
Abstract
BACKGROUND:
Benign paroxysmal positional vertigo (BPPV) is the most common vestibular disorder affecting about 20% of dizzy patients. Early diagnosis and treatment can improve the quality of life for patients.
OBJECTIVE:
We reviewed the classifications of different subtypes of benign paroxysmal positional vertigo and the problems we encountered using the diagnostic criteria of the Bárány Society.
METHODS:
Both the Dix–Hallpike maneuver and supine roll test were performed on 568 patients, and diagnoses were made based on patient history and the type of provoked nystagmus (if any). Next, the numbers of patients with each subtype and other parameters, including age and sex, were analyzed.
RESULTS:
Posterior semicircular canal BPPV (pc-BPPV) accounted for the largest proportion, followed by horizontal semicircular canal BPPV (hc-BPPV). Both anterior canal BPPV and multiple canal lithiasis BPPV were rare, and no patient was diagnosed with cupulolithiasis of the posterior canal.
CONCLUSIONS:
pc-BPPV, hc-BPPV, and cupulolithiasis of the horizontal canal (hc-BPPV-cu) were the three major subtypes that could be definitively diagnosed, whereas the diagnoses of possible benign paroxysmal positional vertigo (pBPPV) and probable benign paroxysmal positional vertigo [spontaneously resolved] (pBPPVsr) require further investigation, with special attention being paid to appropriate differentiation and repositioning maneuvers.
Introduction
The development of diagnostic criteria for benign paroxysmal positional vertigo (BPPV) over the past 3 years constitutes a major advance in the field of vestibular disorders. Diagnostic criteria and/or clinical practice guidelines for BPPV have been developed or revised by many organizations in different countries [2, 21]. In 2015, the Bárány Society developed diagnostic criteria for BPPV, including the pathomechanisms of the condition; two disease categories (established and emerging BPPV) were recognized [21]. In 2017, guidelines for the diagnosis and treatment of BPPV were revised by both the American Academy of Otolaryngology–Head and Neck Surgery Foundation (AAO-HNSF) and the Chinese Association of Otolaryngology–Head and Neck Surgery [2, 4]. These efforts have improved the accuracy of BPPV diagnosis, will promote professional communication in different clinical settings, and benefit BPPV patients.
The diagnostic criteria for posterior semicircular canal (PC) and horizontal semicircular canal (HC) BPPV are similar in all three diagnostic criteria/clinical practice guidelines [2, 21]. A typical history, characteristic nystagmus (or not) upon positional testing, and exclusion of other vestibular disorders are essential for definitive diagnosis. Therefore, PC-BPPV or HC-BPPV diagnosed using any of the above mentioned criteria will represent the same disease entity even in different medical institutions; this standardizes diagnosis and promotes scientific communication among medical professionals and institutions.
The Bárány system includes diagnostic criteria for atypical positional vertigo syndromes. The diagnostic criteria for BPPV include canalolithiasis of the posterior canal (pc-BPPV), canalolithiasis of the horizontal canal (hc-BPPV), cupulolithiasis of the horizontal canal (hc-BPPV-cu), and probable benign paroxysmal positional vertigo [spontaneously resolved] (pBPPVsr). Emerging and controversial syndromes include canalolithiasis of the anterior canal (ac-BPPV), cupulolithiasis of the posterior canal (pc-BPPV-cu), lithiasis of multiple canals (mc-BPPV), and possible benign paroxysmal positional vertigo (pBPPV) [21]. The AAO-HNSF clinical guidelines include only diagnostic criteria for PC-and HC-BPPV [2]. In real clinical practice, quite a few patients do not meet all criteria for PC- or HC-BPPV. Therefore, the Bárány Society system includes specific criteria for variants of BPPV in addition to definitive BPPV.
Although the Bárány criteria have been carefully formulated, their utility in clinical practice has not been adequately evaluated, and the distributions of various subtypes and their clinical features require further investigation. Therefore, we applied the Bárány criteria in our clinical practice for 1 year, to rationalize BPPV diagnosis, to understand the distribution of each disease subtype, and to identify possible problems encountered using the criteria. Here, we report our findings.
Materials and methods
From August 2016 to July 2017, the diagnostic criteria for BPPV proposed by the Bárány Society were used to evaluate patients with histories of positional vertigo who visited our clinic at the Department of Otolaryngology in the Affiliated Sixth People’s Hospital of Shanghai Jiao Tong University. Both the Dix-Hallpike maneuver and the supine roll test were performed on each patient, and the subtypes were classified based on patient history and the nystagmus provoked (if any). The nystagmus was seen by naked eyes. Overall, 568 patients enrolled our study. According to the Bárány criteria, established BPPV and emerging and controversial syndromes form two major categories, each with four subtypes. Thus, in total, eight subtypes of BPPV are distinguished; the diagnostic criteria that we used were strictly in accordance with those of the Bárány Society.
