
Abstract
BACKGROUND:
Many factors threaten occupational health and safety, such as technology and production systems used by businesses as well as employee qualifications. This research addresses the issue of how these factors have become a threat to occupational health and safety.
OBJECTIVE:
This study aims to determine whether healthcare professionals’ fatalistic perceptions affect their perceptions of occupational health and safety practices.
METHOD:
The population of the study consists of 538 nurses and other auxiliary healthcare professionals working in a private hospital in Istanbul. The study initially intended to reach the whole population without establishing a sample, but 221 (41.1%) employees were reached due to reasons such as the shift system, employees’ unwillingness to participate, and personnel on leave. The study employed a survey form consisting of three parts as data collection tool. The first part of the survey includes demographic information, the second part is a Fatalism Scale and the last part is the Occupational Health and Safety (OHS) Practices Scale. Descriptive statistical analyses and SEM analysis were used for data analysis. The analyses were performed within the 95% confidence interval.
RESULTS:
A negative relationship was found between fatalism and occupational health and safety practices. In addition, employees’ fatalistic perceptions negatively affect their occupational health and safety practices.
CONCLUSION:
Fatalistic perception plays an important role in occupational health and safety practices. For this reason, employees can be shown through trainings that occupational accidents are not fate and can be prevented by certain measures they can take.
Introduction
Work is at the heart of a working person’s life. Both in the private and public sectors, if a person has a safe job that is a source of health for him. People who spend one third of their days doing their jobs in their workplaces face various hazards and occupational diseases caused by their work or working conditions [1]. A healthy and safe working environment leads to a positive perception of the workplace by society as well as a positive perception of the health of the individual.
Ensuring employees’ occupational health and safety positively affects their quality of life and productivity and occupies a very important place in this context [2–6]. The employer’s biggest responsibility is to create a healthy and safe working environment for their employees [7, 8]. Occupational health and safety practices at the workplace are an important responsibility towards not only employees but also their family and friends [2, 9]. When the employer provides this environment, this enables the employees to get fewer occupational diseases and prevents them from having occupational accidents.
Unfortunately, many employers do nothing about their employees’ health and safety. Even worse, they do not realize that the practices required for occupational health and safety at the workplace are their moral and legal responsibilities, and they see them as a sanction imposed by the state [10, 11]. Such thoughts may affect the priorities and policies of the business and may directly or indirectly affect the individual decision-making conditions and employees’ attitudes and behaviors [12].
This issue (i.e. occupational health and safety) is in direct relation with the right to live, which is the fundamental right and allows the enjoyment of all remaining rights [13]. Practices related to occupational health and safety are of great importance for employers and employees, and they should be carried out within the framework of a program [14]. As former UN Secretary-General Kofi Annan stated, “Safety and health at work is not only a sound economic policy- it is a basic human right” [15].
Occupational health and safety is defined as the scope of the employees’ mental, emotional, and physical well-being regarding the conduct of their work [16]. According to Bingöl [14], occupational health and safety means to protect the employee’s health and to eliminate the existing dangers that may harm him.
The main objective of occupational health and safety is to determine in advance the problems in the working environment that may harm the employees, to take necessary measures, to ensure work is performed in a safe environment, and to protect the employees’ psychological and physical health against various hazards and occupational diseases [17]. In the context of the health sector, this objective is to improve the health and safety of healthcare professionals. To put it more clearly, it is the creation of a safe health facility environment that does not include physical, chemical, biological, and ergonomic hazards and risks, occupational diseases, and occupational accidents that occur in the working environment and harm health [18]. In this case, occupational health and safety can be defined as preventing employees’ exposure to chemical, biological, and physical hazards related to working or eliminating diseases, injuries, and disorders that may hamper the work [19].
Employees face many problems that threaten their working lives. Among these problems are those related to health [occupational diseases, stress, alcohol and drug addiction) and safety [factors resulting from human and organizational unsafe behaviors) that usually occur in all businesses as well as problems caused by factors such as technology and production systems used by businesses as well as employee qualifications [19]. In this case, the basic question is: “Should a scientific approach be taken to solve occupational health and safety problems, or should it be left to fatalism?”
