
Abstract
BACKGROUND:
The use of electronic health records (EHR) is related to the improvement of service quality and care coordination. The design of this platform generally focuses on the individual use of the system and does not integrate the specific needs of workers to provide support for collaborative activities.
OBJECTIVE:
The study investigated how activity ergonomics (AE) contributed to improve the design of an EHR that supports the collaborative mental health care of children and youth.
METHODS:
This qualitative study, based on the theoretical framework of AE, used individual and group interviews and document analysis as research procedures. The data collection occurred between March and September 2017 in Rio de Janeiro, Brazil.
RESULTS:
The study highlighted the following points: the characteristics that marked the different perceptions of workers regarding the use of a communication tool for collaborative care; the problems related to spreadsheet usability; and the desirable attributes that should be considered in the conception of a new EHR.
CONCLUSIONS:
The research indicated that AE favors improving the design of an EHR by incorporating the work dimension into the project.
Introduction
Since 2014, the Research Group on Public Mental Health Policies (RGPMHP) of the Federal University of Rio de Janeiro has developed a project to improve access and quality of care for children and adolescents with mental health needs, based on collaboration, co-responsibility, and knowledge sharing among professionals from distinct sectors and services. The project, entitled “Network, Territory and Psychosocial Care for Children and Youths: Sharing and Intersectoral Collaboration,” is based on a collaborative care (CC) strategy among services historically committed to the care of this population; Fig. 1 demonstrates the network of services covered by the project [1].
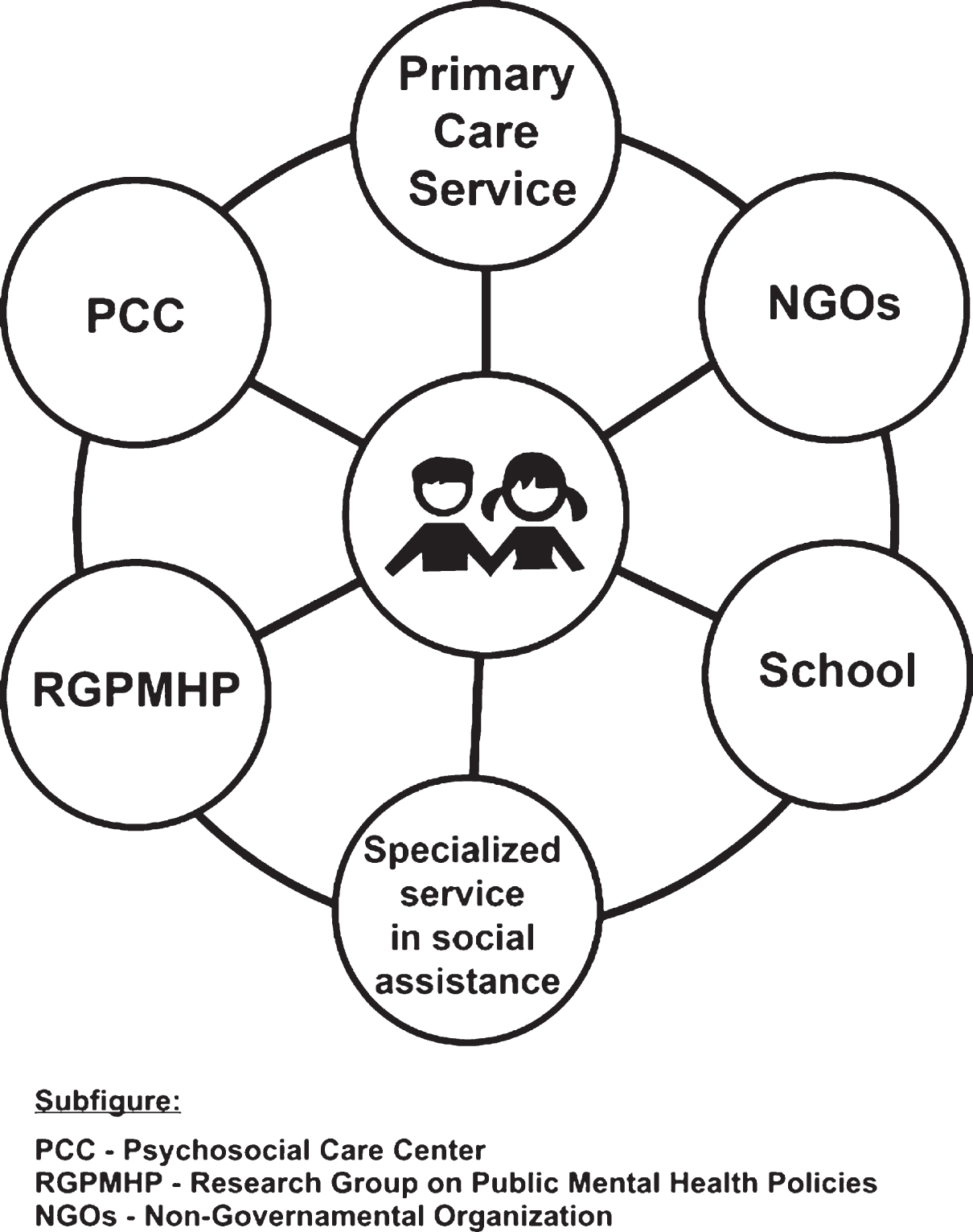
Network of services covered by the CC project.
Collaborative Care is a multifaceted organizational intervention that includes the following: a case manager, who is responsible for the care management of people with mental health problems; mechanisms to promote a liaison between primary care and mental health specialists; and mechanisms to collect and share information on the progress of users [2]. Implementing a CC driven information sharing strategy among professionals from different health or social institutions, user-centered care, and changes in work processes to overcome fragmented care actions among services themselves and users.
In this sense, CC must be established through a partnership between professionals with active and regular forms of exchange. These goals can be accomplished through meetings, discussion of cases, implementation of information technologies, and the development of actions to promote mental health [2–4].
Within this realm, communication is one of the critical factors for consolidating the integration between services, because an effective articulation of work between the different services and professionals depends on the quality and integrity of the information exchanged [5].
