
Abstract
BACKGROUND:
Musculoskeletal disorders cause a significant occupational problem for healthcare workers (HCWs).
OBJECTIVE:
This study aimed to measure the prevalence, associated occupational risk factors and coping strategies for work-related musculoskeletal disorders among HCWs working in five hospitals in Faisalabad, Pakistan.
METHODS:
A previously used validated questionnaire, which consisted of four sections, including demographic information, occupational health questions, and associated occupational risk factors and coping strategies, was used as a survey tool to collect data on health workers working in five hospitals located in the Faisalabad District.
RESULTS:
The finding of this study revealed that 7-day and 12-month prevalence rates of WMSDs were 1226 (83.45%) and 1107 (75.35%) respectively among HCWs and most common WMSDs was low back pain 576 (39.2%) followed by the neck 217 (15%) and ankles 186 (13%) according to body sites. The probability of developing WRMSDs was higher among physiotherapists (OR = 3.63, 95% CI: 1.39–9.51), participants with rank 18 (OR = 4.17, 95% CI: 2.18–7.96), and HCWs who work in primary care (OR = 8.94, 95% CI: 3.47–23.04). The most important risk factor reported was treating an excessive number of patients in one day (66.8%). The main coping strategies reported in this study were to get someone else to help in handling a heavy patient (90%).
CONCLUSIONS:
This study found that the most prevalent WMSD among HCWs was lower back pain. Sedentary lifestyle was shown to be a positive risk factor for acquiring WMSDs. Additionally, the primary risk factor discovered was treating an excessive number of patients, probably owing to a shortage of healthcare staff.
Introduction
The term musculoskeletal disorders (MSDs) refers to a collection of inflammatory and degenerative diseases that affect muscles, tendons, ligaments, joints, nerves, and associated blood vessels, causing pain or discomfort in some areas of the body or throughout the body [1]. MSDs are a major health and safety issue in both developing and industrialized countries [2]. It is reported that musculoskeletal disorders in certain industries and occupations are up to three or four times higher than the average across all sectors and are result of work-related disability in various occupations. Work-related musculoskeletal disorders (WRMSDs) are the leading cause of health-related absence among members of the European Union [3].
The evidence suggests that WMSDs are related to activities such as labor intensive tasks, exaggerated bending, prolonged awkward posture, excessive turning, manual handling and repetitive reaching [4, 5]. These movements are not particularly threatening in activities of daily life, however, repetition of a same task for longer duration makes it more hazardous. The factors such as force and speed of movement and the lack of recovery time between them are also known to contribute [6]. Workplace environments such as heat, cold and vibration also act as contributory factors for the development of WMSDs. WMSDs are considered accountable for the morbidity of many workers and are considered an important occupational problem with reduced productivity, rising healthcare costs, and severely compromised quality of life [7]. Health care work’s profession is included in high-risk job for the development of WMSDs. Studies have shown that nearly one-third of all cases of sick leave among health workers are related to WMSDs. The most commonly reported complaints to doctors, dentists and nurses are back, neck and shoulder pain [5, 8]. Ultimately, this can lead to a reduction in work commitments, a loss of working time and a change to another job, as well as a complete career change [4].
Healthcare workers suffer from WMSDs due to the limited number of staff and co-workers, resulting in an additional workload and minimal breaks in Pakistan [9, 10]. In addition, no mechanical load change facility, non-cooperative organizational environment, limited income resources, inadequate salary and no incentive also exhibit psychosocial stress in hospital staff. However, research on the musculoskeletal problems experienced by HCWs is sparse as per researcher’s knowledge. Therefore, this study was conducted to examine the prevalence of WMSDs and the various coping strategies used to overcome occupational risk factors among healthcare workers in various teaching hospitals in Pakistan’s Faisalabad District.
