
Abstract
BACKGROUND:
Very low birth weight infants born prematurely are at greater risk for growth delays that lead to Ex-utero Growth Restriction (EUGR) during vulnerable periods of organ structural and functional development. There is considerable evidence that early growth failure has adverse effects on long term neurodevelopment in children which often persists into adulthood.
METHODS:
This is a single-center cross-sectional study on live newborn infants with birth weight ranges from 500 to 1500 grams (VLBW) and gestational age (GA) between 24–32 weeks who were admitted to NICU at KAMC-Jeddah over a 5 year period (2009–2013). This study aims to evaluate predischarge growth pattern of VLBW infants in terms of weight, head circumference (HC) and length and to identify important variables that have influenced such growth pattern.
RESULTS:
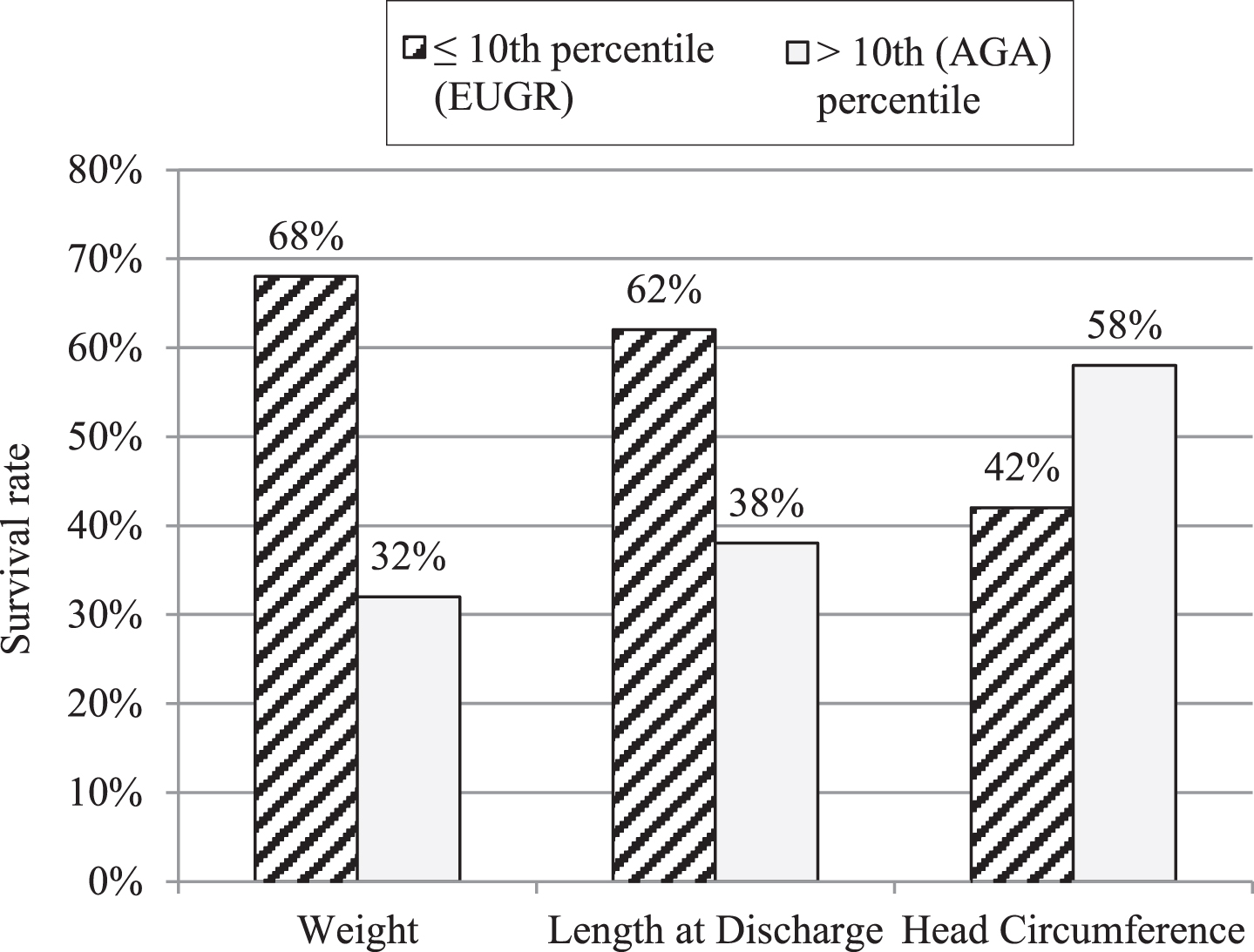
Of the 135 infants included in the final analysis, 68 (50.4%) were male and 67 (49.6%) were female and the mean gestational age was 28.83±2.064 weeks and the mean birth weight 1166.74±256 grams. Ninety-two infants (68%) had discharge weight at ≤10th percentile and forty four (32%) had their weight >10th percentile. HC was the lowest affected among the anthropometric measurements with 42% ≤10th percentile. In terms of linear growth, 62% had their length ≤10th percentile. Amongst infants born ≤750 grams, 71% and 70% had HC and height at ≤10th percentile respectively, at the time of discharge. BPD was significantly associated with EUGR (p = 0.026).
