
Abstract
BACKGROUND:
Patients with posterior- and lateral-(canal)-benign paroxysmal positional vertigo (BPPV)-canalolithiasis sleep in the affected-ear-down head position. Posterior-BPPV-canalolithiasis typically affects the right than left ear; sleeping in the right-ear-down head position may be causal.
OBJECTIVE:
To investigate the relationship between habitual head position during sleep and the onset of BPPV variants.
METHODS:
Among 1,170 cases of BPPV variants with unknown etiology, the affected ears, habitual head positions during sleep based on interviews, and relationships among them were investigated.
RESULTS:
Posterior-BPPV-canalolithiasis and lateral-BPPV-canalolithiasis-geotropic affected the right ear significantly more often. Significantly more patients with posterior-BPPV-canalolithiasis and lateral-BPPV-canalolithiasis-apogeotropic habitually slept in the right-ear-down head position. Patients with posterior- and lateral-BPPV-canalolithiasis and light cupula were more likely to sleep habitually in the affected-ear-down position than in the healthy-ear-down head position; no relationship was observed in patients with posterior- and lateral-BPPV-cupulolithiasis. In patients with posterior-BPPV-canalolithiasis and lateral-BPPV-canalolithiasis-geotropic, the proportion of right-affected ears in those sleeping habitually in the right-ear-down head position was significantly greater than that for the left-affected ear.
CONCLUSIONS:
A habitual affected-ear-down head position during sleep may contribute to BPPV-canalolithiasis and light cupula onset, but not BPPV-cupulolithiasis onset. However, habitual sleeping in the right-ear-down head position cannot explain the predominance of right-affected ears.
Keywords
Introduction
Benign paroxysmal positional vertigo (BPPV) is the most common of vertigo disease. BPPV is thought to occur in three phases. In the initial phase, otoconia become detached from the utricular macula by various inner ear disorders, head injuries, aging, or unknown pathology [2, 20]. During the second phase the detached otoconia fall into the posterior, lateral, or anterior semicircular canal, although the cause is not yet well understood [28]. In the third phase, the detached otoconia either move freely in the endolymph (canalolithiasis [13]) or attach to the cupula (cupulolithiasis [31]).
It’s known that BPPV often occurs in the morning when the individual is getting out of bed [7]. This clinical condition suggests that head position during sleep may be related to the onset of BPPV. In posterior semicircular canal-BPPV-canalolithiasis and lateral semicircular canal-BPPV-canalolithiasis, the affected ear is associated with the habitual head position during sleep [8, 30]. Further, it is more often the right ear for posterior semicircular canal-BPPV-canalolithiasis [35].
Currently, BPPV can be categorized into variants associated with the three semicircular canals (posterior [P], lateral [L], and anterior [A]) and two pathophysiologies (canalolithiasis [Can] and cupulolithiasis [Cup]). Among these, a consensus has been reached and diagnostic criteria have been published for P-BPPV-Can, L-BPPV-Can, and L-BPPV-Cup [18, 34]. However, for L-BPPV-Can, the observed nystagmus is considered to differ depending on whether the otoconia that are detached from the utricular macula move freely within the endolymph of the lateral semicircular canal, or attach to the cupula of the canal side [24, 32]. The former will exhibit paroxysmal geotropic positioning nystagmus (L-BPPV-Can-g), and the latter will exhibit persistent apogeotropic positional nystagmus (L-BPPV-Can-a) in both the right-ear-down and left-ear-down head positions. When persistent apogeotropic positional nystagmus does not change to paroxysmal geotropic positioning nystagmus, it is predicted to be L-BPPV-Cup, in which the otoconia adhere to the cupula of the lateral semicircular canal. However, it is not apparent whether otoconia that are detached from the utricular macula adhere to the utricular or canal side of the cupula.