After definitive diagnosis of BPPV, the Epley and barbecue maneuvers were performed to treat posterior and horizontal canal BPPV, respectively [5, 22]. For patients with pBPPVsr or pBPPV, repositioning maneuvers were attempted, and/or the patients were instructed to perform the Brandt–Daroff exercise at home to aid in vestibular rehabilitation. Transition between subtypes, the affected canals, and pathophysiologies were carefully recorded.
Patients diagnosed with BPPV and treated either physically or medically in other hospitals and who did not exhibit vertigo or nystagmus on positional testing were excluded from the present study because these patients did not have disease of any subtype recognized by the Bárány Society. Patients were also excluded if they were definitively diagnosed with any other vestibular disorder, or if positional nystagmus was accompanied by headache (especially migraine).
All statistical analyses were performed with the aid of SPSS software (ver. 22.0; IBM Corp., Armonk, NY, USA). Ages are expressed as means±standard deviations (SD) and were confirmed to be normally distributed. Student’s t-test (two-tailed, independent) was used to compare differences between males and females. A P-value < 0.05 was considered statistically significant.
Results
Of the 568 patients enrolled, those with established and emerging BPPV accounted for 64.44 and 35.56% of all patients, respectively. For those with established BPPV, pc-BPPV, hc-BPPV, hc-BPPV-cu, and pBPPVsr accounted for 41.90, 8.98, 1.76, and 11.80% of all patients, respectively. For those with emerging BPPV, ac-BPPV, pc-BPPV-cu, mc-BPPV, and pBPPV accounted for 0.35, 0.00, 1.23 and 33.98% of all patients, respectively. For all patients, pc-BPPV and pBPPV were the two major disease subtypes; both the anterior canal and mc-BPPV subtypes were rare, and no patient was diagnosed with cupulolithiasis of the posterior canal (Table 1, Fig. 1).
The proportion of 8 subtypes in all BPPV patients
The proportion of 8 subtypes in all BPPV patients
1. pc-BPPV: canalolithiasis of the posterior canal, 2. hc-BPPV: canalolithiasis of the horizontal canal, 3. hc-BPPV-cu: cupulolithiasis of the horizontal canal, 4. pBPPVsr: probable benign paroxysmal positional vertigo [spontaneously resolved], 5. ac-BPPV: canalolithiasis of the anterior canal, 6. pc-BPPV-cu: cupulolithiasis of the posterior canal, 7. mc-BPPV: lithiasis of multiple canals, 8. pBPPV: possible benign paroxysmal positional vertigo.
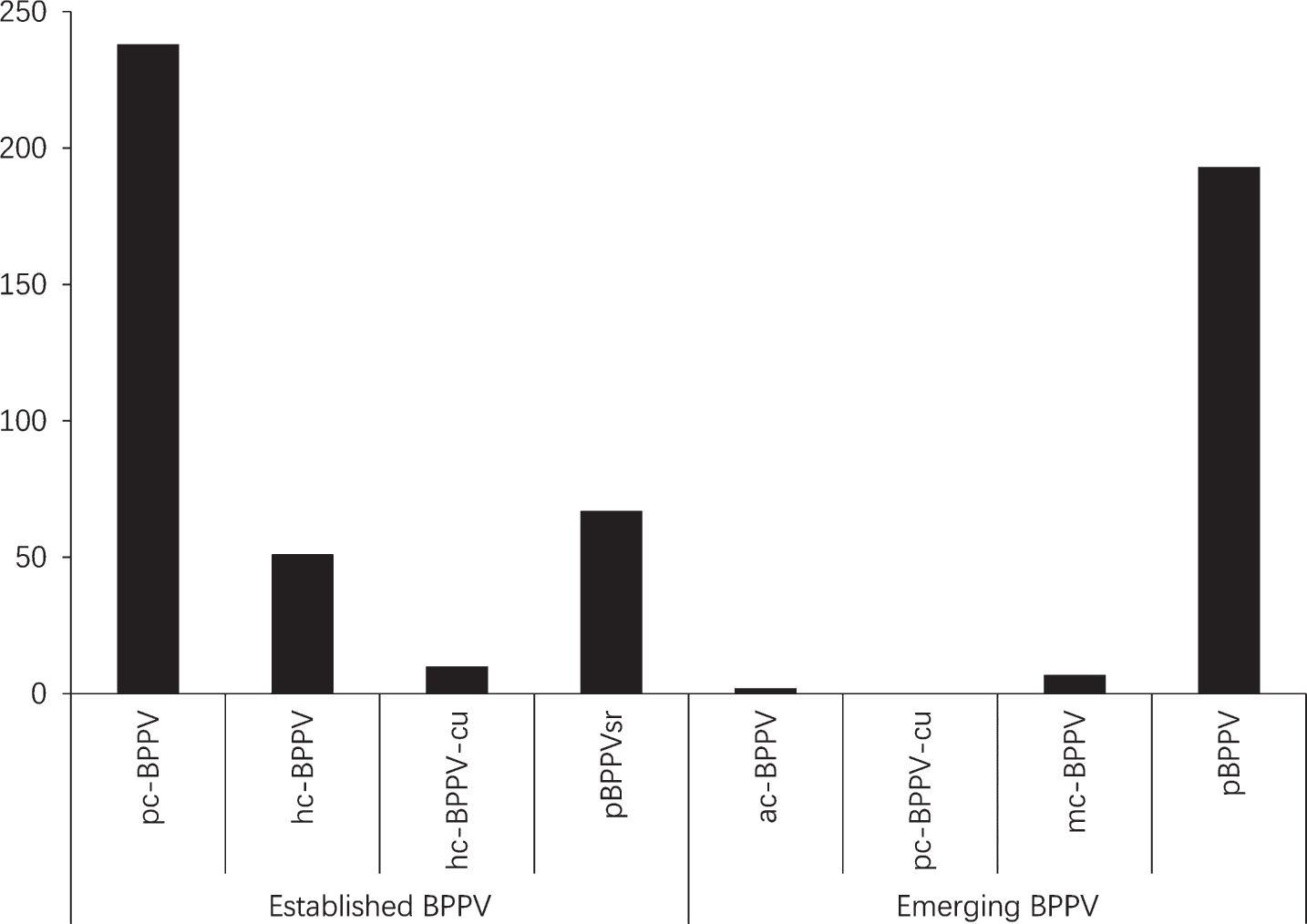
The proportion of 8 subtypes in all BPPV patients.