CONCLUSIONS:
This study demonstrates that almost 2/3rd of VLBW infants born at KAMC-Jeddah with birth weight ≤750 grams were discharged home with EUGR as demonstrated by their weight, length, and HC ≤10th percentile. BPD was found to be significantly associated with EUGR amongst post-natal factors influencing EUGR.
Introduction
Over the past few decades, major advances in perinatal and neonatal practices has resulted in significant improvements in the survival of very premature and extremely low birth weight infants [1]. Despite improvements, infants born extremely premature (i.e., <27 weeks) and particularly those with birth weight of <1000 grams (i.e., extremely low birth weight) still have increased odds for short-term comorbidities and potential adverse neurodevelopmental consequences. Prematurity not only increase their probabilities of developing short-term morbidities but also slowing their growth leading to Ex-utero Growth Restriction (EUGR) during vulnerable periods of maximum structural and functional development [2]. Nutritional insults to the vulnerable periods of brain development has been shown to be associated with decreased number of brain cells, brain size, and later effects on behavior and memory [2].
Studies have shown that the growth pattern of VLBW infants has significant association on their neurodevelopmental status at the 18–22 months of age [3]. For instance, infants in the lowest quartile of growth during their hospital stay are 8 times more likely to develop cerebral palsy as compared to infants at higher quartiles (i.e., Odds ratio (OR)8, CI: 2.07–30.78). Moreover, motor disability index (MDI) <70, physical disability index (PDI) <70, neurodevelopmental impairment (NDI) were all higher in “slow grower” preterm infants as compared to infants grow in the higher quartiles (OR 2.25, 1.92, 2.53, respectively). There is considerable evidence that early growth failure has also long-term negative neurodevelopment effects on children and probably persists into adulthood [4, 5].
American Academy of Pediatrics [6], The Canadian Pediatric Society [7], and European Society of Pediatric Gastroenterology, Hepatology, and Nutrition [8, 9] recommends providing sufficient energy and nutrients to support growth of extremely born preterm infants at a rate that approximates in-utero growth. However, EUGR continues to be common with a prevalence of 43–97% reported from various centers [1, 11]. Thus, this study aims to determine the predischarge growth pattern of VLBW infants admitted to neonatal intensive care unit (NICU) at King Abdulaziz Medical City, Jeddah, Saudi Arabia and to evaluate the prevalence of EUGR over a period of 5 years. Furthermore, association of EUGR and clinical variables influencing growth in the immediate post-natal period were evaluated.
Methods
This is a single-center cross-sectional cohort study on live newborn infants with birth weight ranging from 500 to 1500 grams (VLBW) and gestational age (GA) between 24–32 weeks who were admitted to NICU at KAMC-Jeddah over a period of 5 years (2009–2013). VLBW infants were identified from the neonatal admission registry and those with lethal complex congenital anomalies, intrauterine growth restriction (birth weight ≤10th percentile) or died before hospital discharge were excluded as per the study exclusion criteria. Anthropometric measurements including daily weight and weekly length and head circumference (HC) were extracted from patient’s records. Patients’ demographic and clinical characteristics including birth weight, gestational age, gender, and survival to discharge were recorded and comorbidities including respiratory distress syndrome (RDS), bronchopulmonary dysplasia (BPD), late-onset sepsis, necrotizing enterocolitis (NEC), patent ductus arteriosus (PDA) and intraventricular hemorrhage (IVH) were also collected.