Among the other variants, P-BPPV-Cup is not yet consistently recognized [34]. A-BPPV is reported as a rare form of BPPV that manifests as positional down-beating nystagmus [5, 14]. However, in recent years, P-BPPV cases presenting with positional down-beating nystagmus have also been reported; thus, decisions regarding the diagnosis and affected ear are ambiguous [9, 33]. Additionally, cases of so-called “Light cupula (LiC)”, which exhibit persistent geotropic positional nystagmus, have been reported [4, 29]. The pathophysiology of LiC is unknown, and uncertainty remains about whether it is a variant of BPPV, or not. However, the findings of positional nystagmus in LiC contrast completely with those in Heavy cupula (L-BPPV-Cup). As for a pathophysiology of LiC, L-BPPV due to light debris attachment has been presumed [17]. We therefore included cases of LiC in this study.
All the cases of BPPV were classified into six variants (P-BPPV-Can, P-BPPV-Cup, L-BPPV-Can-g, L-BPPV-Can-a, L-BPPV-Cup, and LiC), and we investigated the relationship between habitual head position during sleep and the BPPV variants.
Subjects and methods
Patients and classification of BPPV
This study included 1,170 cases of BPPV with unknown etiology (Fig. 1). We investigated 1,256 cases of BPPV, which were initially examined at the first author’s clinic between June 2003 and May 2017. Among these, we excluded 86 cases with various comorbid conditions. Individuals were excluded if they had secondary BPPV due to apparent disorders of the inner ear (e.g. Ménière’s disease, delayed endolymphatic hydrops, acute low-tone sensori-neural hearing loss, vestibular neuronitis, sudden deafness with vertigo, Hunt’s syndrome, or enlarged vestibular aqueduct). Additionally, individuals with suspected inner ear disorders (head injuries, intramuscular injection of streptomycin, postoperative resting, or dialysis) were excluded. Lastly, we excluded individuals with past or present central nervous system disorders.
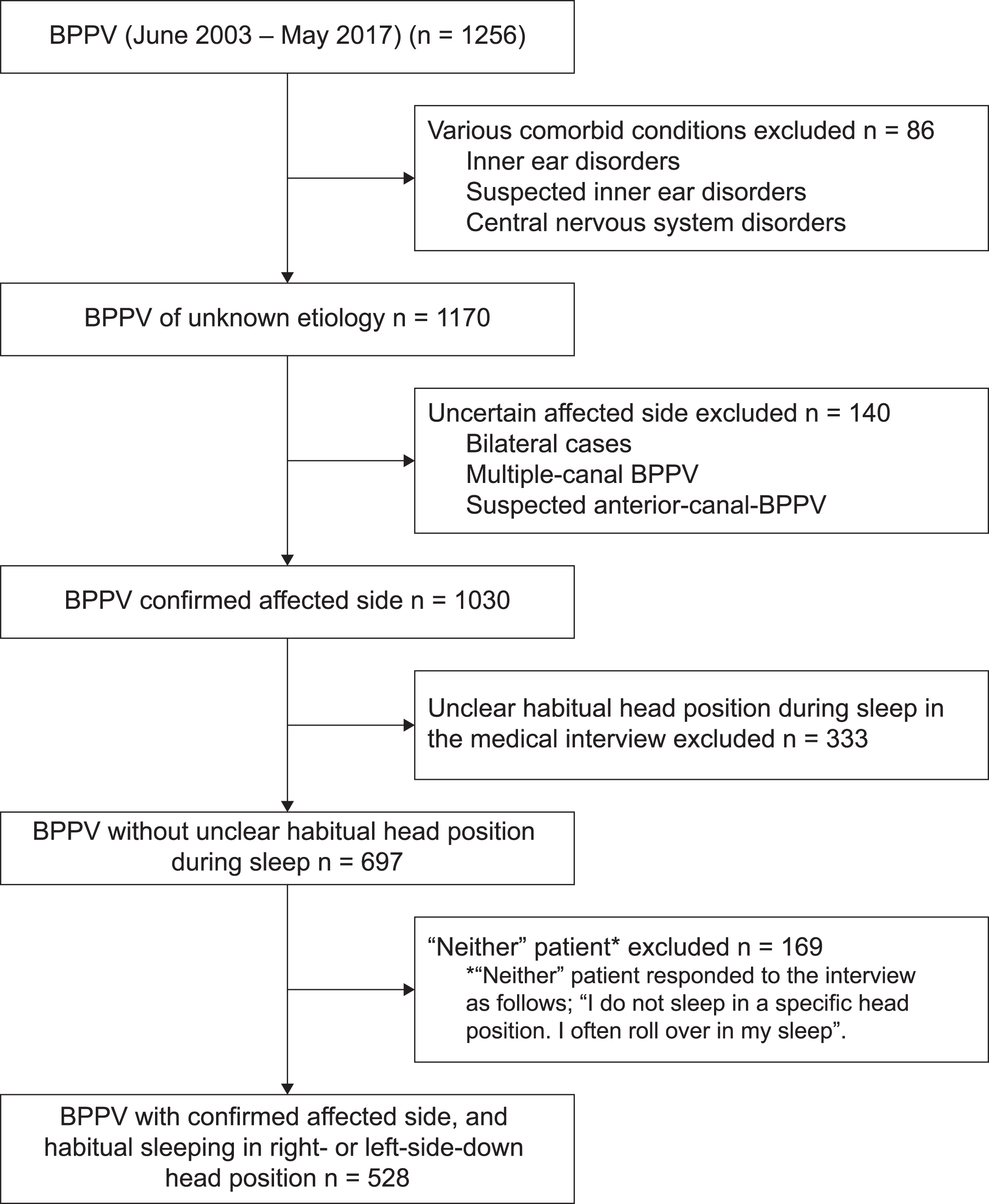
Flowchart of patient selection.
Patients who were initially examined due to a chief complaint of positional vertigo were administered a positional nystagmus test or a positioning nystagmus test. For the positional nystagmus test, static nystagmus was observed in the following positions: sitting (upright), face-up supine, supine right-ear-down and supine left-ear-down (right- or left-ear-down about 60° tilting head position from face-up supine position, respectively), and prone. A direction-changing nystagmus was induced both in a right-ear-down head position and a left-ear-down head position, and both in a supine position and a prone position. Further nystagmus lasting for more than a minute without any decrease in intensity (persistent), led to the diagnosis of cupulolithiasis. For the positioning nystagmus test, a direction-changing nystagmus was provoked either by the Dix-Hallpike maneuver or by the supine head roll test in which the patient’s head is rapidly moved from the