
Abstract
BACKGROUND:
Kangaroo mother care (KMC) is defined as prolonged skin to skin care between a mother and infant with the infant lying in prone position on mom’s chest. KMC decreases morbidity and mortality and promotes physiologic stability. The aim of this study is to measure work of breathing (WOB) during KMC in very low birth weight (VLBW) infants on non-invasive respiratory support.
METHODS:
A prospective observational pilot study was conducted comparing WOB indices during standard care (SC) and KMC. Respiratory inductive plethysmography (RIP) measured WOB indices non-invasively: phase angle and labored breathing index. VLBW infants who were stable on non-invasive respiratory support were randomized to receive RIP measurements during KMC or during SC first. Summary statistics and mixed linear models were used to compare WOB and vital signs.
RESULTS:
A total of 32 infants were consented for the study, data collection and analysis was completed on 28 infants. There were no significant differences in mean phase angle during KMC or SC (73.5±4.6 SE deg vs 66.8±3.9 SE deg, p = 0.25). No differences in WOB and vital signs were detected. Controlling for respiratory support or randomization/first location did not change the results.
CONCLUSION:
In this pilot cohort, infants demonstrated no differences in work of breathing indices or oxygen saturation during KMC or SC while receiving non-invasive respiratory support. KMC appears to be safe and well tolerated with no worsened WOB. Larger studies should be performed to confirm our findings.
Abbreviations
Very low birthweight
Kangaroo Mother Care
Respiratory Inductance Plethysmography
Nasal cannula
High flow nasal cannula
Continuous positive airway pressure
Work of breathing
Labored breathing index
Heart rate
Respiratory rate
Oxygen Saturation
Standard Care
Bronchopulmonary dysplasia
Patent ductus arteriosus
Intraventricular hemorrhage
Introduction
Premature birth is a significant cause of infant and child morbidity and mortality [1]. In the United States, preterm births account for 9.5% of all births. Very low birth weight (VLBW) infants account for 15% of preterm infants [2]. Survival among VLBW infants has increased over the past ten years but survival without morbidity has remained stable [3].
Kangaroo mother care (KMC) is defined as prolonged skin to skin care between a mother and her infant with the infant lying prone on the mother’s chest [4]. KMC decreases morbidity and mortality and promotes physiologic stability in preterm infants [5–7]. A 2016 meta-analysis of all low birthweight infants demonstrated less tachypnea, higher oxygen saturation, and less apnea during KMC [8]. Additional studies have shown improved cardiorespiratory control among infants undergoing skin to skin care [9–11]. The physiologic reason for these observed benefits has yet to be defined.
In addition to cardiorespiratory benefits, KMC has also been associated with increased breastfeeding rates among preterm infants, enhanced mother/infant bonding, greater weight gain, lower nosocomial infections, increased tolerance to procedural pain, and improved neurodevelopmental outcomes at 5 and 10 years [12–15]. Despite strong evidence, routine KMC has yet to be fully incorporated into many neonatal intensive care units due to residual concerns posed by earlier, largely discounted studies assessing the safety of the practice [16].
Respiratory inductive plethysmography (RIP) is a tool used to assess thoraco-abdominal motion. Thoraco-abdominal synchrony plays a role in the efficiency of lung ventilation and synchronous thoraco-abdominal motion represents calm, efficient breathing [17, 18]. During normal breathing, the diaphragm contracts during inspiration resulting in outward abdominal motion followed immediately by outward rib cage motion [19]. With increased work of breathing (WOB), the rib cage lags behind abdominal wall movement and this asynchrony leads to diaphragmatic muscle fatigue and increased energy expenditure [20, 21]. RIP obtains measurements using the relative timing and amplitude of ribcage and abdominal excursions during respiration and can provide an objective measurement of work of breathing indices. Although pneumotachograph is considered the gold standard for tidal breathing measurements, this technique is invasive and difficult to perform, may alter breathing pattern, and cannot be done for an extended period of time. RIP is an accepted noninvasive technology for monitoring breathing patterns and has been shown to provide accurate tidal volume measurements of infants in both the prone and supine positions [22]. RIP has been used in multiple studies to assess breathing in premature infants, but normative values have not been established [20, 23].
