
Abstract
OBJECTIVE:
To evaluate the role of functional echocardiography for prediction of patent ductus arteriosus (PDA) closure and development of adverse outcome in very low birth weight newborn.
METHODS AND STUDY DESIGN:
Functional echocardiography was done in 143 neonates with birth weight less than 1250 g on day 3. Nine echocardiographic parameters were analyzed for babies with PDA for prediction of spontaneous closure and development of one or more adverse outcomes (bronchopulmonary dysplasia, necrotizing enterocolitis≥stage 2 and intraventricular hemorrhage > grade 2) during hospital stay.
RESULT:
The mean (±SD) birthweight and gestational age of the cohort were 1017 (±17) g and 30.8 (±2.7) weeks. PDA was found in 60 (41.9%) babies on day 3 among the recruited babies. Binary logistic regression model showed strong prediction ability of early (day 3) functional echocardiography markers in predicting future spontaneous closure of PDA and development of one or more adverse clinical outcome. In multivariate analysis, abnormal flow pattern (growing or pulsatile) was found to have increased risk for persistence of PDA (adjusted OR 22.9, CI 1.97-269) in comparison to PDA with closing/bidirectional pattern.
CONCLUSION:
Early functional echocardiography, especially the flow pattern, is useful for prediction of PDA closure. Adverse clinical outcome prediction is possible with functional echocardiography markers when combined with gestational age and PDA closure status.
Introduction
Patent ductus arteriosus (PDA) is one of the common diagnosis or occurrences in preterm neonate, especially in babies less than 1000 g or 28 weeks of gestation. It is reported in about one third of babies weighing 501–1500 g and almost half of the infants <1000 g require intervention for symptomatic PDA [1, 2]. A clinically significant PDA has been linked to common neonatal respiratory, cardiovascular and gastrointestinal morbidities. There are various treatment strategies for persistent patent ductus like symptomatic or presymptomatic management or even conservative ‘bystander’ approach [3–7]. But neither of the interventions is free from renal, gastrointestinal and respiratory complications nor can show any consistent favorable neurodevelopment outcome [7, 8]. Hence which duct needs intervention and at what point of time is still unanswered [9]. Abnormal hemodynamics of PDA shunt precedes the clinical symptoms of PDA at least by 2-3 days. Functional echocardiography in recent days is utilized at bedside to assess the hemodynamics of PDA shunt even when it is silent clinically [10]. There are different protocols of functional echocardiography to assess different aspects of PDA like PDA morphology and flow pattern as well as myocardial performances, systemic perfusion, and pulmonary over circulation. Use of composite PDA scores with a number of functional echocardiography parameters for staging of the disease or as diagnostic tool for respiratory morbidity and treatment requirement in preterm babies have been found in literature but those studies are few in number, heterogenous and are mostly retrospective in design [10–16]. Practically it is difficult to perform PDA severity scoring or staging always using several parameters at bedside for treatment decision and we need some definite point of care solution. Here we explore a hypothesis generating prospective study in a cohort of very low birth weight newborn especially with birth weight of less than 1250 g in a tertiary care neonatal intensive care unit in India to identify the most significant functional echocardiography parameters as early as on day 3 that can predict future spontaneous closure of PDA and development of adverse outcome like significant necrotizing enterocolitis (NEC), intraventricular hemorrhage (IVH) or bronchopulmonary dysplasia (BPD), so that judicious treatment can be adopted at the earliest.
Methodology
This study was done as a prospective, longitudinal, observational study in the neonatal intensive care unit (NICU) of a tertiary care hospital in Kolkata, India. We have included inborn babies, with birth weight of less than 1250 g, born during February 2014 to January 2016. Informed consent was taken from the parents before enrolment. The babies with major congenital anomalies and congenital heart disease (excluding isolated ductus arteriosus and patent foramen ovale) were excluded.
Participant flow
Recruited babies underwent functional echocardiography examination on day 3 for assessment of PDA. Echocardiography was done by PHILLIPS ENVISOR C Echocardiography unit with neonatal probe S12 (12 to 4 MHz extended frequency range). The images were recorded by one of the investigator who was a neonatologist, trained in functional echocardiography. The images were subsequently reviewed and confirmed by another investigator, cardiologist. Details of functional echocardiography parameters were also recorded on day 3. Further, serial echocardiography was done in babies with PDA daily, to know the whether spontaneous closure occurred by day 7 of life. Alternatively, babies were recorded as having persistent PDA. Babies with no PDA were reviewed with echocardiography till discharge for reopening. Babies with persistent PDA were also evaluated with echocardiography every weekly or as required by the clinical team. The clinical team was blinded to the details of functional echocardiography information and they independently determined whether PDA was symptomatic. They decided to treat PDA when there was cardiomegaly and pulmonary congestion in x-ray along with clinical worsening like difficulty to wean from respiratory support or increase in respiratory support or occurrence of major apnea, feed intolerance, severe shock or acidosis, not explained by any other reasons in presence of a patent ductus with left to right shunt, confirmed by echocardiography. Treatment was done with ibuprofen or paracetamol or with surgical ligation, if medical therapy failed.
