
Abstract
BACKGROUND:
Neonatal opioid withdrawal syndrome (NOWS) is a growing public health problem associated with complex and prolonged medical care and a significant resource utilization burden. The objective of this study was to compare the cost of different convalescent care settings for infants with NOWS.
METHODS:
Retrospective comparison study of infants with NOWS discharged directly from NICU, transferred to an acute care pediatric floor (PPCU) or rehabilitation hospital (PRH). Primary outcomes were length of stay (LOS) and cost of stay (COS).
RESULTS:
Infants had 1.3 (95% CI: 1.1,1.6) times and 2.5 (95% CI: 2.1,3.1) times significantly longer mean LOS for PPCU and RH discharges compared to NICU discharges. NICU discharged infants had the lowest mean COS ($25,745.00) and PRH the highest ($60,528.00), despite PRH having a lower cost per day. PRH discharged infants had higher rates of methadone and benzodiazepine and less buprenorphine exposure than NICU/PPCU discharged. Infants born to mothers on marijuana and buprenorphine had a 28% lower mean COS compared to unexposed infants. Median treatment cumulative morphine doses were six-fold higher for PRH than NICU discharge.
CONCLUSIONS:
Infants transferred to convalescence care facilities had longer and more costly admissions and received more medication. However, there may be a role for earlier transfer of a subset of infants at-risk for longer LOS as those exposed to methadone and/or benzodiazepines. Further studies exploring differences in resource utilization, convalescent care delivery and cost expenditure are recommended.
Background
Neonatal opioid withdrawal syndrome (NOWS) is characterized by physiologic symptoms in a neonate following in-utero opioid exposure either alone, or in combination with other substances. It is a growing public health issue associated with complex and often prolonged medical care after birth. Treatment for NOWS involves both pharmacologic and nonpharmacologic measures as well as a controlled, low-stimulation environment [1, 2]. Infants with in-utero drug exposure are more likely to have low birthweight, respiratory distress, feeding difficulty, concern for sepsis, and seizures; thus often require neonatal intensive care unit (NICU) admission [3–5].
Hospitalization days for infants affected by NOWS is estimated to be approximately 16–23 days, with associated costs ranging from $37,000 to $79,000 per patient [1, 7]. The incidence of NOWS increased fourfold from 2003–2012, while the cost nationwide surged from a total of $61 to $316 million [2]. An estimated 78% of infants with NOWS receive Medicaid [1]. Moreover, healthcare utilization expands beyond birth admission for infants with maternal opioid exposure, who have approximately four times the risk of hospitalization within a year after birth compared to their counterparts [8]. In a recent study based on census of 47 states and the District of Columbia databases showed a NOWS rate of 7.3/1000 birth hospitalizations in 2017 which was an increase of 4/1000 birth hospitalizations from 2010 [9]. Cost-effective management may the reduce the financial impact on the public health system.
Given the increasing financial impact of NOWS, some hospitals are exploring alternative treatment settings to reduce both NICU admissions and costs [10–13]. Several hospitals have explored treatment of infants with NOWS on acute care pediatric floors and have had success with this model [10–12]. However, treatment in a pediatric rehabilitation hospital has yet to be examined. The objective of this study is to explore the resource utilization patterns in terms of length of stay (LOS) and cost of stay (COS) for infants with NOWS discharged from three different care settings; NICU, an acute care pediatric floor that can provide continuous vital sign monitoring for patients aged 0–21 years (referred to as Pediatric Progressive Care Unit or PPCU), and a pediatric rehabilitation hospital (PRH). A secondary outcome is a comparison of the cumulative doses of morphine administered for treatment of withdrawal symptoms in the same three clinical settings. We hypothesized that the cost of care would be significantly lower when patients are transferred to the PRH as compared to discharge from the PPCU or NICU, due to its lower daily cost.