Previous studies have demonstrated improved physiologic stability during KMC but to our knowledge, no studies have assessed the impact of KMC on work of breathing indices. Thus, based on the positive physiological responses associated with KMC, we hypothesize that work of breathing will improve during KMC in VLBW preterm infants on non-invasive respiratory support.
Methods
This prospective pilot study was conducted at the Christiana Care Neonatal Intensive Care Unit from November 2018 to March 2020. The trial was registered on clinicaltrials.gov, NCT03683316. After Institutional review board approval, consent was obtained from mothers of enrolled infants prior to the initiation of the study. All infants were de-identified after demographic, clinical, RIP and pulse oximetry data were extracted from the electronic medical record.
Inclusion criteria included infants with a birth weight < 1500 g who were > 4 days post-natal age and were on non-invasive ventilation (nasal cannula (NC), high flow nasal cannula (HFNC), or continuous positive airway pressure (CPAP) for≥12 hours and requiring≤40% supplemental oxygen. Infants with skeletal, neuromuscular, or abdominal surgical disorders were excluded due to possible effect on accuracy of work of breathing (WOB) measurements. Infants who did not meet criteria to participate in KMC at our institution were also excluded. This included infants diagnosed with persistent pulmonary hypertension of the newborn, pneumothorax requiring chest tube placement, and/or seizures.
Respiratory Inductance Plethysmography is a non-invasive method to determine WOB indices. RIP obtains tidal breathing measurements via thoracoabdominal motion analysis on digital signals associated with rib cage and abdominal wall motion. RIP involves the use of two soft, elastic, cloth bands (Respibands Plus, Viasys, San Diego, CA or NOX RIP Belts, Nox Medical, Iceland) encircling the rib cage and the abdomen. The bands contain a flexible sinusoidal wire that can measure motion. The relative motions of the rib cage and abdominal bands are analyzed to determine WOB indices as previously described [24]. The presence of thoracoabdominal asynchrony is reflective of increased WOB.
The pneuRIP instrument and software package (Creative Micro Designs, Newark, DE) allows the digital transfer and instantaneous analysis of RIP data on an iPad (Fig. 1). The validation of this research method has been previously published and has been shown to be consistent with the traditional approach using the Respitrace system (Sensormedics, Yorba Linda, CA) [25–28].
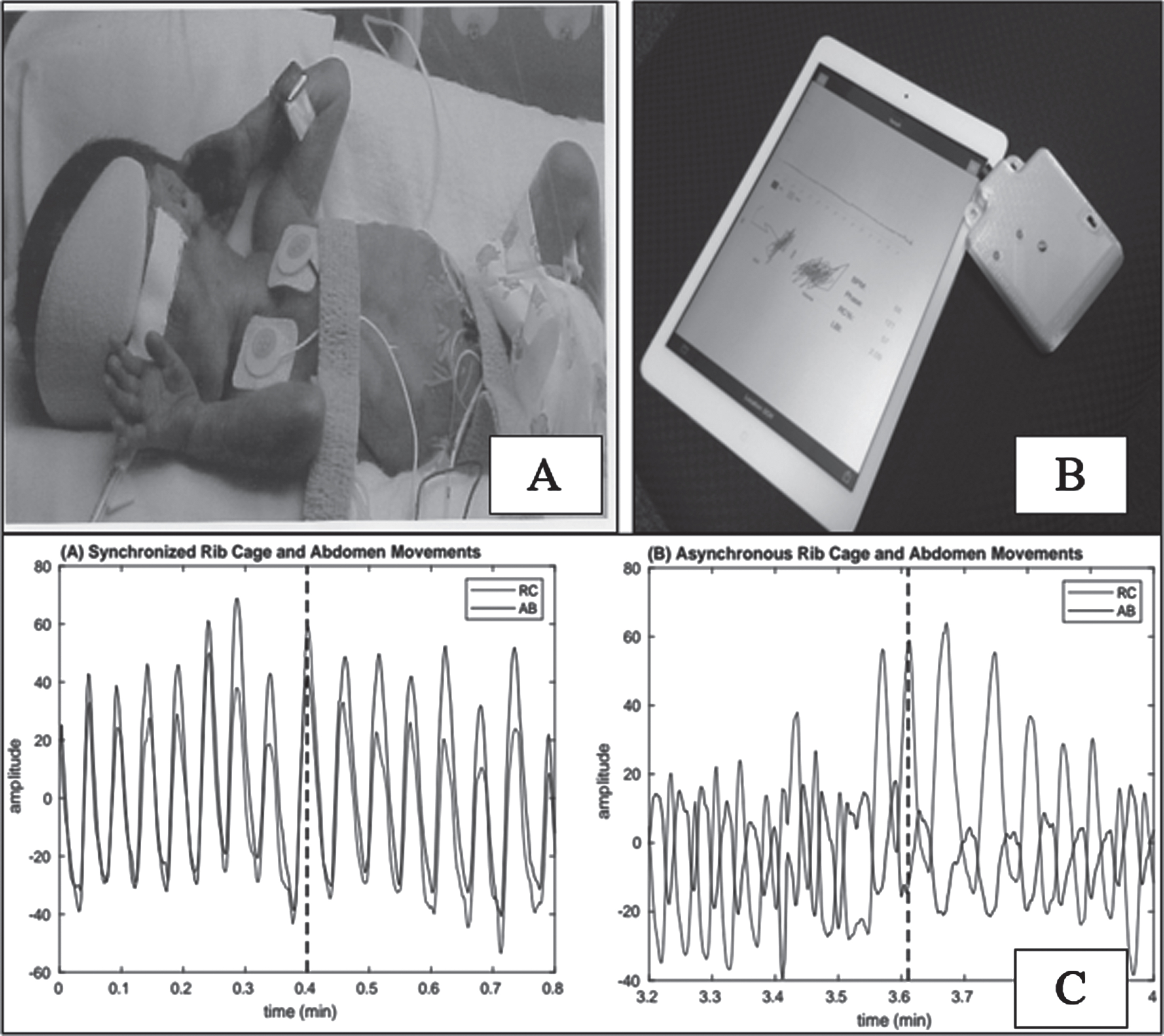
