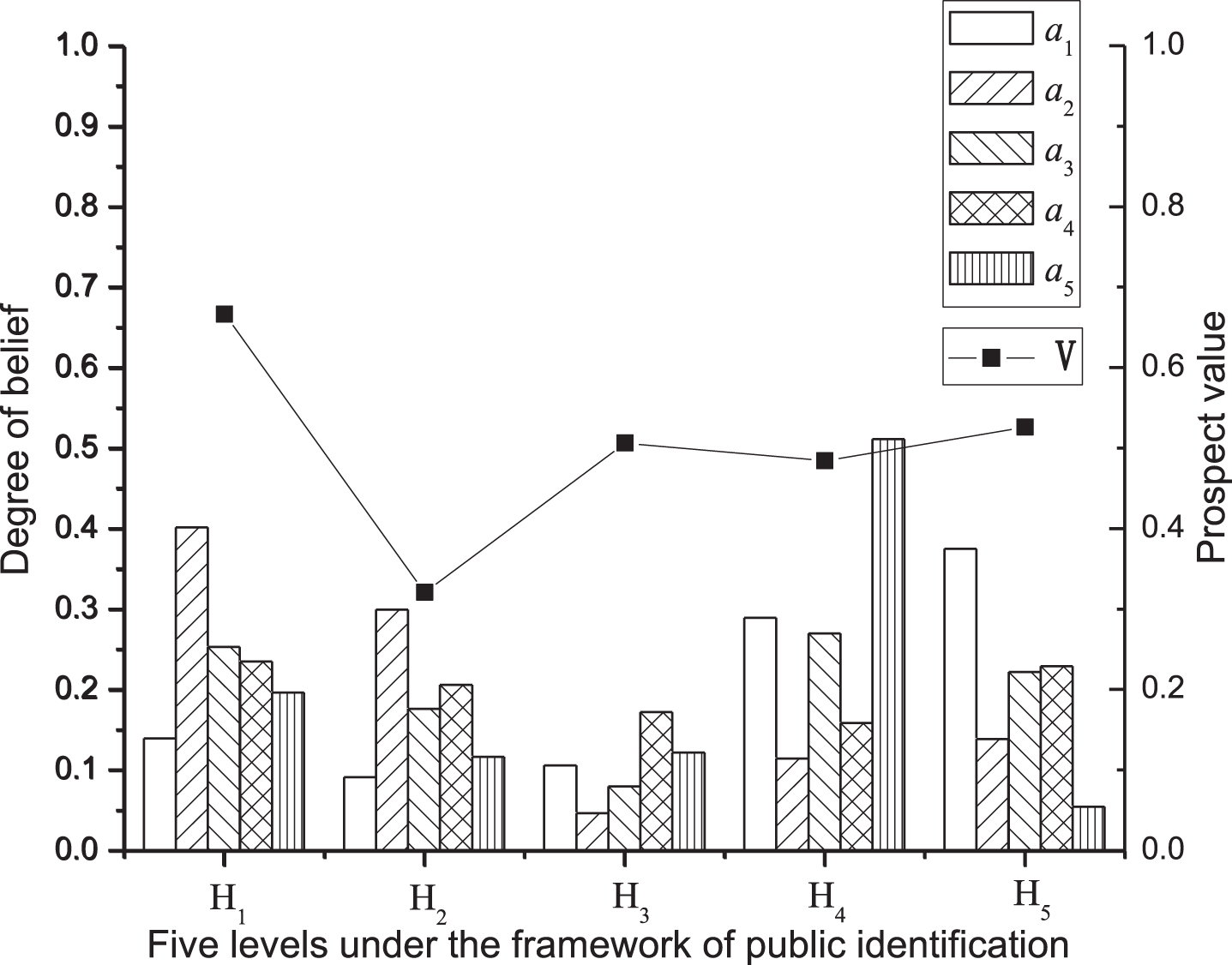
Belief allocation and overall prospect values of five medical associations.
The analysis of the given model explains that the greater the risk attitude coefficients α and β of the decision-making weight function in prospect theory are, the higher the risk attitude of decision makers, implying that they likely take risks. In this chapter, the risk attitude coefficient is adjusted from the initial 0.5, to 0.2, and 0.8 to analyze the impact of the different risk attitudes of decision makers on the decision-making results. Moreover, the influences on the evaluation result of a medical association and on the sequencing of five medical associations are analyzed.
