
Abstract
OBJECTIVE:
To assess the claim that Parkinson’s disease (PD) specifically reduces religiosity religious faith and spirituality.
METHODS:
A longitudinal case-control study over 12 months of spirituality in 42 patients with idiopathic PD and 39 disease controls matched for age, gender, educational attainment and disability. There was no selection on grounds of religious affiliation. Participants were assessed on the Beck Depression Inventory, Medical Outcomes Score (MOS), cognitive tests including Paired Associate Learning [PAL], One Touch Stocking [OTS]) and Stroop test. Tests of spirituality were the Brief Multidimensional Measure of Religiousness and Spirituality questionnaire (BMMRS), a Mystical Experiences Questionnaire (MEQ), and the Rivermead Life Goals Score, supplemented by qualitative interview methods.
RESULTS:
Over one year, as expected, mobility and cognition declined in the PD group. However, there was no significant change in scores of religiosity and spirituality scores in this group. Likewise, there were no subjective reports of a decrease of interest in religious faith or spirituality, although anecdotal accounts of decreasing mobility, loss of driving ability, increasing emotional lability and tiredness meant reduced participation in some religious and spiritual practices. However, over one year there was a significant fall in controls’ religiosity score due mainly to a fall in ‘religious practices’ with no clear underlying reason.
CONCLUSIONS:
Compared to non-neurological patients with similar disability, Parkinson’s disease is not associated with a decline in religious faith or spirituality. Declining mobility and cognition in Parkinson’s disease does not lead to diminished religiosity.
Keywords
Introduction
Studying the effect of neurological disease on spirituality is important, not only to aid physicians, patients and carers understand their experience of the disease, but also because it may reveal the neuronal mechanisms underlying normal religiosity. Yet spirituality in neurological disease is rarely examined [Reviewed in (Coles & Collicutt, 2019)].
It would be unsurprising if people with Parkinson’s disease experience an alteration in spirituality, because the disease’s diffuse neuropathology (Braak & Del Tredici, 2017; Smith et al., 2019) leads to impairment of many cognitive processes (Piredda, Desmarais, Masellis, & Gasca-Salas, 2019), some of which are likely to subserve religious belief and thinking. However, a small literature claims there is a selective deficit of spirituality in Parkinson’s disease (P. M. Butler, McNamara, & Durso, 2010; P. M. Butler, McNamara, Ghofrani, & Durso, 2011; McNamara, Durso, & Brown, 2006). Elsewhere, we have argued that these studies are inadequately controlled for the physical, cognitive, emotional and social confounds of a progressively disabling disease (Redfern & Coles, 2015).
In this study of spirituality in Parkinson’s disease, we sought to minimise confounds by using both internal and external controls. We assessed changes in spirituality over one year in in a group of people with PD and compared results (i) internally, with changes in the PD group’s cognition and mobility; and (ii) externally, with a control group of people with non-neurological impairment of mobility. To capture nuances in participants’ experience and interrogate religious coping, we also conducted qualitative interviews. We tested the hypothesis that there is a selective defect in spirituality in Parkinson’s disease.
Methods
This study had approval from the ethics committee (REC 12/EE/0456) and Research and Development department at Addenbrooke’s hospital. All participants gave written informed consent.
Subject recruitment
142 PD patients from the PD Research Clinic database at the Cambridge Centre for Brain Repair were invited to take part. Eligible patients had a definite diagnosis of Parkinson’s disease (as diagnosed using UK Parkinson’s Disease Brain Bank criteria (Marsili, Rizzo, & Colosimo, 2018)), were aged >18 years, had no significant cognitive deficit (ie MMSE ≥25) (Folstein, Folstein, & McHugh, 1975) and had no history of head injury or substance abuse. Controls with non-neurological chronic diseases were recruited from rheumatology, respiratory and vasculitis clinics or were family members of the PD group. Selection criteria were: age >18 years and MMSE ≥25. Religious affiliation was not an eligibility criterion, and this study was not advertised in any religious contexts. Levodopa equivalent dosage was calculated using recognised formulae (Williams-Gray, Foltynie, Brayne, Robbins, & Barker, 2007).