Respiratory Inductance Plethysmography Schematic. Bands with sinusoidal wires are placed around the chest and abdomen of the premature infant (A). A transmitter receives output from the bands and sends data to the iPAD with pneuRIP software (B) Synchronized and asynchronized breathing patterns and WOB measurements are displayed on the screen (C).
Phase Angle is defined as the phase shift between the abdominal and rib cage excursions. A phase angle of zero degrees represents perfect synchrony whereas a phase angle of 180 degrees represents complete asynchrony. Based on previous studies, a value of≥40 represents the start of asynchrony and increased WOB [27].
Labored breathing index (LBI) is defined as the sum of maximal excursion of the ribcage and abdomen divided by the tidal volume. A value of one represents perfect synchrony and greater than one represents paradoxical motion of either the rib cage or abdomen. This index is a relative number as the RIP measurements are uncalibrated and the tidal volume is therefore an arbitrary volume [20].
The primary outcome is the average phase angle during Kangaroo Mother Care compared to the average phase angle during standard incubator or crib care. Secondary outcomes included heart rate (HR), respiratory rate (RR), oxygen saturation (SpO2) and LBI.
After written informed parental consent was obtained, infants were randomized to receive either RIP measurements during KMC or standard incubator/crib care (SC) first. Infants were randomized to ensure that any observed differences were not due to the order of measurements. Standard Care First represents infants who were randomized to have measurements taken in the SC position first. Kangaroo Care First represents infants who were randomized to have measurements taken in the KMC position first.
After randomization, all infants were placed prone for at least 30 minutes prior to the study. Soft elastic cloth bands were placed around the chest and abdomen of the infant and connected to a receiver. RIP data is transmitted wirelessly from the receiver to a study iPad. Measurements were taken after a five minute stabilization period and for at least 20 minutes in each position (Fig. 2). During KMC, mothers held infants while sitting in a reclined chair. The angle of recline was determined by maternal preference and comfort. All study measurements were made in the prone position and each infant only participated once. A research team physician was present throughout the study with the plan to intervene and stop the study procedures if the infant became unstable or hypoxic.
