
Abstract
PURPOSE:
Complete whitening of one half of the thorax on a chest radiograph (CXR) is termed an opaque hemithorax. It often indicates the presence of significant pathology resulting in respiratory compromise. There are numerous causes of an opaque hemithorax, but these are not immediately apparent on CXR. Thoracic ultrasound (TUS) has a higher accuracy to differentiate between opacities on CXR and may help to correctly identify underlying pathologies. The purpose of this literature review is to report the causes of an opaque hemithorax, identify how TUS can assist diagnosis and explore the role physiotherapy has opaque hemithorax management.
METHODS:
A systematic search was conducted (PubMed, Medline, Embase, CINAHL, AMED and BNI) up until March 2018. Inclusion: Adults. Primary research reporting a complete opaque hemithorax on CXR.
RESULTS:
1117 papers were identified in search. Following inclusion and exclusion criteria: 58 papers were selected. 54 papers were case reports and four were observational studies. The causes of the opaque hemithorax were collated and divided into 16 categories. Eight studies included the use of TUS to differentiate the cause of the opaque hemithorax. Two studies reported the involvement of physiotherapy in opaque hemithorax.
CONCLUSIONS:
Numerous pathologies can cause an opaque hemithorax on CXR making differential diagnosis difficult. Even when mediastinal shift is present it does not appear to be a reliable way to identify the underlying cause. Thoracic ultrasound has the potential to much more accurately differentiate between pathologies. This would assist physiotherapists to identify patients amenable to physiotherapy treatment techniques.
Introduction
Complete whitening of one half of the thorax on a chest radiograph (CXR) is termed an opaque hemithorax and commonly referred to as a “whiteout”. It often indicates the presence of significant pathology resulting in respiratory compromise necessitating medical intervention and, on occasion, a referral for “chest” physiotherapy. There are numerous causes of an opaque hemithorax, but these are not all immediately apparent on CXR which makes differential diagnosis difficult. One method of diagnosis is based on the volume of the affected hemithorax as determined by the positional shift of the mediastinum or more specifically the trachea on CXR. The accuracy of this technique is, however, questionable. According to a recent systematic review thoracic ultrasound (TUS) has a higher accuracy to differentiate between opacities on CXR [1] and may help to correctly identify the underlying pathologies causing an opaque hemithorax. The purpose of this literature review is to report on the varied causes of an opaque hemithorax, identify how mediastinal positioning can assist in its diagnosis as well as explore the roles TUS and physiotherapy have in the management of an opaque hemithorax.
Methods
A systematic search of electronic databases (Medline, Embase, PubMed, CINAHL, AMED and BNI) was conducted up until March 2018. The following search terms were combined: “hemithorax” or “hemi-thorax” or “hemithora*” or “opaq*” or “opac*” or “whiteout” or “white-out” or “white out”. Inclusion criteria: Primary research published in any language reporting a complete opaque hemithorax on CXR. Study subjects are adults (18 years or over). Conference abstracts published in English were also included. Exclusion: Animal or tissue studies. Duplicate papers within or between databases were excluded. The remaining full-text papers were screened by two reviewers (SH and LH). Discrepancies between reviewers were resolved through consensus. Papers that met the inclusion criteria had the following information extracted: Cause of the opaque hemithorax, report of mediastinal shift to determine opaque hemithorax on CXR, use of TUS to assist in diagnosis and involvement of physiotherapy within the management strategy of an opaque hemithorax.
Results
A total of 1117 papers were identified in the database searches. Following removal of duplicates and application of the inclusion and exclusion criteria 58 full papers or abstracts were selected (Fig. 1). Four of the papers were observational studies [2–5] and included a total 249 subjects between them. Two of the four observational studies were reported by the same team from Taiwan [4, 5]. The other two separate papers both reported on an Indian (Indian subcontinent) subject population [2, 3]. Fifty-four (93%) of the papers were case reports [6–58] or case series [59] with many reporting rare and unusual causes of opaque hemithoracies (Table 1).