(1) Influence of risk attitude coefficient on the evaluation of medical couplet body a1
In this chapter, medical couplet body a1 is taken as a sample to investigate the influence of different risk attitude coefficients on the prospect value of each three-level index, as illustrated in Fig. 6.
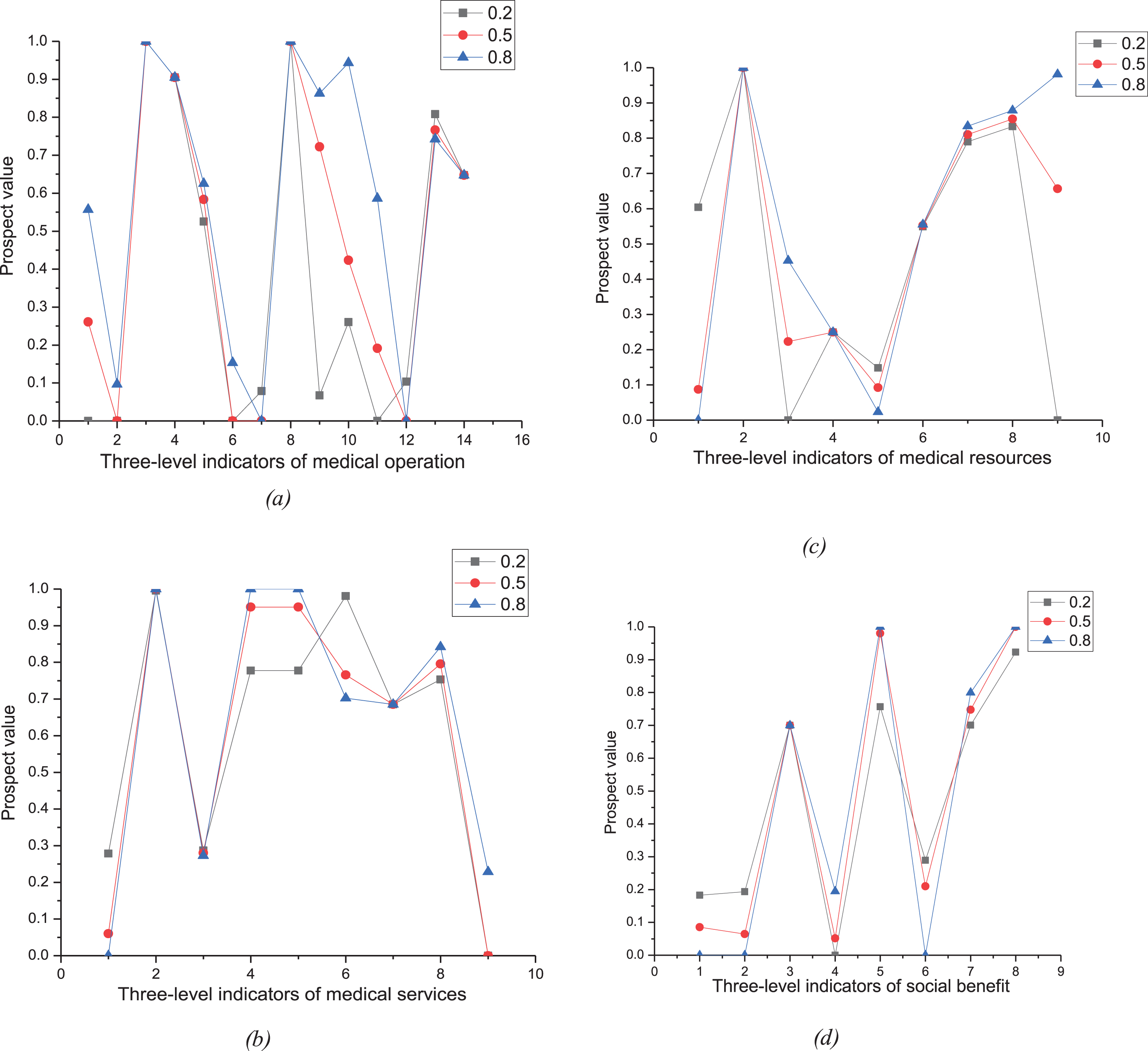
Overall prospect values for bottom indicators belonging to different top indicators with different α.