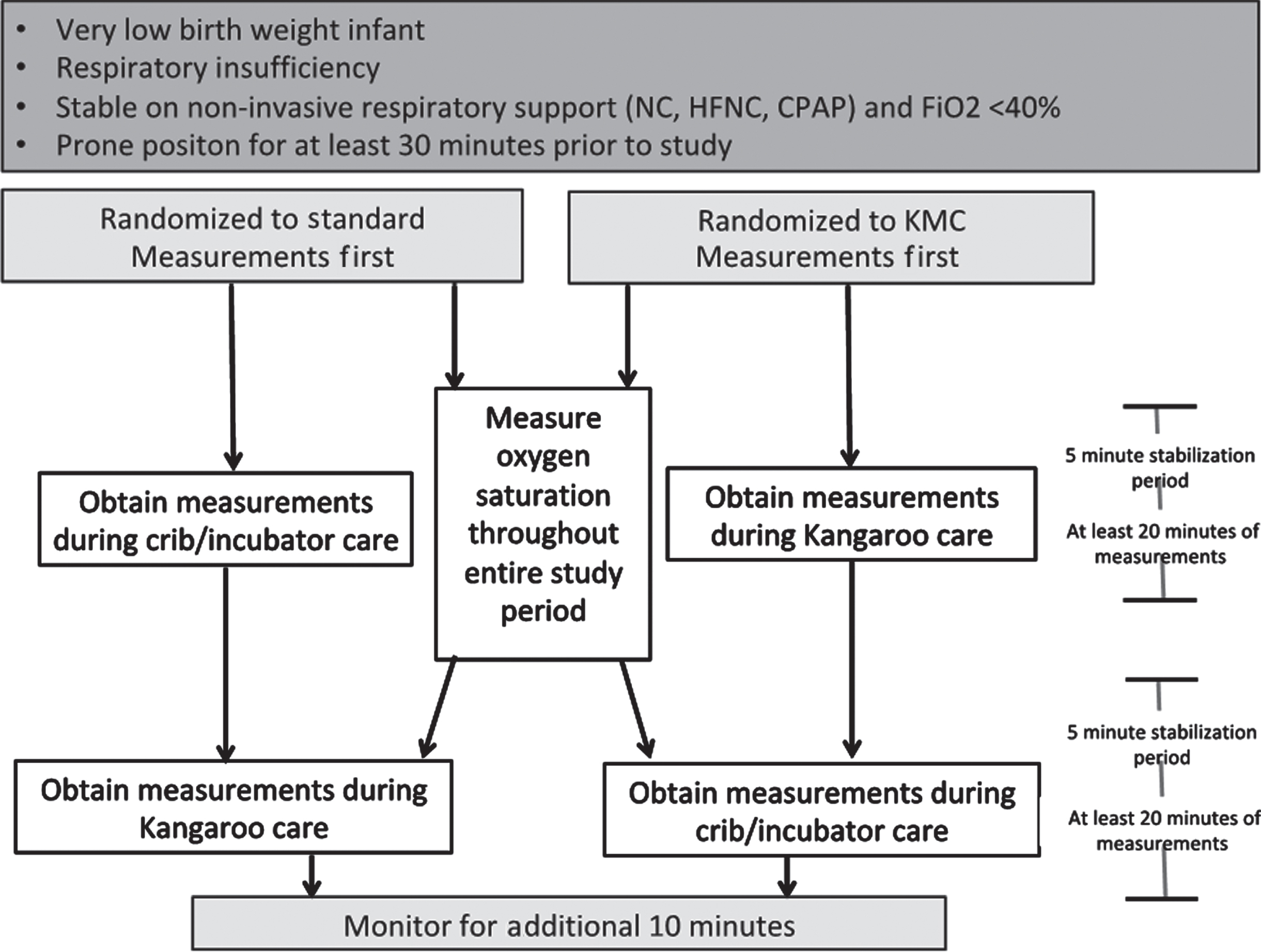
Study inclusion criteria and flow algorithm.
