
Abstract
BACKGROUND:
Newborn infants with birth weight less than 1500 grams defining very low birth weight (VLBW) constitute 1.2–1.5% of total live births and 15–20% of all admissions to neonatal units. Advances in antenatal care, care at delivery, and neonatal practice over the past few decades, have substantially improved outcomes in VLBW infants, and reduced neonatal mortality.
METHODS:
A retrospective single tertiary care center cohort study of VLBW infants with gestational age between 23–33 weeks admitted to the neonatal intensive care unit (NICU) in King Abdulaziz Medical City, Jeddah (KAMC-J) between January 1, 1994, and December 31, 2019 (26 years). The trends of survival of VLBW infants and major changes in clinical practice of premature care over a period of 26 years were evaluated.
RESULTS:
Over a period of 26 years, 1,247 VLBW infants were admitted to the NICU that represents 1.43% (1.25–1.83%) of total live births. 50.80% (n = 634) were male, whereas the 49.2% (n = 613) were female. Among them, 1013 (81.2%) were discharged home alive. There was a significant and progressive improvement in the survival rate of VLBW infants over a 26-year period from 66.83% in period 1 (1994 –1998) to 90.0 % in period 5 (2014 –2019), which represents a 34.67% total improvement rate. The improvement in survival rates was observed in all gestational ages between 23–33 weeks, particularly in infants weighing ≤750 grams and ≤1000 grams, and with gestational age between 23–27 weeks. Infants with a gestational age of ≤26 weeks and birth weight ≤750 grams delivered by cesarean section had a higher survival rate. Moreover, female infants with a gestational age of ≤26 weeks and birth weight ≤750 grams had a higher survival rate compared to males but not statistically significant.
CONCLUSIONS:
The survival rate of VLBW infants had improved significantly over the past 26 years (1994 –2019). This is attributed mainly to the improved survival of ELBW infants (<1000 grams) and gestational age of ≤26 weeks.
Abbreviations
Assist-Control Antenatal corticosteroids Bronchopulmonary dysplasia Canadian Neonatal Network High-Frequency Oscillatory Ventilation High-Frequency Oscillatory Ventilation with Volume Guarantee Nasal Continuous Positive Airway Pressure National Institute of Child Health & Human Development Neonatal Intensive Care Unit Nasal Intermittent Ventilation Pressure Support Ventilation Respiratory distress syndrome Synchronized Intermittent Mandatory Ventilation Very low birth weight Vermont Oxford Network
Introduction
Newborn infants with birth weight less than 1500 grams defining very low birth weight (VLBW) infants constitute 1.2–1.5% of total live births and 15–20% of all admissions to neonatal units [1]. Prematurity remains the commonest cause of neonatal death after lethal congenital anomalies and the second leading cause of death in children younger than 5 years of age [2, 3]. Neonatal mortality rate diminished over the past few decades partly due to improved survival of VLBW infants [1, 3]. Although the survival rates of VLBW infants varied between different institutions and nations, however, with the improvement of antenatal care, care at delivery, and advances in neonatal practice, the outcome in VLBW infants has substantially improved and reduced neonatal mortality. Several studies from Saudi Arabia [4–13] demonstrated the improved survival of premature infants over the last two decades, yet no study evaluated the trends in survival rates over a longer period and correlates the change in survival with the major changes in clinical practice of premature care. Therefore, this study evaluated the trends of survival of VLBW infants at a single tertiary care center over a 26-year period and discussed the major changes in clinical practice of premature care during that period.