supine right-ear-down position to the supine left-ear-down position and vice versa. Nystagmus that lasted for less than a minute and was characterized by an increase followed by a decrease in intensity (paroxysmal), led to the diagnosis of canalolithiasis. Positional and positioning nystagmus were observed and recorded using spectacles equipped with an infrared charge-coupled device (CCD) camera (SNIR-1, Nagashima Medical Instruments co., Ltd.) and the presence or absence, duration, and direction of nystagmus were confirmed.
Diagnoses of P-BPPV-Can, L-BPPV-Can-g and L-BPPV-Cup, and identification of the affected ear were based on classification and diagnostic criteria from the Bárány Society and the Japan Society for Equilibrium Research [18, 34]. Diagnoses of P-BPPV-Cup, L-BPPV-Can-a and LiC, and identification of the affected ear were determined according to the following criteria.
In P-BPPV-Cup, nystagmus is upward vertical-torsional nystagmus in the face-up supine position and in the supine right- or left-ear-down position, and direction-changing in the supine right- and left-ear-down positions and/or in the face-up supine and prone positions (in the Dix-Hallpike position, either no nystagmus or weaker nystagmus is observed). Duration of the nystagmus is persistent. The upward vertical and the upper pole of the eye rotates toward the affected ear in the face-up supine, and in the supine right- or left-ear-down position. In L-BPPV-Can-a, nystagmus is direction-changing apogeotropic nystagmus in the supine left- and right-ear-down positions, and in the face-up supine and prone positions. Duration of the nystagmus is persistent. If apogeotropic nystagmus transitions into paroxysmal geotropic positioning nystagmus on repeating the supine head roll test or on 360° barbecue rotation toward the healthy side [11], L-BPPV-Can-a may be diagnosed instead of L-BPPV-Cup. The presumed affected ear of L-BPPV-Can-a is the lower ear for which a neutral position exists, or the lower ear for which the nystagmus and vertigo are milder (neutral position is the head position in which the direction of nystagmus is reversed, where the axis of cupula of the affected semicircular canal is presumed to be aligned with gravity [6, 28]. When the head position changes from the sitting to the supine position, horizontal nystagmus directed to the affected ear can be observed in most cases [1], although the observed nystagmus may be weak in some cases). In LiC, nystagmus is direction-changing geotropic nystagmus in the supine right- and left-ear-down positions, and in the face-up supine and prone positions [4, 29]. The presumed affected ear is the lower ear for which a neutral position exists (neutral position is the head position in which the direction of nystagmus is reversed [21, 29]. When the head position changes from the sitting to the face-up supine position, horizontal nystagmus directed to the healthy ear can be observed in most cases [16, 29], although the observed nystagmus may be weak in some cases).