Fatalism refers to the worldview that everything is predetermined by fate, and that man cannot change that predetermined fate [20]. According to Giddens [21], a fatalistic view is an obedient approach which accepts that events proceed in a predetermined course. Hence, the expressions “what would happen happened” or “what will be will be” can be summarizing the fatalistic approach [22].
Some studies conducted on fatalistic perceptions suggest that individuals with high fatalistic perceptions take risks but do not take precautions for protection or safety [23–25]. Similarly, Rundmo [26] found that fatalistic perception, one of the sub-dimensions of safety attitude, affects employees’ risk perception. On the other hand, in another study, no relationship was detected between fatalistic perception and compliance with safety rules, use of protective equipment, and risk-taking behaviors [27]. In this regard, the purpose of this study is to determine whether healthcare professionals’ fatalistic perceptions affect their perceptions of occupational health and safety practices. To this end, the hypotheses of the study were formulated as follows:
H 1: There is a relationship between employees’ fatalistic perceptions and their occupational health and safety (OHS) practices.
H 2: Employees’ fatalistic perceptions affect their OHS practices.
Materials and method
The population of the study consists of nurses and auxiliary healthcare professionals working in a private hospital in Istanbul. The total number of nurses and other auxiliary healthcare professionals working in the hospital is 538. The study initially intended to reach the whole population without choosing a sample, but 221 (41.1%) employees could be reached due to reasons such as the shift system, employees’ unwillingness to participate, and personnel on leave.
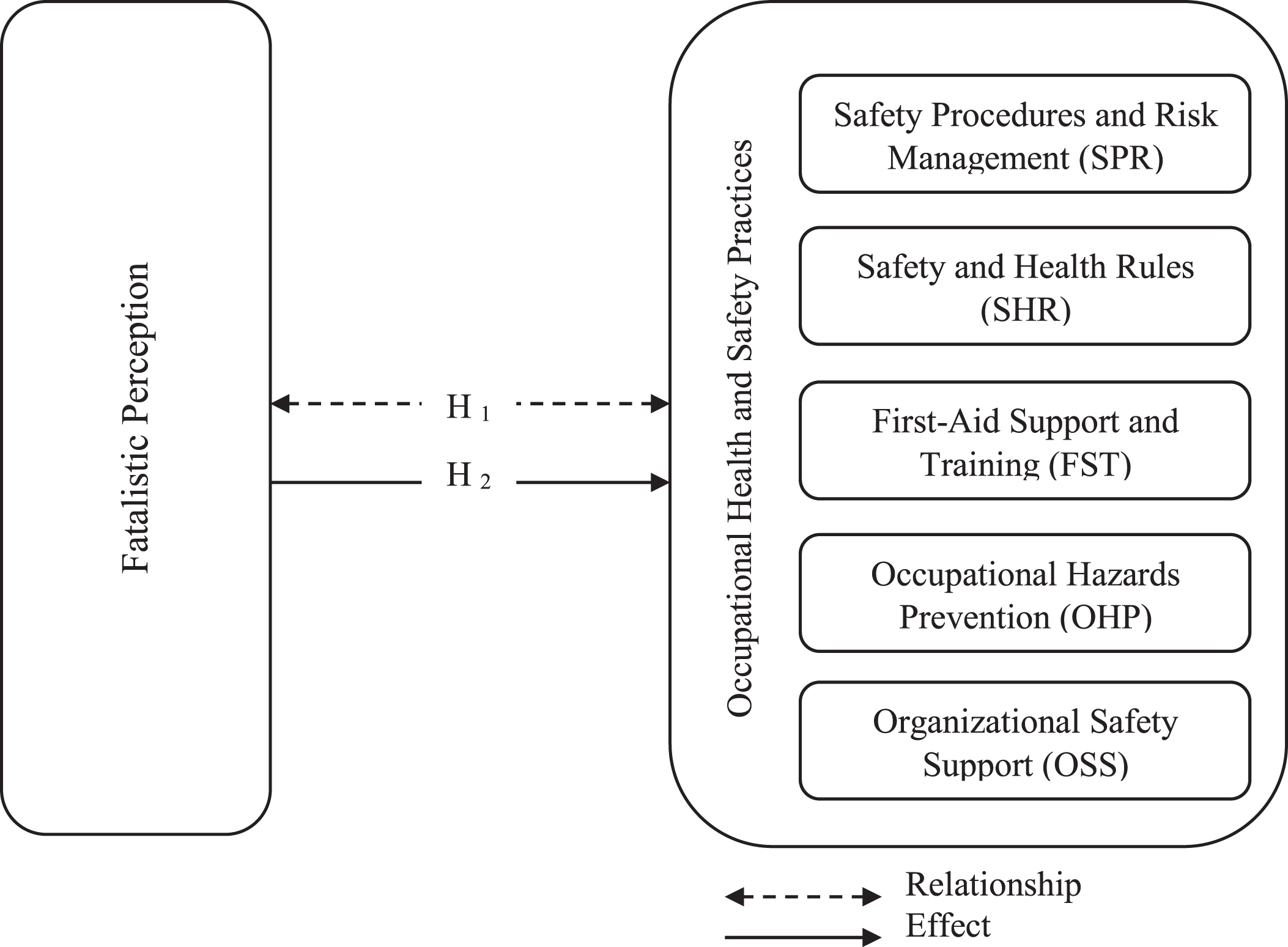
Research model.
The study employed a survey form as data collection tool. The survey form consists of three parts: Demographic Information, the Fatalism Scale, and the OHS Practices Scale. This study used a 5-point Likert-type scale. The participants were asked to choose the best among the options from 1- “I totally disagree” and 5- “I totally agree” in the survey form.
Demographic Information includes 14 questions designed to measure the participants’ demographic variables such as age, gender, educational background, profession, working time, whether or not they have been exposed to an occupational disease, occupational accidents, a near-miss accident or witnessed a friend’s involvement in an occupational accident before.
