
Abstract
BACKGROUND:
Few studies exist that have evaluated the effects of indomethacin dosing frequency as a factor associated with successful patent ductus arteriosus closure in very low birth weight neonates. The objective of this study is to determine if indomethacin dosing strategy is associated with efficacy for initial patent ductus arteriosus management in very low birth weight neonates.
METHODS:
This retrospective review compared every 12 hour and every 24 hour indomethacin regimens primarily for efficacy in initial patent ductus arteriosus management, defined as an absence of repeat medical and/or surgical treatment, and secondarily for safety in both univariate and multivariate models.
RESULTS:
One hundred three very low birth weight neonates were included: 56 (54%) received every 12 hour and 47 (46%) underwent every 24 hour indomethacin dosing. Repeat medical and/or surgical patent ductus arteriosus treatment rates were similar between groups. Less ligation of the patent ductus arteriosus occurred with every 12 hour versus every 24 hour dosing (11% vs. 26%, p = 0.05), though this effect was mitigated controlling for birth weight and gestational age. Renal function, respiratory outcomes, feeding outcomes, length of stay, and mortality were similar between groups.
CONCLUSIONS:
Neither the every 12 hour nor the every 24 hour indomethacin regimen demonstrated inferior efficacy or safety for initial management of patent ductus arteriosus. Further prospective analysis of indomethacin dosing strategy is warranted.
Introduction
Patent ductus arteriosus (PDA) is a common diagnosis in very low birth weight (VLBW) neonates [1 –3]. Shunting of blood across the PDA affects both pulmonary and systemic circulation, resulting in pulmonary overcirculation and decreased systemic perfusion [3, 4]. Given the significant morbidity and heightened mortality associated with PDA [3 , 6], medical and/or surgical closure of PDA remains a relatively common practice in the neonatal intensive care unit (NICU) [4 , 8].
Over the last several decades, multiple studies have assessed the effects of early closure of hemodynamically-significant PDA on numerous neonatal outcomes [2 , 9]. However, PDA management remains an area of significant controversy. Currently, indomethacin, a cyclooxygenase inhibitor which diminishes prostaglandin-mediated maintenance of ductal patency, remains a commonly used drug for medical PDA closure [2 , 10–12].
In VLBW neonates, several studies have evaluated the effectiveness of different indomethacin dosing strategies for PDA closure. Knight et al. (2006) noted improved PDA closure rates with an extended course of indomethacin (6–7 days) compared to a 2–3 dose regimen, though multiple adverse outcomes were not evaluated in this study [2]. Furthermore, Jegatheesan et al. (2008) showed that high-dose indomethacin did not improve PDA closure rates compared to standard dosing [13]. Currently, no studies have evaluated the effects of indomethacin dosing frequency as a factor associated with successful PDA closure in VLBW neonates.
In our institution, indomethacin is administered as a three-dose course (0.2 mg/kg/dose), given either every 12 hours (q12h) or every 24 hours (q24h) based on clinician preference. As no specific rationale has been identified for choice between q12h and q24h regimens, we sought to determine whether either regimen demonstrates superiority with regard to efficacy and safety for initial PDA closure following a single treatment course. We hypothesized that the q12h regimen would demonstrate noninferiority for PDA closure compared to the q24h dosing regimen.
Patients and methods
A single-center retrospective chart review was conducted among VLBW neonates to compare q12h and q24h indomethacin dosing regimens for the primary outcome of successful initial PDA management following a single 3-dose course. Stony Brook University School of Medicine Institutional Review Board approval was obtained for this minimal risk study.