Habitual head position during sleep before the onset of BPPV was assessed in a medical interview at initial examination. All patients responded to the questions “do you habitually sleep in a right- or left-ear-down head position?” and “have you recently had pain in your shoulder or back causing you to habitually sleep in a specific head position?”. Answers were classified into four categories: “I habitually sleep in a right-ear-down head position (Right),” “I habitually sleep in a left-ear-down head position (Left),” “I do not sleep in a specific head position. I often roll over in my sleep (neither),” and “I do not know (unclear).”
This clinical study was approved by the Ethical Review Board of the Nagasaki City Medical Association (No. 2017-4-1). We omitted informed consent, however the study information was posted in the first author’s clinic, and all patients were given an opt-out choice.
We investigated the habitual head position during sleep before onset in all 1,170 cases of BPPV with unknown etiology (Fig. 1). Excluding 140 cases in which the affected ear was uncertain, bilaterally affected cases, and multiple-canal BPPV cases from this total, for the remaining 1,030 cases we compared the affected ear among the different BPPV variants. It was difficult to differentiate the 19 cases of suspected A-BPPV exhibiting positional down-beating nystagmus from P-BPPV on the opposite ear; we thus included these cases with the cases in which the affected ear was uncertain [5, 34]. We investigated whether there was bias in the affected ear by BPPV variant, assuming an expected value denoting no left-right difference in the affected ear (0.5; binomial test).
Excluding 333 cases for which the habitual head position during sleep was unclear in the medical interview from these 1,030 cases, the remaining 697 cases were classified according to BPPV variant, sex, age [SD], and habitual head position during sleep (right-ear-down, left-ear-down, neither). We investigated differences in habitual head position during sleep (right-ear-down, left-ear-down, neither), age, and sex between each BPPV variant and the entire sample of 1,170 cases of BPPV with unknown etiology (chi-square test). We also investigated possible bias between patients who habitually slept in a right- and left-ear-down head position, assuming that an expected value of 0.5 denoted no right-left difference in the habitual head position during sleep (binomial test).
Among the 697 cases assessed, 169 cases were excluded for which the habitual head position during sleep was reported as “I do not sleep in a specific head position. I often roll over in my sleep (neither)” during the medical interviews. For each BPPV variant among the final number of 528 cases assessed, we investigated the agreement between the habitual head position during sleep and the affected ear. Cohen’s kappa coefficient was used to determine this agreement, taking into account the possibility of the agreement occurring by chance.
For each BPPV variant among the 528 cases, we compared the proportions of the number of affected-right-ear to those of habitual sleeping in right-ear-down head position, and the same for the affected-left-ear, to assess possible differences between the both ears (chi-square test and Fisher’s exact test).
The binomial test, Cohen’s kappa coefficient, chi-square test (with Yates’ correction for continuity), and Fisher’s exact test were used for hypothesis testing with a significance standard of p < 0.05. The statistical software used was Statmate IV (ATMS Co. Ltd.).
Results
Regarding the habitual head position during sleep for the 1,170 cases of BPPV with unknown etiology, 363 patients (31%) responded that they sleep with their right-ear-down, 242 patients (21%) that they sleep with their left-ear-down, 194 patients (16%) that they do not sleep with their left- or right-ear-down or that they often roll over in their sleep, and 371 patients (32%) that they were unaware of which head position they slept in.