The analysis in Fig. 6 explains that the prospect value of each three-level indicator under the four first-level indicators of management operation, medical service, medical resources, and social benefits changes as the risk attitude coefficient changes. Specifically, in the overall trend, the increase of decision makers’ risk attitude coefficient results in the increase of the prospect value of each index correspondingly, that is, the more inclined decision makers are to take risks, the higher the prospect value of each index and the higher the possibility of decision selection are.
Figures 7, 8, and 9 indicate that as decision makers’ risk attitude coefficients change, the confidence of the four first-level indicators in the evaluation index system of medical couplet body fluctuates at all levels. Evidently, the change of decision makers’ risk attitude poses a great impact on the focus of medical couplet body construction. When the risk attitude is conservative, the overall evaluation of “management operation” is poor. Therefore, during the process of promotion and development, medical consortia should strengthen their construction of management operation, and the government should consider management operation when formulating relevant policies or providing special support. The construction emphasis in “management operation” can be analyzed by the confidence distribution of the second-level indicators obtained by the ER algorithm, but such an emphasis is not repeated in this chapter. When decision makers’ risk attitude is neutral, the overall evaluation of “medical resources” is poor. Therefore, during the process of construction and development, the construction and investment of subordinate indexes should be given focus. When the attitude is risky, the overall evaluation of “social benefits” is low, suggesting that the construction and development of medical couplet body must be given attention.
The belief allocation of four top-indicators with α = 0.2.
The belief allocation of four top-indicators with α = 0.5.
The belief allocation of four top-indicators with α = 0.8.
(2) Effect of risk attitude coefficient on the sequencing of five medical associations
Figure 10 indicates that under different risk attitude coefficients, the size and ranking of the prospect value of the development level of the five medical associations are represented. When the evaluation index system and method of the development ability of medical couplet body proposed in this chapter are utilized to make a decision, the evaluation result can be affected by decision makers’ risk attitude. Fig. 10 shows that when the risk attitude changes from 0.2, to 0.5, and to 0.8, the