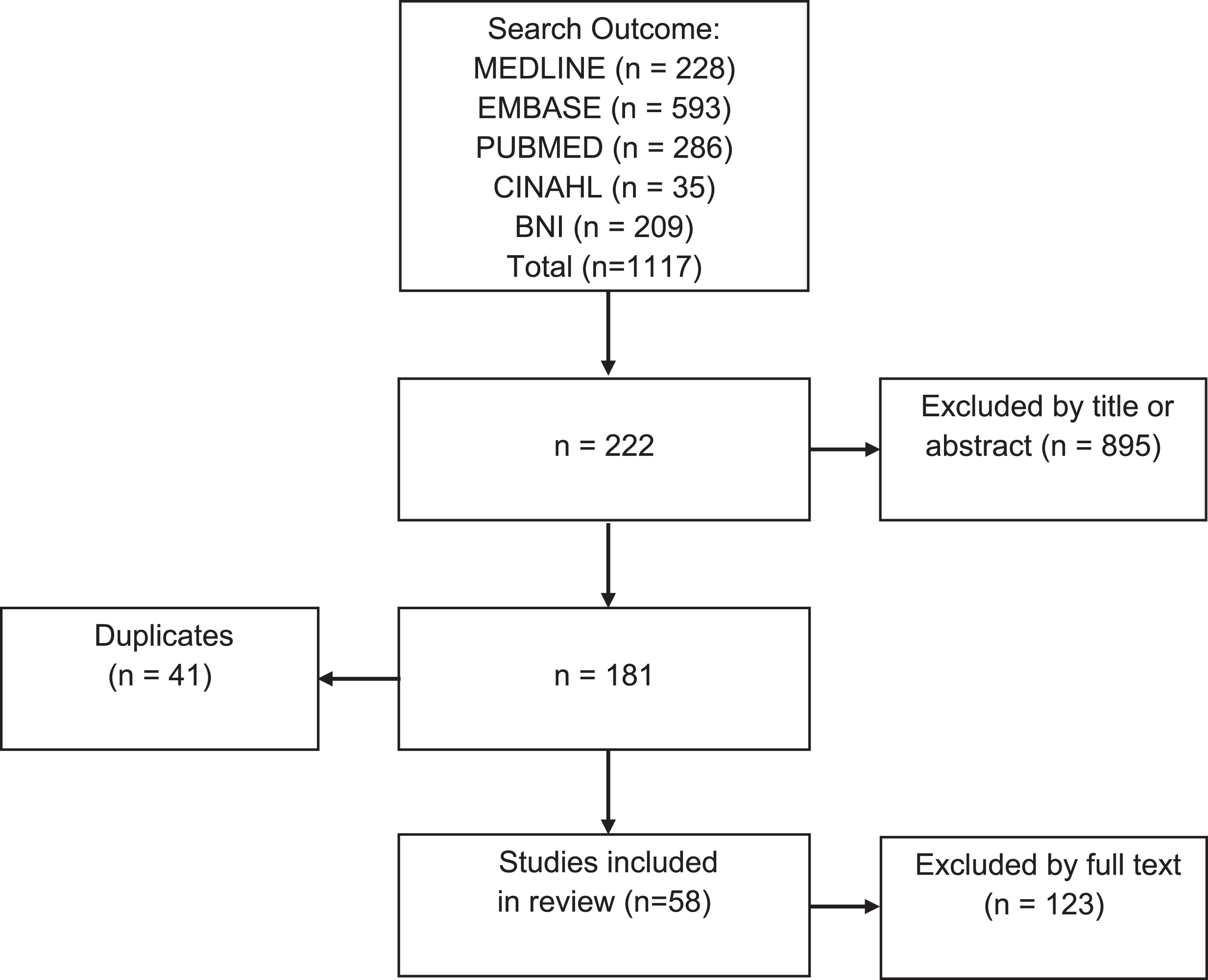
Search strategy.
Extracted data
The various causes of an opaque hemithorax were collated from all fifty eight included studies and divided into 16 categories (Table 2): Pleural effusion, empyema, haemothorax, chylothorax, consolidation, mucus plugging, foreign body occlusion, endobronchial mass, extrabronchial mass, diaphragmatic compromise, cyst, main bronchus intubation, pneumonectomy, agenesis, tuberculosis and bronchial stenosis.
Potential causes of an opaque hemithorax
Most common causes of an opaque hemithorax according to the four included observational studies were pleural effusion (with or without underlying malignancy/mass), empyema, tuberculosis, consolidation/atelectasis, extrabronchial mass and endobronchial mass (Table 2).