The investigators followed the standard protocol of the functional echocardiography for views, image acquisition and recording of parameters.
Data collection and functional echocardiography parameters
Mode of delivery, gender, birth weight, gestational age (by New Ballard score or from maternal record of first trimester ultrasound), intrauterine growth (small for gestational age as defined by birth weight <10th percentile in Lubchenco’s chart), requirement of surfactant, use of invasive mechanical ventilation and ionotropes within first 7 days of life were recorded.
Functional echocardiography parameters were chosen based on clinical relevance as well as evidence from the previous studies [10, 18]. We chose transductal diameter of PDA in millimeters, peak ductal flow velocity (left to right) in cm/sec (Vmax, PDA), peak velocity of left pulmonary artery antegrade diastolic flow in cm/sec (LPA diastolic flow), ratio of left atrium and aortic root diameter in M mode (LA/Ao), ratio of trans mitral E and A velocity (E/A ratio), intra ventricular relaxation time in ms (IVRT), left ventricular output in ml/kg/min (LVO), ratio of left ventricular output and superior vena caval flow (LVO/SVC ratio) and doppler flow pattern of PDA like pulmonary hypertension, bidirectional, growing, pulsatile and closing recorded by 2D, M mode, color doppler and doppler modes for each echocardiography session. We followed the description laid down by Su BH et al. [17] for recording of PDA flow pattern by echocardiography.
We reported spontaneous closure of PDA as primary outcome and adverse clinical outcome during NICU stay as secondary outcome. The adverse clinical outcomes recorded were bronchopulmonary dysplasia (BPD) (as defined by Jove and Banchalari, 2001) [19], necrotizing enterocolitis (NEC)≥stage 2 (Modified Bell’s criteria, 1987) [20] and intraventricular hemorrhage (IVH) > grade 2 (graded by Papile et al. 1978) [21]. We also recorded treatment requirement for PDA and death during hospital stay.
Statistical analysis
Data was recorded in Excel sheets. Statistical analysis was done by SPSS version 21 software. Comparison between two groups of babies was done by Independent sample t test or Mann-Whitney U test for continuous data and Chi-square test for categorical data. Separate Binary logistic regression analysis was done for prediction of spontaneous closure and adverse outcome.
The study was approved by Institutional Ethics Committee (approval no Inst/IEC/644 dated 03.03.2014)
Result
We recruited 173 babies with a birth weight < 1250 gram initially, but 30 babies were excluded due to various reasons as per the exclusion criteria. Among 143 finally enrolled neonates 68 (46.8%) were males and 75 (52.4%) females. The mean (±SD) birth weight and gestation of the population was 1017 (±179) g and 30.8 (±2.7) weeks respectively. Seventy-two babies were small for gestational age (50.3%). Surfactant was required for respiratory distress syndrome in 26.7% of babies. Invasive mechanical ventilation and ionotropes with 7 days of life were required in 18.1% and 16.8% of babies respectively. The incidence of BPD, NEC≥stage 2, IVH > grade 2 and death during hospital stay was 29.5%, 7.9%. 7.7% and 15.4% respectively.
The participant flow was depicted in figure (Fig. 1). Ductus arteriosus was found to be patent on day 3 in 60 babies (41.9%) only. In the final analysis, total 54 babies with PDA on day 3 were included, as 6 babies died with PDA before 7 days. Spontaneous closure by 7 days of life was seen in 28 (51.8%) babies and persistent PDA beyond this age was seen in 26 (48.1%) babies. Pharmacological treatment was required in 10 babies (16.8%) among persistent PDA group for clinical symptoms.