overall evaluation sequence of medical couplet body slightly changes. Only when the risk attitude is 0.8 can the overall ranking of a4 and a5 change. This finding indicates that the change of risk attitude can have a relatively large impact on the evaluation of the first-level indicators of a single medical couplet body, thereby leading to the change of construction focus. However, the result poses little impact on the evaluation order of the whole medical couplet body.
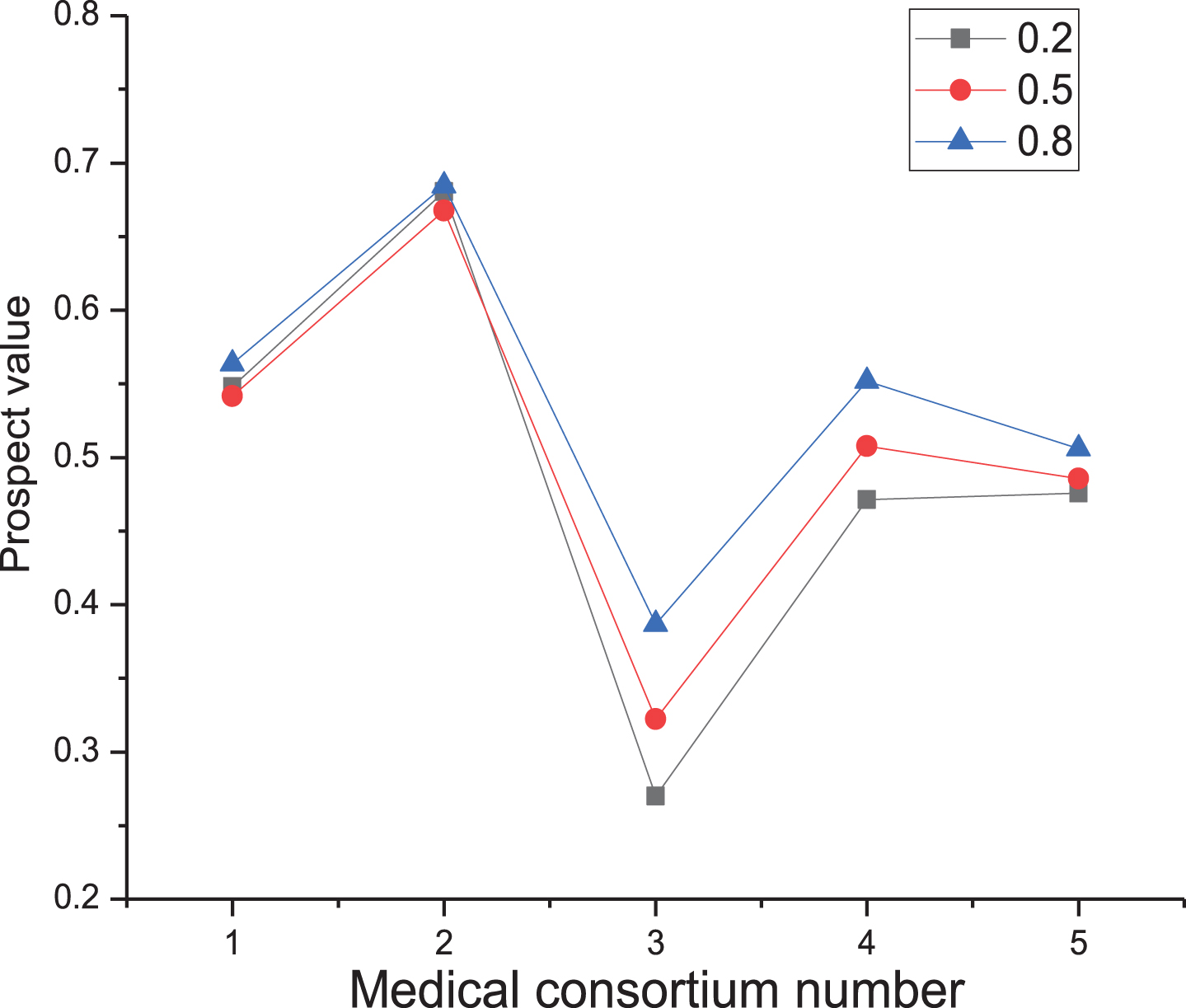
Influence of decision makers’ risk attitude on the ranking of medical associations.
The mode of medical association is developed on the basis of the new medical reform plan to solve the uneven distribution of medical resources, the disorder of residents’ medical treatment, and the independence of hospitals at all levels. The plan aims to establish a new medical service pattern of the rational division of labor, full utilization of all medical resources, and orderly medical treatment for residents. This study mainly evaluates the development level of medical couplet body. However, most current development evaluations of medical couplet body by domestic scholars focus on qualitative analysis and index construction, and effective quantitative studies are few. The evaluation of the development level of medical couplet body is conducive to the strengthening of the linkage between the optimal allocation of medical resources and two-way referral. Through the horizontal and vertical comparisons of medical couplet body, the key factors restricting its development can determined. The following are the advantages of using ER method in this study. First, a comprehensive and deep evaluation index system is constructed by integrating the qualitative analysis of domestic scholars while analyzing the evaluation objects and objectives. Second, given the limitations of the utility theory of decision makers in the traditional ER method, this study adopts the prospect value-based method to uniformly process the original data. This method enhances the applicability of the traditional ER method to an extent.
In general, the establishment of medical couplet body is a long-term, complex, and systematic project in which the government, hospitals, and residents have their own characteristics. Hospitals must consider their own medical equipment and personnel training among other aspects. Resident patients must select the appropriate medical unit for medical treatment according to their own situation. This study only focuses on the evaluation of the development index of medical association, without a comprehensive and multi-angle discussion, thus implying its limitation.