Methods
Before data collection, institutional review board (IRB) approval was obtained from the hospital system (IRB: HP-00088997). The University of Maryland, Baltimore IRB determined the exemption of this research. In this retrospective cohort study, we reviewed the charts for infants admitted to the University of Maryland NICU, a Level IV tertiary care center from December 2015 through June 2019. The NICU has 52 single patient rooms with an average daily census of 44.9 during the study period. Infants were identified using diagnostic ICD-10 codes P96.1 [Neonatal Abstinence Syndrome], [drug withdrawal], and [drug exposure]. In our institution, all inborn infants undergo urine screening for substance exposure at birth. Infants with in-utero drug exposure are admitted to the NICU if they demonstrate persistent symptoms warranting pharmacotherapy, as directed by an institutional treatment protocol [14]. Infants who are no longer escalating on pharmacotherapy doses are transferred to the PPCU pediatric floor within our own facility, where they will continue management. Alternatively, infants may be transferred to an 87-bed local pediatric rehabilitation hospital with dedicated infant specialty care services, including rehabilitation and social work services. It is staffed by neonatologists, pediatricians, and nurse practitioners. NOWS management is guided by a separate institutional treatment protocol. For all study settings, adaptations in management for infants with polysubstance exposure (e.g. TCH, benzodiazepines) were provider-specific and not protocol-driven.
Electronic medical records were reviewed to identify infants ≥35 weeks’ gestation with in-utero drug exposure and NICU admission. In-utero exposure was identified based on maternal and infant toxicology results or by maternal history. Infants who were <35weeks’ gestation or with major congenital anomalies, comorbidities or diagnosed with iatrogenic withdrawal were excluded to avoid complications related to prematurity or other abnormalities. Data on infant characteristics were collected, including gestational age, ethnicity, age, race, gender, birthweight, maternal characteristics, feeding problems, respiratory distress, breastfeeding status, and medication administration.
The primary outcome measures were total LOS and COS. NICU LOS and total LOS were recorded for each infant, as well discharge location. The costs calculated are the direct variable costs of the NOWS patient population; including inpatient stay, laboratory, drugs, therapy, etc. The fixed portion incurred by the hospitals was not included in this study. Cost calculations included an additional overall within state ambulance and transport services cost of $1500 for infants transferred to the PRH. The secondary outcome measure was cumulative dose of morphine used to treat withdrawal.
Statistical analysis
Descriptive statistics were obtained and stratified by discharge location. Continuous variables were summarized as mean/median (range), as appropriate, and categorical variables as frequency (percentage) and compared between discharge locations. Continuous variables were compared using analysis of variance (ANOVA)/ Mood’s median test and categorical variables were compared using the chi-squared test. Multiple linear regression on natural log-transformed primary outcome variables (LOS and COS), and secondary outcome variable (cumulative morphine dose), was performed with discharge location as the primary predictor variable. The log-transformation was performed to satisfy normality assumptions required for the linear regression procedures and the interpretation of the results were made on the mean response variables on the original scale. The analysis was adjusted for other apriori covariates based on clinical importance. The covariates included gestational age, birthweight, small for gestational age, gender, methadone use, buprenorphine use, heroin use, marijuana use, breast feeding, tobacco use, alcohol use, cocaine use and other opiate use. Barbiturate use, amphetamine use, antipsychotic use and SSRI use were not included in the analysis as less than 10 patients were exposed. A step-wise regression was performed with both forward inclusion and backward elimination based on Akaike information criteria (AIC) to derive the final set of predictors. A two-sided level of significance of 0.05 was used and the results are reported as adjusted estimates with 95% confidence intervals. All statistical analyses were performed using R 3.6.1 (R Core Team, 2019) and RStudio interface (2019).
Results
The results of the search criteria yielded 214 infants, 132 of which were included in the analysis of COS and LOS. The chart review process and preparation of analysis dataset is depicted in Fig. 1. The cumulative morphine dose analysis included only subjects who were on pharmacotherapy (N = 124).