Thus, to meet the communication demands of the CC project explored in this article, a spreadsheet, available online through a cloud service, was developed. Regulated by rules and conventions, this solution was then used for several months. However, both the registration of the cases and the consultation of the information in the spreadsheet did not meet minimum usability requirements, which reduced the use of this solution.
Thus, an electronic health record (EHR) project was initiated to find a substitute for this spreadsheet. The reason for choosing such a system was because this type of tool directly relates to the improvement of service quality and care coordination [6–8], which aligns with the purposes of the project developed by RGPMHP.
Although, the EHR design generally focuses on the individual use of the system and does not integrate the specific needs of the workers to provide support for collaborative activities [9]. To address this gap, the EHR project in this study took a different path based on the principles of activity ergonomics (AE), which includes an analysis of the work of the EHR users, meet the demands of work collaboration.
Therefore, this article shows the contributions of AE in the process of the participatory design of an EHR that aims to support the collaborative mental health care of children and youth in Rio de Janeiro.
The theoretical framework that guided the design of the EHR tool was the ergonomics of activity (EA), which is a comprehensive approach that explores the content of the work and its consequences both for the health of workers and for production. Thus, this discipline studies the experience of working in real contexts, revealing the strategies used by workers to overcome unforeseen events [10–15].
Additionally, the approach of studying actual work can highlight problems of work inadequacy that can be caused by projects of production systems, processes, work organization, tools, and tasks[15, 16].
Specifically, in computer device design processes, such as that built for the CC project, EA has specialized in studying computer activities that predict difficulties related to the work use situation of the system [17]. EA also supports other methodological approaches that include the dimension of use in design processes, such as a user-centered approach and participatory design.
The user-centered design approach, a broad term to describe a design process in which end-users influence how a design takes shape [18], emphasizes the importance of having a good understanding of the users, without necessarily involving them actively in the design process [19]. The participatory design approach presents another perspective about the role of the user in the project. The research and practice of participatory design can underscore how collaborative processes can enable the participation of those who will be affected by the results. In this scenario, the design is understood as a process driven by social interaction and engagement among users and designers [20–23].
