
Abstract
BACKGROUND:
Children regularly use tablets in a variety of postures. Previous studies have shown that prolonged use of such an IT device increases the risk of musculoskeletal pain.
OBJECTIVE:
To investigate pain and muscle activity during tablet use by children in three different workstation positions–on the table with a case set, on a table, and on the lap.
METHODS:
Twenty five healthy and right-handed participants aged 10–12 years were recruited and assigned to play computer games for 15 minutes in each workstation. Pain(VAS) was measured at the neck, shoulder, upper back, and forearm regions immediately after tablet use. Electromyography (EMG) was measured at the cervical erector spinae (CES), upper trapezius (UT), middle trapezius (MT), and wrist extensors (WE) muscles during the final two minutes.
RESULTS:
Results showed that using a tablet on the table with a case set caused the least pain in the neck region (p < 0.05), compared with the use on the table and on the lap(which had pain scales of 0.37±0.86, 1.74±1.77, 1.72±1.90, respectively; mean±SD). EMG of cervical erector spinae during tablet use on the table with a case set was significantly lower (p < 0.05) than those on the table and on the lap (muscle activity of 22.38±9.54,35.37±16.82, 35.29±13.30 respectively).
CONCLUSIONS:
Tablet use on the table with a case set demonstrated a significantly lower severity of pain at the neck region than tablet use on the table and on the lap. To prevent musculoskeletal disorders, tablet use on the table with a case set is recommended as the optimal workstation for children.
Introduction
Computer tablet use has become popular globally, particularly among children. In 2018, the population of tablet user is 1.28 billion [1]. The suitable size, light weight, mobility and an easy-to-use touch screen are the properties that enable children to use them easily.
Children have been found to use information technology (IT) devices such as computers, laptops, or tablets at school and home more than twice a week [2]. Interestingly, the frequency of tablet use in children at home is greater than at school. However, such usage is not without risk as children who spend long periods of time on a tablet, in a sustained posture, can increase the risk of skeletal disorders. Regions in which problems are generally found are the neck, shoulder, upper back, and forearm [3]. In particular, for tablets, the angle of the screen is set lower than the natural height of the gaze, due to the small screen; this in turn increases the head neck flexion angle which could cause neck pain.
A previous comparison of neck muscle activity between tablet use and computer use found that the cervical erector spinae activity during tablet use was greater than during computer use. It also found that there was greater shoulder elevation with arm abduction during tablet use [4]. We have previously studied the effects of adults using tablets for 20-minutes: after this period,95% of users complained of pain in at least one region of the body, especially the neck [5]. However, there has been no previous study of pain caused by tablet use among children.
Interaction between children and computers differs from adults because children have greater trunk rotation than adults, and the cervical erector spinae muscle activity in children is significantly greater than adults [6]. The immature musculoskeletal system in children results in greater head and body proportions than adults, so the neck muscles of children probably work harder than adults in similar workstations [6]. In addition, the upper extremity and body height of children differs in muscle activity and pain experience in child users of tablets may be very different to adults. Information concerning pain and muscle activity arising from tablet use would be very useful to inform ergonomic guidelines to prevent musculoskeletal pain during tablet use among children.
The purpose of the study was to compare pain and muscle activity during touch-screen tablet use in children, aged 10–12, playing computer games for 15 minutes, in three different positions: on at table with a case set, on a table, and on the child’s lap.
Method
This study was approved by the Human Ethic Committee of Faculty of Physiotherapy, Srinakharinwirot University. A parent and child signed an informed consent form prior to participation in the current study.
Study design
Cross-sectional study design was used to examine the effect of three tablet workstation positions on pain and muscle activity in the neck, shoulder, upper back, and forearm.
Participants
Twenty-five healthy participants (13 males and 12 females), aged 10–12 years old, with a reported tablet use of at least twice a week or 2 hours a week, were recruited. All participants were right hand dominant, had no current musculoskeletal pain, and had normal or normal corrected vision, as well as a Body Mass Index (BMI) (Range = 14.5–19.3 kg/m2) and all were of a height (Range = 137.5–151.0 cm). Participants were excluded from this study if they had pain at the neck, shoulder, upper back, or forearm, or had a history of spinal, hip or arm surgery or spinal deformity.
Variables
Independent variables
The workstation positions of tablet use (shown in Fig. 1) observed in primary school children (grades 4–6) were on a table with a case set (60 degrees tilt), on a table (placed flatly on the table surface), and on the child’s lap. Participants sat on a chair and table commonly used in elementary school children with no adjustment of height and tilt. The tablet was placed directly in front of participants, 5 centimeters (cm) from the edge of the table. In the laboratory, the climate and light were controlled.