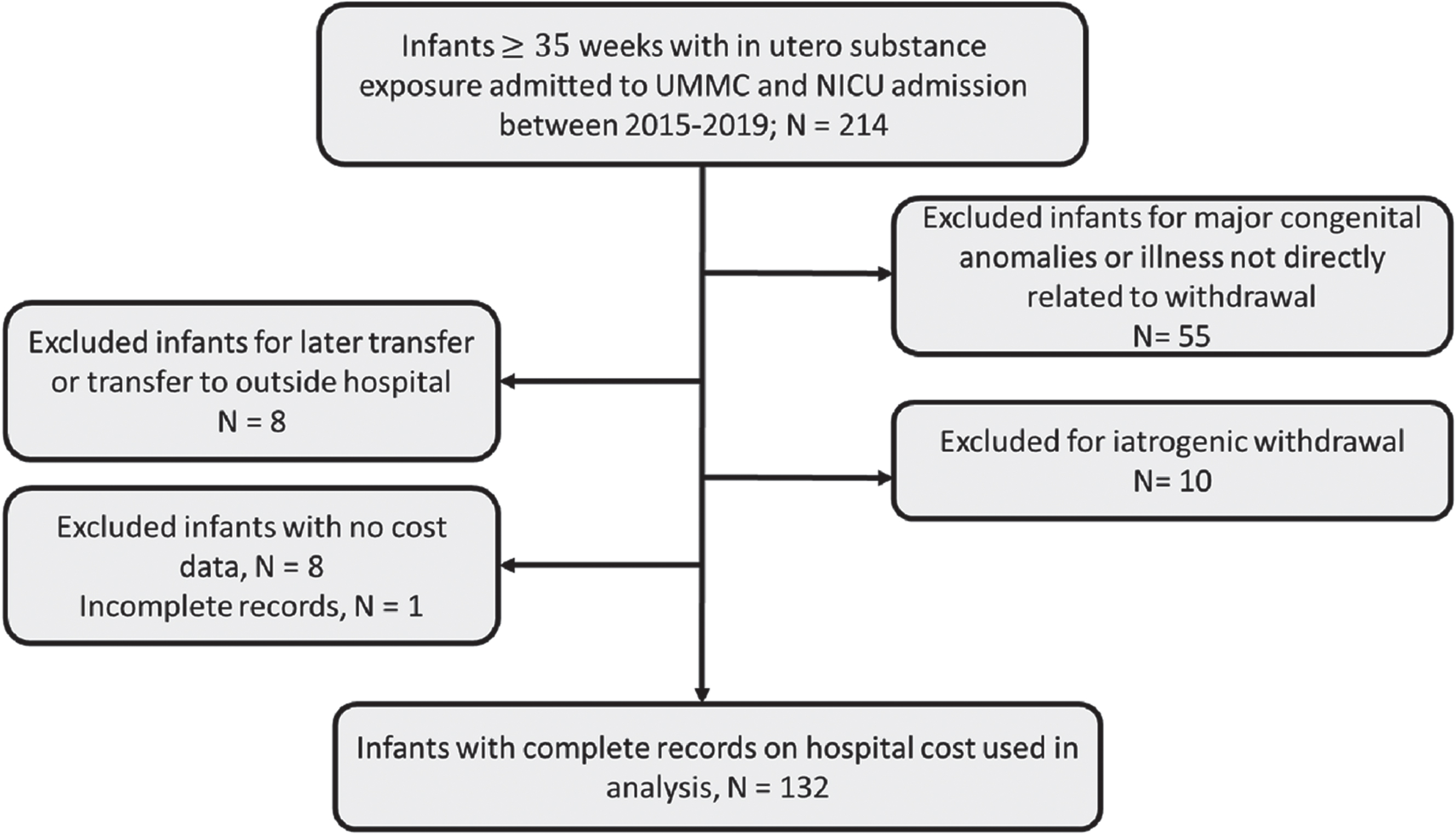
Chart review process and preparation of dataset for analysis. Note: NICU, Neonatal intensive care unit; UMMC, University of Maryland Medical Center.
Table 1 provides infant and maternal baseline characteristics by discharge location. Baseline characteristics were similar between each of the three cohorts. Over 96% of infants had public health insurance. The median NICU LOS was similar for all patients regardless of transfer status, but the median total LOS was longer for infants discharged from the PPCU or PRH. Median LOS was 13, 16, and 38 days for infants discharged from NICU, PPCU, and PRH respectively (p < 0.001). Infants with prenatal exposure to methadone or benzodiazepines were more likely to be transferred to PRH, while those exposed to buprenorphine were much less likely to be transferred.
Baseline characteristics of infants who were transferred from NICU, PPCU and PRH
Note: NICU, Neonatal intensive care unit; PPCU, Pediatric progressive care unit; PRH, Pediatric rehabilitation hospital; LOS, Length of stay; COS, Cost of stay.
Table 2 shows the adjusted mean estimates (95% CI) for the discharge location predictor variable after adjusting for other significant covariates with respect to LOS, COS, and cumulative dose of morphine. Infants discharged from PPCU and PRH had 1.3 (95% CI: 1.1,1.6) times and 2.5 (95% CI: 2.1,3.1) times longer mean LOS than those discharged from NICU, keeping other significant predictors constant. However, mean LOS when discharged from PPCU was mot significantly different from NICU discharge. Adjusting for other significant predictors, infants with benzodiazepine exposure had 1.5 times longer mean LOS than those unexposed while those with methadone exposure had 1.2 times longer mean LOS than those unexposed.