Table 1 presents the 1,030 cases, excluding those in which the affected ear was uncertain, bilaterally affected cases and multiple-canal BPPV cases, categorized by BPPV variant and the affected ear. P-BPPV-Can and L-BPPV-Can-g occurred significantly more often in the right ear than in the left (p < 0.001, binomial test), but P-BPPV-Cup, L-BPPV-Can-a, L-BPPV-Cup, and LiC occurred with equal prevalence in both ears.
Affected ear grouped by BPPV variant (n = 1030)
Affected ear grouped by BPPV variant (n = 1030)
P: posterior canal; L: lateral canal; BPPV: benign paroxysmal positional vertigo; Can: canalolithiais; Cup: cupulolithiasis; g: geotropic; a: apogeotropic; Lic: light cupula.
Table 2 presents the characteristics (number of cases, sex, age [SD], and various head positions during sleep) by each BPPV variant for the 697 cases, excluding cases in which the affected ear was uncertain, bilaterally affected cases, multiple-canal BPPV cases, and cases in which the habitual head position during sleep was unclear. There were no significant differences in sex ratio or mean age between each BPPV variant and the entire sample of 1,170 cases of BPPV (chi-square test). Excluding LiC (p < 0.05, Chi-square test), there were no significant differences in the ratios of the various head positions during sleep (right, left, neither) reported during the medical interview between each BPPV variant, and the entire sample of all cases of BPPV with unknown etiology. For P-BPPV-Can and L-BPPV-Can-a, significantly more patients habitually slept in a right-ear-down head position than a left-ear-down head position (p < 0.001, p < 0.01 respectively; binomial test), but no such differences were observed in patients with P-BPPV-Cup, L-BPPV-Can-g, L-BPPV-Cup, or LiC.
Clinical characteristics and habitual head position during sleep by BPPV variant (n = 697)
All BPPV: all cases of BPPV with unknown etiology, neither: I do not sleep in a specific head position. I often roll over in my sleep
Table 3 presents the agreement between habitual head position during sleep and affected ear for the 528 cases, separately for each BPPV variant with kappa coefficients and 95%confidence intervals. The levels of agreement above chance between habitual head position during sleep and affected ear were relatively high in P-BPPV-Can, L-BPPV-Can-g, L-BPPV-Can-a, and LiC (Kappa coefficients: 0.35, 0.44, 0.58, and 0.47, respectively). No agreement was observed in P-BPPV-Cup and L-BPPV-Cup.