Detailed nutritional data were collected including composition and volume of total parenteral nutrition (TPN), other intravenous fluids, volume of enteral feeding and caloric additives (Human Milk Fortifiers). The unit has a detailed nutritional and feeding protocol which serves to guide nutritional and feeding of VLBW infants. During the study period, all VLBW infants less than 1.25 kg received TPN and infants above this weight as per the attending (consultant) discretion. TPN started early (0–3 days of life) and minimal enteral feeding (MEF) preceded feeding if birth weight is <1000 grams. Standardized feeding protocols were used according to birth weight category and target of 110–120 kcal/kg reached at 5–7 days of age. Fenton infants (unisex) growth chart was used to evaluate weight (daily), length, and HC (weekly) and plotted in terms of completed weeks of gestation. EUGR was defined as having a measured growth parameter (weight, length and HC) below the 10th percentile of postmenstrual age (PMA) at the time of hospital discharge. Statistical Package for Social sciences (SPSS) version 24 (IBM SPSS Statistics 24, IBM Corporation, Somers, NY) was used for data coding and analysis. Appropriate parametric and non-parametric statistical tests were used to evaluate significance among the selected variables. Chi-square was used to evaluate categorical variables in relation to outcome and P value of <0.05 was considered significant.
Results
Over the period of 5 years (i.e., 2009–2013), 15,162 infants were born at King Abdulaziz Medical City, Jeddah, out of which 1,715 were admitted to NICU for various indications representing 11.3% of total live births. VLBW infants were 239 in number which represented 1.58% and 13.9% of total live births and admission to NICU, respectively. Thirty-six died before hospital discharge (survival rate of 85%) and were excluded as per the exclusion criteria (including deaths secondary to lethal congenital anomalies). Fifty-six were excluded as their birth weight was ≤10th percentile and 4 were excluded as they are born outside and transferred at a later age. Three infants were excluded because of major nonlethal anomalies and 5 excluded because of incomplete medical records. A flow diagram of the study selection process is presented in Fig. 1. Of the 135 infants included in the final analysis, 68 (50.4%) were male and 67 (49.6%) were female, mean gestational age was 28.83±2.064 weeks and mean birth weight 1166.74±256 grams as shown in Table 1. Ninety-two infants (68%) had discharge weight of ≤10th percentile and 44 (32%) had their weight >10th percentile. HC was the least affected among the anthropometric measurements in which 42% (vs. 68% for weight) have their HC of ≤10th percentile (Table 2 and Fig. 2). However in subgroup analysis, in infants with birth weight ≤750 grams, 71% had their HC ≤10th percentile. In terms of linear growth, 62% of all infants had length ≤10th percentile whereas 70% of smaller infants (≤750 grams) had their height ≤10th percentile at the time of discharge (Table 3). Among the clinical variables and comorbidities studied, BPD was significantly associated with EUGR at the time of discharge (Table 4).
