
Abstract
BACKGROUND:
In preterm infants, persistence of ductus arteriosus is an important medical condition. Functional echocardiography for patent ductus arteriosus (PDA) may guide clinical decision-making regarding treatment requirement strategies. Objectives of the study were to assess the trends of clinical and functional echocardiographic parameters with evolution of ductus arteriosus in babies≤1250 gm of birth weight and to evaluate whether there is any association of these parameters with persistence of ductus.
METHODS:
In this prospective observational study, recruited babies were assessed serially for clinical events and functional echocardiography. Babies were classified into three groups: without PDA, with PDA but PDA spontaneously closed (within 7 days) and persistent PDA.
RESULT:
We included 143 infants (Birth weight 1017±179 g, gestational age 30.8±2.7 weeks). Out of 60 babies with PDA, PDA failed to close spontaneously in first week in 32 (53.4 %) infants. PDA Doppler flow pattern on day 3 was found to be one of the most significant markers for future ductus. The highest frequency of growing pattern (37.5%) and pulsatile pattern (59.4%) was seen in persistence ductus group. PDA diameter and LA/Ao ratio were found strongly correlated with all other variables except E/A ratio.
CONCLUSION:
We noticed persistence of ductus in preterm infants had significant clinical and echocardiographic association. PDA doppler flow pattern on day 3 was found to be a significant marker for future behaviour of ductus. Significant correlation was found among individual functional echocardiographic parameters in babies with PDA. This would guide judicious treatment of PDA in preterm neonates.
Introduction
Patent ductus arteriosus (PDA) is a major clinical problem in preterm, especially in babies less than 1000 gm or 28 weeks of gestation. PDA closes spontaneously in 34–40%of babies less than 28 weeks of gestational age and/or birth weight of less than 1000 g [1, 2]. Echocardiography is the gold standard for diagnosing PDA. Pathological PDA increases the risk of chronic lung disease (CLD), necrotizing enterocolitis (NEC), intra ventricular hemorrhage (IVH), and death [3–5]. But the association is difficult to interpret depending on the variability of incidence of PDA, which further depends on timing of echocardiography, diagnostic criteria used [6] and characteristics of the population studied. Cochrane reviews have proved that treatment of PDA reduces ductal patency only at the cost of some renal or gastrointestinal side-effects but lack evidence of consistent effect [7–13]. So, when to treat PDA is really a matter of debate, especially for very low birth weight (VLBW) babies [14]. Though the guideline is clear-cut for extremely premature population, selection of candidates for closure with drugs versus conservative treatment sometimes becomes difficult. Functional echocardiography performed by neonatologist for study of PDA hemodynamics is now practiced in few centers [15, 16].
There is dearth of evidences in literature regarding the course and impact of PDA and the role of point -of- care functional echocardiography in neonatal intensive care units (NICU) [17, 18].We need more prospective studies on preterm PDA for natural evolution and role of functional echocardiography parameters to identify the ideal subset for treatment. The primary objective of this study was to identify the clinical and functional echocardiographic parameters associated with the evolution of ductus arteriosus in babies less than equal to birth weight of 1250 gm. Secondarily, this study also aimed to assess clinic -echocardiographic determinants of future persistent PDA and inter-parameter correlation of functional echocardiographic markers of preterm PDA.
Methodology
This study was done as a prospective, longitudinal, observational study in a level 3 NICU of a medical college in India from February 2014 to January 2016. Any baby with birth weight less than or equal to 1250 gm, born in this hospital and admitted in NICU during the study period were included in the study. Informed consent was taken from the parents/caregiver before enrolment. The babies with major congenital anomalies, congenital heart disease were excluded from the study. Echocardiographic examination was done by PHILLIPS ENVISOR C Echocardiography unit with neonatal probe S12 (12 to 4 MHz extended frequency range) on day 3 for determination of ductus status followed by twice weekly till day 10 of life and weekly afterwards to detect spontaneous closure before endpoint of death or discharge in case of patent PDA. The images were recorded by one of the investigators who was a neonatologist trained in functional echocardiography. The images were subsequently reviewed and confirmed by another investigator who was a cardiologist. Treatment was done with ibuprofen orally or intravenous paracetamol if oral drug was contraindicated. Oral paracetamol was used in case of treatment failure with ibuprofen.