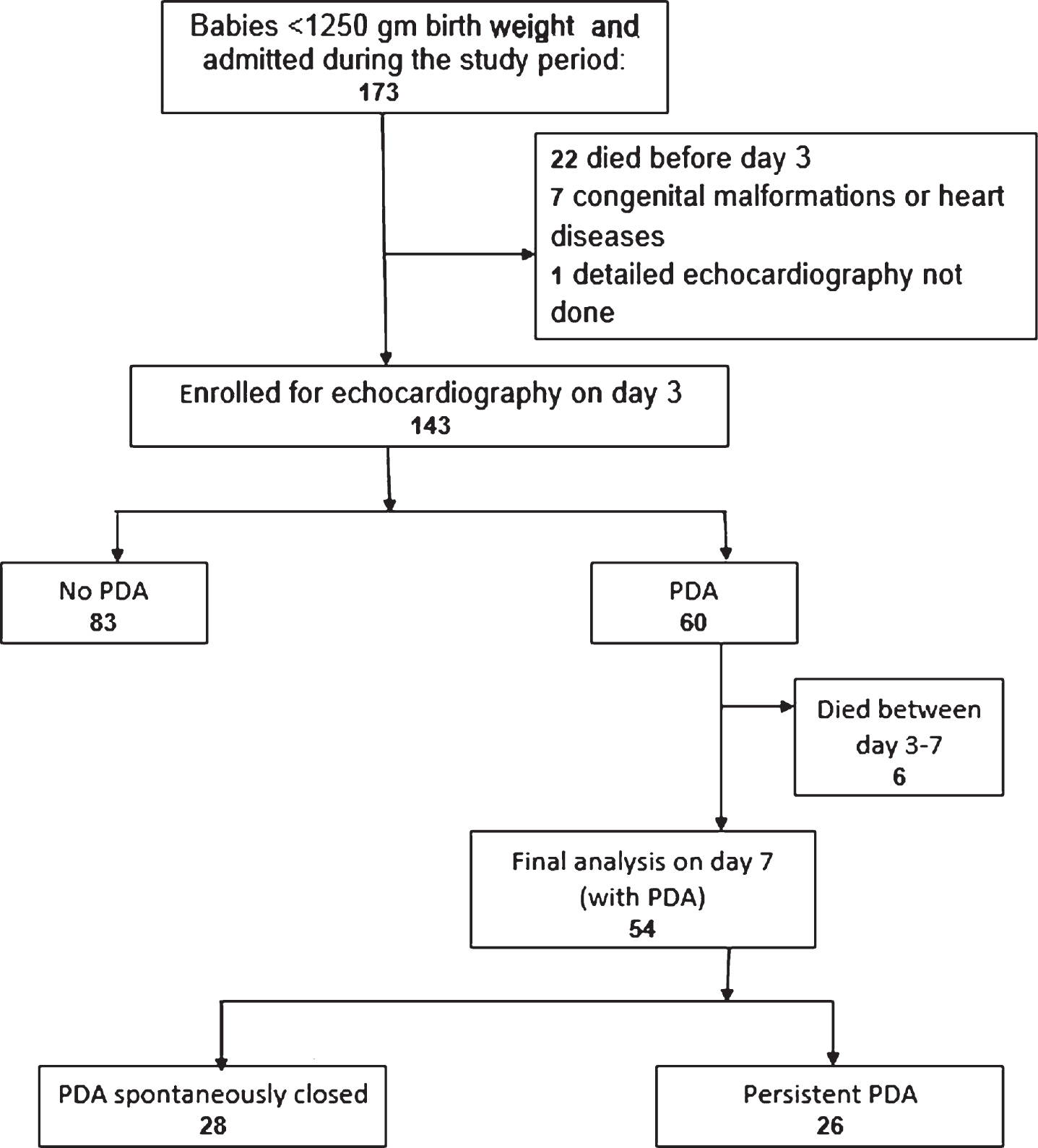
The study population and participant flow diagram. PDA = patent ductus arteriosus, Echo = Echocardiography.
Both groups of babies, spontaneously closed PDA and persistent PDA, were comparable in terms of demography and background risk. Univariate analysis showed significant difference between two groups for all echocardiographic variables except PDA flow velocity and E/A (Table 1).
Comparison of demographic and echocardiography variables between groups based on PDA closure
RDS = respiratory distress syndrome, IVRT = intra ventricular relaxation time, LPA = left pulmonary artery, LVO = left ventricular output, LA/Ao = ratio of Left atrium and aortic root diameter in M mode, E/A = ratio of trans mitral E and A velocity, LVO/SVC = ratio of left ventricular output and superior vena caval flow, PDA = patent ductus arteriosus, IQR = interquartile range. P value < 0.05 was considered statistically significant.
Various PDA flow patterns were dichotomized as either abnormal pattern (growing/ pulsatile) or benign (closing/ bidirectional) pattern. Abnormal flow pattern (growing or pulsatile) has increased risk for persistence of PDA (OR 45, CI 5–383) in comparison to PDA with closing/bidirectional pattern in univariate analysis.