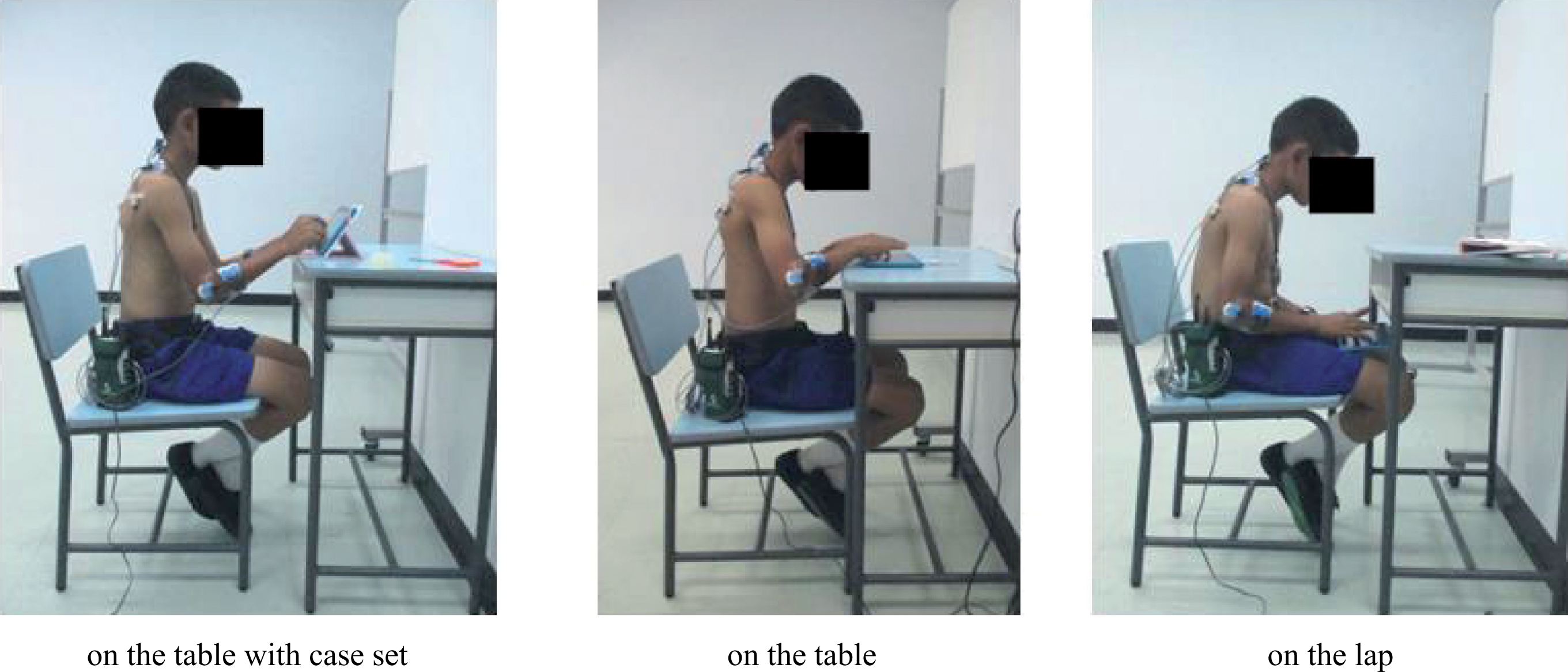
Tablet workstation positions on the table with case set, on the table, on the lap.
Location and severity of pain were measured with visual analog scale (VAS) and a body pain chart [7]. The level of pain scale was between 0–10 where 0 indicated no pain and 10 indicated extreme pain. Pain was classified into 4 levels: no pain (VAS = 0–0.04), mild pain (VAS = 0.05–2.5), moderate pain (VAS = 2.6–5.0), and severe pain (VAS = 5.1–10) [8]. Muscle activity was measured in the last 2 minutes of a 10 minute session by electromyography (Noraxon USA) using surface electrode placement at abdomen area [9, 10] and ground at the lateral epicondyle of the elbow [11]. The EMG signals are collected with a 16-channel surface EMG system (MyoSystem 1400A, Noraxon U.S.A. Inc., Scottsdale, AZ, USA). Cervical erector spinae (CES), upper trapezius (UT), middle trapezius (MT), and wrist extensors (WE) were the muscles that collected the signals of EMG. Lateral epicondyle of the humerous is the location to place the ground electrode. Raw EMG data was rectified with Band-pass filter 16–500 Hz and calculated Root Mean Square and Smooth at 100 ms.