Babies were followed up as different subgroup related to PDA: without PDA (Group I), with PDA but PDA spontaneously closed (within 7 days) (Group II) and persistent PDA (beyond 7 days) (Group III) for comparison to document the evolution of PDA.
Parameters of evaluation
Clinical parameters
Other than demographic profile, clinical history like perinatal asphyxia (In cord blood gas or venous blood gas within 1 hour of birth, base deficit < -6, gasping or no respiration at birth and requirement of positive pressure ventilation), maximum fluid intake (ml/kg /day) in first 7 days, culture confirmed sepsis, clinical sepsis (clinical symptoms suggestive of sepsis and treated with antibiotics for at least 7 days), duration of phototherapy (in hours) were noted for each recruited babies.
We also recorded various clinical events like presence of tachycardia (> 160/min) persisting more than 24 hours and not explained by causes other than ductus, systolic murmur,wide pulse pressure (> 30 mm Hg), requirement of any form of respiratory support, duration of mechanical ventilation, duration of any respiratory support (invasive or noninvasive), duration of ‘nothing per mouth’(NPM) in days, time to reach full feeds, presence of shock with requirement of inotropes, presence of moderate to severe metabolic acidosis (pH < 7.1 or base deficit < -12) and presence of abnormal X ray (pulmonary congestion or edema or cardiomegaly) for each recruited baby.
Functional echocardiographic parameters [19–22]
Day 3 echocardiogram was recorded for analysis. The functional echocardiographic parameters like the transductal diameter of PDA (mm), peak ductal flow velocity (left to right) in cm/sec (Vmax, PDA), peak velocity of left pulmonary artery antegrade diastolic flow (LPA diastolic flow), ratio of Left atrium and aortic root diameter in M mode (LA/Ao), ratio of left ventricular end diastolic dimension and aortic root diameter in M mode (LV/Ao), E/A ratio of trans mitral E and A velocity (E/A ratio), Intra ventricular relaxation time (IVRT, ms), Left ventricular output (ml/kg/min)(LVO), Ratio of left ventricular output and Superior vena caval flow (LVO/SVC ratio) and Doppler flow pattern: pulmonary hypertension, bidirectional, growing pulsatile and closing were recorded.
Outcome analysis
Requirement of treatment for PDA, success or failure of treatment, death during hospital stay, bronchopulmonary dysplasia (BPD) (as defined by Jove and Banchalari, 2001) [23], Necrotizing Enterocolitis (NEC)≥stage 2 (Modified Bell’s criteria, 1987) [24], Intraventricular Hemorrhage (IVH) > grade 2 (graded by Papile et al., 1978) [25] were recorded as outcome parameters.
Statistical analysis
Data was summarized by descriptive statistics. Continuous variable was expressed in either mean and SD or median and IQR or range. Categorical variable was expressed in percentage. For univariate analysis, continuous variables were compared between groups by One-way Anova test or Kruskal Wallis H test depending on the normality along with relevant post hoc tests (Tukey’s Honest Significance Difference Test). Pearson’s Chi-square test was employed for intergroup comparison of categorical variables. Pearson correlation coefficient test was applied for finding out inter-parametric relationship between various echocardiographic variables.
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Institutional Ethics Committee (Inst/IEC/644 dated 03.03.2014).
Result
Total 143 neonates were enrolled for the study (Table 1) (Fig. 1). PDA was detected in 60 babies. PDA failed to close spontaneously in first week in 32 (53.4 %) babies. Among babies with PDA, systolic murmur was present in 50 %of babies. Persistent tachycardia, wide pulse pressure, apnea > 6 episodes / day and feed intolerance were recorded in 40 (66.6%), 38(63.3 %), 25 (41.7%) and 22 (36.7%) babies respectively. Moderate to severe metabolic acidosis and shock were found in 20 (33.3%) and 22 (36.7%) babies. In 15 babies (25%) there were feature of pulmonary congestion and cardiomegaly in chest x-ray.