Other concepts explored in computer design processes by AE are utility and usability [17]. For EA, utility is relative to the needs of work situations and corresponds to significant advantages for the user in a given activity. However, this advantage should always be relativized by its objectives, the tools available, the environment of use, and its interdependence with other activities.
There are several interpretations for usability. In this context, we adopted the definition that indicates “how useful, usable, and satisfying a system is for the intended users to accomplish goals in the work domain by performing certain sequences of tasks” [24]. A computing device, however, may have positive usability ratings without users being able to satisfy their goals, a situation that usually occurs when the model used in the project follows general heuristics, not taking into account specificities of the actual work [6, 25].
In addition to the unique integration of the operator and the work dimension in the computer device designs, according to Burkhardt and Sperandio [17], an adequate methodology of cooperation, collection, and analysis is both necessary and complementary. EA procedures can, thus, contribute to the process of participatory projects of technological systems, including the analysis, the work, tools, prototypes, and user satisfaction.
Based on the studies mentioned above, the designers, in general, materialized solutions in the form of blueprints, models, prototypes, and beta versions of the system. The models were developed to perform simulations that created and validated the design choices with the users before the project was finalized.
An assessment of the proposed solutions should be done at every stage of the design process. Thus. two assessment models can thus be put into motion: one that requires direct participation of the users and another that involves analyzing interface characteristics while focusing on specific technological issues.
After the development, assessment, and construction of the computer system, the last stage of the project consisted of examining its use in a real-world environment, followed by an assessment of its field use, to obtain information about the difficulties encountered by the workers in conditions not anticipated during the testing phase.
Methods
Study design
This study was a qualitative investigation, and its procedures for collecting and analyzing data were guided by the theoretical framework of EA, which includes the following research stages: 1. demand analysis; 2. organizational, technical, economic, and social environment analysis; 3. analysis of the work activities and situations; and 4. a review of the results, a validation of the study, and formulation of recommendations to improve the work [10].
The results of the demand analysis phase, which used individual and group interviews and document analysis as research procedures, are presented. The data collection occurred between March and September 2017.
Study setting and sampling
The study was executed within three services involving the mental health care of children and youth in a specific region of Rio de Janeiro. The services included a primary health care service, a psychosocial care center (PCC) and members of the RGPMHP group. This final group is a service affiliated with the Federal University of Rio de Janeiro that develops studies that investigate the adequacy of public policies regarding mental health in Brazil; these studies required the EHR project addressed in this article. Team composition and figures are provided on Table 1.
Team Composition and number of professionals
Team Composition and number of professionals
The participants were recruited through informational meetings, and the anonymity and voluntary participation of the workers were ensured. The purposeful sampling strategy was used to identify and select workers who used the spreadsheet that was no longer in use to share information, as well as other professionals who had experience in the mental health care of children and adolescents and who perceived the need for integration among services.
A general practitioner (GP), a nurse, and a community health agent (CHA) from the primary care service, as well as two psychologists from the PCC and a researcher linked to RGPMHP, were interviewed. These professionals were selected by the leadership in the work developed by the project in their services, that have been identified as key professionals of Collaborative Care.
We used non-directed interviews that aim to explore the perceptions of professionals on the usage of the old spreadsheet and what they want for the future tool. They were recorded and then transcribed.
The content of the spreadsheet that the professionals previously used to share information regarding cases was analyzed. The results of this analysis were the basis for eliciting the first data on information sharing between the services explored in this study, as it represents the nature, volume and content of information shared between the users, as well indicates communications and solicitations between users. Both interviews and spreadsheet content were analyzed using the content analysis principles proposed by Mayring (26) which was carried out in three phases. The first phase consisted of the material organization, by reading, formulating hypotheses and objectives, referencing contents, and elaborating indicators. The second phase constituted in categorizing the material. In the last phase, we conducted the reflective and critical content analysis. The categories were based on the verification of the records made during the research, being, therefore, the open model of categories, which is recurrent in exploratory studies (27).
Ethical procedures
This research project was approved by the Research Ethics Committee of the Institute of Psychiatry of the of the Federal University of Rio de Janeiro (61982216.9.0000.5263). All members participated voluntarily and provided written, informed consent. In order to protect the privacy of workers and their services, any personal or identifying information was omitted.