A binary logistic regression model was constructed with PDA closure as the dependent variables and the selective echocardiography parameters as covariates or predictors. The model was best constructed when PDA diameter, LPA diastolic flow, LA/Ao, IVRT, LVO/SVC (continuous variables) and PDA flow pattern (categorical variable) were used as predictors. The logistic regression model was found statistically significant (Omnibus Tests of Model Coefficients < 0.001), was strong enough to explain 62.2% of the variance in PDA closure (Nagelkerke R2 0.62) and correctly classified PDA closure group in 83.3% of cases. Only abnormal flow pattern (growing/ pulsatile) was found to be an independent risk factor for persistence or non-closure of PDA (adjusted OR of 22.9, CI 1.97–269).
Among 60 babies with PDA on day 3, only 40 babies were discharged, and 20 babies died during NICU stay. But of the died babies, 12 already had developed one or more adverse outcomes like BPD or NEC≥stage II or IVH > Grade 2 before death. Hence outcome analysis was done with such 52 (40 + 12) babies with PDA on day 3, who was either discharged healthy or died/ discharged with one or more adverse outcomes. There were 36 babies who developed one or more adverse outcomes like BPD or NEC≥stage II or IVH > Grade 2 (69.3%) whereas 16 babies (30.7%) were healthy at discharge. In univariate analysis, only LPA diastolic flow and LVO/SVC ratio were found to be associated with adverse outcome (Table 2). Pulsatile / growing flow of PDA had higher risk also for adverse outcome in comparison to closing / bidirectional flow (OR 3.89, CI 1.10–13.69). Incidence of adverse outcome was more in persistent PDA group (87.5% vs 41.5%, p = 0.001).
Comparison of clinical and echocardiography variables between groups based on adverse clinical outcome
IVRT = intra ventricular relaxation time, IQR = interquartile range, LPA = left pulmonary artery, LVO = left ventricular output, LA/Ao = ratio of Left atrium and aortic root diameter in M mode, E/A = ratio of trans mitral E and A velocity, LVO/SVC = ratio of left ventricular output and superior vena caval flow, PDA = patent ductus arteriosus. P value < 0.05 was considered statistically significant.
In the second binary logistic regression model considering development of one or more adverse outcomes (NEC, IVH or BPD) as the dependent variable and LPA diastolic flow, LVO/SVC, PDA flow pattern, PDA closure status and gestational age at birth as predictors, it was found that functional echocardiography parameters individually failed to showed any increased risk when adjusted for gestation and PDA closure status. However, the prediction model was statistically significant and strong enough to explain 61.6% of the variance in development of adverse outcome (Nagelkerke R2 0.616) as well as correctly classified adverse outcome group in 85% of cases.
Functional echocardiography has enabled us to follow the evolution of preterm PDA more closely. We examined here prospectively the babies <1250 g, starting from day 3 of life and in pre symptomatic period, for prediction of spontaneous closure of PDA and development of adverse clinical outcomes with functional echocardiography. Our study population with average gestation of 30.8 weeks and 50.3% small for date babies can be considered as representative of the VLBW babies of developing countries who are surviving in large numbers after wide spread introduction of facility based neonatal care in districts.They are slightly more mature and larger than extreme preterm babies of the developed countries NICU and are completely a new cohort. We included babies below birth weight of 1250 gm as larger babies were less likely to suffer from PDA and its consequences. Hence prediction of PDA closure with functional echocardiography in this cohort claims a new implication.
Sehgal and McNamara [14] first proposed in 2007, the echocardiography based staging system for PDA for treatment selection, especially ligation. Later a few retrospective studies by Sehgal et al. [12, 15] have shown importance of echocardiographic scoring for respiratory outcome. He popularized the functional echocardiographic parameters for detection of hemodynamically significant ductus arteriosus (HSDA). The scoring and staging process is based on conventional cut-off of each functional echocardiography parameter and may not be useful here as the cut-offs are not specific for our own population. Instead we used regression model to evaluate the role of different functional echocardiography parameters to predict PDA closure and development of adverse outcome. The need of treatment for symptomatic preterm PDA in later days is easy to decide, but in pre-symptomatic period, the decision to treat or not is often critical considering presence of morbidities vis a vis chance of spontaneous closure especially in VLBW babies. This is why we tried to identify easily doable, focused yet best predictive functional echocardiography parameter for PDA.