Clinical profile of the study population
Clinical profile of the study population
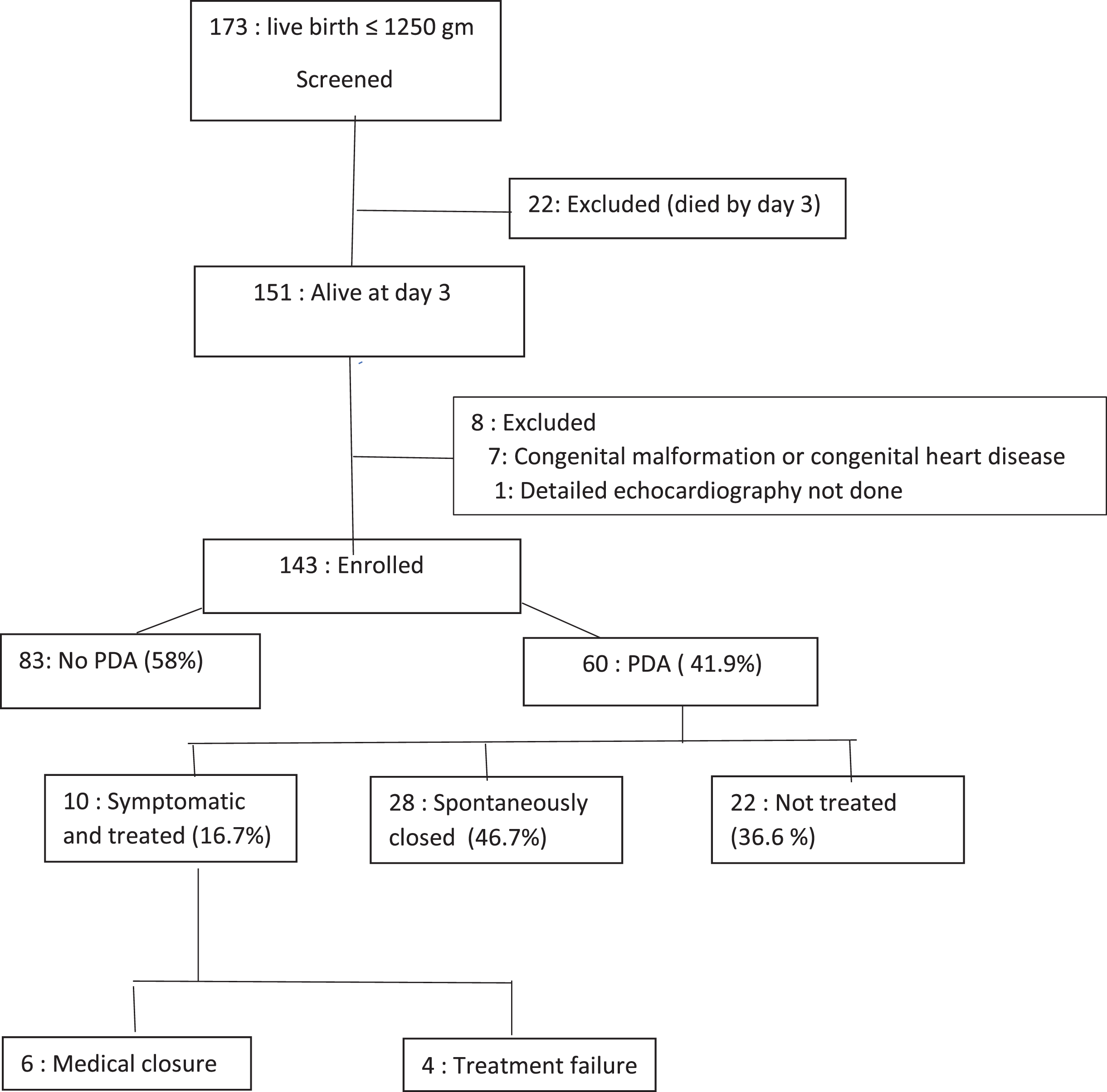
Flow chart of the study population and the evolution of PDA.
The association of the ductus arteriosus in relation to the clinico-epidemiological factors and functional echocardiographic parameters were analyzed by categorizing the babies in 3 groups: group I –without PDA (n = 83); group II spontaneously closed PDA (n = 28); group III –persistent PDA (n = 32) (Table 2).