Instrumentation
VAS is a line with two endpoints of 0 (no pain) and 10 (severe pain). The participant was asked to mark a level of pain on the VAS line. The body pain chart reached of several areas. These are the neck, shoulder, upper back, and forearm regions of the human form. A participant was asked to shade the body areas where they feel pain. Table (width x depth x height = 59×39.5×70 cm) and chair (width x depth x seat height x total height = 41×41×38×73 cm) for elementary school children. The EMG signals are collected with a 16-channel surface EMG system (MyoSystem 1400A, Noraxon U.S.A. Inc., Scottsdale, AZ, USA). Cervical erector spinae (CES), upper trapezius (UT), middle trapezius (MT), and wrist extensors (WE) were the muscles that collected the signals of EMG. Lateral epicondyle of humerous is a location to place the ground electrode. Raw EMG data was rectified with a Band-pass filter 16–500 Hz and calculated a smooth signal at 100 ms.
Task
A computer game with delightful color and fun game play, which is appropriate for children, was provided which children played for 15 minutes in each workstation position, with a 15-minute rest period between workstations.
Procedure
Instructions concerning the required workstations and tasks were given. A surface electrode was placed and the maximum voluntary contraction (MVC) of (Cervical erector spinae, Upper trapezius, Middle trapezius, and Wrist extensors) were collected for normalization. Participants performed tablet use in three workstations given at random via a sealed envelope, with 15 minutes for each workstation and they were given a 15-minute break before the next station started. Participants were asked to indicate the location and severity of pain on the body pain chart and visual analog scale immediately after each 15 minutes of tablet use.
Statistical analysis
The Kolmogorov-Smirnov test (SPSS for Windows® version 20, SPSS Inc., Chicago, IL, USA) was used to confirm normal distribution. The differences of pain and muscle activity between workstations were compared by using one-way ANOVA and Bonferroni correction which were selected to evaluate the differences in process of post hoc multiple comparison analysis that was suggested by ANOVA. The significance level was 0.05.
The percentage of participants who experienced pain, the number of regions and intensity of pain in the region were marked on the body chart and was calculated for mean and standard deviation.
Results
Participants
Twenty-five participants comprising 13 males and 12 females, aged 10–12 years (Mean±SD =11.04±0.79 years). Height ranged from 137.5–148 cm (Mean±SD = 141±4.69) in males and 138.5–151 cm (Mean±SD = 146.2±5.2) in females. The average Body Mass index (BMI) was 16.7±2.2 kg/m2 in males and 17.2±2.1 kg/m2 in females.
Pain
Severity of pain
Pain level at the neck region during tablet use on the table with a case set was statistically significantly lower than with tablet use on the table, and on the lap. (p = 0.005, of which the average severity of pain during tablet use on the table with a case set and on the lap were 0.37±0.86 and 1.72±1.90 respectively). In addition, for the use of the tablet on the table with a case set, the severity of neck pain was statistically significantly less than on the table, without a case set (p = 0.002 of which the average severity of pain during tablet use on the table with a case set and on the table without a case set were 0.37±0.86 and 1.74±1.7 consecutively) (Table 1).
Severity of pain (VAS) during tablet use on the table in three positions
Severity of pain (VAS) during tablet use on the table in three positions
**Repeated measures ANOVA, significant different at 0.05 level. ¥Severity of pain (VAS): No pain (0–0.04), Mild (0.05–2.5), Moderate (2.6–5.0), Severe (5.1–10) [8].
Four pain levels were used to define the severity of pain (no pain, mild pain, moderate pain, severe pain) [8]. Results showed that five participants reported mild pain and only one participant reported moderate pain, at the neck region, while using a tablet on the table with a case set; no participants reported severe pain. Interestingly, moderate and severe pain at the neck were reported after tablet use on the table (moderate: n = 6, severe: n = 1) and on the lap (moderate; n = 4, severe: n = 3) (Table 2).
Number of participants experiencing pain and severity of pain at neck, shoulder, upper back and forearm (N = 25)
Number of participants experiencing pain and severity of pain at neck, shoulder, upper back and forearm (N = 25)
Pain at the upper back and forearm were not reported as moderate and severe pain, but only as mild pain (Table 2).
The number of participants who reported any pain while using the tablet on the table with a case set was less than when using the tablet on the table or on the lap (64%, 88%, and 88%, respectively (Table 3).
Number of participants experiencing any pain, number of regions, intensity of region marked (the highest severity of region was considered) and overall intensity (N = 25)
Number of participants experiencing any pain, number of regions, intensity of region marked (the highest severity of region was considered) and overall intensity (N = 25)
Tablet use on the table with a case set showed fewer pain regions, compared with use on the table or on the lap (average number of regions at 0.92, 1.28, and 1.32, respectively) (Table 3).
Tablet use on the table with a case set showed less intensity of regions marked (the highest severity of pain in all regions was considered), compared with the tablet on the table or on the lap with an average intensity of the region marked at 1.3, 2.0, and 2.1 respectively (Table 3).