Concordance between habitual head position during sleep and affected ear (n = 528)
Figure 2 presents the proportions of the number of affected-right (left) -ear to those of habitual sleeping in right (left) -ear-down head position, for each BPPV variant. In patients with posterior-BPPV-canaloli-thiasis and lateral-BPPV-canalolithiasis-geotropic, the proportion of right-affected ears in those who habitually slept in the right-ear-down head position was significantly greater than that of left-affected ears (P-BPPV-Can: p < 0.001, L-BPPV-Can-g: p < 0.05, chi-square test and Fisher’s exact test). No significant differences were found in patients with BPPV-Cup, L-BPPV-Can-a, or LiC.
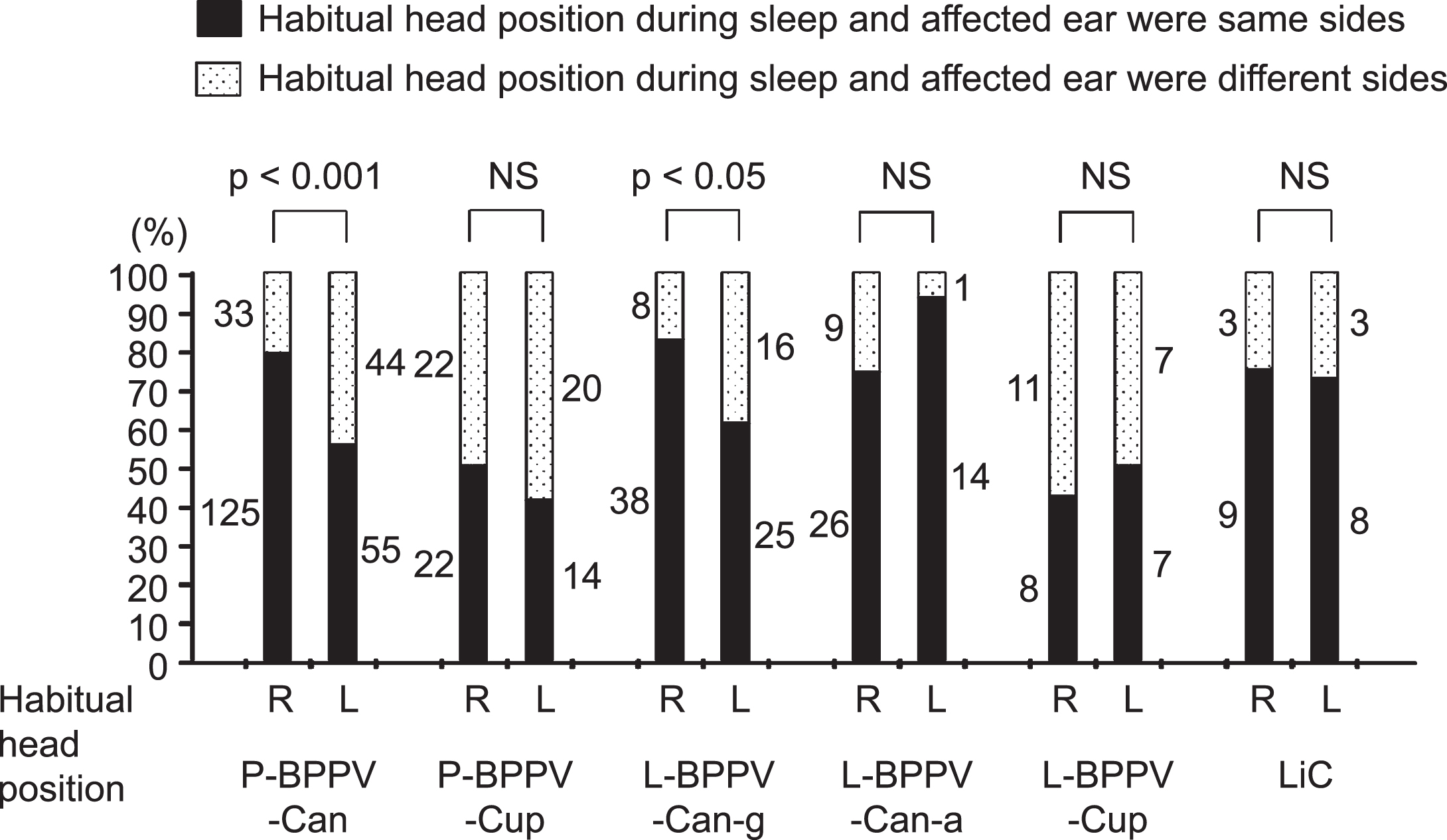
Proportions of the number of affected-right (left) -ear to those of habitual sleeping in the right (left) -ear-down head position, for different BPPV variants.
Habitually sleeping in the affected-ear-down head position may be involved in the onset of BPPV-Can and Light cupula. However, there is no evidence for involvement of the habitual head position during sleep in the onset of BPPV-Cup.
It has been reported that patients with P-BPPV-Can who habitually slept in a right-ear-down head position before onset were likely to be affected on the right side, while patients who habitually slept in a left-ear-down head position were likely to be affected on the left side [8, 23]. Meanwhile, it has been reported that patients with L-BPPV-Can-g also likely slept in an affected-ear-down head position [15, 30]. We previously [28] measured the actual head position during sleep in cases of P-BPPV-Can and L-BPPV-Can-g after confirmation of the disappearance of positional vertigo and nystagmus, and found that recurrent cases of BPPV spent significantly longer sleeping in the affected-ear-down 45° (37.5–52.5°) head position (hereafter referred to as the “affected-ear-down 45° head position”) than did first-time BPPV cases. Significant differences were not found for the other head positions. We hypothesized that, when the head is in the affected-ear-down 45° head position, the non-ampullated half of the posterior and lateral semicircular canal are nearly in the earth-vertical position, making it easier for the detached otoconia to fall into the posterior or lateral semicircular canal, agglomerate, and attain a certain size in the lowest portion of each semicircular canal. The head position during sleep, particularly the affected-ear-down 45° head position, could be an etiologic factor of BPPV-Can.