Data were analyzed on a study iPad using pneuRIP. Data with poor signals (RR < 5 or > 120, LBI < 1 or > 5) were excluded. For pulse oximetry data, a high-resolution pulse oximeter with 2 second sampling (Masimo Rad 87) was placed on the preductal extremity. Oxygen saturation was recorded continuously throughout the study period. Demographic and clinical characteristics were collected from the electronic medical record. Clinical characteristics included Post Menstrual Age (PMA), weight, caffeine exposure, and diagnosis of bronchopulmonary dysplasia (BPD), patent ductus arteriosus (PDA), or intraventricular hemorrhage (IVH) at the time of the study. Baseline respiratory support (NC, HFNC, CPAP) and oxygen requirements were recorded throughout the study.
This study was designed as a pilot study. RIP measurements have never been performed in this population and normative WOB indices values have not been established. A goal sample of 30 infants was selected.
Baseline and demographic characteristics were compared between groups using standard statistical measures, including chi-squared test and Student’s t-test as appropriate. Univariable analysis of mean phase angle, labored breathing index, mean respiratory rate, and oxygen saturation were compared using a paired t-test. A linear mixed effect model was used to determine the effect and interaction of KMC vs SC on WOB indices while controlling for respiratory support. A p value < 0.05 was considered statistically significant.