Assessments
Participants were seen at baseline and then 12 months’ later (“year 1”), in their homes or a clinic room, with the same assessment procedures on each occasion. Age, handedness and years of education were noted; Parkinson’s medication, side of onset and years since diagnosis were recorded for the PD group. The Medical Outcome Study questionnaire (MOS) was given to assess physical disability (range 14–49, higher score reflects greater mobility; 14 signifies complete dependence, being chair or bed-bound; 49 fully independent and able to participate in vigorous sport) (Tarlov et al., 1989). The Beck Depression Inventory (Beck, Ward, Mendelson, Mock, & Erbaugh, 1961) in its current form [BDI-II] contains 21 questions, each answer being from 0 to 3, with higher scores denoting more severe depressive symptoms. The standardized cutoffs are 0–13: minimal depression; 14–19: mild depression; 20–28: moderate depression 9–63: severe depression. The Rivermead Lifegoals Score evaluated the participants’ priorities for personal care, hobbies, work, relationships and religion or life philosophy.(McGrath & Adams, 1999) with statements scored as follows: 0 = not at all important;1 = slightly important; 2 = moderately important; 3 = extremely important.
Cognitive function testing
Participants undertook the Mini-mental state examination (MMSE) as a measure of global cognitive performance (Folstein et al., 1975). They were also assessed using the ‘one touch’ Tower of London (or One-touch Stocking) (Owen et al., 1995), which tests executive functioning, specifically planning. We also used the Paired Associate Learning [PAL] test, which scores the accuracy of encoding and retrieving newly formed associations among stimuli. (Robbins et al., 1994). Participants completed all three stages of the Stroop test, which builds on the cognitive mismatch between text meaning and colour: colour reading, colour naming and colour-word interference, which involve the dorsolateral prefrontal cortex and anterior cingulate (Golden, 1978).
Religiousness and spirituality measures
One researcher (CR) carried out all the questionnaires face-to-face, phrasing questions similarly to all participants. The ambiguity of some questions tended to facilitate discussion. For example, the statement: ‘I find comfort and strength in my religion’ frequently provoked the response ‘What do you mean by religion?’ Participants were encouraged to use their personal interpretation of religion or spirituality in answering these. Finally, participants were asked whether their disease or disability affected their religious beliefs or practice.
The Brief Multidimensional Measure of Religion and Spirituality (BMMRS) questionnaire is a standardized US tool for measuring religiousness (Underwood et al., 1999) which addresses five domains of spiritual experiences and beliefs (positive and negative), public and private religious practices, and religious community support. Questions regarding ‘forgiveness’ were omitted because, in an earlier survey with a patient research support group, they were considered too ambiguous; the same participants criticised the protestant Christian bias of the questions (e.g. presupposing a personal relational God) which led to slight textual changes. The remaining 30 items were scaled using an established methodology (Johnstone, Yoon, Franklin, Schopp, & Hinkebein, 2009). “Combined religious support” was derived from combining the categories of “positive support” (knowing help is available from congregation) and “negative support” (feeling criticized by such a congregation) as both are related to the degree of involvement in the religious community. To complement the emphasis on theistic belief in the BBMRS, noted by the research support group, 4 statements were adapted from the Hood Mystical Experience Inventory (Hood, 1975) and Cloninger Temperament and Character Index (Cloninger, Svrakic, & Przybeck, 1993). These reflect classic accounts of mystical states (Eliade, 1957; James, 1902) asking about unifying quality, ‘I have had moments where I realized the oneness, or unity, of myself with everything else’, noetic quality, ‘I have had an experience where deeper aspects of reality were revealed to me’, loss of temporal/spatial awareness, ‘I have had an experience in which time and space seemed non-existent’ and connection with a transcendent power, ‘I have had personal experiences in which I felt in contact with a divine and wonderful spiritual power’.
Qualitative assessment
Because of the rich variety of responses about both religious beliefs and experiences which the various interview questions yielded, and also the physical, emotional and social effects of chronic disease on religious practice, and religious coping, a change to the protocol was approved, to enable audio-recording of responses in the second assessment. These accounts were transcribed, then analysed with the help of NVivo qualitative analysis software ("NVivo qualitative data analysis software: version 10,” 2014).
Statistics
Changes over one year in all group data were compared by parametric tests (Student’s T tests) paired within the PD cohort and unpaired between PD and controls, using Prism 5 for Windows.