Method
This is a retrospective single tertiary care center cohort study of VLBW infants weighing 500–1500 grams and with a gestational age between 23–33 weeks admitted to neonatal intensive care unit (NICU) in King Abdulaziz Medical City, Jeddah (KAMC-J) between January 1, 1994, and December 31, 2019 (26 years). VLBW infants were identified from the neonatal unit admission registry and infants with lethal or complex congenital anomalies, and with a gestational age of >33 weeks were excluded from the study. Data on perinatal and neonatal patient characteristics (demographic data), including antenatal care, use of antenatal corticosteroids, mode of delivery, gestational age, birth weight, surfactant use, gender were collected and analyzed. The study population was stratified according to gestational age, birth weight, and year interval (5 years) to determine the trend in survival rates of VLBW infants over the 26 years, and major changes in clinical practice related to very premature care were evaluated. The statistical analysis was performed using the Statistical Package for Social Sciences (SPSS), version 20.0 (IBM Corp., Armonk, NY, USA). The data were presented as mean and standard deviation for continuous variables and frequencies and percentages for categorical variables. Chi-square test was used for comparison of categorical variables. The level of significance was set at a p-value of <0.05.
Results
Between January 1, 1994, and December 31, 2019, 69815 (2686 + 623 per year) infants were born alive at KAMC-J. Among them, 7,992 (307 + 56 per year) infants were admitted to NICU out of which 1,247 were VLBW infants, representing 1.43% (1.25–1.83%) of total live births and 15.4% (12–21%) of admissions to NICU. There were 634 males (50.80%) and 613 females (49.2%) in the cohort. 680 (54.5%) were delivered by cesarean section and 539 (43.2%) by spontaneous vaginal delivery. The mean gestational age was 29.01 (±2.96) weeks and the mean birth weight was 1095 grams (±270) (Table 1).
Perinatal and neonatal characteristics of VLBW infants (1994-2019)
Perinatal and neonatal characteristics of VLBW infants (1994-2019)
ANC, Antenatal corticosteroids.
Overall, in the period between 1994 and 2019, 1013 (81.2%) out of 1247 VLBW infants were discharged home alive. There was a significant and progressive improvement in the survival rate of VLBW infants over a 26-year period from 66.83% in period 1 (1994 –1998) to 90.0 % in period 5 (2014 –2019), which represents a 34.67% total improvement rate (Table 2). This upward trend in survival was seen and observed in all the periods with variable improvement rates (Fig. 1). The improvement in survival rates for infants weighing ≤750 grams significantly improved from 27.27% in period 1 to 60.71% in period 5 and that in ELBW infants from 48.61% in period 1 to 76.47% in period 5, respectively (Table 2). The survival rates trends were evaluated and analyzed per gestational age in weeks and progressive improvement in the probability of survival in all gestational ages from 23 to 33 week was observed, however, an improvement was more significant at a lower gestational age between 23–27 weeks (Table 3, Figs. 2 and 3).