The Fatalism Scale was developed by Rundmo and Hale [28] and translated into Turkish by Dursun [25] from Havold and Nesset [29]. The validity and reliability analyses of the scale were conducted by the researchers. The scale consists of 7 questions and evaluates the employees’ fatalistic beliefs about occupational accidents.
The OHS Practices Scale consists of 29 items and 5 dimensions for measuring occupational health and safety practices of workers employees. The scale was adapted by Tuygun Toklu [11] from the studies of Christopher et al. [30] and Glendon and Litherland [31]. The validity and reliability analyses of the scale were also performed by Tuygun Toklu [11]. The scale consist of five dimensions: Safety Procedures and Risk Management (SPR-6 items), Safety and Health Rules (SHR-7 items), First-Aid Support and Training (FST-4 items), Occupational Hazards Prevention (OHP-7 items), and Organizational Safety Support (OSS-5 items) [11].
Socio-demographic characteristics of the participants
Descriptive statistical analyses and a structural equation modeling (SEM) analysis were performed within the scope of the data analysis. The analyses were performed within the 95% confidence interval.
The participants’ socio-demographic characteristics indicate that 70.6% are female, and 29.4% are male. The majority of employees are under the age of 23 and mean age is 29.72 (±7.89). 36.7% of the participants are nurses, and 63.3% are other auxiliary healthcare professionals. Because the hospital is a new one, 48% of the participants have been working in the hospital for≤2 years, while 52% for≥3 years. 6.8% of the participants work in polyclinics, 57.5% in clinics, 28.1% in support units, and 7.7% in diagnostic units. In terms of education level, 10.4% of the participants have a primary education degree, 51.6% a secondary education degree, and 38% a higher education degree. According to their statements, 93.7% of the participants have received OHS training before, and 11 have been exposed to occupational diseases. The participants’ statements show that 17.6% of them have experienced occupational accidents, 27.1% of them have experienced a near-miss accident, and 41.6% of them have witnessed a colleague’s involvement in an occupational accident.