Results
Subjects and baseline characteristics
44 PD patients were screened and 2 were excluded (cognitive impairment and diagnostic uncertainty). 39 controls with non-neurological chronic diseases were recruited from medical clinics (n = 27, with rheumatological, systemic vasculitic or lung diseases [without significantly reduced O2 saturation levels or CNS involvement]) or family members (n = 12, with lower back pain, serious back injury and multiple myeloma). All participants were white British apart from four of Asian origin (2 PD patients and their spouses, who agreed to act as controls).
PD patients had varying disease severity (Hoehn-Yahr stage 1 (n = 3), 2 (n = 23), 3 (n = 11), 4 (n = 3) and 5 (n = 2); disease onset was right-sided (n = 17), left-sided (n = 23) or neither (n = 7).
The two cohorts were well matched for baseline characteristics (Table 1) including depression scores although more PD patients were taking anti-depressant medication. Over the year of observation, three PD patients and one control died; two other controls left the study.
Demography and disease history at baseline and year 1
Demography and disease history at baseline and year 1
Both cohorts were well matched using self-designated religious affiliation (Table 2) with most choosing ‘Christian’. Some in this category were agnostic but identified themselves as Christian for ethical or social reasons. At baseline, there was no difference in spirituality scores between PD patients and controls. BMMRS mean scores for women were higher than for men (mean scores were 51.2 for women versus 40.6 in men in the PD group (p = 0.081) and 41.0 versus 52.9 (p = 0.046) in controls) mirroring what is seen in the general population (Beit-Hallahmi, 2014). Contrary to previous reports (P. M. Butler, McNamara, & Durso, 2011; Giaquinto, Bruti, Dall’Armi, Palma, & Spiridigliozzi, 2011) there was no effect of laterality of PD disease onset on these scores; a trend towards higher BMMRS scores with left-sided disease onset was due to the higher proportion of females in this subgroup.
Religious affiliation, spirituality and lifegoals scores
Religious affiliation, spirituality and lifegoals scores
All baseline data from those who subsequently died or left the study has been omitted. Over the year of observation, three PD patients and one control died; two other controls left the study. *Two left study, and one who was ‘agnostic’ at baseline, chose ‘christian agnostic’ at yr 1.
Although the group averages of BMMRS were not different between PD patients and controls, the profile of their scores was different (Fig. 2), specifically, at the higher end of the spread of spirituality scores, controls scored higher than PD patients. Qualitative data from the 10 highest scorers in the PD group provides a partial explanation. Eight of these were practicing Christians who had in the past been members of a church, one was a Buddhist and one was ‘spiritual but not religious’. Seven of these gave specific examples of how PD had affected their religious practice: one was too emotional to attend church, two had difficulty meditating, three had given up driving and this limited their ability to attend religious meetings; one had sleep problems so had reduced commitments because of tiredness.
All but 6 participants (4 PD and 2 controls) scored zero on the item “negative spiritual experiences” (feeling abandoned or punished by God); 5 of these six had significant depression (BDI >20).
Mobility declined significantly in the PD cohort (Figs. 13), as mean MOS fell from 35.4 (95% CI 32.8–38.1) to 33.3 (95% CI 30.5–36.1) (p = 0.006,). There was no significant change in the controls: 37.6 (35.0–40.2) at baseline versus 36.9 (34.0–39.8) at year 1 (p = 0.32). Likewise the PD group, but not the controls, showed a decline in cognitive function with PAL first trial memory score reduced from 13.74 (95% 12.88–14.61) to 12.49 (11.34–13.63) (p = 0.033 paired T test); and PD patients had a lower score than controls in the OTS test at year 1:14.53 (95% CI: 13.0–16.0) versus 16.5 (95% CI: 15.76–17.24) (p = 0.026). There were no other significant changes in cognitive outcomes.

Baseline BMMRS (by domain and total) and MEQ (Mystical Experience Questions) with 95% confidence intervals, for PD and control group.