Footnotes
Appendix 1
Evaluation indicator system of comprehensive medical association
| Top -indicators | Sub-indicators | Bottm-indicators | Characters |
| Management operations E(1) | Management structure E1(1) | Organizational structure E11(1) | L,M |
| The management system E_12(1) | L,M | ||
| Personnel and site protection E_13(1) | L,M | ||
| Members of the unit E_2(1) | Number of class a hospitals E_21(1) | T,M | |
| Number of primary medical institutions E_22(1) | T,M | ||
| Cooperation tightness E_23(1) | L,O | ||
| Internal medical technical personnel exchange frequency E_24(1) | T,O | ||
| Implementation of two-way referral E_25(1) | L,M | ||
| Information level E_3(1) | Information platform construction E_31(1) | L,M | |
| Internal communication of diagnosis results E_32(1) | L,O | ||
| Telemedicine E_33(1) | L,M | ||
| Business level E_4(1) | National key(characteristics) specialized subject E_41(1) | T,O | |
| Provincial key (characteristics) specialized subject E_42(1) | T,M | ||
| The municipal key (characteristics) specialized subject E_43(1) | T,M | ||
| Quantity of medical services E_1(2) | Annual number of outpatient and emergency department visits E_11(2) | T,M | |
| Medical service E(2) | Annual hospital discharge times E_12(2) | T,M | |
| Efficiency of medical services E_2(2) | Hospital bed utilization rate E_21 (2) | T,M | |
| Average hospital stay E_22(2) | T,M | ||
| Utilization of primary medical institutions E_23(2) | T,O | ||
| Convenience of medical service E_3(2) | Proportion of nurse beds E_31(2) | T,M | |
| Ratio of doctors to nurses E_32(2) | T,M | ||
| The average hospitalization time before elective surgery E_33(2) | T,M | ||
| Quality care services E_34(2) | L,O | ||
| The human resources E_1(3) | Total number of medical technicians E_11(3) | T,M | |
| Scientific research and innovation of professional technical personnel E_12(3) | L,M | ||
| Medical resources E(3) | Employees’ sense of identity to medical couplet body E_13(3) | L,O | |
| Financial resources E_2(3) | Revenue growth rate E_21(3) | T,M | |
| Growth rate of total assets E_22(3) | T,M | ||
| Get the government’s special investment quota E_23(3) | T,O | ||
| Material resources E_3(3) | Rate of return on fixed assets E_31(3) | T,M | |
| Equipment utilization E_32(3) | T,M | ||
| Joint ward E_33(3) | L,O | ||
| Public satisfaction E_1(4) | Service object satisfaction E_11(4) | T,M | |
| Employee satisfaction E_12(4) | T,M | ||
| Brand effect recognition E_13(4) | L,O | ||
| Social benefits E(4) | Recommendation intention of medical couplet body E_14(4) | L,O | |
| Cost control E_2(4) | Every time the average of outpatient service charge E_21(4) | T,M | |
| Average cost per hospital stay E_22(4) | T,M | ||
| The doctor-patient relationship E_3(4) | Incidence of medical disputes E_31(4) | T,M | |