Material and methods
Participants recruitment
Participant ReHCWs including doctors, surgeons, physiotherapists, nurses, and laboratory technicians who worked in five randomly selected hospitals in Faisalabad, namely: (1) Allied Hospital, the largest tertiary care hospital in Faisalabad, (2) the District Headquarters Hospital (DHQ) located in Faisalabad, (3) Tehsil Headquarters Hospital (THQ) which is a secondary care hospital situated in Samundri, (4) General Hospital, which is a secondary care hospital sited in Samanabad, and (5) Independent University Hospital (IUH), which is a tertiary care hospital representing the privately owned hospitals located in Faisalabad.
HCWs of both genders, with at least one year of experience in tertiary care hospital and those were present during the survey time were included. HCWs with current musculoskeletal trauma or congenital musculoskeletal disorders, working in the teaching departments, retired, who were not parting clinical work and those who refused to participate were excluded. Moreover, HCWs except doctors, surgeons, physiotherapists, nurses, and laboratory technicians were also excluded from this study.
Data collection
A previously used validated questionnaire was used, which consisted of different sections, including demographic information (name, age, gender, weight, height, BMI, job title, marital status, hand dominance and experience), section 2; Nordic Musculoskeletal Questionnaire (NMQ), and section 3; on occupational risk factors which identified ‘0-1’ as no problem, ‘2–7’ as a minimal to moderate problem and ‘8–10’ indicated that the job factor was considered a major problem, and section 4; coping strategies as a survey tool to collect data on health workers working in five hospitals located in the Faisalabad District. To determine the prevalence of work-related musculoskeletal pain, among HCWs screening was carried out by the two researchers using the NMQ [11]. The NMQ is frequently used to determine musculoskeletal symptoms in nine major body regions, including the neck, shoulder, upper back, elbows, wrists / hands, lower back, hips / thighs, knees, and ankles / feet [12]. HCWs selected by a simple random technique from selected hospitals were interviewed by two researchers and asked to fill out a written questionnaire. During data collection, only HCWs who were on duty were interviewed. The Institutional Review Committee of Riphah International University approved this study. Data collection approval was granted by the Chief Executive Officer of District Health Authority Faisalabad and Medical Superintendent of IUH Faisalabad, and all participants provided written informed consent.
Data analysis
The data were entered and analysed using the Statistical Package for the Social Sciences (SPSS), version 21.0 (SPSS Inc., Chicago, IL, USA). Quantitative data, including height, weight, BMI, and experience of the participants, were measured in terms of means and standard deviations. The risk was assessed using the odds ratio and the 95% confidence interval. A univariate analysis was performed to determine the predictors for WMSDs. P-values equal to or less than 0.05 were used to indicate statistical significance.
Results
A total of 1,750 survey forms were disseminated to HCWs in the selected hospitals, of which 1570 were returned, corresponding to a response rate of 89.7%. 101 of the returned survey forms were excluded due to inadequate information. In this study, out of 1469 HCWs, 310 physicians, 298 surgeons, 119 physical therapists, 480 nurses and 262 technicians participated. The mean height in inches was 65.66±6.38, the weight in kg was 69.16±13.07, the BMI was 25.20±5.44 and the experience with the HCW was 5.53±3.280. The period prevalence of WRMDs among HCWs was 1226 (83.45%). Low back pain was most commonly reported in 559, with 321 (40%) men and 238 (36%) women. The point prevalence was 1107 (75.35%), out of which LBP was most common with prevalence of 521 with 288 (36%) males and 233 (35%) females (Tables 1–3).
Descriptive information of all respondents to questionnaire (N: 1469)
Descriptive information of all respondents to questionnaire (N: 1469)
7-days (point prevalence) among HCWs
12-months (period prevalence) among HCWs
The univariate analysis showed that the probability of having WRMSDs was significantly higher among HCWs with sedentary lifestyles (OR = 1.932, 95% CI: 1.482–0.2.517). The probability of having WRMSDs was significantly lower among HCWs in the age group 20–23 years (OR = .477, 95% CI: 0.267–0.852) and HCWs in the age group less than 19 years (OR = 0.422, 95% CI: 0.222–0.801). The probability of having WRMSDs was significantly lower among nurses (OR = 0.56, 95% CI: 0.37–0.84) and surgeons (OR = 0.49, 95% CI: 0.32–0.76) and was higher in physical therapists (OR = 3.63, 95% CI: 1.39–9.51). The probability of having WRMSDs was significantly higher among HCWs of rank 18 participants (OR = 4.17, 95% CI: 2.18–7.96). The probability of having WRMSDs was significantly higher among HCWs working in primary care (OR = 8.94, 95% CI: 3.47–23.04). The probability of having WRMSDs was significantly lower among HCWs in participants having experience 5-6 years (OR = 0.177, 95% CI: 0.095–0.331), in participants having experience 1-2 years (OR = 0.424, 95% CI: 0.230–0.781). Gender, job titles, hand dominance, work status, working hours, working posture and smoking were non-significant factors in having WRMSDs in the past 12 months (Table 3).