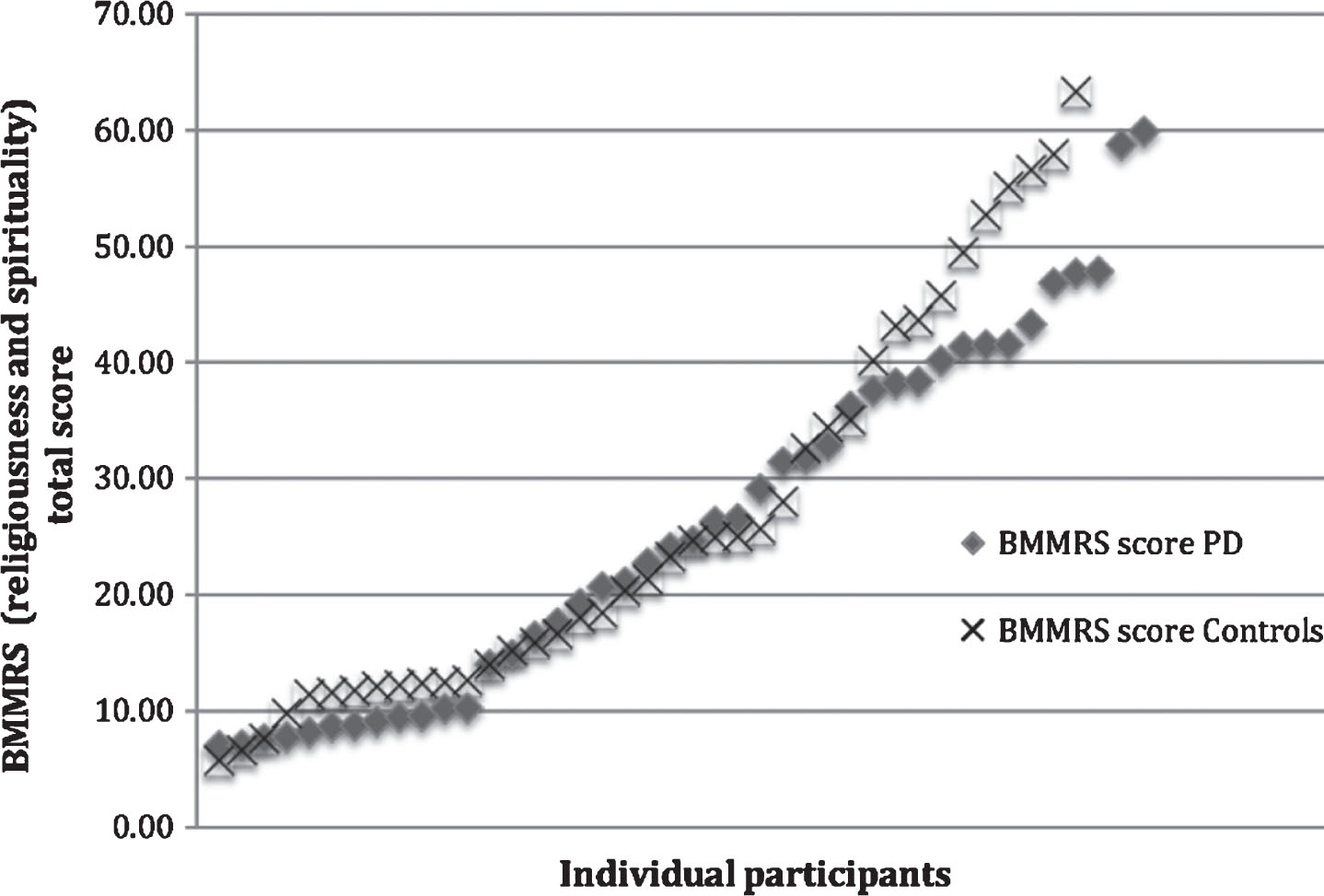
Distribution of spirituality (BBMRS) scores for participants at baseline.