Subjects
Data were collected from electronic medical records by the primary investigators for neonates admitted to the Stony Brook Children’s Hospital NICU from July 2010 through July 2015. Subjects receiving indomethacin were identified via Stony Brook Children’s Hospital Pharmacy and Stony Brook NICU-Specific Regional Perinatal Center database searches. Included subjects consisted of VLBW neonates (<1500 g birth weight) who received at least two doses of indomethacin (0.2 mg/kg/dose) as medical therapy for PDA management. Neither ibuprofen nor acetaminophen were used for medical PDA management in any subject during the study period. No infants received indomethacin for intraventricular hemorrhage prophylaxis, as this was not routine practice at Stony Brook Children’s. Neonates with major congenital anomalies, complex congenital heart disease, death within the first 3 postnatal days, and incomplete electronic data were excluded.
PDA assessment/outcomes/analysis
Initial PDA screening guidelines included echocardiograms obtained in all infants with birth weight <1000 g. For neonates with birth weights of 1001–1500 g, echocardiograms for PDA screening were obtained based on attending discretion. Screening echocardiograms were obtained most often between the third and fifth postnatal day. Echocardiographic determinants of hemodynamic significance included PDA size (qualitatively reported as small, moderate, or large) and quality of flow (qualitatively described as non-restrictive versus restrictive). Individual treatment decisions for suspected hemodynamically-significant PDA were based on a combination of clinical and echocardiographic data and were additionally determined based on NICU clinician discretion. Parameters such as BUN, creatinine, platelets, and other clinical data were routinely evaluated by clinicians with regard to PDA-related treatment decisions.
The primary outcome was successful initial medical management of PDA. In this retrospective study, this was indirectly defined as no additional indomethacin administered (following a single 3-dose course) and no PDA ligation performed. Follow-up echocardiograms were not routinely obtained following initial indomethacin therapy. The decision to repeat an echocardiogram was also based on attending discretion, most frequently due to ongoing clinical evidence of hemodynamically-significant PDA. Based on this PDA management strategy, the lack of further indomethacin treatment courses and absence of PDA ligation were assumed as surrogate indicators of successful initial PDA management.
Given the controversial nature of PDA management and our retrospective study design, a robust list of secondary outcomes were additionally analyzed as proxy measures for comparisons between neonates receiving q12h versus q24h indomethacin courses. These secondary outcomes included acute kidney injury (based on elevated creatinine levels from baseline) [14], changes in platelet counts, intraventricular hemorrhage (modified Papile grading method) [15], spontaneous intestinal perforation, duration of parenteral nutrition, necrotizing enterocolitis, ventilator and oxygen days, bronchopulmonary dysplasia (based on presence of oxygen requirement at 28 days of life) [16], length of stay, and mortality. Importantly, screening for intraventricular hemorrhage was performed at birth, 7 days, and 30 days with more frequent studies if indicated. All neonates were screened prior to initiation of indomethacin treatment per unit guideline. There was no set guideline for stopping enteral feeds during indomethacin management, except per clinician discretion, though neonates were not advanced on enteral feeds during treatment.
Preliminary review retrospectively extending to the inception of electronic medical records at our institution identified 103 VLBW indomethacin recipients who met the inclusion criteria, consisting of 56 (54%) who received the q12h regimen and 47 (46%) who received q24h dosing. On power analysis for study sample size calculations, this subject distribution was determined sufficient to demonstrate up to a 30% effect size for the primary outcome of successful initial medical management of PDA between groups to demonstrate noninferiority with 80% power and 2-tailed alpha of 0.05. Given the retrospective nature of this project, power analyses were not additionally performed for the secondary outcomes as listed above. Lastly, given incomplete indomethacin treatment courses in some subjects, analyses were performed both among all subjects and excluding those receiving less than three initial doses. Statistical analyses included Student t-test (following confirmation of normal distributions), chi square, and multivariate linear regression where applicable based on between-group comparisons.
Results
Demographic information among VLBW neonates receiving indomethacin for initial PDA management
Demographic information among VLBW neonates receiving indomethacin for initial PDA management
Data displayed as Mean±SD (median; IQR) or number (%).