| Patient complaint rate E_32(4) | T,M |
NOTE: L and T denote qualitative and quantitative indicators, respectively; M and O denote mandatory and optional indicators, respectively.
Appendix 2
Original recognition frameworks of evaluation indicator system for five medical associations in our experiment
| Bottm -indicators | Original recognition framework |
| E11(1) | {H1, H2, H3} |
| E12(1) | {H1, H2, H3, H4} |
| E13(1) | {H1, H2, H3, H4, H5, H6} |
| E23(1) | {H1, H2, H3, H4, H5} |
| E25(1) | {H1, H2, H3, H4} |
| E31(1) | {H1, H2, H3} |
| E32(1) | {H1, H2, H3, H4, H5, H6} |
| E33(1) | {H1, H2, H3} |
| E34(2) | {H1, H2, H3} |
| E12(3) | {H1, H2, H3, H4} |
| E13(3) | {H1, H2, H3} |
| E33(3) | {H1, H2, H3, H4, H5} |
| E13(4) | {H1, H2, H3, H4} |
| E14(4) | {H1, H2, H3} |
Appendix 3
The unified basic belief assginment for each indictor in evaluation indicator system of hospital association developmental ability
| Bottm -indicators | The unified basic belief assginment for each indictor in evaluation indicator system of hospital association developmental ability (a1, a2, a3, a4, a5) | ||||
| a 1 | a 2 | a 3 | a 4 | a 5 | |
| E11(1) | (0,0.830,0.170,0,0) | (0,0,0,0.472,0.528) | (0,0.947,0.053,0,0) | (0,0,0.269,0.731,0) | (0,0,0,0,1) |
| E12(1) | (1,0,0,0,0) | (0,0,0,0,1) | (0.335,0.655,0,0,0) | (0.641,0.359,0,0,0) | (0.805,0.195,0,0,0) |
| E13(1) | (0,0,0,0,1) | (0,0,0.340,0.660,0) | (0,0,0,0.657,0.343) | (0,0,0,0.424,0.576) | (0,0,0.766,0.234,0) |
| E21(1) | (0,0,0,0.743,0.257) | (0,0,0.654,0.346,0) | (1,0,0,0,0) | (0,0,0.933,0.067,0) | (0,0,0,0.743,0.257) |
| E22(1) | (0,0,0.123,0.877,0) | (0,0,0,0.816,0.184) | (0.422,0.578,0,0,0) | (1,0,0,0,0) | (0,0,0,0.060,0.940) |
| E23(1) | (1,0,0,0,0) | (0,0,0,0,1) | (0,0.303,0.697,0,0) | (0,0,0.841,0.159,0) | (0.557,0.443,0,0,0) |
| E24(1) | (1,0,0,0,0) | (0,0.765,0.235,0,0) | (0.388,0.612,0,0,0) | (0,0,0.571,0.429,0) | (0.388,0.612,0,0,0) |
| E25(1) | (0,0,0,0.080,0.920) | (0,0,0,0.462,0.538) | (0,0,0,0.865,0.135) | (0,0,0,0,1) | (0.749,0.251,0,0,0) |
| E31(1) | (0,0,0,0.719,0.281) | (0.782,0.218,0,0,0) | (1,0,0,0,0) | (0.323,0.677,0,0,0) | (0.778,0.222,0,0,0) |
| E32(1) | (0,0,0.986,0.014,0) | (0,0,0.621,0.379,0) | (0,0,0.200,0.800,0) | (0,0,0.845,0.155,0) | (0,0,0.587,0.413,0) |
| E33(1) | (0.354,0.646,0,0,0) | (1,0,0,0,0) | (0.326,0.674,0,0,0) | (0,0,0.519,0.481,0) | (0,0,0.718,0.282,0) |
| E41(1) | (1,0,0,0,0) | (0,0,0,0,1) | (0,0.862,0.138,0,0) | (0,0.263,0.737,0,0) | (0,0,0.537,0.463,0) |
| E42(1) | (0,0,0.055,0.945,0) | (0,0,0,0,1) | (0,0.955,0.045,0,0) | (0,0,0,0.630,0.370) | (0,0,0.486,0.514,0) |
| E43(1) | (0,0.974,0.026,0,0) | (0,0,0,0,1) | (0.608,0.392,0,0,0) | (0,0.845,0.155,0,0) | (0,0.974,0.026,0,0) |
| E11(2) | (0.604,0.396,0,0,0) | (0,0,0,0,1) | (0,0,0,0.791,0.209) | (0,0,0.899,0.101,0) | (0,0,0.016,0.984,0) |