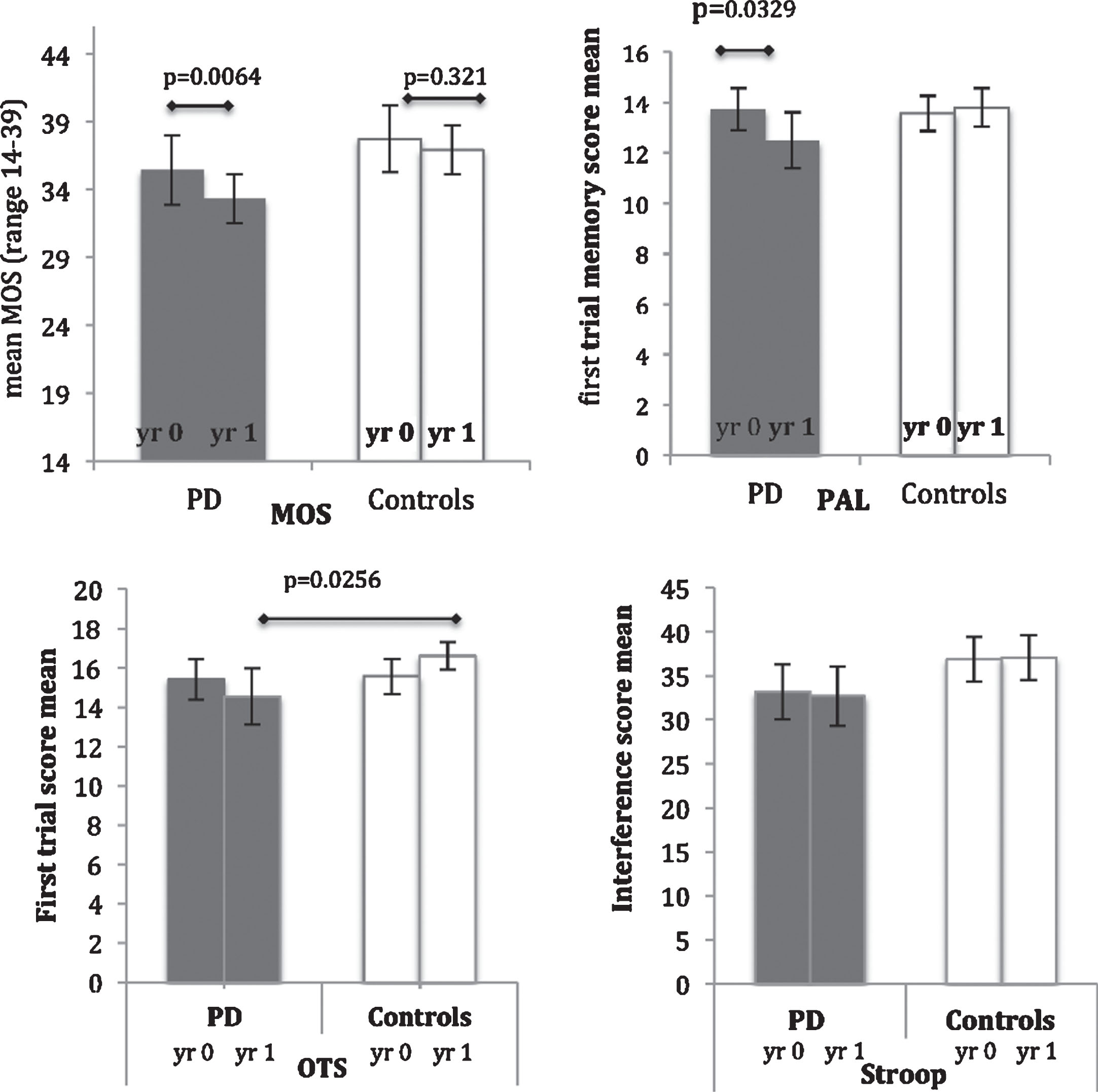
Change in selected mobility and cognitive scores over 12 months.
There was little change in self-designated religious categories (Table 2). And there was no change in any spirituality score of PD patients between baseline and year 1. However, there was a significant fall in controls’ BMMRS score from 26.0 (95% 20.4–31.7) to 23.7 (18.7–28.7) (p = 0.014) due mainly to a fall in ‘religious practices’ from 3.1 (95% CI: 1.9–4.2) to 2.6 (95% CI: 1.6–3.7) (p = 0.049; Fig. 4 and Table 2). There was no change in Rivermead Lifegoals scores.