Survival rate of VLBW infants stratified by birth weight groups (1994–2019)
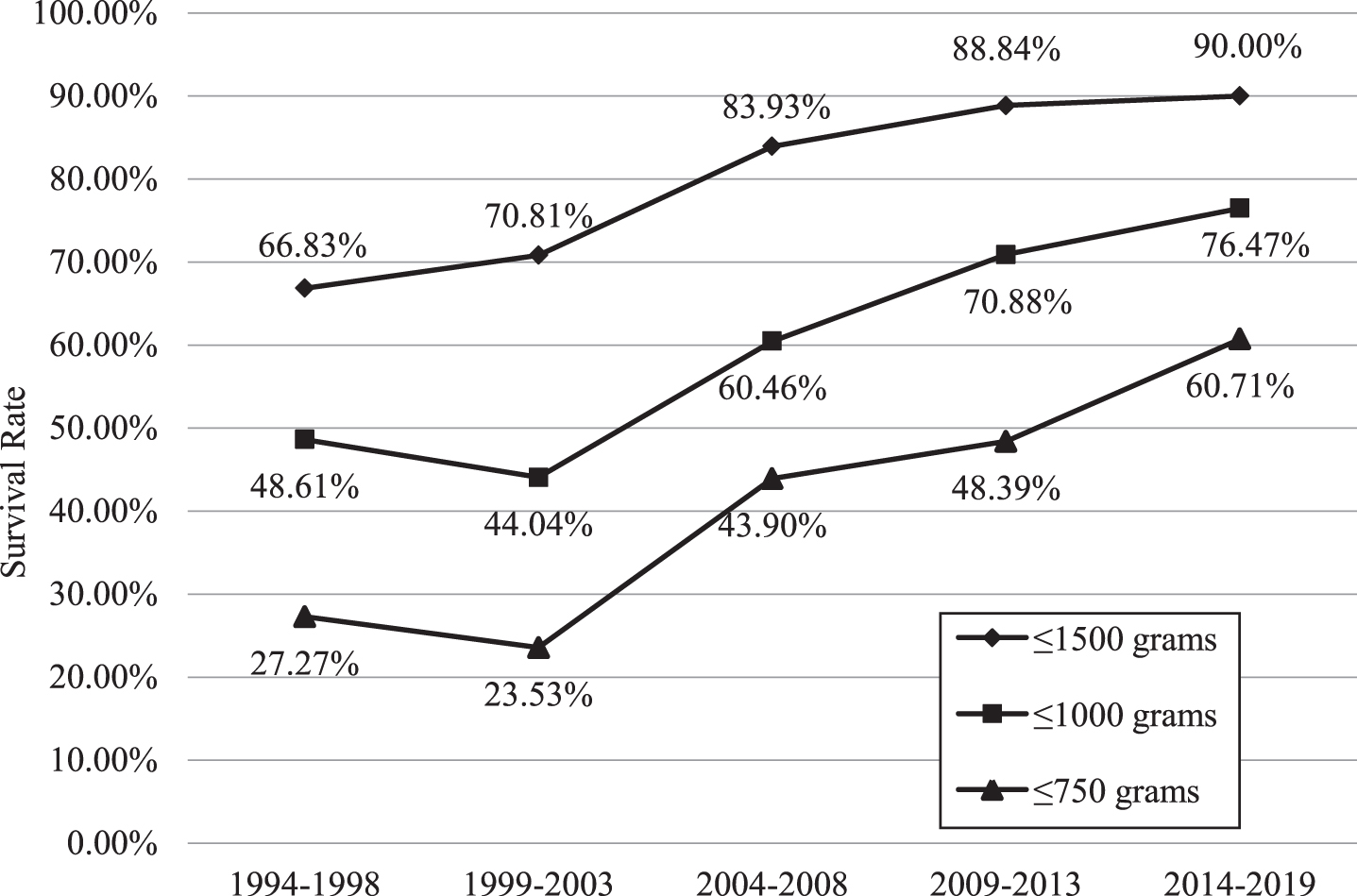
Survival rate of VLBW infants stratified by birth weight groups (1994 –2019).
Survival rate of VLBW infants stratified by gestational age groups (1994–2019)
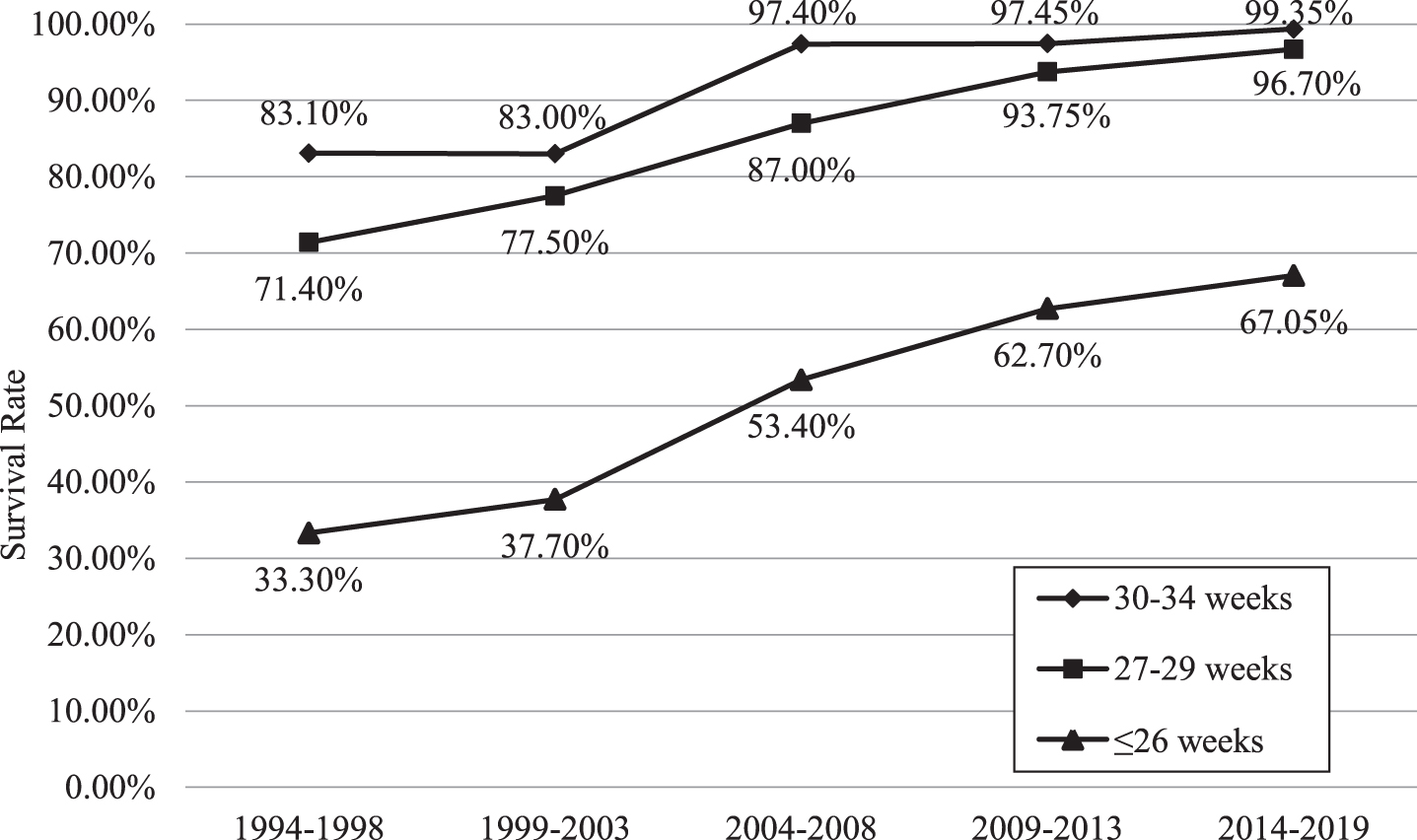
Survival rate of VLBW infants stratified by gestational age groups (1994-2019).
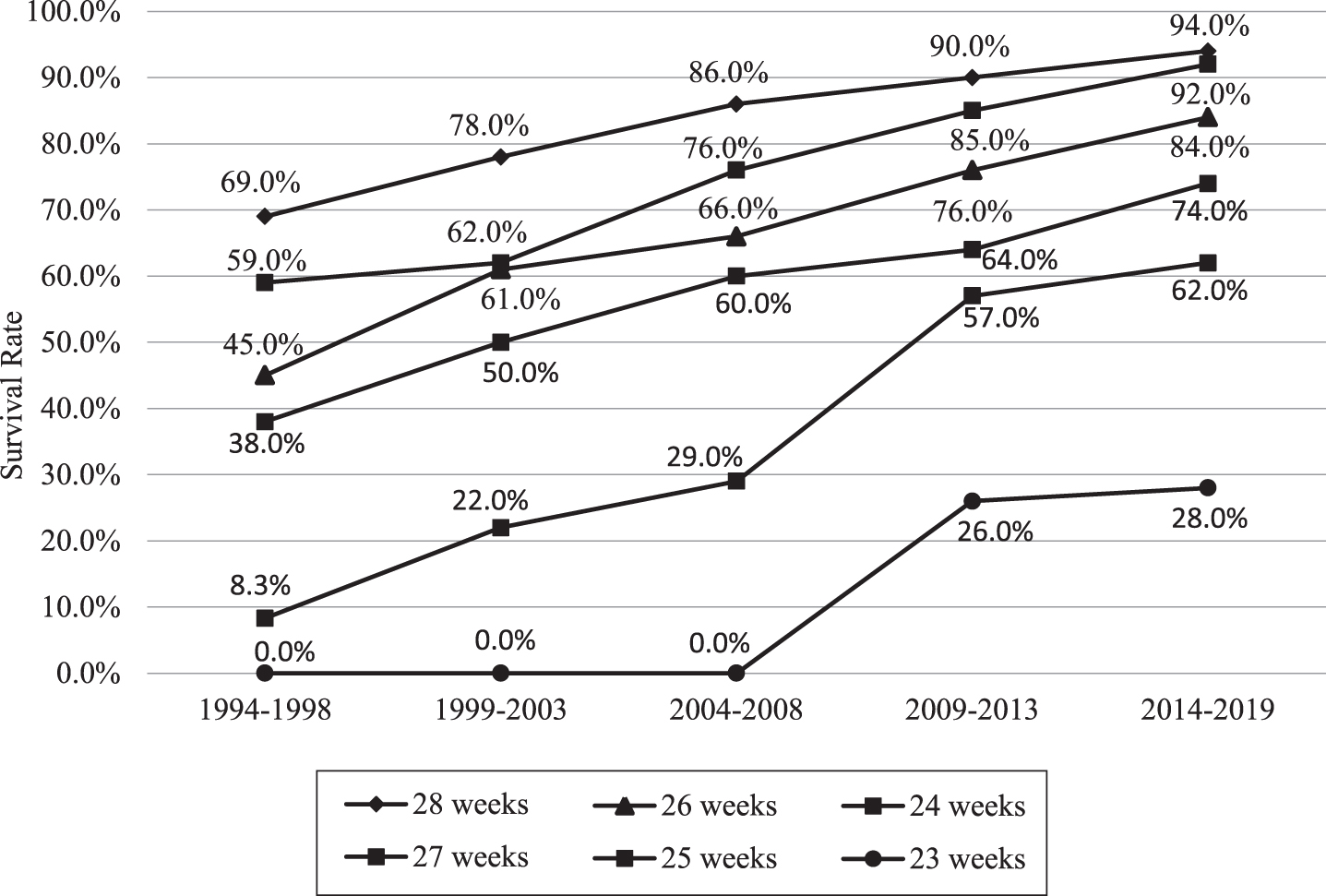
Survival rate of VLBW infants according to gestational age by weeks (1994-2019).
VLBW infants delivered by cesarean section had a higher survival rate when compared to infants born vaginally (88.97% vs 72.91%, p < 0.001). On subgroup analysis based on gestational age and birth weight, VLBW infants of gestational age ≤26 weeks and birth weight ≤750 grams had a higher survival rate when compared to infants born vaginally (69.15% vs 44.5%, p < 0.001 and 64% vs 37.4%, p = 0.001, respectively). For infants born with gestational above 26 weeks and birth weight more than 750 grams, cesarean birth was not associated with statistically significant improvement in survival (88% vs 84.62%, p = 0.335 and 78.52% vs 71.05%, p = 0.164, respectively).