Results
The results highlighted the following points: the characteristics that mark the different perceptions of workers regarding the use of a communication tool for CC; the problems related to spreadsheet usability; and the desirable attributes that should be considered during the conception of a new EHR.
The different perceptions of workers regarding the use of a communication tool directed toward CC
Through the data analysis, the results identified the different perceptions that workers have regarding the objective and use of a tool for sharing care information. Concerning to the perception of the professionals from the primary care center, the GP and nurse wanted to access and register the health condition data of a given child, while the CHA considered family organization aspects to be more important, even though all three worked for the same service.
In turn, psychologists from PCC wanted to obtain data on school attendance. Besides, they deemed critical the narrative reporting of all activities performed in their service as critical, whereas the GP wanted to access more concise information.
The perceptions on the communication tool in use expressed by the RGPMHP professionals addressed questions related to mental health work prescriptions, which were based on public policies, rather than questions related to the usage of the tool.
In summary, mental health CC for children and youth encompasses an intersectoral network of services that are articulated in the construction of care. This type of organization requires an intensive exchange of information from experts of distinct backgrounds, such as social workers and education and health care professionals. Because the workers have different values, tools, and practices, the challenge of sharing information is not overcome merely by overlapping of narratives.
Reddy and colleagues [9] showed that EHR projects that seek to support collaborative work must exceed the assessment of the necessity of information. Instead, the projects must recognize the multiplicity of settings and perspectives that are at stake, because the differences will have implications on how the information is registered within the system and whether the information will favor or hinder collaboration [9]. Therefore, the first challenge identified in our research was building a tool that integrated different values and practices in mental health care for children and youth.
According to Daniellou and Béguin [28], the need to integrate different points of view in a project created additional difficulty in the work process because, whatever the object of conception, these viewpoints cannot be unified from a juxtaposition of technical systems. It will always be necessary to integrate the distinct points of view on the object in a coherent and coordinated way. Similarly, it is expected that the EA contributed prominently to the design of the EHR, by providing the characteristics of each of the professional areas involved in the CC project.
Problems related to spreadsheet use and the desirable attributes that must be considered in the creation of a new EHR
The difficulties in the use of the spreadsheet as a communication platform between the services of the CC project, as identified by the workers within this study, are listed in Table 2.
Difficulties perceived per professional
Difficulties perceived per professional
The data indicated two obstacles regarding the use of a communication tool. The first hindrance to the use of the tool concerned unexpected issues that emerged from working conditions, such as the scarcity of computers in the services and the difficulty of accessing the Internet.
The guarantee of access to both computers and the Internet is a condition necessary for the operation of the information-sharing tool; however, designers do not always foresee and thus address these problems. Hence, design solutions can be improved by highlighting the difficulties faced by the workers in their daily lives and understanding the causes, such as the challenges of financing for maintenance of equipment.
The second difficulty was related to the usability dimension, characterized by the difficulty in finding information and inserting data on the spreadsheet and by the incompatibilities among the different software used by professionals of the CC services. Usability issues are elements that limit the use of the information exchange tool.
Further, the organization of work, in the different settings covered by the CC project, must allow professionals to have time to register, update, and consult data related to the cases studied. Thus, information about the work process must not be neglected, because in-depth knowledge about work conditions provides crucial elements; the designers of the new tool can then match this information with the characteristics of the real work.
The possibilities of exchanging messages between professionals and access through smartphones exemplify desirable requirements for the new EHR (Table 3).
Desired Requirements per professional
Instant messages are already used by an application that allows the rapid exchange of information. However, the messages exchanged are difficult to recover, which makes a more in-depth analysis of the cases difficult to challenging.
The desire to access the tool through smartphones is closely associated with the infrastructure problems, such as lack of computers and the poor quality of the Internet, in the services that we studied. Further, access via mobile devices is related to the nature of the position of the CHA, who works in the territory served by the primary health care service.
Studying the frequency of registered patients using the services was shown to be significant for the psychologists because they could monitor the adherence of a patient to a specified therapeutic plan.