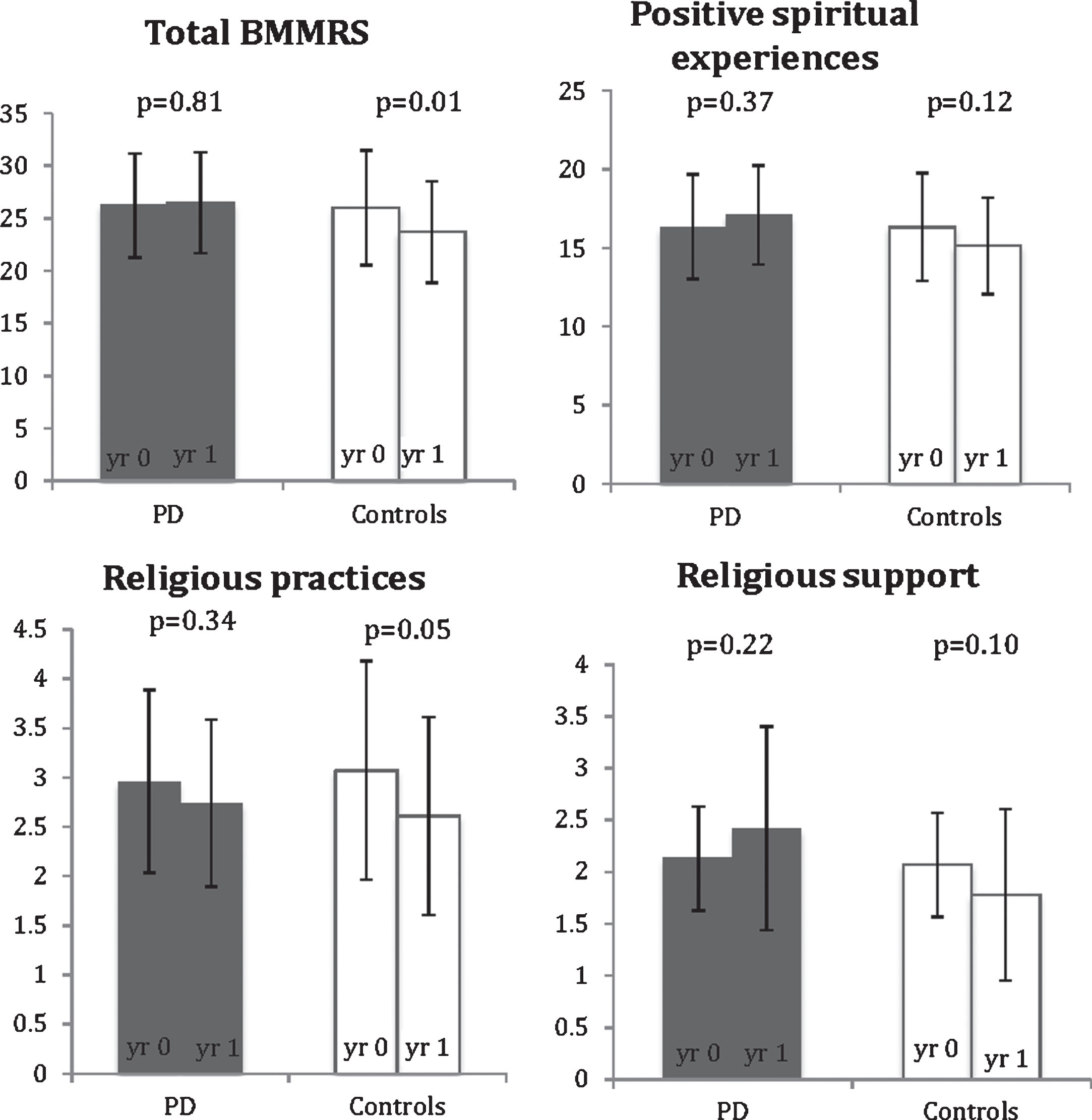
Change in selected spirituality score over 12 months.
Overwhelmingly, participants said their religious faith (or lack of it) had not changed with the onset of Parkinson’s disease. 3/42 PD patients said they blamed God or felt abandoned: “it’s easy to think you’ve, you’ve kind of been abandoned and then another day you’ll think well thank goodness you do believe that something is there because it’s … you can say well help me out with this, don’t let this happen” [a Christian]. Similarly, one participant, agnostic about God, mentioned his interest in spirituality had increased: “Well,..it has probably made me more interested … .because sooner or later it’s going to get worse - and I need to find some way of coping.” (You think it might help?) “It’s possible … yes.” [a Christian]. Many noted that PD interferes with practising a religious faith. “before I can meditate all day but now less...sitting just sitting is hard with the shaking … the dyskinesia, the shaking … But even so, I want to try it, it does help” [a Buddhist, who also mentioned being unable to visit the Buddhist temple as before]. Many mentioned practical difficulties about getting to church, for example: “I depend on my husband to drive me … and to walk me, in case … I need to have something to walk, to support me” [a Christian]. Most PD patients indicated that existential questions about the existence of God were important to them, whether they were religious believers or not. For example: “I know there’s a God I’m trying to prove to myself where he is, what he is, where he came from and whether he cares about us … . there’s a lot out there. A lot of religions give you a lot of insight into spirituality” [a Christian].