As for overall intensity, the average overall pain intensity after tablet use on the table with a case set was less than that with the use on the table or on the lap (overall intensity of 1.7, 2.0, and 2.1, respectively (Table 3).
The EMG of cervical erector spinae while using the tablet on the table with a case set (22.38±9.54) was significantly lower (p = 0.001) than tablet use on the lap (35.29±13.30) (p = 0.001)or on the table (35.37±16.82). However, no significant difference was found in EMG recorded at this muscle between tablet use on the table and on the lap (Table 4).
Electromyography of Cervical erector spinae, Upper trapezius, Middle Trapezius and wrist extensors during tablet use in three workstations (N = 25)
Electromyography of Cervical erector spinae, Upper trapezius, Middle Trapezius and wrist extensors during tablet use in three workstations (N = 25)
*Repeated measures ANOVA, significant difference at 0.05 level.
The EMG of upper trapezius during tablet use on the table (22.38±9.54) was significantly (p = 0.004) higher than on the lap (13.73±10.69), but there was no significant difference between other workstation positions (Table 4).
The EMG of wrist extensors during tablet use on the lap (18.79±10.31) was significantly (p = 0.005) higher than on the table (15.30±6.69), but there was no significant difference between this muscle when compared with the other workstations (Table 4).
There was no significant difference for the middle trapezius after 15-minute tablet use in the three workstation positions (Table 4).
The current study was the first to examine pain and muscle activity simultaneously during tablet use among children in three different workstation positions. Results were notable in that pain at the neck region during tablet use on the table with a case set was significantly lower than in other positions (on the table and on the lap). Furthermore, the study showed clearly that pain, number of regions marked, intensity of region marked, and overall intensity during tablet use on the table with a case set tended to be lower than on the table and on the lap. The tablet screen was close to eye level while using the tablet on the table with a case set which led to less neck flexed posture compared with the other two workstation positions. Young et al. (2012) similarly found that adults who used a tablet on the table with a case set (63 degree tilting) had better head neck posture than when used on the lap [13]. Ergonomic guidelines for computer users have suggested that the desktop screen should be located close to eye level, requiring not too much bending over or bending down, with the neck in straight alignment [5, 14]. Current findings are also consistent with Grieg et al.’s results (2005) which showed that a workstation with a low screen desktop could affect users which lead to neck pain. The head and neck flexion of users would be increased, thus the neck muscle need to work harder to resist gravity and ultimately lead to increased head neck flexion moment [2, 16]. In addition, head and body proportions in children are greater than in adults [17], and the relatively higher level of force on neck structures such as the tendons, bones, and joints could result in pain and muscle overuse.
The EMG of the cervical erector spinae in tablet use on the table in the current study was similar to previous studies [17]. The average EMG was 35.29 and 38.0 respectively because both studies set tablet use on the table, 5 cm away from edge, and over a short duration.
Furthermore, this study found that regarding tablet use on the table, upper trapezius muscle activity was significantly higher than on the lap workstation. Children had shoulder elevation, and placed arms on the table so they could use the tablet comfortably; this concurred with Straker et al.’s observations of shoulder elevation and arm abduction in children while using tablets on the table [4].
It was obvious that participants reported pain at the neck region in tablet use on the table and on the lap significantly greater than in the other workstation (p = 0.005; average severity of pain at neck region was 1.74, 1.72 and 0.37 respectively). Due to children sitting in ‘over flexion’ neck postures for long duration, overuse of neck muscle activity occurred – also called sustained muscular contraction17.Sustained muscular contraction could decreased blood flow into that muscle and finally result in pain. However, pain was reported in mild levels (VAS <2.5 in 10) in all workstations. It may be caused by no adjustment in the workstations; table and chair. Only the positions of the tablet were adjusted.
Limitations of the study
This study investigated pain and muscle activity during tablet use in children (aged 10–12 years), and results should be applied to this age group. Further studies on the effects of tablet use and EMG in other age groups in different workstations, such as adjusting tablet and chair, should be examined. This study indicated that participants reported pain after 15 minutes of use; it is unclear what may happen over longer periods. This study is a cross-sectional study which collected data, studying pain within children after one time use of tablets. The results of this one time study found that the pain level was low.
Clinical application
Results of this study can inform ergonomic guidelines for tablet use among children. We would recommend that children in this age group should use a tablet on a table with a case set as opposed to on the lap to prevent the risk of musculoskeletal pain and reduce neck muscle activity.
Conclusion
Tablet use on the table with a case set showed a significantly lower severity of pain at the neck region than tablet use on the table and on the lap after the use of 15 minutes. Cervical erector spinae muscle activity was also significantly lower in this position. EMG of the upper trapezius and wrist extensor were higher for tablet use on the table compared with use on the lap. Nonetheless, there were no significant differences for the middle trapezius among the three workstations.
Conflict of interest
None to report.