The combined surrogate measure of successful PDA management, lack of additional medical and/or PDA ligation, was observed more frequently in the q12h group (43/56 (77%) versus 26/47 (55%), p = 0.04; see Fig. 1), though this effect was mitigated when controlling for birth weight and gestational age (p = 0.16). Individually, no difference between q12h and q24h indomethacin treatment groups were observed regarding repeat medical PDA management. However, less PDA ligation was demonstrated with the q12h dosing regimen (6/56 (11%) versus 12/47 (26%), p = 0.05), an effect also mitigated when controlling for birth weight and gestational age (p = 0.09). Repeat medical therapy and PDA ligation data are demonstrated graphically in Fig. 2.
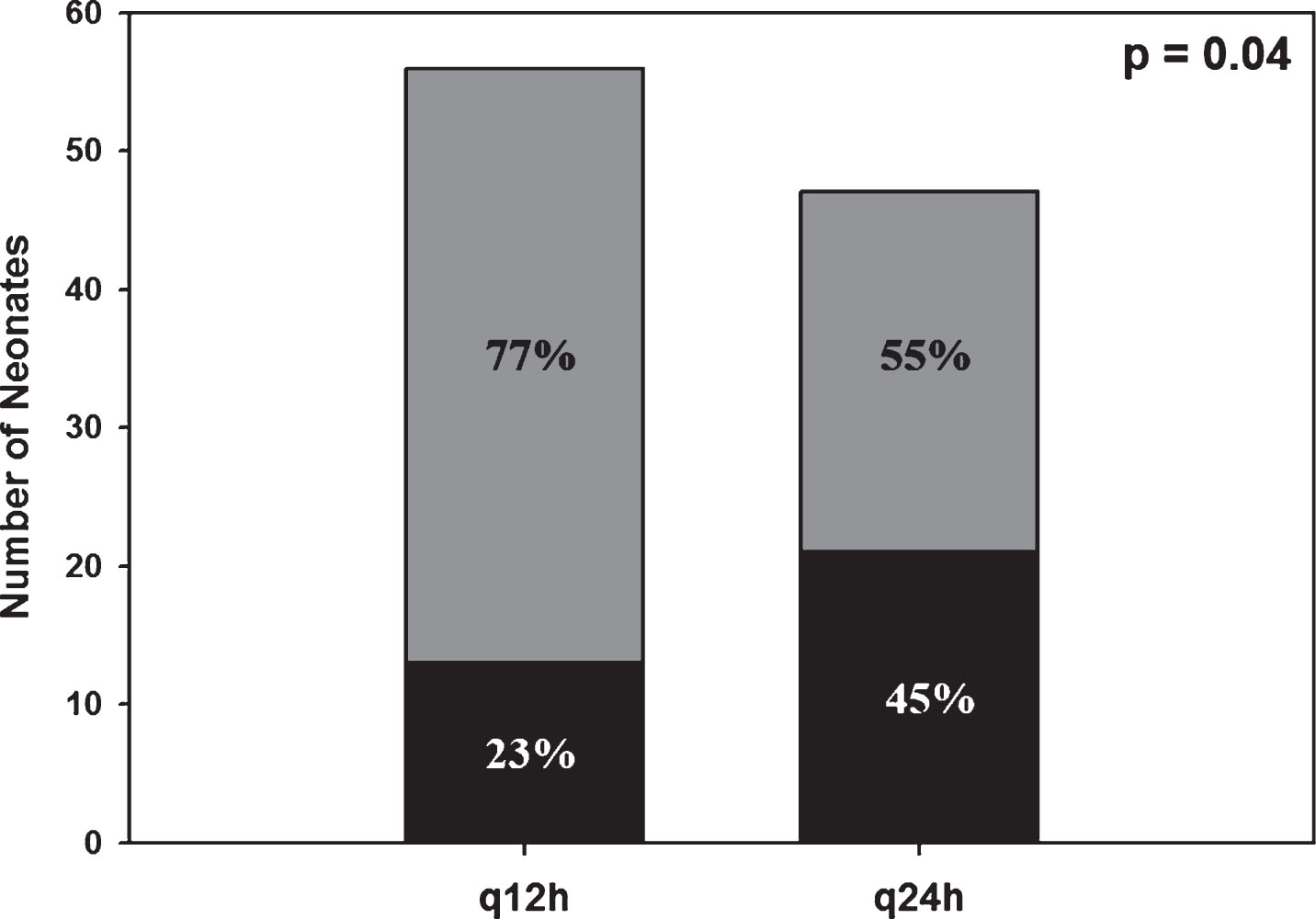
Combined repeat indomethacin dosing and/or PDA ligation comparing q12h and q24h indomethacin dosing strategies. In each graph, the proportion of subjects who received either repeat indomethacin courses and/or PDA ligation is represented in black.