Many reported that their beliefs helped them cope with the disease. “I believe that I’m not alone, I’m not doing this myself, you know I’ve sat here and said well I’ve got these things I can either sit down and cry and rail and rant at the world and say why me or I can think well I’ve been given them for a reason I don’t know what the reason is, I may find out one day I may not, um, I believe I will, um, but I don’t think I’ve been given anything that I can’t cope with” [spiritual but not religious]. “I’m always conscious that there is somebody there to whom I can, whom I can raise my problems with … -yes -it’d be very much a loss without that” [a Christian]. “it’s an anchor, it’s helps me through difficult times, um, it’s a good feeling I think to have a belief, because otherwise you’ve got nothing” [a Christian].
Discussion
This controlled longitudinal study of people with established Parkinson’s disease does not show that spirituality is diminished over 12 months despite deterioration in motor and cognitive function. None of the PD group reported a loss of faith, and two specifically mentioned an increased interest during this short follow up time. However, Parkinson’s disease prevented people from attaining the highest scores in spirituality, in comparison to disease controls. At interview, it became clear that people with Parkinson’s disease had difficulty practising their faith but did not experience a change in their religious beliefs. Specifically, motor disability meant increased reliance on others to attend services, impairment in concentration interfered with practices such as meditation and emotional lability inhibited participation in public worship. Only three PD patients mentioned feelings of anger, though not entirely directed at God and also not persisting; these self-reported themselves as either being a Christian or ‘spiritual but not religious’. Conversely, qualitative accounts from some of the patients indicated religious faith was an important source of comfort as they faced their disease.
The study participants were broadly representative of a UK provincial population and were not enlisted on the basis of any declaration of faith, and were recruited in non-religious settings. The proportion who self-identified as Christians (55–61%) was representative of the population average (58% for Cambridgeshire, from the Office of National Statistics Review of Religion in England and Wales 2011 survey). Limitations of the study include its small size and the well-recognised difficulty in assessing spirituality. There is ambiguity in some questions of the BMMRS which, without care to ensure that the participants were all using similar interpretations, might lead to discrepancies. For example, scores for frequency of meditation could vary greatly depending on whether meditation was taken to mean a specific religious discipline requiring expert instruction or, alternatively, a form of praying without words or intention, or even just being thoughtful and calm. The BMMRS questionnaire is supposedly applicable to all faiths, however we found it difficult to ask questions in the ‘spiritual experience’ domain with Buddhist participants for whom the concept of God was irrelevant. Nevertheless, BMMRS correlated well with the importance attached to religion as reported in the qualitative interview. In the present study, we sought to reduce the variance introduced by these ambiguities by careful introduction to the questions, and by using the internal control of focusing on the change in scores over a year. This allowed us to assert that spirituality does not change as mobility and cognitive function deteriorate. This conclusion is only valid for moderately disabling Parkinson’s disease, as most of the cohort were at Hoehn-Yahr stages 2-3; it is possible that spirituality might be affected by later stages of the disease and also at diagnosis.
Our result contradicts a small literature (P. M. Butler et al., 2010; P. M. Butler et al., 2011; McNamara et al., 2006) from one group that claims there is a selective deficit of spirituality in Parkinson’s disease. We have argued elsewhere (Redfern & Coles, 2015) that these studies were not well controlled, in particular lacking controls with matched impaired mobility. In order to control for this, we used controls with non-neurological disease and similar levels of mobility impairment; we cannot explain why the spirituality scores of this group fell over one year. Our interviews of PD patients did not indicate any change in belief in people with Parkinson’s disease, and some suggested that religious faith and spirituality were important in coping with the effects of the disease.
We conclude that the personal experience of spirituality is not affected by declining mobility and cognitive function in moderately severe Parkinson’s disease. However, we did observe reduced participation of individuals in communal practices of religion as their disease progressed.
Conflict of interest
AC has received honoraria, travel support and grant funding from Genzyme (a Sanofi company); the University of Genzyme has also received funding from Genzyme. RAB has received honoraria from Springer and Wiley. He is in receipt of consultancy payments from LCT Sciences.