Validity and reliability analyses of the scales were carried out within the scope of the present study. First, a confirmatory factor analysis was made. In the confirmatory phase, the convergent and discriminant validity of the scales constituting the proposed model was first evaluated. For convergent validity, it is expected that all factor loadings of the scales are over 0.703; the composite reliability (CR) is over 0.8 or Cronbach’s alpha value is over 0.65, and the average variance extracted (AVE) for each scale is over 0.5 [32, 33]. As shown in Table 2, the average variance extracted (AVE) for each construct in the model is in the range of 0.61–0.80; the composite reliability (CR) values are in the range of 0.90–0.95, and the Cronbach’s alpha values are in the range of 0.87–0.93. In addition, the factor loadings of the latent variables constituting the model vary between 0.72 and 0.96 (Fig. 2). For the discriminant validity of a model, the cross values that represent the AVE square roots of the latent variables are expected to be greater than the correlation values of the other latent variables in rows and columns [32]. In the model, the cross values representing AVE square roots were found to be greater than the correlation values of the other latent variables in rows and columns. This being the case, the model provides the necessary conditions for convergent and discriminant validity.
Reliability, average variance extracted, and composite reliability values of scales
Reliability, average variance extracted, and composite reliability values of scales
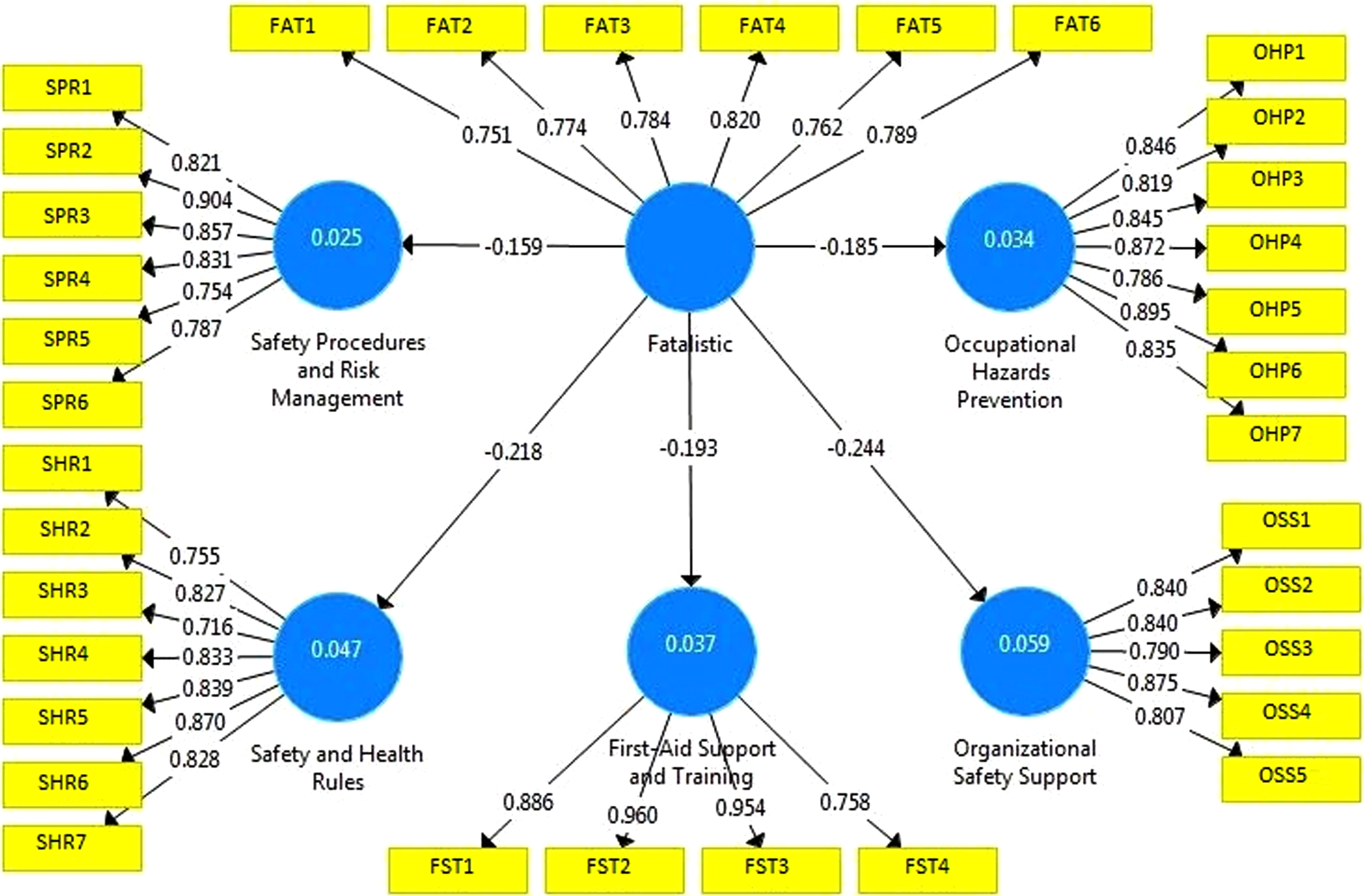
Model output: Note: SPR1-SPR6: Items of Safety Procedures and Risk Management sub-dimension; SHR1-SHR7: Items of Safety and Health Rules sub-dimension; FST1-FST4: Items of First-Aid Support and Training sub-dimension; OHP1-OHP7: Items of Occupational Hazards Prevention sub-dimension; OSS1-OSS5: Items of Organizational Safety Support sub-dimension; FAT1-FAT6: Items of Fatalistic Perception Scale.
As shown in Table 2, although the participants’ mean agreement levels regarding fatalistic perceptions are lower (2.32±1.13), their mean agreement values regarding attitudes and behaviors related to occupational health and safety practices vary in the range of 3.40±1.10–3.97±0.93. This is important in that it shows that healthcare professionals are more sensitive about occupational health and safety. In addition, the table shows the relationships between fatalism and OHS practices and the means of each scale. The results of the analysis indicate that there are negative relationships between the participants’ fatalistic perceptions and such OHS practices as SPR (r = –0.16), SHR (r = –0.22), OSS (r = –0.24), FST (r = –0.19), and OHP (r = –0.19). Accordingly, as the participants’ fatalistic perceptions increase, their attitudes and behaviors related to occupational health and safety practices decrease. Based on these findings, the hypothesis H1 (There is a relationship between employees’ fatalistic perceptions and their OHS practices) is accepted.