| E12(2) | (0,0,0,0,1) | (0,0,0.805,0.195,0) | (0,0,0.240,0.760,0) | (0,0,0.971,0.029,0) | (0,0,0,0.514,0.486) |
| E21(2) | (0,0,0.480,0.520,0) | (0,0,0,0.751,0.249) | (0,0,0,0.132,0.868) | (0,0,0.022,0.978,0) | (0,0,0,0,1) |
| E22(2) | (0,0,0,0.347,0.653) | (0,0,0.489,0.511,0) | (1,0,0,0,0) | (0,0,0.270,0.730,0) | (0.632,0.368,0,0,0) |
| E23(2) | (0,0,0,0.230,0.770) | (0,0,0,0.897,0.103) | (0,0,0.200,0.800,0) | (0,0,0,0,1) | (0,0,0.740,0.260,0) |
| E22(2) | (0,0,0.214,0.786,0) | (0,0,0,0,1) | (0.500,0.500,0,0,0) | (0.028,0.972,0,0,0) | (0.301,0.699,0,0,0) |
| E32(2) | (0,0,0.281,719,0) | (0.703,297,0,0,0) | (1,0,0,0,0) | (0,0,0,0,1) | (0,0,0,0.292,0.708) |
| E33(2) | (0,0,0.338,0.662,0) | (0,0,0,0,1) | (0.634,0.366,0,0,0) | (1,0,0,0,0) | (0.711,0.289,0,0,0) |
| E34(2) | (0.781,0.219,0,0,0) | (0.035,0.965,0,0,0) | (0.516,0.484,0,0,0) | (0,0,0.200,0.800,0) | (0.553,0.447,0,0,0) |
| E11(3) | (0.423,0.577,0,0,0) | (0,0,0,0.365,0.635) | (0,0,0,0,1) | (0,0,0,161,0.839) | (0,0,0,0.586,0.414) |
| E12(3) | (0,0,0,0.339,0.661) | (1,0,0,0,0) | (0.136,0.864,0,0,0) | (0,0,0,0.406,0.594) | (0.005,0.995,0,0,0) |
| E13(3) | (0,0.866,0.134,0,0) | (0,0,0.200,0.800,0) | (0.079,0.921,0,0,0) | (0.546,0.454,0,0,0) | (0,0,0.243,0.757,0) |
| E21(3) | (0,0,0.841,0.159,0) | (0,0,0.033,0.967,0) | (0,0,0,0.789,0.211) | (0,0,0,0.302,0.698) | (0,0.826,0.174,0,0) |
| E22(3) | (0.432,0.568,0,0,0) | (0.182,0.818,0,0,0) | (0,0.899,0.101,0,0) | (0,0,0.537,0.463,0) | (0,0,0,0,1) |
| E23(3) | (0,0,0.966,0.034,0) | (0,0,0.334,0.666,0) | (0,0,0.309,0.691,0) | (0,0,0,0.090,0.910) | (0,0.080,0.920,0,0) |
| E31(3) | (0,0,0.106,0.894,0) | (0,0,0,0,1) | (0.320,0.680,0,0,0) | (0.778,0.222,0,0,0) | (0,0,0,0.890,0.110) |
| E32(3) | (0,0,0,0.805,0.195) | (0,0,0,0.079,0.921) | (0,0,0,0,1) | (0,0,0,0.629,0.371) | (0,0,0,0.572,0.428) |
| E33(3) | (0,0,0,0.350,0.650) | (0.920,0.080,0,0,0) | (0,0,0.585,0.415,0) | (0.346,0.654,0,0,0) | (0,0,0,0,1) |
| E11(4) | (0.433,0.567,0,0,0) | (0.939,0.061,0,0,0) | (0,0,0,0.650,0.350) | (0,0.830,170,0,0,0) | (1,0,0,0,0) |
| E12(4) | (0.555,0.445,0,0,0) | (0,0,0.216,0.784,0) | (0,0,0,0.880,0.120) | (1,0,0,0,0) | (0,0,0.080,0.920,0) |
| E13(4) | (0,0,0.200,0.800,0) | (0,0,0.876,0.124,0) | (0.306,0.694,0,0,0) | (0,0.589,0.411,0,0) | (1,0,0,0,0) |
| E14(4) | (1,0,0,0,0) | (0,0.852,0.148,0,0) | (0,0,0,0,1) | (0.670,0.330,0,0,0) | (0,0.313,0.687,0,0) |
| E21(4) | (0,0,0,0.073,0.927) | (0,0,0,0.913,0.087) | (0,0,0,0.992,0.008) | (0,0,0.203,0.797,0) | (0,0,0,0.852,0.148) |
| E22(4) | (0,0,0.654,0.346,0) | (0,0,0,0.918,0.082) | (0,0,0.894,0.106,0) | (0,0,0,0.492,0.508) | (0,0,0.336,0.664,0) |
| E31(4) | (0,0,0.637,0.363,0) | (0,0,0,0.412,0.588) | (0.569,0.431,0,0,0) | (0.877,0.123,0,0,0) | (0.461,0.539,0,0,0) |
| E32(4) | (0,0,0,0,1) | (0,0,0.064,0.936,0) | (0.452,0.548,0,0,0) | (0,0,0,0.847,0.153) | (0.262,0.738,0,0,0) |