pc-BPPV, hc-BPPV, and hc-BPPV-cu are three subtypes of established BPPV that can be definitively diagnosed using the Bárány criteria, and the demographic characteristics of patients with these three subtypes of disease are summarized in Table 2. The posterior canal was the canal that was most affected, followed by the horizontal canal (238 and 51 patients, respectively). In terms of pc-BPPV, the number of female patients was twice that of males (females: males, 170:68) and the right posterior canal was most often affected (right: left, 148:90) (Table 2). In terms of pc-BPPV, the average age of male patients was 3 years less than that of females, but the difference was not significant (p > 0.05). In terms of horizontal canal BPPV, 15 of 61 patients could not identify the affected side. The total numbers of canalolithiasis and cupulolithiasis cases were 37 and 9, respectively, with no significant between-sex or -side difference (both p > 0.05).
Demographic features of pc-BPPV, hc-BPPV and hc-BPPV-cu patients
Ages are shown in years.
Transition between canals, and changes in the pathophysiological types of disease, occurred in 16 patients between the first and follow-up visits (10 at the first and 6 by the follow-up visit; Table 3). Transition of canalolithiasis from the posterior to the horizontal canal occurred in 11 patients. A transition from right pc-BPPV to a combination of right hc-BPPV and right pc-BPPV was evident in one patient. Two patients exhibited transitions from right hc-BPPV to right pc-BPPV, and one from left hc-BPPV to a combination of left hc-and pc-BPPV. One patient exhibited pathophysiological changes associated with a transition from right hc-BPPV to hc-BPPV-cu.
Transitions between canals and pathophysiology
1. LP: left pc-BPPV, 2. LH: left hc-BPPV, 3. RP: right pc-BPPV, 4. RH: right hc-BPPV, 5. ca: canalolithiasis, 6. cu: cupulolithiasis.
pBPPVsr and pBPPV patients constituted 45.78% of all patients (11.80 and 33.98%, respectively). Of 260 patients with pBPPVsr or pBPPV, 11 were diagnosed with pc-BPPV or hc-BPPV within the 4-week follow-up period.
A major aim of BPPV diagnostic criteria/guide-lines is to improve BPPV diagnosis [2]. Detailed diagnostic criteria for pc-and hc-BPPV are given by both the Bárány Society and the AAO-HNSF. Positional nystagmus evoked by the Dix–Hallpike maneuver and/or the roll test plays an important role in diagnosis, which must be consistent with the expected direction of nystagmus during canal excitation or inhibition of nystagmus. Although we diagnosed pc-BPPV, hc-BPPV, and hc-BPPV-cu based on the Bárány criteria, the same results would be obtained using the AAO-HNSF guidelines. pc-BPPV, hc-BPPV, and hc-BPPV-cu are three subtypes of an established type of BPPV that can be definitively diagnosed using the Bárány criteria, allowing comparisons of diagnoses and treatment effects among different institutions.