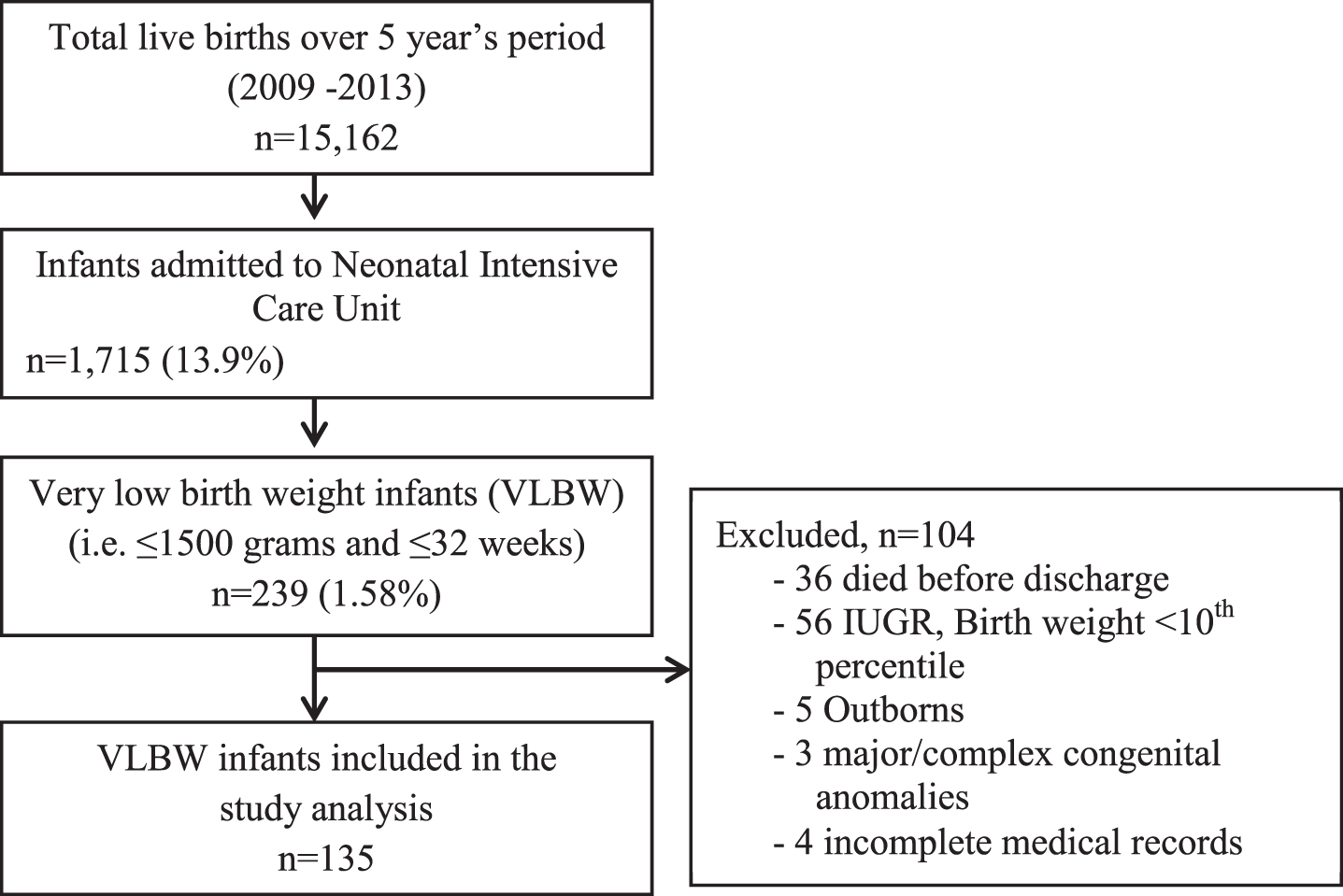
Flow chart in the selection of samples.
Demographic characteristics
Note: gender values are presented by frequency and percentage; values in terms of grams, days and weeks are presented by mean and standard deviation; Mean (SD).
Pre-discharge growth parameters of VLBW infants for five (5) years compared to inutero growth for 135 infants.
Weight, length, and head circumference at discharge for VLBW infants
Significance of relevant variables associated with birth weight ≤10th percentile (EUGR) at time of discharge
Significance of common comorbidities and EUGR at discharge (weight ≤10% percentile)
In-utero fetus doesn’t encounter an interrupted nutritional supply, depletion of nutritional supplies, or increased energy consumption as seen ex-utero [12]. In spite of all efforts to match the ex-utero “fetal” growth to in-utero growth rate, EUGR continues to occur in the majority of extremely born preterm infants [10, 11].
In our study, 68% of VLBW infants had their discharge weight ≤10% percentile. NICHD had reported 79% rate of EUGR in the same category [11]. The higher incidence reported in the NICHD reflects many centers and much higher population size with heterogeneous care, while our rate reflects a single center wherein homogenous care is expected. However, others like Clark et al. [1] had reported a lower rate at 28% in infants of gestational age of 23–34 weeks and Shan et al. [13], reported an incidence of 56.8% in infants <37 weeks. In premature infants with birth weight ≤750 grams higher incidence of EUGR (100%) was noticed when compared to infants with higher birth weight category (71% for birth weight 750–1000 grams and 64 % for birth weight of 1000–1500 grams). This is comparable with Stewards study [14] (89% rate of EUGR), for infants with birth weight less (<) 1000 grams in his study.