Comparison of clinical parameters among three groups
*Significance of difference between group I and group II. †Significance of difference between group II and group III. ‡Significance of difference between group I and group III.
Functional echocardiography parameters: The echocardiographic parameters showed consistent increasing trend for parameters like PDA diameter, LPA diastolic velocity, La/Ao, LV/Ao, E/A, LVO and LVO/SVC and consistent decreasing trend for IVRT and PDA Vmax from Group I to Group III with Group III (persistent ductus) having the most severe parameters. There was statistically significant difference of mean for all parameters among different groups. Closing pattern of PDA was seen more in group II than group III (60.7 %vs 3.1%). The highest frequency of growing pattern (37.5%) and pulsatile pattern (59.4%) was seen in babies of Group III. The overall flow pattern analysis showed statistically significant association with between babies with closed ductus and babies with persistent ductus.
Pearson correlation coefficient among different echocardiographic variables in babies with PDA was presented in Table 4. PDA diameter and LA/Ao ratio were found strongly correlated with all other variables except E/A ratio. Newer parameters like LVO/SVC ratio were well correlated with all other variables except LV/Ao ratio.
Pearson correlation of functional echocardiographic parameters
**Correlation is significant at the 0.01 level (2-tailed). *Correlation is significant at the 0.05 level (2-tailed). (Vmax = peak velocity, LPA = left pulmonary artery, LA/Ao = left atrium and aortic root diameter ratio, LV/Ao = left ventricle and aortic root diameter ratio, E/A = Transmitral E and A wave velocity ratio, IVRT = intraventricular relaxation time, LVO = left ventricular output, LVA/SVC = left ventricular and SVC out put ratio).
The behavior of patent ductus arteriosus in preterm newborn was extensively observed in the present study. There are very few published literatures that have prospectively assessed the pattern and evolution of the preterm PDA with echocardiography [17, 27]. We selected babies below 1250 gm since infants above that weight rarely pose a significant clinical problem. In the majority of cases, the conservative approach of management of PDA was followed by our clinician; hence our study has got the potential to represent the natural evolution and morbidity profile of preterm population, unbiased from the effect of early treatment.
In our study, the incidence of PDA was 41.9%on day 3 of life. The incidence of PDA among babies≤29 weeks was found as 58.8%. The incidence was somewhat lower than that reported in published literature [28] but comparable with the published study from the LMIC [17]. The result was also comparable with the review by Reller et al. [29] who reported an incidence of PDA on day 3 around 50 %of babies≤29 weeks. Our study observed a spontaneous closure rate of 46.7 %which is somewhat higher than that reported in the studies by Visconti et al. [18], Afiune et al. [17] and Koch et al. [30] (5–33%). High rate of spontaneous closure can be explained by large number of small for date babies in the present study.
Like previous studies, the lower birth weight and gestation were significantly more associated with occurrence and persistence of preterm PDA [30]. In univariate analysis, perinatal asphyxia, RDS and clinical sepsis became significant risk factors for occurrence and persistence of ductus that corroborated the result of the previous studies by Visconti et al. [18] and Reller et al. [29]. This can be explained by increased release of inflammatory mediators which would impair the physiologic closure of ductus.
On the other hand, no association was seen for factors like maternal pregnancy induced hypertension, antenatal steroids, premature rupture of membrane, chorioamnionitis and culture positive sepsis. The poor detection rate of chorioamnionitis, less incidence of culture positive sepsis and very poor coverage of complete antenatal steroid may be the reason behind this.
A significantly more duration of phototherapy among the babies with PDA compared to No PDA was found like the previous studies [31]. Change in systemic circulation and failure of ductal smooth muscle contraction by phototherapy were two hypotheses behind this causal relationship.
Comparison of different functional echocardiography parameters among the groups
Comparison of different functional echocardiography parameters among the groups
(Vmax = peak velocity, LPA = left pulmonary artery, LA/Ao = left atrium and aortic root diameter ratio, LV/Ao = left ventricle and aortic root diameter ratio, E/A = Transmitral E and A wave velocity ratio, IVRT = intraventricular relaxation time, LVO = left ventricular output, LVA/SVC = left ventricular and SVC out put ratio; *Significance of difference between group I and group II, †significance of difference between group II and group III, ‡significance of difference between group I and group III).