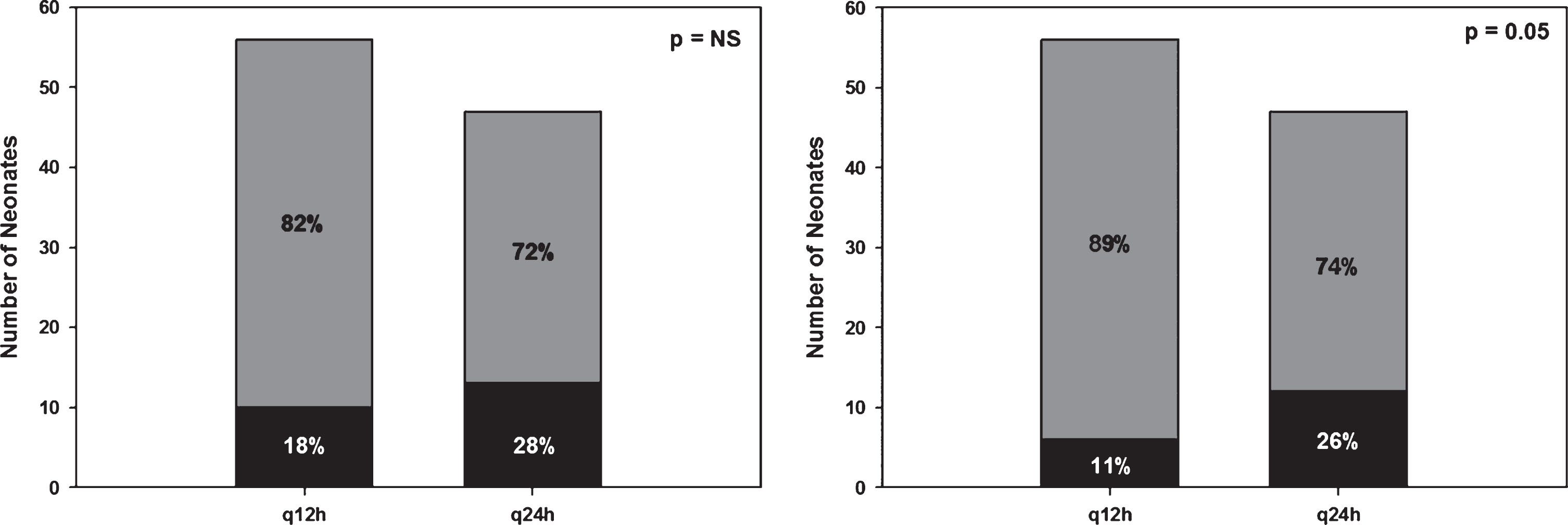
Individual repeat indomethacin dosing (left panel) and PDA ligation (right panel) graphs comparing q12h and q24h indomethacin dosing strategies. In each graph, the proportion of subjects who received either repeat indomethacin courses or PDA ligation is represented in black.