Univariate analysis of possible risk factors for work-related musculoskeletal disorders (WRMSD) in the past 12 months among study (n = 1468) care workers (HCWs)
*p < 0.05, **p < 0.01, ***p < 0.001.
In this study, 17 conditions and tasks at work that could contribute to job-related problems. A score of 0 to 1 was equivalent to a job factor being “no problem,” a score of 2 to 7 was rated as a “minimal to moderate problem,” and a score of 8 to 10 indicated that a job factor was considered a “major problem.” The Majority of the study participants considered the factor “Unanticipated sudden movement or fall by patient” as no pain-causing factor. A vast majority of the HCWs, 66% considered factors “Performing the same task over and over” and “Working near or at your physical limits” as minimal to moderate pain-causing factors (Fig. 1). In terms of coping techniques used by participants to mitigate the risk of developing WRMSDs, over 93 percent of participants sought assistance while handling heavy things at work (Fig. 2).
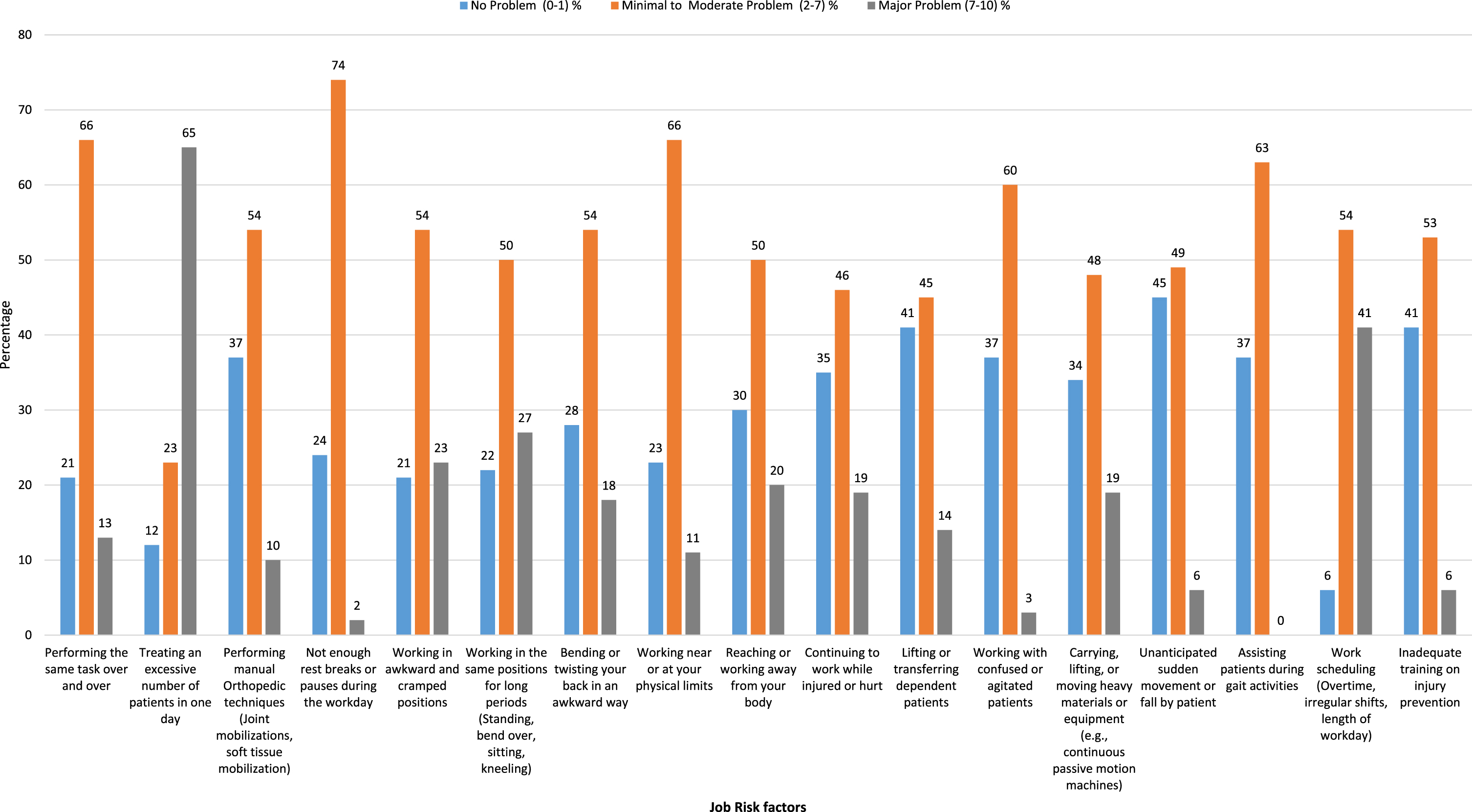
Percentage indicating respondents’ perceptions of job risk factors.
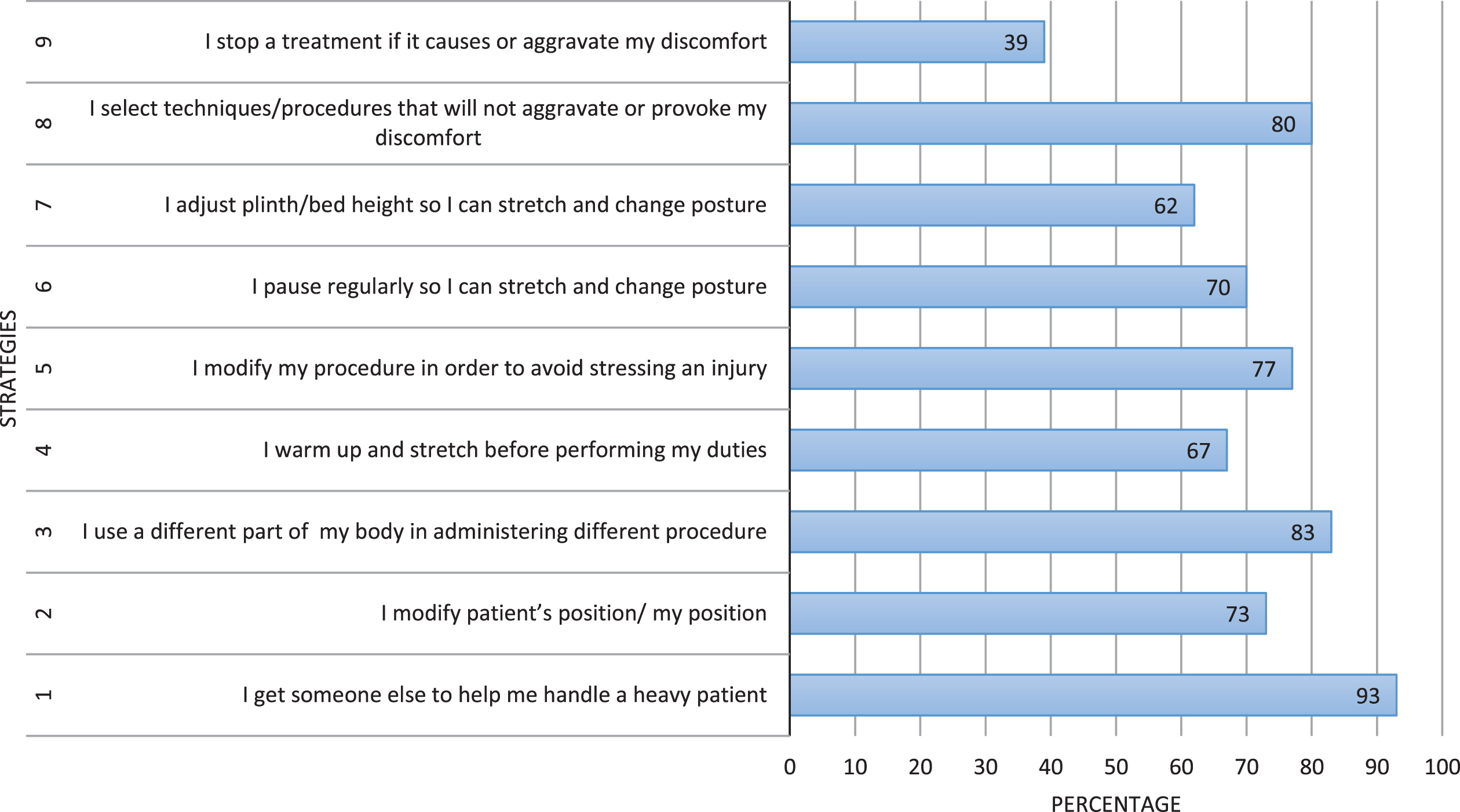
Coping strategies to reduce the risk for development of WRMSDs.
Health hazards in the workplace are widespread in almost all areas of the work environment and are steadily increasing. Musculoskeletal disorders are connected to the musculoskeletal system, which significantly affect occupational health [13].