There are few retrospective studies on echocardiography parameters for prediction of preterm PDA behavior and the outcome variables are largely heterogeneous. Most commonly the ductal diameter was studied for PDA. Kluckow and Evans [16] showed the early prediction of a significant PDA is possible most accurately with PDA diameter only and not with LVO or La/Ao ratio. But the ductal diameter can vary widely from pulmonary end to aortic end. Ramos et al. [13] also proved the role of PDA size only as predictor for need of treatment while LA / Ao ratio or flow pattern was not proved significant. Alternatively, Flood T and Guthrie JD in 2015 [22] refuted LVEF as a significant predictor for PDA where combination of the LA/Ao ratio (cut off 1.5), PDA/LPA ratio and PFO diameter was proved to be predictive of the presence of PDA. LV/Ao ratio and Pulmonary artery diastolic flow, ductal diameter was considered to be as good predictor based on traditional cut off values by Engur D et al. [23]. Hence, the methodology is not standardized and not yet tested for our own population.
We here analyzed the role of total nine major echocardiographic markers recorded as early as day 3 of life. PDA diameter, LA/Ao, Ductus Vmax, LPA diastolic flow, IVRT, LVO, LVO/SVC and flow pattern, all were found significant in univariate analysis in relation to chance of spontaneous closure of PDA. The study is first of its kind in this population and unique in including easily doable ductal flow pattern rather than relying only continuous variables like diameter or LA/Ao ratio. We showed that strong prediction for spontaneous closure of PDA in preterm babies can be done best if we use the selective echocardiography variables like PDA diameter, LA/Ao ratio, LPA diastolic flow, IVRT, LVO/SVC ratio and PDA flow pattern. Focused echocardiography with these minimum five parameters can be useful for PDA management in NICU. As per the results, even only PDA flow pattern can be used as strongest predictor, irrespective of LA/Ao ratio or diameter of the PDA. Biologically also flow pattern is the most definite marker of pathological shunt and fits with this hypothesis well. In this case, presence of growing or pulsatile pattern of a PDA if picked up on day 3 even before symptoms, was proved to be a robust predictor of persistence of PDA in future. Su et al. [17] earlier proved the utility of flow pattern to predict clinically symptomatic PDA only and here we expanded its use to predict chance of spontaneous closure also. Not many studies earlier tried this as a useful marker for targeted echocardiography at bed side for small preterm babies. Avoidance of unwanted overtreatment as well as need for early treatment in true cases, both can be achieved if one relies on this sign judiciously.
We found also a high incidence (69%) of babies having one or more adverse outcomes like BPD or NEC (≥stage 2) or IVH (>grade 2) in babies with PDA during hospital stay. But uniquely, the conventional parameters like PDA diameter and LA/Ao ratio failed to show any association with adverse outcome. Again, only LPA diastolic flow, LVO/ SVC ratio and abnormal PDA flow pattern were found to be associated with adverse outcome in univariate analysis in this cohort of VLBW babies. There are some evidences in favor of LVO/SVC flow, being directly proportional to ductal flow and a precise indicator for the magnitude of the ductal shunt, to determine the future outcome by day 2-3 of life. The risk persists even if the PDA is closed later [24, 25]. For this cohort, gestational age at birth, final PDA closure status and three echocardiographic parameters like LPA diastolic flow, LVO/ SVC ratio and PDA flow pattern together predicted adverse outcome well in the prediction model. But in multiple regression analysis, these markers individually lost their significance for outcome prediction when adjusted for gestational age and final PDA closure status. We need a larger sample size to test this hypothesis. It corroborates the finding of a previous study by Elsayed Y et al. [26] who showed that after adjustment for gestation, PDA diameter did not predict any adverse outcome, but composite PDA score was associated with increased risk of any adverse outcome. It can be said still now clinical outcome of babies with PDA in NICU could not be predicted by early echocardiography parameters of PDA alone because it is also influenced by gestational age at birth as well as final PDA closure status.
Small sample size is the limitation of the study. Hence, we could not include all parameters together as predictors in regression model. Despite small sample size, our result reflects the present scenario of PDA related issues in VLBW babies, especially babies <1250 gm, who are the major candidates for neonatal care units in India.
Conclusion
We conclude by saying that functional echocardiography markers as on day 3 of life in babies of birth weight less than 1250 gm with patent ductus arteriosus can predict future chance of spontaneous closure very well. Ductus shunt flow pattern is the most useful marker for such prediction. But no single echocardiography marker is helpful for prediction of subsequent adverse clinical outcome. Adverse outcome prediction is possible with functional echocardiographic markers when combined with gestational age and PDA closure status.
Funding
No funding required.
Conflict of interest
The authors declare no conflict of interest.
Contribution of authors
SS, AKS and SC contributed to the protocol development and literature search. AKS and BM participated in patient screening, enrolment, data collection and outcome assessment. AKS wrote the manuscript. AKS and SC did data analysis and interpretation while SKS supervised the final data analysis. All the authors approved the submitted manuscript.
Footnotes
Acknowledgments
none