Increases in BUN and creatinine from baseline were observed in both groups during treatment (p = 0.01), though the degree of increase was not statistically different between groups (Fig. 3). Mean platelet counts demonstrated no changes during treatment in either group and were not statistically different between groups either before or following initial indomethacin courses. No additional differences were observed between groups with regard to multiple secondary outcomes, as summarized in Table 2.
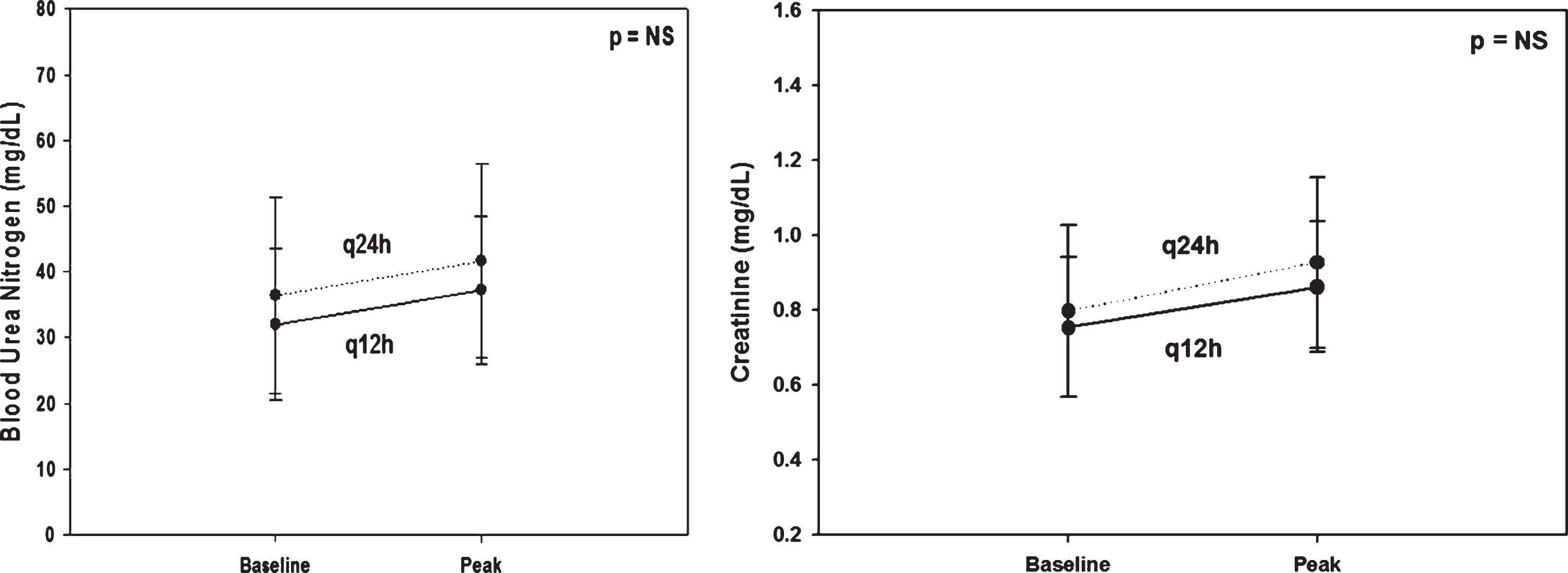
Change in mean (±SD) blood urea nitrogen (left panel) and creatinine (right panel) from baseline comparing q12h to q24h indomethacin dosing regimens. The solid line represents q12h dosing whereas the dashed line represents the q24h indomethacin regimen. Increases in both BUN and creatinine from baseline were observed in both groups, though the magnitude of change was not significantly different between groups.
Clinical outcomes among VLBW neonates receiving indomethacin for initial PDA management
Data displayed as Mean±SD (median; IQR) or number (%).
In this retrospective study, neither the q12h nor q24h indomethacin regimen demonstrated inferior efficacy for initial PDA management. In addition, there was no apparent safety benefit favoring either indomethacin dosing regimen. Though no specific rationale has been identified for choice between q12h and q24h regimens, in this cohort more premature, smaller, and sicker babies received the q24h indomethacin dosing regimen.