In this investigation, as with past reports, patients with P-BPPV-Can, L-BPPV-Can-g, and L-BPPV-Can-a were more likely to sleep in the affected-ear-down head position before the onset of BPPV. Therefore, the habitual head position during sleep, probably the affected-ear-down 45° head position, could be an etiologic factor contributing to the onset of such BPPV-Can.
Brevern et al. [35] reported that 1.4-fold more patients with P-BPPV-Can had a right than left-affected-ear, and speculated that sleeping in a right-ear-down head position was a cause. In the present investigation, patients with P-BPPV-Can had 1.8-fold more cases of right than left-affected-ear, and exhibited more cases of habitual sleeping in right- than left-ear-down head position. In contrast, patients with L-BPPV-Can-g also had 1.8-fold more cases of right- than left-affected-ear, but indicated no right-left difference for habitual head position during sleep. This suggests that habitual sleeping in the right-ear-down head position alone is not the cause of the predominance of right affected ears among patients with BPPV-Can. The proportion of right-affected ears in those who habitually slept in the right-ear-down head position was significantly greater than that of left-affected ears in P-BPPV-Can, which was the same for L-BPPV Can-g. It appears that patients who habitually sleep in the right-ear-down head position were more subject to BPPV-Can than were those with habitual sleeping in left-ear-down head position. It is unlikely that this intriguing difference is due to a morphological difference between the right and left inner ears. With regard to why right affected ears are more prevalent in patients with P-BPPV-Can and L-BPPV-Can-g, one possible reason is that more patients may sleep in a right-ear-down 45° head position than in a left-ear-down 45° head position.
De Koninck et al. [10] observed the development of sleep position in five healthy age groups, and showed that the right-side positions for both the head and the trunk were particularly prevalent in elderly individuals 65 years of age or older, who were right-handed. Although the mechanism underlying this relationship remains unknown, some reports have speculated that cardiovascular conditions might be involved [10, 35]. However, cardiovascular conditions or right handedness does not necessarily explain why patients with P-BPPV-Cup, L-BPPV-Can-g, L-BPPV-Cup and LiC showed no right-left preference for habitual head position during sleep, although patients with P-BPPV-Can and L-BPPV-Can-a slept more frequently in a right-ear-down head position. In this study, the reasons for habitual sleeping in right- or left-ear down head position answered by interviews were as follows: unknown (easy to sleep somehow, approximately 70%), physical factors (inter alia, pain in the shoulder or back, or after certain types of surgery including gastrectomy and others, approximately 30%) and environmental factors (sleep positions of the family, bed position within the room, and others). A wide variety of factors seems to contribute to the tendency of many patients with BPPV-Can to sleep habitually in the right-ear-down head position or in the right-ear-down 45° head position.
In L-BPPV-Can-a, a proposed pathophysiology is considered that free otoconia initially enter from the non-ampullated end of the lateral semicircular canal, migrate, and then attach to the lateral semicircular canal cupula on the canal side. Accordingly, the lateral semicircular canal cupula on which the otoconia attached becomes a heavy cupula, and persistent apogeotropic positional nystagmus appears. L-BPPV-Can-a and L-BPPV-Can-g are believed to differ only in the position of the otoconia within the long-arm of the lateral semicircular canal, therefore, both are classified as BPPV-Can [24, 34]. In the present investigation, both patients with L-BPPV-Can-a and L-BPPV-Can-g were more likely to sleep with the affected-ear-down head position (Kappa coefficient: 0.58 and 0.47, respectively), but these two variants showed some characteristic differences. Although the right-affected ears were prevalent in patients with L-BPPV-Can-g, there was no difference in the number of right- and left-affected ears in patients with L-BPPV-Can-a. It is difficult to explain these attributes of L-BPPV-Can-a completely, but we suggest the following pathophysiology. Many patients with L-BPPV-Can-a probably spent a certain time sleeping in the affected-ear-down 45° head position. If there is no habitual right-left bias toward sleeping in the affected-ear-down 45° head position and then turning over to the affected-ear-down lateral position, there would be no difference in the number of patients with an affected right ear vs. an affected left ear. In addition, there would be no difference between the proportion of right-affected ears in those who habitually slept in the right-ear-down head position and that of left-affected ears. Thus, when sleeping in the affected-ear-down 45° head position, otoconia probably enter from the non-ampullated end of the affected lateral semicircular canal and develop freely within the endolymph of the lateral semicircular canal. Subsequently, when changing head position from a face-up supine position to an affected-ear-down lateral position the free otoconia would migrate toward the ampulla due to the inertia, and should attach to the canal side of the cupula.