There was a trend toward higher survival for females compared to males (82.06% vs 80.44%) but not statistically significant. This trend was more observed for infants with birth weight ≤750 grams and gestational age ≤26 weeks (47.25% for female vs, 40.86% for male, p = 0.382 and 53.85% vs 50.66%, p = 0.584, respectively).
Over the past few decades, the survival of VLBW infants has improved. Advances in neonatal-perinatal care and technology-driven by accumulating evidence paved the way for neuro-developmentally intact survival of many premature infants who were deemed nonviable years ago [14]. This study evaluated the trends in survival of VLBW infants at a single institution over a period of 26 years and described the major changes in clinical practices related to premature care over time (Table 4). Across all birth weight subgroups (500–1500 grams), there was an improvement in survival by 34.67% (66.83% in the period from 1994–1998) to 90.0% in the period from 2014-2019. Nevertheless, the magnitude of the improvement was more significant in infants weighing ≤750 grams (122.62% improvement rate), and ELBW Infants (57.31% improvement rate). For all gestational age (23–33 weeks), there was also a progressive improvement but more significantly among infants with a gestational age of 24, 25, and 26 weeks, with an improvement rate of 647%, 95%, and 87%, respectively. This study had observed improvement in outcomes of VLBW infants, which are believed to be related to significant changes in neonatal and perinatal care practices, technological advances, and therapeutics that the unit had adopted and these are presented in detail in Table 4.