Multiple linear regression analysis of primary and secondary outcome variables
Note: NICU, Neonatal intensive care unit; PPCU, Pediatric progressive care unit; PRH, Pediatric rehabilitation hospital; LOS, Length of stay; COS, Cost of stay. *20 subjects had missing cumulative dose information. #Since the regression analysis was performed on log-transformed variables, the adjusted regression coefficient needs to be exponentiated for interpretation. For example: exp(0.262) = 1.3, implies that mean LOS was 1.3 times higher for PPCU as compared to NICU.
Total COS was lowest for infants discharged from the NICU (median: $25,745) and highest for patients discharged from PRH (median: $60,528), despite the lower cost per day at PRH (PRH: $1,592 vs NICU: $1,980). The mean COS was 1.4 (95% CI: 1.2,1.8) times higher for AC and 2.3 (95% CI: 1.8,3.0) times higher for PRH discharge than for NICU discharge. Mean COS was 1.7 times higher for infants with benzodiazepine exposure. Interestingly, infants born to mothers on marijuana or buprenorphine had approximately 28% lower mean COS as compared to unexposed infants. (ie., the 28% estimate was derived by taking the exponent of the adjusted estimate from Table 2 with respect to buprenorphine use and comparing to 100%, for example: exp(–0.330) = 0.72 leading to 28% lower).
Median cumulative morphine dose was much higher for infants discharged from PPCU or PRH than for those discharged from NICU (2.7 mg (0.9 mg/kg) (NICU), 4.7 mg (1.6 mg/kg) (AC), and 16.7 mg (5.3 mg/kg) (PRH) p < 0.001). Infants discharged from PPCU had a 2.1 (95% CI: 1.3,3.6 times higher mean cumulative morphine dose and infants discharged from PRH had 3.5 (95% CI: 2.0,6.1) times higher mean cumulative morphine dose than those discharged from NICU. Adjusting for other significant predictors, infants born to mothers on benzodiazepines had 2.1 times higher mean cumulative morphine dose as compared those unexposed, while infants born to mothers on tobacco had 59% lower mean cumulative morphine dose as compared to those unexposed.
While treatment of NOWS has traditionally occurred mainly in the NICU, the paradigm may be shifting, with emerging evidence for treatment outside of the ICU environment [11, 13]. Given the significant costs associated with treating NOWS [1, 15], the most efficient care location should be considered. While some studies have examined outcome differences for management in pediatric floors or a residential facility [11, 13], and another addressed the prolonged length of stay associated with transfer of Medicaid NOWS infants to another hospital [1]; none to our knowledge has specifically addressed convalescence cost in a rehabilitation hospital. As our institution needs to maintain availability of ICU beds for critically-ill infants, transfer to a rehabilitation hospital is an important mechanism for the transition to discharge. However, in our study, infants transferred to PRH had a higher associated LOS, COS, and cumulative dose of morphine; though the cost is likely to be primarily driven by the longer length of stay.
Our study shows that 31% of the NOWS infants were transferred to a community pediatric rehabilitation hospital, with a significantly increased total LOS. In line with our findings, a study examining different management locations cited a median LOS of 24 days for NICU, 26 days for a NOWS unit, and 33 days for an outpatient center [13]. While their LOS differed from ours, their trend towards longer LOS for infants managed outside the hospital of birth is similar. Alternatively, a 2019 study examined NOWS treatment in a pediatric floor and reported an average LOS of 27 days for NICU and 14 days in the pediatric floors, [11] though this study did not involve a NICU to pediatrics floors transfer.