For BPPV-Cup, it is unclear whether otoconia that have detached from the utricular macula adhere to the utricular or canal side of the cupula. If we assume that otoconia in patients with P-BPPV-Cup and L-BPPV-Cup are adhered to the canal side of the respective cupula, then it should be a necessary condition that first, by sleeping in the affected-ear-down head position, otoconia enter the endolymph of the semicircular canal from the non-ampullated end of the semicircular canal, in the same manner as P-BPPV-Can, L-BPPV-Can-g, and L-BPPV-Can-a. However, for both patients with P-BPPV-Cup and L-BPPV-Cup, in contrast to patients with BPPV-Can, no statistically significant relationship was found between the affected ear and head position during sleep. In P-BPPV-Cup and L-BPPV-Cup cases, this indicates that otoconia detached from the utricular macula probably enter from the ampullated end of the affected semicircular canal [3, 25] and adhere to the utricular side of the cupula rather than the canal side.
In this investigation, the rates of head positions during sleep (right, left, neither) in patients with LiC differed from all patients with BPPV. Significantly more subjects with this variant reported that they sleep in the affected-ear-down head position than in the healthy-ear-down position. Our results suggest the pathophysiology of LiC differs from that of the other variants and remains unknown, but it should be noted that patients with LiC habitually slept in the presumed affected-ear-down head position. Further studies of this condition are needed, with a larger patient cohort.
In the present investigation, approximately one third of patients with BPPV reported that they were unaware of which head position they slept in; thus, the habitual head position during sleep could not be indicated. It was also assumed that the reported head position during sleep did not necessarily coincide with the actual head position during sleep. Gordon et al. [12] reported that the actual head position during sleep for healthy individuals who reported that they habitually sleep in a lateral position had a concordance rate of 89%, but that most of those who reported that they sleep in a supine position actually slept in a lateral position. Russo et al. [26] classified the answers to the question “How often do you sleep in a supine position?” from medical interviews with sleep apnea patients into five categories (always, usually, half the time, sometimes, never) and found that the actual time sleeping in a supine position generally matched the reported time, but there was a considerable range of response accuracy. These studies indicate that the reported habitual head position during sleep does not necessarily indicate the actual head position during sleep for individual cases. Nonetheless, because in the present investigation habitual head position during sleep (right-ear-down or left-ear-down) before onset in patients with BPPV-Can more likely coincided with the BPPV-affected ear, this is considered to show a relationship between BPPV onset and head position during sleep. To understand this relationship in more detail, it would be beneficial to record the actual head position during sleep in cases of BPPV with a frequent recurrence before and after onset.
Despite the importance of the association between BPPV and the head position during sleep, there have been few relevant reports. It is difficult to reliably measure the head position during sleep using current technology. However, we are developing a gyro-based measuring instrument for the future, and this paper is a report of a pilot study.
Conclusion
Patients with P-BPPV-Can, L-BPPV-Can-g, and L-BPPV-Can-a are more likely to sleep in the affected-ear-down head position before the onset of BPPV-Can. Therefore, the habitual head position during sleep may be an etiologic factor for the onset of BPPV-Can. However, habitual sleeping in the right-ear-down head position cannot explain the predominance of right-affected ears in P-BPPV-Can and L-BPPV Can-g. For both P-BPPV-Cup and L-BPPV-Cup, a relationship between the affected ear and head position during sleep is unlikely. Although the pathology of light cupula is unknown, patients with Light cupula habitually sleep in the presumed affected-ear-down head position.
Footnotes
Acknowledgments
We would like to thank Prof. Sumihisa Honda, Ph.D., statistician (Nagasaki University Graduate School of Biomedical Sciences, Nagasaki, Japan) for his help in performing the statistical analysis.