Major changes in premature care practices at the NICU, KAMC-J from the early 1990s till present
Major changes in premature care practices at the NICU, KAMC-J from the early 1990s till present
Several studies from many centers in Saudi Arabia [4–13] had evaluated the outcome of VLBW and ELBW infants. Although these studies represent a different time period, however, the demonstrated improvement in survival of this group is comparable to survival rates reported from other developed countries and renowned neonatal networks (i.e., National Institute of Child Health & Human Development (NICHD) [15], Vermont Oxford Network (VON) [16], and Canadian Neonatal Network (CNN) [17] (Table 5 and Table 6). Nationally and based on published data, the survival rate ranges anywhere from 80% to 88.8% for VLBW and 58.5% to 77% for ELBW infants [4–13] (Tables 5 and 6). The studies also evaluated survival rates for very low gestations and demonstrated survival rates ranging anywhere from 52% to 70% for 24 weeks, 70% to 84% for 25 weeks, and 80% to 90% for 26 weeks similar to rates reported by developed countries and international neonatal networks. Unfortunately, these rates reflect the outcome in tertiary care, resource-rich centers, and not necessarily nationwide statistics [10, 11]. There is an urgent need to establish a neonatal vital statistics network for perinatal and neonatal outcomes to evaluate the quality of care and monitor key performance indicators, which would help to guide projects and initiatives that aim to further improve perinatal and neonatal outcomes.
Survival rate of VLBW infants of KAMC-J (2010–2019) as compared to other national centers in the Kingdom of Saudi Arabia and international neonatal networks
KFSH-RC, King Faisal Specialist Hospital, and Research Center-Riyadh; KKUH, King Khalid University Hospital, Riyadh; KFH, King Fahad Hospital, Al Khobar; KAH-A, King Abdulaziz Hospital, Al Hasa.
Survival rate for VLBW infants with a gestational age of 23 to 29 weeks in national centers and compared with CNN and NICHD data
*Note: Include≤23 weeks.
Antenatal corticosteroids accelerates fetal lung maturation that prevents respiratory distress syndrome, brain injury, and thus neonatal mortality [18–21]. In the last three decades, ANC became the routine and standard practice for preterm birth (<33 weeks), however, its use varies widely among centers. The use of antenatal corticosteroids in our center started in the mid to late 1990s, however, its widespread use was hampered by several factors. Only 44% of mothers were booked in the mid-1990s and had antenatal care which affected the use of ANC for preterm birth, however, a steady and progressive increase in the rate of antenatal care which reached 83% for the past 6 years (2014 –2019) led to an increase in the use of ANC for preterm births explaining the slow adoption of its use earlier, moreover hindering the chance of survival of the highest risk group (≤750 grams, ≤26 weeks) in the earlier years of the study period. We observed a progressive increase of ANC in the past 15 years as it became standard practice and more recently its use expanded to include preterm births as low as 23 weeks and up to 37 weeks gestation (late preterm birth). This increase is driven by the concomitant improved survival of lower gestational age ≤26 weeks and birth weight ≤1000 grams and the advances in perinatal care since the establishment of the Materno Fetal Unit at our center which enhanced the utilization of ANC for premature births ≤37 weeks of gestation.
Surfactant discovery in the early 1980s was truly a “Game Changer” rescuing many premature infants who used to die early secondary to Respiratory Distress Syndrome (RDS) and by the late ’80s and early ’90s, surfactant became widely used to manage preterm infants with RDS [22, 23]. Our center started using the Synthetic Surfactant (Exosurf) by the early 1990s, and a few years later natural Surfactant replaced the synthetic type after which the practice didn’t differ significantly during the study period (26 years) and its use range from 74% to 84% in VLBW infants. Though its administration guidelines are kept changing concerning its revised indications, frequency, timing, and routes as more evidence evolved, surfactant continued to be a pivotal and vital drug to prevent and treat RDS and reduce mortality.