General Practitioners and primary care nurses professed a need for accessibility to case summaries, as these professionals manage many patients and need to access the characteristics of the disease and the current treatment of the patient instantaneously during a consultation.
The compatibility of the tool with different devices and platforms is essential to support the transportation of information on cases from other registry devices, such as electronic medical records.
Information security was required by the CHA to allow the possibility of deleting sensitive data, because these types of professional practices are located in extremely violent urban areas and there are fears that the exposure of patient data could generate reprisals to those reporting this information in the system. In the old tool, such workers were only allowed access to the consultation of specific data, revealing an inequality of status between the professionals of the CC project. For the design of the new tool, it is understood that, because it is collaborative, this inequality must be overcome.
Finally, concerning alerts and notifications for each new entered piece of information into the tool on cases, the classification of data by type of service and the search function have the potential to improve the usability of the tool in the daily work of the professionals.
Table 4 summarizes the characteristics of the spreadsheet and the new requirements suggested as a way to make the tool adequate for collaborative care.
Comparison between spreadsheet characteristics and new requirements for the EHR
The data regarding the usage problem and desirable requirements for the new tool will serve as a base for the creation of a new EHR. These data are closely related to the perception of the professionals interviewed and are also supported by previous experience with the information-sharing worksheet. However, the design of the new EHR cannot be based only on the correction of the difficulties experienced with the prior instrument and the list of desirable requirements without contextualizing them with the actual work of its operators.
More than the design of a technological tool, the construction of the collective work of the teams involved in the CC project is a crucial element. Each team involved carries its operative modes and perspectives of tool handling, which are distinct from each other but have a common goal: the patient’s care. Collaboration, characterized as a collective activity in which operators perform on the same object but with different operations that are articulated with one another with a common goal in the short or medium term [29], is an essential requirement for theproject.
For Caroly and Barceline [30], collective work situations were increasingly equipped with computer tools that sustained teamwork but were often thought of in terms of maintaining the cooperation prescribed rather than supporting the construction of collective activity. Few tools directly support the construction of representations about the competencies, roles, and expertise of other workers, which limits the possibility of using them as an ultimate resource for the development of the collective work. According to Schmidt [31], the issue of how multiple users work together and coordinate their individual activities—“through” the system or “around” it—was not addressed directly and systematically as a specific design question.
Several studies highlight the need for applications of a socio-technical approach for the creation of information technology [32]. These needs can be reduced by bottom-up studies, like those based on the AE guidelines, that address the complexity related to the work, instead of representing it by means of abstract models. Additionally, this kind of research is not based on preconceived and formal representations, but on empirical studies, often qualitative, that offer a sociocultural everyday process perspective [32–34].
From a participatory design approach and vision, the development of computer-based systems that support the articulation of cooperative work to make the work more flexible, efficient, and practical underscores how multiple users must coordinate and mesh their activities [35].
Activity Ergonomic, therefore, favors the improvement of the project considering that the worker is both a device user and an operator whose actions have a purpose. From the perspective of the framework of EA, the worker is thus a co-designer [15, 36].
Conclusion
This study showed the contributions of AE in the process of the participatory design of an EHR that supports the collaborative mental health care of children and youth in Rio de Janeiro.
Therefore, its contribution was to put into evidence the perception of workers about the use of EHR to incorporate some aspects of the work dimension into the design of a new EHR.
Nevertheless, in addition to the in-depth work analyses, which will be conducted in a future study, it is vital to promote discussions among the different users. In this sense, the simulation is a crucial step to enable workers to develop a common representation of the object being designed and discuss the controversies surrounding its future activity [23, 37–39].
Thus, for further analysis, simulations will be conducted using paper mockups of the software to approximate work situations confirming or discouraging the design requirements presented here. In addition to allowing the development of collective work, which is the primary goal of the new EHR, the simulations should strengthen the reiteration of the rules of EHR use and the discussions about the quality criteria.
In conclusion, although this study has the limitation of being a preliminary report of the first step of one research study, its results can be incorporated into a reflection on the accomplishment of a participatory design of an EHR without a generalization of its effects.
Conflict of interest
None to report.