We enrolled 238 patients with unilateral pc-BPPV; the right posterior canal was affected 1.64-fold more often than the left. Brevern et al. reviewed 3,426 patients identified by a Pubmed search and found that the right ear was affected 1.40-fold more often than the left. Similarly, 54 of 80 patients presenting to their dizziness clinic were affected in the right ear; the right/left ratio was 2.08 [23]. A possible explanation for the observed difference is the preferred lateral position during sleep. Lopez-Escamez et al. found that more patients slept on the right than the left side, and the involved canal was significantly associated with the side assumed during bed rest [11]. Similar results have been reported by other investigators [10], and also upon evaluation of patients diagnosed with mild-to-moderate, obstructive sleep apnea [7]. Higher proportions of females than males had pc-and hc-BPPV, perhaps because declines in estrogen levels after menopause cause labyrinthine fluid imbalances in females [13]. The ratio of pc-BPPV-cu is 6.3%, and the incidence rate of ac-BPPV was 3% (range 1–17.1%) [1], but we did not find patients with pc-BPPV-cu although there were 2 patients with ac-BPPV in the present study. When upbeat nystagmus with torsional component evoked by Dix-Hallpike maneuver lasts longer than 1-minute, pc-BPPV-cu should be considered [21]. However, vestibular migraine and other central lesions may also present persistent upbeat nystagmus with or without torsional component [6, 8]. Therefore, careful differentiation should be made when persistent torsional nystagmus is encountered, and the clinical characteristic of pc-BPPV-cu should need further investigation.
pBPPVsr and pBPPV are another two major subtypes, accounting for 11.80 and 33.98% of all our cases, respectively. pBPPVsr was diagnosed based on a history of positional vertigo, but no observable nystagmus or vertigo during positional testing; this is thought to reflect testing during a symptom-free interval. Unlike pBPPVsr, which yielded negative positional testing results, pBPPV was associated with vertigo or nystagmus during positional testing. However, the nystagmus could not be explained by excitation of a specific canal, or inhibition of induced eye movements. Also, a specific canal could not be identified when multiple canals were involved [21]. In our previous study on 133 patients with histories of BPPV but who were negative upon positional testing (n-BPPV), and 250 patients with typical BPPV, n-BPPV was equivalent to pBPPV of the present study. 65 of 133 patients were subsequently diagnosed with typical BPPV, 37 (56.9%) within 10 days of the first visit. Patients with n-BPPV or typical BPPV did not differ significantly in terms of either treatment outcome or recurrence rate [18]. Similar results were reported by Uno et al. [20], who found that 118 of 619 (19%) patients exhibited no nystagmus but were suspected to have BPPV because they complained of vertigo episodes. Presently, we performed repositioning maneuvers on most pBPPV and pBPPVsr patients or instructed them to perform such maneuvers or Brandt-Daroff exercise at home. Although follow-up was not strict, few patients were identified with typical BPPV during the follow-up period of the present study. And the pathogenesis of the majority pBPPV patients remained unclear. It should be differentiated from vestibular migraine (VM), brainstem/cerebellar lesions, phobic postural vertigo, and chronic subjective dizziness [3, 21]. Recurrent episodic positional vertigo is a common symptom of VM which can mimic the manifestation of BPPV. Persistent pure vertical nystagmus, the duration of the symptomatic period and frequent episodes (several times per year) can help to differentiate BPPV and VM, and the migraine accompanying symptoms and other oculomotor signs can also be helpful [8, 12]. In addition, vestibular function testing and imaging should be adopted to help differentiate BPPV and other vestibular disorders, especially central disorders [19].
Otoconia debris movements between canals, or changes in the pathophysiological type of disease, can develop after repositioning maneuvers [17, 20]. In the present study, transitions between the posterior and horizontal canals, or between horizontal canal canalolithiasis and cupulolithiasis, were observed in 16 patients (5.35% of those with established pc-and hc-BPPV). Uno et al. [20] reported that 6 of 610 patients evidenced canal transitions, the incidence of which was thus very similar to that of the present study.
Conclusion
In conclusion, pc-BPPV, hc-BPPV, and hc-BPPV-cu are three major subtypes of BPPV that can be definitively diagnosed. Further work is required to determine if pBPPV and pBPPVsr patients belong to the BPPV group; appropriate differentiation and repositioning maneuvers require special attention.
Declaration of interest
No author has any conflict of interest.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (grant nos. 81271093 and 81470703) and a Shanghai Municipal Education Commission Gaofeng Clinical Medicine Grant (no. 20152233), Shanghai leading talent program (no. 2017062) and the project of Shanghai Jiao Tong University Medicine-Science and Engineering Interdisciplinary Foundation (no. YG2016ZD02).