Linear growth is an important growth parameter as it doesn’t only reflect lean body mass and body accretion rate [15, 16] but more importantly is an index for organ development including the brain [17], however it is less monitored and given less attention compared to weight and HC. There are growing evidences that linear growth suppression, irrespective of weight gain, is associated with poor cognitive outcomes [10, 11]. In our study, 62% of VLBW had their length ≤10% percentile at hospital discharge and it was more concerning for infants of birth weight ≤750 grams (79%) being higher than what reported by Clark et al. (34%). Head growth was relatively spared with only 42% with HC ≤10% percentile at time of hospital discharge. Head growth correlates well with overall growth during fetal life, infancy, and early childhood and development achievements of VLBW infants [18]. Infants with lesser birth weight had higher incidence of smaller head size at discharge (79%, 71%, and 42% for ≤750 grams, 751–1000 grams, and 1001–1500 grams, respectively).
EUGR was reported by many investigators around the world. Sakural and colleagues [19] had reported an incidence of 57%, 48%, 6% for weight, length, and HC from 22 centers in Japan. Kim et al. from Seoul [20], South Korea had reported 37%, 27%, and 32% for weight, length, and HC for infants <32 weeks gestation. Among the several variables and comorbidities studied, our study found that BPD was statistically significant independent risk factor for EUGR and this is agreement with study by Clark and Ehrenkrans [1, 10]. There was no difference in days to start enteral feeds or days to reach full feeds between normal and growth restricted infants, also reported by Shan et al. [13]. There was a trend toward EUGR for later or no use of TPN.
Male gender, gestational age, birth weight and length of hospital stay were related to EUGR in study by Shan et al. [13] (logistic regression analysis), however, our study observed a trend towards EUGR for female gender and ELBW infants (<1000 grams). Time to regain birth weight was found to be 3 weeks for gestational age for 24–25 weeks and 2 weeks for 28–29 weeks gestation in the study by Ehrankranz et al. [10] whereas infants in our study regained birth weight within a mean of 13.87±4.9 days.
Our infants had an average length of stay of 52±30 with mean birth weight at discharge of 1991.46±437. Patel and his colleagues had reported 77.6±25 for hospital stay and 2087±538 for weight at discharge [2]. The smaller LOS and weight at discharge may be due to the fact that the unit adopts physiological criteria for premature discharge.
This study has several limitations including its retrospective design and relatively small sample size. Nevertheless, this study recommends that nutritional and feeding practices in infants born premature should be targeted towards approximating ex-utero “infants” growth to in-utero “fetal” growth with a goal to achieve improved long-term neurodevelopmental outcomes.
Conclusions
EUGR is common among VLBW infants born at KAMC-Jeddah particularly in infants with birth weight ≤750 grams. 68.2%, 62%, and 42% of all infants were discharged home with their weight, length, and HC ≤10% percentile for age respectively. BPD is an independent risk factor for EUGR. All efforts should be made to achieve in-utero fetal growth for prematurely born infants as their neurodevelopmental outcome is adversely affected with postnatal growth failure.
Disclosure statements
Conflicts of interest
The author declares that there is no conflict of interest.
Funding statement
The author received no financial support for the re-search, authorship, and/or publication of this article.
Human research statement
This study was approved by the Institutional Review Board of King Abdullah International Medical Research Center (KAIMRC), Jeddah, Saudi Arabia. This study was also approved by the head of the Department of Pediatrics, Division of Neonatology, King Abdulaziz Medical City, Jeddah, Saudi Arabia, and was conducted according to the Declaration of Helsinki, Ethical principles for medical research involving human subjects, as set by the World Medical Association.
Animal research statements
Not applicable.
Other disclosure statements
Not applicable.
Footnotes
Acknowledgments
The author is grateful to Dr. Mohammad Al Zahrani and Dr. Faysal Farahat for their support in data management and statistical analysis. I would like also to thank Mr. Juan Manlangit Jr. for his helpful comments, recommendations and editing the manuscript and for Ms. Cecille Selda and Ms. Maricel Tan for their secretarial support.