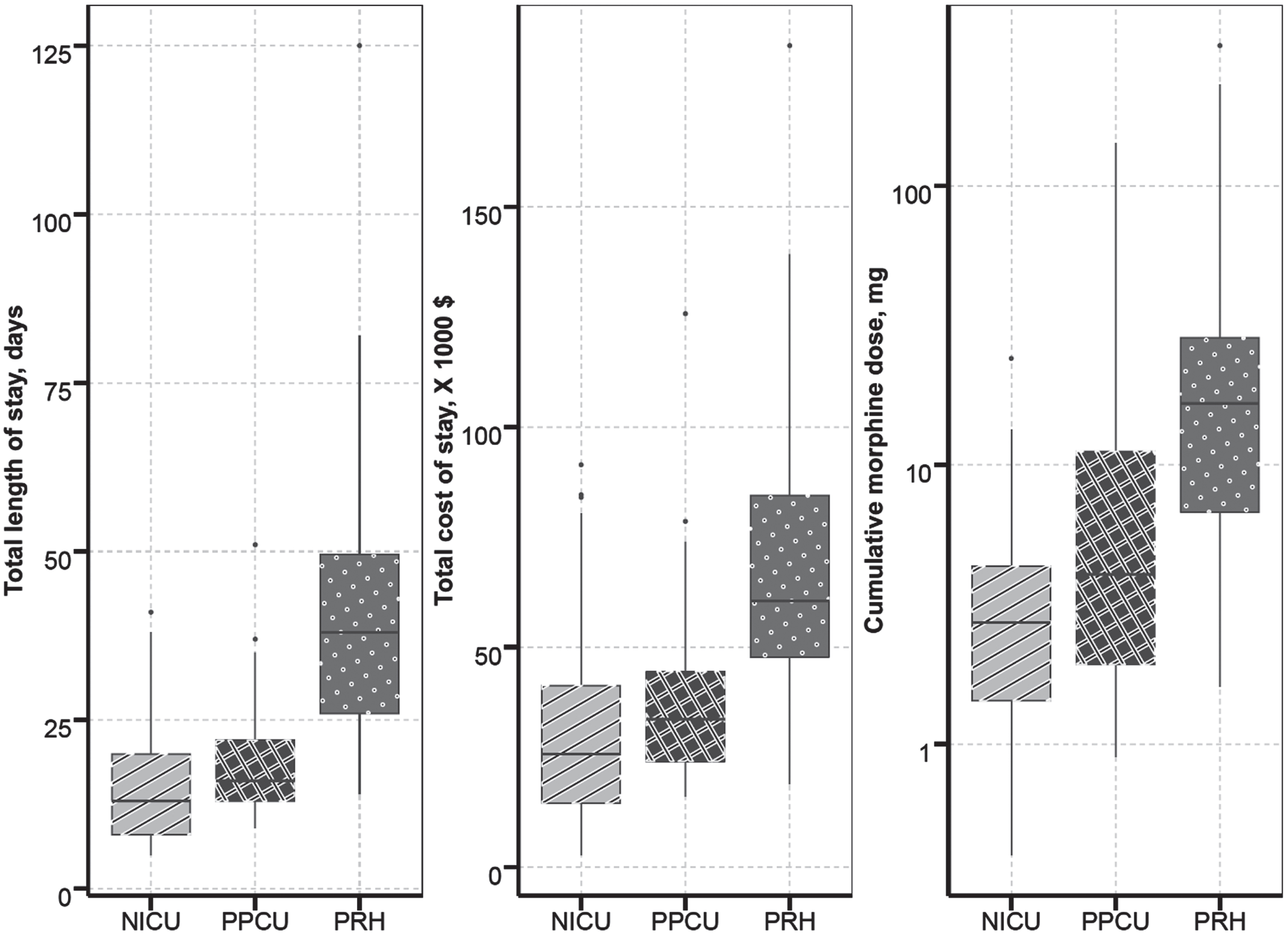
Distribution of total length of stay, Total cost of stay (x 1000) in dollars and Cumulative morphine dose by location of discharge (NICU, PPCU and PRH). Note: NICU: Neonatal intensive care unit, PPCU: Pediatric progressive care unit, PRH: Pediatric rehabilitation hospital.
Another contributor to the increased LOS observed with PRH discharge may be inherent to the transfer process itself. Wait time for placement/bed availability ranges from days to weeks. Bed availability is communicated 1-2 days before transfer, during which time insurance approval must be obtained. Occasionally, planned transfers are deferred with little to no notice due to lack of timely insurance approval, with reasons ranging from inactive insurance status to anticipated discharge within the next week. Additionally, transfers are sometimes postponed to accommodate more urgent transfers. Many infants in the PRH group spent some time in the PPCU while awaiting bed placement at PRH, which likely delayed medication weans due to the inherent lack of continuity in multiple transfers. Also, the increase in total duration of hospitalization associated with the transfer to another convalescence care hospital could be explained by the interruption in the standardized care provided in the transferring facility as well as the required period of familiarization by providers [16].