The findings obtained from the SEM analysis are shown in Fig. 2. The model shows that fatalistic perception has a negative and significant effect on SPR (β= –0.16, t = 2.04, p = 0.04], SHR (β= –0.22, t = 3.20, p = 0.00), FST (β= –0.19, t = 2.31, p = 0.02), OHP (β= –0.19, t = 2.41, p = 0.02), and OSS (β= –0.24, t = 3.59, p = 0.00]. This finding is important in that it shows that healthcare professionals’ fatalistic perceptions negatively affect their occupational health and safety practices. However, the β coefficients indicate that this effect remains weak. On the other hand, hypothesis H2 (Employees’ fatalistic perceptions affect their OHS practices) is accepted.
Healthcare professionals’ biggest disadvantages are spending most of their time in the hospital environment and the numerous risk factors in the workplace. The hospital environment includes people who come in as patients to treat their health problems, not healthy people. Thus, the hospital environment bears physical, chemical, social, and psychological risks for healthcare professionals. Occupational accidents and occupational diseases that may occur if OHS measures are not taken may cause negative events including those involving deaths. Hence, it is very important to identify and evaluate the risks to which health personnel is exposed.
The current study found that 93.7% of the participants have received OHS training. This result reveals that the hospital gives the necessary importance to occupational health and safety. However, those 6.3% who have not received training may pose a serious threat in terms of occupational accidents. Sanmiquel et al. [34] emphasized that occupational accident rates are high in organizations that give low importance to occupational health and safety practices. According to another study, most of occupational accidents are caused because of human mistakes [35]. For this reason, it is important to consider occupational health and safety measurements and provide adequate training in workplaces. The current study also found out that 17.6% of the participants have experienced occupational accidents, 27.1% of them have experienced a near-miss accident and 41.6% of them have witnessed a friend’s involvement in an occupational accident. The results show that the rate of occupational accidents experienced cannot be underestimated. Therefore, it is important that all employees should be trained on occupational health and safety practices in order to minimize occupational these risks.