Regarding the analysis of clinical features in different subgroup of babies the most striking feature was that whether ductus spontaneously closed or persistent, no difference existed in terms of duration of any mode respiratory therapy, time to reach full feed or duration of NPM. But the babies from both group either persistent PDA or spontaneously closed PDA required more days of ventilation or total respiratory therapy or NPM and more time to reach full feed in comparison to babies with no PDA. It implies ductus either closed by 7 days or persistent beyond that, the impact on the babies is all same and mostly occurs by initial 48–72 hours. So, the efficacy of the conservative approach or late symptomatic approach of treatment of the persistent ductus raises some serious doubt and needs further judgment.
We observed presence of murmur in 53.1 %of the babies with persistent PDA but only in 28.4%of babies whose PDA closed spontaneously later. Obviously, the babies with persistent PDA were found to have significantly higher incidence of symptoms in comparison to other groups (Table 2). The result was comparable with previous studies by Afiune et al. [18] and Kupferschmid et al. [32] which also observed the presence of such clinical features in range of 50–70%. Surprisingly highest incidence of abnormal x-ray was only 25 %even if in persistent PDA group.
Our study also evaluated a wide spectrum of functional echocardiographic parameters. Several studies have data on significant functional echocardiographic markers [18]. We observed a significant difference of echocardiographic markers as early as on day 3 among all the said groups of preterm population which signified the association of the parameters with the persistence of ductus. The three groups seemed to be hemodynamically distinct from each other since early days of life and prior to becoming symptomatic. Therefore, functional echocardiography parameters were important determinants of evolution of PDA.
In the present study, we included a novel parameter like PDA flow pattern done on day 3. Babies with spontaneously closed PDA had mostly the closing pattern (60.7%) where the persistent PDA babies had mostly pulsatile pattern (59.4%) and growing pattern (37.5%). Flow pattern itself was predictive of persistence of PDA as corroborated by a previous work by Su et al. [22].
The results of the functional echocardiographic variables were comparable with the previously published studies by Afiune et al. [17], Viscoti et al. [18] and Khositseth A et al. [26] but none of them incorporated all of the important parameters of interest.
Lastly the study also presented the data on the short-term outcome of morbidities or death during hospital stay. The incidence of death, CLD, NEC≥stage 2, IVH > grade 2, ROP≥stage 2 was significantly higher in persistent ductus group. Again, the incidence of death, CLD, NEC≥stage 2, IVH > grade 2, ROP≥stage 2 was increasing from group I to group II and group II to group III significantly which was also evident in the literatures [3, 27].
The study demonstrated strong interparametric correlation among echocardiographic parameters which is rarely found in previous literature. One such retrospective study by Sehgal A et al. [33] similarly showed correlation of ductal diameter with other indices but correlation of all the parameters among themselves have been presented here for the first time.
There are few limitations of the study. The recruitment procedure of this study was not dictated by proper sample size calculation, rather done by sample of convenience where consecutively babies were recruited in a time frame. The investigators were not blinded to the decision of the treatment by clinical team. The strength of our study that it prospectively recorded all the related clinico-echocardiographic parameters in a preterm birth cohort and to our knowledge very few prospective studies have included larger cohort of babies with comparable gestational age from single unit.
Our study has set a standard of various clinical and echocardiographic markers in relation with PDA among babies ≤< 1250 g of birth weight. The selective clinical and early functional echocardiographic markers were found significantly associated with future persistence of ductus. PDA Doppler flow pattern on day 3 was found to be one of the most significant markers for future behavior of the ductus. Significant correlation was found among individual functional echocardiographic parameters in babies with PDA.
Source of funding
No funding required.
Disclosure statements
The authors declare that there are no proprietary, financial, professional or other personal conflict of interests. The research involving human subjects submitted to the journal was conducted in accordance with the ethical standards of institutional ethics committee and the World Medical Association’s Helsinki Declaration.