A substantial increase in resource utilization, especially for Medicaid, was associated with the surge in hospitalization secondary to NOWS [9]. The current study revealed that although the cost/day in a PRH was the lowest, the prolonged LOS made the total cost expenditure per NOWS patient the highest in the three clinical settings. The average COS for infants with NOWS ranges from $37,000 to $79,000 depending on factors such as timing, LOS, and need for pharmacotherapy [1, 7]. Patrick and colleagues reported a 35% increase in COS for NOWS infants, from $39,400 in 2000 to $53,000 in 2009, with 78% of charges attributed to Medicaid [1]. Comparable costs were revealed by our study, with a median COS of $25,745 to $60,528, based on similar factors in addition to discharge location. A recent national estimate cited a mean additional cost of $16,400 for NOWS admissions compared to birth hospitalization without NOWS [9].
Different treatment settings for infants with NOWS cited median COS of $90,601 for the NICU, $68,750 for a dedicated NOWS unit, and $17,688 for an outpatient neonatal withdrawal center despite a longer LOS for the outpatient center [13]. In contrast, our study reported lower hospital costs, with median COS of $25,745 (NICU), $33,610 (PPCU), and $60,528 (PRH). The longer LOS for PRH discharged infants outweighed its lower average daily cost, making PRH discharge the costliest of the three options.
The increased LOS and COS at PRH found in our study were associated with multiple risk factors. First, prenatal co-exposure of NOWS infants to methadone and benzodiazepine were independently associated with longer LOS, consistent with current literature [17–22]. Infants exposed to benzodiazepines had longer LOS and higher cumulative dose of morphine, consistent with the drug’s ability to enhance the action of the central nervous inhibitory neurotransmitter; g-aminobutyric acid receptor [23].
Buprenorphine, however, was associated with a shorter LOS and a low rate of PRH transfer, also consistent with emerging literature [24–32] indicating shorter LOS for infants with exposure to buprenorphine than for other substances (e.g. heroin, methadone). Buprenorphine is a partial mu-opioid agonist with lower intrinsic receptor efficacy than methadone, [33] and is primarily metabolized by CYP 3A4 that is substantially reduced in neonate, thus decreasing drug clearance [34, 35], possibly contributing to less severe withdrawal.
Interestingly, the prenatal opioid co-exposure to marijuana was associated with decreased cost. There is early evidence suggesting the use of marijuana can potentially prevent or decrease opioid use in pregnancy thus ameliorating the severity of withdrawal [36]. However, there is also conflicting evidence that marijuana brain receptor (CB1) agonizes the effects of opioids and may increase withdrawal [37].
This study does have several limitations as a retrospective chart review. A relatively small sample size was included in the analysis as the cost expenditure data is only available for the past 5 years. The COS was unavailable for patients prior to 2015 and for 8 patients meeting inclusion criteria. The prenatal doses of methadone and buprenorphine administered prior to delivery were not available for correlation with study outcomes. While we do not believe this affected our results, we recognize it impacts data completeness. Lastly, we were unable to quantify wait times for PRH transfer. Since we believe this directly contributes to LOS, it will be important to quantify in future studies. Furthermore, given the longer LOS observed at PRH despite similar LOS in the NICU prior to transfer, it is possible that those being transferred experienced more severe withdrawal for reasons not yet addressed in the literature. Given the substantial knowledge gaps in the complex entity of NOWS, further study is needed to adequately explore this possibility.
LOS, COS, and opioid treatment doses were all greater for NOWS patients transferred to a pediatric rehabilitation (PRH) hospital for convalescent care. Although the daily cost at PRH is the lowest, the costs incurred with prolonged hospitalization surpass cost-effective benefits of the transfer. There is an identifiable subgroup of infants with recognized longer withdrawal; infants exposed to Methadone and/or co-exposed to benzodiazepines may benefit from earlier transfer to convalescent care facilities. Our findings are an important early step to informing a holistic model of care and strategic planning for patients affected by NOWS. While a comprehensive explanation for these differences has yet to be determined, further investigation is warranted given the substantial opportunity for cost savings and earlier discharge to home.
Footnotes
Acknowledgments
We thank Patrick Kenville, Senior Decision Support Analyst for providing the direct variable costs for infants admitted to the neonatal intensive care and the pediatric progressive care Units at the University of Maryland. We also thank Linda Carson, Director of Health Information & Privacy Officer, for providing the medical records of the neonates transferred to the pediatric rehabilitation hospital; Mt. Washington Pediatric Hospital.
Disclosure
The authors have no competing financial interests to disclose.