A total of 52 infants were eligible for the study. Enrollment was terminated prematurely due to institutional restrictions on clinical research during the COVID-19 pandemic. The final cohort included 28 infants (Fig. 3). The final analysis included 78% of total collected data after exclusion of low quality RIP data associated with movement artifact and/or sudden changes in respiration not associated with quiet breathing (cough, swallow, etc). No apnea events were recorded during the studies and no studies were stopped prematurely.
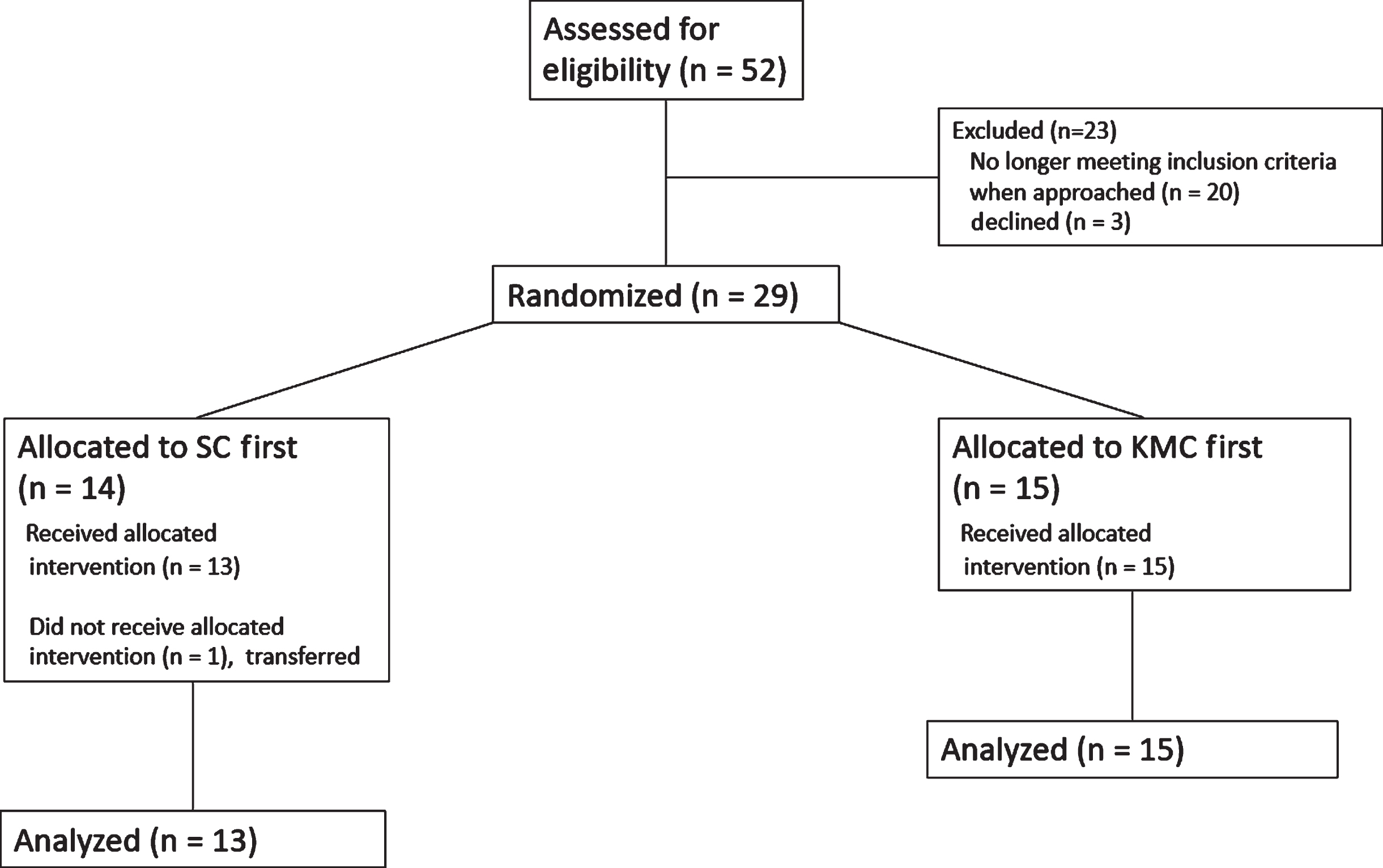
Study enrollment diagram.
The mean gestational age and birthweight for the entire cohort (n = 28) was 27.8 (±1.6 SD) weeks and 974.5 (±256.1 SD) grams. Most infants were White, male, on high flow nasal cannula (mean flow 3 LPM, range 1.5–6 L), and were receiving caffeine for apnea of prematurity. Demographic and clinical characteristics did not differ between randomization groups (Table 1).
Demographic and baseline characteristics. The values are mean and standard deviation or raw number and percent
GA: Gestational age; BW: birth weight; CPAP: continuous positive airway pressure; HFNC: high flow nasal cannula; NC: nasal cannula; FiO2: fraction of inspired oxygen; BPD: bronchopulmonary dysplasia; IVH: intraventricular hemorrhage; PDA: patent ductus arteriosus.
The mean phase angle among all infants in the cohort was 70.1 (±3.7 SE) degrees. Phase angle, LBI, SpO2, HR, and RR did not differ between the groups (Table 2). There was no difference in mean phase angle when stratified by randomization/first location (Fig. 4).