Nationwide in the late 1980s and early 1990s, NICU was partially covered (except few Centers) by specialized Consultants/Attending Credentialed as Neonatologists as mostly NICU were covered by Pediatricians who have an “Interest” in Neonatal Medicine. At that time, the number of qualified Neonatologists was not too many and our center was not an exception. In the 1990’s the coverage/care by credentialed Neonatologists was in the range of 30–40% and colleagues from the Pediatric Department used to cover/care around 60–70% of the time (nights/weekend). It took until the year 2000–2002 to have the unit fully covered by certified and credentialed Neonatologists who had structured training in the field of Neonatal-Perinatal Medicine and as years went by, Consultants/Attending and Assistant consultants (Registrars) joined the Institution to match the increasing demand. For the last 10 years, the Neonatal Unit operates as a standalone division (24/7 by neonatal staff).
The advances in the respiratory care of preterm infants were and continued to be one of the main reasons not only to rescue them from dying from RDS but also to have less lung injury and Bronchopulmonary dysplasia (BPD) as less invasive, more gentle, and volume-oriented respiratory support concepts were adopted [6–8, 24]. Before 2002, preterm infants requiring respiratory support were placed on pressure-limited, time cycled, continuous flow ventilators (not synchronous, noisy, unknown tidal volume delivery) and occasionally placed on High-Frequency Oscillatory Ventilation (HFOV) for those who fail conventional ventilation. Subsequently, the unit has changed its practice with regards to respiratory care by adopting volume-targeted ventilation with plethora of patient-triggered modes including Synchronized Intermittent Mandatory Ventilation (SIMV), Assist-Control (AC), and Pressure Support Ventilation (PSV) which in return facilitated the respiratory management of the smallest preterm babies. However, the use of invasive ventilation had become less popular in the past 10–15 years since accumulating evidence of the success of Nasal Continuous Positive Airway Pressure (NCPAP) and more recently (last 10 years) the success of noninvasive respiratory support strategies using in addition to NCPAP, and Nasal Intermittent Ventilation (NIV). Currently, most of the preterm infants who require respiratory support are placed on noninvasive modes (NIV and NCPAP) and if invasive ventilation is required, volume targeted modes are the routine practice even if HFOV is used too (i.e., High-Frequency Oscillatory Ventilation with Volume Guarantee (HFOV-VG)).
The survival rate of VLBW infants had improved significantly over the past 26 years (1994 –2019). This is attributed mainly to the improved survival of ELBW infants. The chance of survival has improved across all gestations in the study population, particularly in the gestational age of 23–26 weeks. Adopting evidence-based practice changes and the major advances in Neonatal-Perinatal Care and technologies over the last 3 decades are behind the significant upward trend in the survival of VLBW infants.
Disclosure statement
Conflict of interest
The author declares that there is no conflict of interest.
Funding statement
The author received no financial support for the research, authorship, and/or publication of this article.
Human research statement
This study was initiated as our department project to determine progress in neonatal care throughout the years based on the prospectively generated data by our department that need not be approved by the Institutional Review Board. However, the project was approved by the head of the Department of Pediatrics, Division of Neonatology, King Abdulaziz Medical City, Jeddah, Saudi Arabia, and was conducted according to the Declaration of Helsinki, Ethical principles for medical research involving human subjects, as set by the World Medical Association.
Animal research statements
Not applicable.
Other disclosure statements
Not applicable.
Footnotes
Acknowledgments
The author is grateful to Dr. Mohammad Anwar Khan for his help with data management and statistical analysis. I would like also to thank Mr. Juan Manlangit Jr for his helpful comments, recommendations, and editing the manuscript and for Ms. Eman Al Thobaiti and Ms. Mariam Kidwani for data collection and Ms. Maricel Tan for her secretarial assistance with the manuscript.