The four observational studies [2–5] also reported on the position of the mediastinum (and trachea) on CXR to differentially diagnose the cause of an opaque hemithorax based on the volume of the affected hemithorax (Table 1). There are typically three variations reported: Increased hemithorax volume causing a shift of the mediastinum towards the unaffected side (contralateral). i.e. typically, pleural effusions or thoracic mass. Reduced hemithorax volume causing a shift of the mediastinum towards to affected side (ipsilateral). i.e. typically, agenesis, pneumonectomy or atelectasis. Unchanged hemithorax volume with no mediastinal shift (central). i.e. typically, consolidation.
Of the 249 subjects in the four observational studies, 199 had a pleural effusion (with or without another pathology) contributing to the opaque hemithorax. Traditionally a moderate pleural effusion does not cause a mediastinal shift (trachea remains central) or if of sufficient size, a contralateral shift. As can be seen in (Table 3) this method of differential diagnosis has a questionable degree of accuracy. When the data from the 4 observational studies were combined for the subjects with a pleural effusion, 46% had a contralateral shift and 35% had no shift (central) as expected. However, the remaining 19% (38/199) had an ipsilateral shift which contradicts the previously described expected presentation.
Mediastinum (shift) position in patients with pleural effusion
When the same data is split into pleural effusion alone and pleural effusion with an associated malignancy/mass, the percentages begin to diverge further (Table 4). With a pleural effusion alone, the combined ipsilateral presentation of 19% reduces to 9%, whereas when a pleural effusion with an associated malignancy/mass the ipsilateral presentation increases to 30%.
Difference between the mediastinum (trachea) position in patients with pleural effusions vs. pleural effusions with mass
The underlying diagnosis/etiology and mediastinal position, when reported, for the individual case reports can also be found in (Table 1).
Wu et al. (1989) report that they found no correlation between the CXR volume pattern (mediastinal shift) and the underlying pathological cause. Yu et al. (1993), a follow up study to Wu et al. (1989) by the same team, also states that observing volume changes is not a satisfactory method of CXR diagnostic capabilities in opaque hemithorax. In their findings, when a pleural effusion is associated with a malignancy/mass the volume, and resulting mediastinal shift, can increase, decrease or remain unchanged.
Eight studies included the use of TUS to differentiate the cause of an opaque hemithorax and included four case reports [6, 32], one case series [59] along with three observational studies [2, 4–5] (Table 1). Studies using TUS to differentiate an opaque hemithorax ranged in date from as early as 1985 [59] to 2018 [6]. The three observational studies included one paper where CXR is compared directly to TUS in 65 patients [5]. The other two compare CXR and TUS against the “gold standard” of computed tomography (CT) in a combined total of 80 patients [2, 4]. Only Yu et al. (1993) reported any results regarding the sensitivity or specificity of TUS when compared against the reference standard of CT.
Only two studies reported the involvement of physiotherapy, once for sputum plug removal [53] and once when the physiotherapist identified the cause of the opaque hemithorax themselves using TUS [25].
A wide range of pathologies may present as an opaque hemithorax on CXR making differential diagnosis difficult. Within this review those pathologies have been divided into sixteen different categories (Table 2). Surprisingly, fifty four of the fifty-eight (93%) published works on opaque hemithorax are single patient case reports or case series. This introduces publication bias as only unusual or rare case presentations would be published, thus skewing the reported population away from the most common presentations. The four observational studies [2–5] perhaps report on more typical populations due to larger sample sizes and therefore offer slightly better heterogeneity. As mentioned previously, two of the observational studies were published over 25 years ago by the same team in Taiwan [4, 5], while the two more recent studies take data from an Indian (Indian subcontinent) population [2, 3]. So, with most publications in this review being subject to publication bias and the larger observational studies taking subjects from only two countries, the application of these findings to other subject populations should be done with caution.