Primary and secondary outcome data
SpO2: Oxygen saturation; HR: heart rate; RR: respiratory rate.
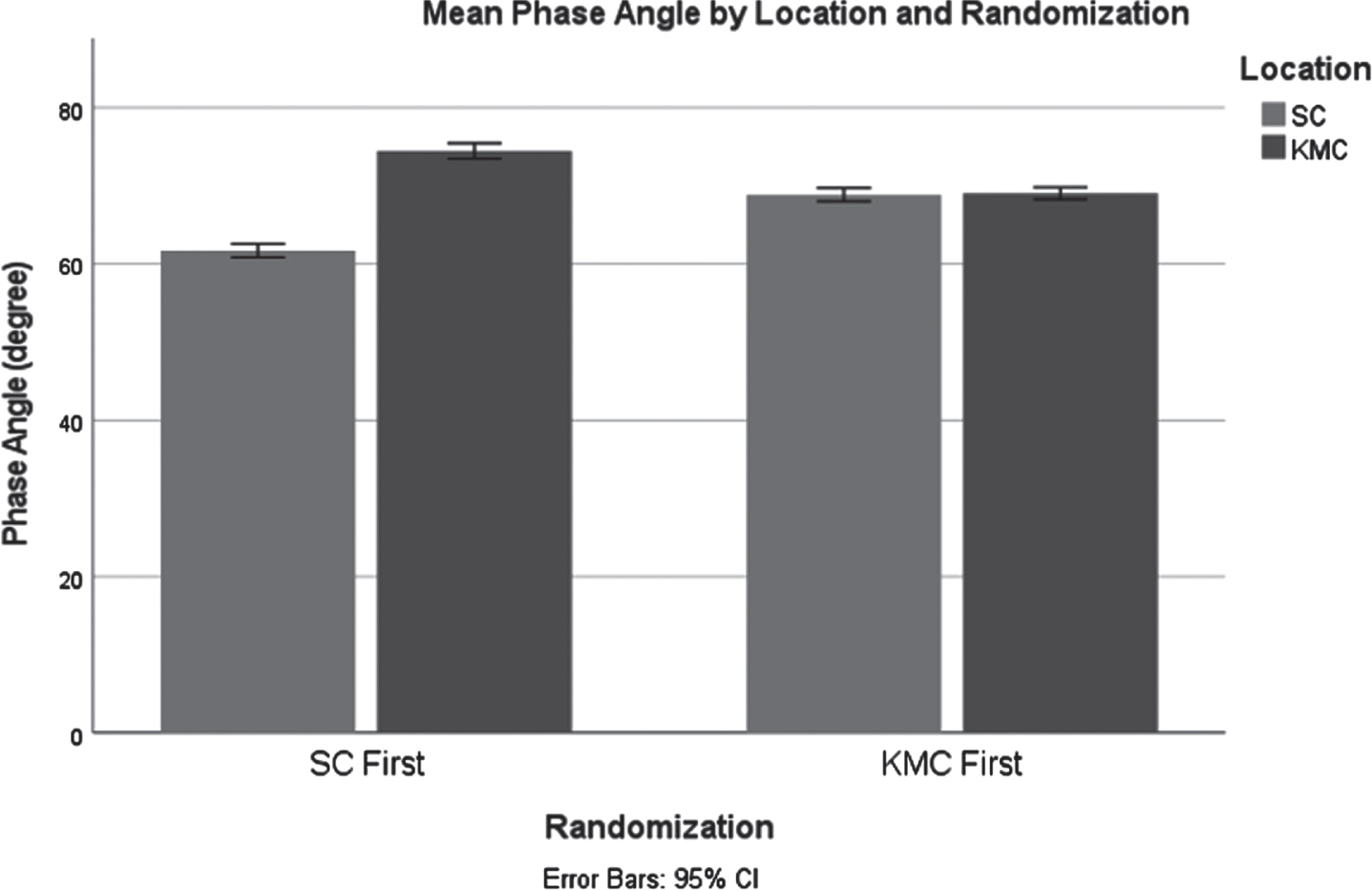
Mean Phase Angle during Standard Care and during Kangaroo Mother Care when stratified by randomization order. Phase angle was measured in degrees.
In univariate analysis, there were no differences in mean phase angle when evaluated by birth weight < 1000 g (KMC 76.6±5.2 SE deg. vs. SC 59.9±2.6 SE deg., p = 0.10) and 1000–1500 g (KMC 70.9±4.2 SE deg. vs. SC 72.7±4.3 SE deg., p = 0.78). The percent time spent with Sp02 < 90% in infants undergoing KMC was 15% vs 16% during SC (p = 0.88). Respiratory support (p = 0.03) but not KMC (p = 0.25) impacted mean oxygen saturation during the study period.
In a multivariate analysis, KMC did not impact work of breathing when corrected for respiratory support. Phase angle change between SC and KMC is +6.8 deg (95% CI –4.9, 18.4, p = 0.249). There was also no significant difference in LBI (increase of 0.05±0.04 SE, p = 0.25) or percent of rib cage involvement (decrease of 2.36±3.59 SE, p = 0.51) when correcting for respiratory support.
This prospective pilot study of VLBW infants demonstrates no differences in phase angle or oxygen saturation during Kangaroo Mother Care or standard incubator care while receiving non-invasive respiratory support. There was no evidence of worsening work of breathing indices while skin to skin with mother. Randomizing the order of SC or KMC measurements did not affect the results.