Management of PDA remains an important area of inquiry in the neonatal population [17–19 , 25]. While previous studies have demonstrated significant morbidity and mortality among preterm neonates with PDA [3], specific treatment strategies remain an area of active investigation [6 , 25]. Currently, indomethacin remains a commonly used medication for PDA management given its effectiveness in achieving PDA closure and decreasing the need for surgical ligation [22 –24]. However, relatively limited data exist concerning specific indomethacin dosing strategies, including dose, interval, and treatment duration [2 , 25]. Insufficient data also exists regarding the benefits of early versus late treatment for PDA, along with the clinical effects of long-term ductal patency [25]. Robust investigations are needed to create improved guidelines for managing PDA in preterm neonates [25]. At present, no specific data has been reported comparing indomethacin dosing intervals, resulting in practice variability as seen in this report.
Our data set demonstrates a selection of q24h indomethacin dosing among more premature, smaller, and sicker neonates compared to those selected for q12h dosing. While the specific factors behind this decision are not available in this retrospective study, it seems feasible that patient safety-related concerns may have contributed to this selection. Nevertheless, similar efficacy outcomes were observed for the q12h and q24h dosing strategies, with neither regimen appearing to confer inferior safety.
Significant limitations exist in this retrospective study with regard to assignment of indomethacin treatment regimen. As above, factors specifically contributing to dosing regimen selection were not available to be explored. In addition, criteria to describe hemodynamically-significant PDA need to be clearly defined for future studies. In our practice, no specific changes in indomethacin dosing strategies occurred during the time period from which these data were accrued. Moreover, while no apparent pattern for choice of indomethacin regimen was observed, ongoing controversy regarding the need for medical and/or surgical PDA management likely influenced overall PDA management decisions during this study. Additionally, by dividing groups solely based on indomethacin dosing interval, additional factors influencing PDA-related outcomes, including fluid management decisions, could not be accounted for. Finally, this study cannot fully account for ongoing changes in neonatal practice (i.e., antenatal steroid therapy, neonatal resuscitation changes) that occurred during this study’s 5 year data collection interval.
Furthermore, as follow-up echocardiograms were not routinely obtained following initial indomethacin therapy, we needed to rely on additional indomethacin dosing beyond the first course and/or PDA ligation as surrogate measures of successful initial medical PDA management. In addition, as decisions regarding additional indomethacin courses and/or PDA ligation were also based on multiple case-specific clinical factors, whether indomethacin dosing interval actually influences initial PDA management efficacy remains to be proven. Clearly, prospective analysis including clear treatment criteria and incorporating pre-and post-treatment qualitative and quantitative echocardiographic data is required to further delineate the effect of indomethacin dosing regimen on successful initial PDA closure. Finally, this study was not able to assess long-term neurodevelopmental outcomes among neonates based on which course of indomethacin they received. A prospective study investigating neurodevelopmental outcomes related to indomethacin treatment course would benefit future clinicians.
The management of PDA in VLBW neonates remains an area of ongoing inquiry and controversy. While other therapies (e.g., ibuprofen, acetaminophen) now exist for the treatment of hemodynamically-significant PDA, indomethacin remains a common medication utilized to facilitate PDA closure [6, 21]. In this retrospective analysis, neither the q12h nor the q24h indomethacin regimen demonstrated inferior efficacy or safety. Prospective studies are needed to assist in establishing an indomethacin regimen that will optimize the risk/benefit ratio of this medication for future VLBW neonates.
Financial disclosures
The authors of this study have no financial disclosures.
Footnotes
Acknowledgments
We would like to extend our appreciation to the Stony Brook Children’s Neonatology Faculty, Nurses, Staff, and the Pediatrics Residency Research Committee for supporting this research project.