According to Wu et al. (1989), the reason for an absent correlation between the mediastinal position on CXR and the underlying cause is because an opaque hemithorax often results from a combination of pathologies. The same team’s subsequent publication, Yu et al. (1993), explains that it is not satisfactory enough to just observe changes in lung volume and its effect on neighbouring soft tissue structures to diagnose the cause of an opaque hemithorax. The CXR converts a 3-dementional structure into a 2-dimentional image which allows pathologies from a pleural, parenchymal, mediastinal or diaphragmatic origin to not only look similar on CXR but also underestimate the degree to which they may interact and impact on each other. The results presented in Tables 3 and 4 show that within this collection of papers the premise that a contralateral shift implies pleural effusion and an ipsilateral shift implies collapse is incorrect. Even when a single pathological process is involved, i.e. pleural effusion only, the expected contralateral shift is only seen 50% of the time and no shift 41% of the time (Table 4). Nine percent of the time a pleural effusion large enough to cause an opaque hemithorax results in an ipsilateral shift making this method of differential diagnosis incorrect in nearly 1 in 10 patients. The inaccuracy of using mediastinal shift on CXR only worsens when a second pathology is introduced into the clinical picture. When a pleural effusion is associated with a malignancy or tumour mass a contralateral shift is seen less often, only 42% of cases. Interestingly the remaining cases are almost evenly split between central (28%) and an ipsilateral shift (30%). This makes the position of the mediastinum even more unreliable as a method of differentially diagnosing an opaque hemithorax. This difference is made worse by the fact that CXR cannot easily distinguish between a pleural effusion on its own and one associated with a malignancy or tumour mass.
Within the individual case reports, when mediastinal position is reported, this unreliable pattern continues. It would appear too simplistic that a pleural effusion large enough to cause an opaque hemithorax always results in a contralateral shift and an ipsilateral shift rules out a pleural effusion.
It seems reasonable to explore ways of differentially diagnosing the underlying cause of an opaque hemithorax when CXR is unclear. In the eight papers that use TUS, all of them advocate the use of TUS as a useful, non-invasive tool to examine the cause of an opaque hemithorax prior to any potential request for CT. Wu et al. (1989) and Yu et al. (1993) both advocate the use of TUS as most causes of an opaque hemithorax produce an “acoustic window” allowing improved sonographic images. This can either be due to a loss of aeration of the lung parenchyma (consolidation/atelectasis), pleural pathology (pleural effusion) or various thoracic tumours. It is suggested that if an obvious pathology causing the opaque hemithorax is in doubt or complex pathology is suspected following CXR, then TUS should be considered. Esmadi et al. (2013) also support the use of TUS as it helps identify the nature of the lung pathology. Taking this concept further, Bedi et al. (1985) state that when TUS is used as the first method of imaging, it is usually not necessary to perform other examinations. It must be stated, that however useful TUS may prove, if there is any doubt regarding the cause of an opaque hemithorax then more advanced imaging, such as CT, should be requested.
According to this selection of studies physiotherapists appear to have a limited role in the management of opaque hemithorax. Only two studies report on the involvement of physiotherapy in the management of opaque hemithoracies. Barker et al. (2003) report on the use of physiotherapy to assist in the removal of endobronchial blood clots that had resulted in an opaque hemithorax with an ipsilateral shift. The second study by Leech et al. (2015) report on an opaque hemithorax, initially thought to be due to sputum retention, but then later confirmed as a pleural effusion identified through physiotherapy-performed TUS. These two studies hint at a more effective use of physiotherapy resources through the correct diagnosis of the opaque hemithorax using TUS. The TUS could be performed by a member of the medical team or alternatively the physiotherapist could perform it themselves one adequately trained. This could aid in the differential diagnosis of an opaque hemithorax and either more accurately identify patients amenable to physiotherapy treatment techniques or avoid unnecessary and ineffective physiotherapy interventions.
Conclusion
Numerous pathologies of the pleural, parenchymal, diaphragmatic and mediastinal origin can cause an opaque hemithorax on CXR making differential diagnosis difficult. Even when mediastinal shift is present it does not appear to be a reliable way to identify the underlying cause. Thoracic ultrasound has the potential to much more accurately differentiate between pathologies. This would assist physiotherapists to identify patients amenable to physiotherapy treatment techniques.
Author contributions
SH developed and performed the search. SH and LH both shortlisted and performed the data extraction. SH wrote the manuscript, LH provided feedback on manuscript structure and content.
Conflict of interest
None to report.
Footnotes
Acknowledgments
Thanks go to the Physiotherapy department, Critical Care teams and the Library services at Blackpool Teaching Hospitals NHS Foundation Trust.