The results of the study revealed that although the participants have low fatalistic perceptions. Workers do not leave their jobs to fate regarding occupational health and safety. Another study conducted during the Covid-19 pandemic period showed that the perception of fatalism of healthcare employees was low [36]. These findings support the current study. In this sense, health workers’ perceptions of occupational accidents related to fate are highly low. Another results of the study revealed that. The perceptions of the participants about OHS practice were moderate to high. Findings of this study are similar to the literature [37]. Current study’s result indicates that healthcare professionals have high good levels of OHS knowledge, and they give the necessary importance to occupational health and safety practices. Participation of employees on OHS is very important, as risks of OHS are quite high in the health sector [38]. For this reason, the perceptions of the OHS practices of healthcare professionals are considered very important. The results of this and the other studies in the literature are important in terms of showing that healthcare professionals do not leave the OHS issue to fate and are aware of the seriousness of the situation.
Another important research finding is an inverse relationship between fatalism and OSH practices. In addition, employees’ fatalistic perceptions negatively affected their SPR. Accordingly, as individuals’ perception of fatalism increases, they attach less importance to occupational health and safety procedures and risk management. Another variable that the perception of fatalism negatively affects is SHR. As the fatalism perception of the employees’ increases, the SHR compliance of the employees decreases. Similarly, the results of the study show that as the fatalism perception of the participants’ increases, the OHP decreases. These results show that employees’ commitment to occupational health and safety will reveal important occupational health and safety risks. According to another result of the study, the fatalism perceptions of the participants affect the FST and OSS negatively. According to Tuygun Toklu [11], FST in terms of improving the motivation of the participants and preparing an environment for the employees to show positive behavior in order to prevent occupational accidents and diseases; OSS, on the other hand, is an important component of OHSP in that it enables organizations with a good working climate to raise their employees’ potential to higher levels. The results of the study show that the increase in the fatalism perceptions of the employees causes them to give less importance to the training and support provided by the organization related to occupational health and safety. In this sense, the perception of fatalism threatens the organizational occupational health and safety climate. There are several studies that support these results of the study. there was an inverse relationship between fatalistic perceptions and safety training and safety priority, and that fatalistic perception has a negative effect on compliance with safety rules [25]. Similarly, a different study suggests that the fatalism perceptions of healthcare workers negatively affect their work accident prevention behavior; it has been found that as employees’ fatalism perception increases, they attach less importance to occupational health and safety practices [36]. The results of a study conducted in another sector also reveal the relationship between the perception of fatalism and security practices [39]. In comparison of our study with the discussed studies above, it can be said that the perception of fatalism has an important effect on occupational health and safety practices.
Conclusion and recommendations
This study was conducted to determine whether the fatalism perceptions of health professionals affect occupational health and safety practices and offers some suggestions for practice. The results of the current study showed that occupational accidents can occur frequently. Therefore, more strict measurements should be taken to prevent them. Another result of the study revealed that the fatalistic perception plays an important role in occupational health and safety practices, and it is recommended to emphasize through trainings given to employees that occupational accidents are not fate and to show that this problem can be prevented by certain measures they can take. It is considered even more important emphasize occupational health and safety in health institutions that serve human health. Because health employees are at risk of exposure to occupational infections with subsequent risk of contracting diseases, disability, and even death [40]. This is because the weaknesses in this area threaten not only the employees but also the patients. Therefore, OHS practices should be given more importance for the safety of employees and patients in all health institutions.
Limitations
The scales used in the study are self-reported. Participants are likely to be biased in self-assessment [41], which is an important limitation of the study. Another limitation of the study is that the study was conducted in a single private hospital. Therefore, the study can only be generalizable for the selected hospital.
Conflict of interest
None of the authors have any conflict of interest to report.
Ethical considerations
Ethical issues (including plagiarism, informed consent, misconduct, data fabrication and/or falsification, double publication and/or submission, redundancy, etc.) have been completely considered by the authors.
Funding
No financial support was received for this study.