Often, VLBW infants are perceived to be too fragile and staff members and family worry that infants may decompensate during skin to skin [25]. Skin to skin contact between mother and infant encourages and integrates rhythmic, tactile, and sensory stimulation which promotes cognitive development [29]. These benefits are often unrecognized and therefore KMC is not routinely encouraged in many NICUs.
Our study supports previous research that KMC is safe in this patient population with respiratory insufficiency on non-invasive respiratory support. Ludington-Hoe et al. noted stable cardiorespiratory parameters and no bradycardic events during KMC in preterm infants [30]. Park et al. demonstrated no change in HR, RR, blood pressure or body temperature among infants 25–32 weeks’ gestation undergoing intermittent KMC [31]. A study of 45 preterm infants noted no hypothermic, bradycardic or desaturation events during KMC [32]. An additional study of twenty infants with average birth weight 1380 g who were either mechanically ventilated or receiving nasal CPAP noted no significant changes in temperature, respiratory rates or oxygen saturations during KMC [33]. The VLBW infants in our study tolerated KMC without increased work of breathing indices, vital sign instability, or increased respiratory support needs and no studies were stopped prematurely.
Although our study did not demonstrate improved cardiorespiratory stability during KMC, other studies have suggested improved oxygen saturation levels during KMC. Bier et al. demonstrated that low birthweight infants maintain a higher mean oxygen saturation during KMC and are less likely to have desaturation events less than 90% [10]. A retrospective review of 145 extremely low birthweight infants revealed that KMC was a protective factor for shortening non-invasive ventilation duration and supplemental oxygen support [34]. Bera et al. demonstrated that preterm infants had a mean average increase in SpO2 by 5% during KMC [35]. The percent of time that infants within our study spent < 90% SpO2 was less than 20% which was consistent with published acceptable ranges [36].
We hypothesized that infants would have improved work of breathing indices during KMC. We did not find evidence for this. We chose to place infants prone for SC (crib, incubator) measurements as this most closely mirrored how they would be positioned during KMC. It’s possible this impacted our results. Full prone positioning has been shown in other studies to improve thoraco-abdominal synchrony. Almost thirty years ago, Wolfson et al. demonstrated that phase angle was decreased in prone versus supine position in preterm infants recovering from respiratory distress syndrome [37]. Gouna et al. supported this finding and demonstrated significantly lower phase angles when prone as opposed to side-lying or supine [38]. Additionally, many infants were being fed during our study when skin to skin with their mother. Mild abdominal distension may have worsened our infants’ thoraco-abdominal asynchrony.
Strengths of our study include its prospective, pre/post, and randomizedd design, the use of PneuRIP technology to objectively measure work of breathing, and the use of a high-resolution pulse oximeter for continuous SpO2 monitoring rather than intermittent vital sign documentation. We eliminated data that did not meet a predefined standard and allowed for a 5 minute stabilization period which likely increased the accuracy of our data. Although designed as a pilot study, it was 90% powered to detect a 20 degree change in phase angle at alpha of 0.05 for our 28 patient cohort. It is unlikely that a larger sample size would identify a clinically significant change in phase angle but may be considered to determine the impact of KMC on WOB indices in certain subpopulations.
Limitations of our study include short duration of KMC, lack of standardization of maternal/infant positioning during KMC, sleep-wake cycles not documented, and inconsistent feeding during KMC. We chose to allow feeding as this is standard practice during KMC at our institution and it allowed mothers to spend the most time holding their infant between care times.
Conclusion
KMC appears to be safe and well tolerated in VLBW infants with regard to their respiratory status. Infants in our study maintained normal HR, RR and SpO2, though no significant respiratory benefits were noted during the duration of our intervention. We hope that this information will support the continued implementation and encouragement of KMC in this patient population however, larger studies should be performed to confirm our findings.
Footnotes
Acknowledgments
None.
Disclosure statement
The authors have no financial conflicts of interest to disclose.
Research involving human subjects was conducted in accordance with the ethical standards of all applicable national and institutional committees and the World Medical Association’s Helsinki Declaration.