The current study was conducted to report the prevalence, associated occupational risk factors, and coping strategies for WRMSDs among HCWs working in five hospitals in Faisalabad, Pakistan. The present study reported 32% of the most common WMSDs in the lower back, followed by 15% in the neck and 13% in the ankles, depending on the region of the body. Similarly, one study found that the lower back was 88.2%, followed by the neck at 76.5% and the shoulder at 60.3% in HCWs [14]. In the areas of musculoskeletal injuries during work, the highest incidence is found in the lower back. Biomechanical studies have shown that physical stress factors such as flexion, rotation and weight loading play a role [15]. Flexion and rotation of the trunk and lifting at work are moderate risk factors for low back pain, especially at greater levels of exposure. The degree of trunk flexion appeared to be a risk factor for low back pain. Extreme trunk flexion led to an increased risk of low back pain when the trunk is in a minimum of 60° of flexion for more than 5% of the working time. The weight of a load also appeared to be a risk factor for low back pain. Lifting 25 kg or more increased the risk of low back pain when this occurred more than 15 times per working day, and a slight increase in risk was observed with a further increase in the frequency of lifting [16].
The present study reported an overall 1-year prevalence of WMSDs among HCWs working in district Faisalabad of 83.45% while a study conducted in Saudi Arabia reported the prevalence to be 73.9% with 95% CI [17]. It is highly recommended to report the 1-year prevalence as this reduces the recall bias of the participants, highlights the severity level of the pathology, and identifies what needs to be addressed on priority basis. Few other studies have come out with similar results depicting higher prevalence as study conducted among nurses gave the figure of 72% [18], results of research carried out in Turkey informed the prevalence to be 53% among HCWs [19] while in the same region, among the nursing population the prevalence was found to be 77.1% [20], more than 72% physical therapists and 63% physicians reported having WMSDs [20].
The current study reported that the low back area was the most commonly reported painful region as 43% of the physicians, 38% of the surgeons, 47% of the physical therapists, 35% of nurses, and 40% of the technicians suffered from low back pain in the last year. This pattern of distribution is consistent with the literature findings [21]. The second most commonly affected body part was wrist/hand in physicians, ankles in surgeons and nurses, neck in physical therapists and shoulder region among technicians. The neck region was the third most painful site for the physicians, for the surgeons it was the knee region, among the physical therapists the knee region was the third most commonly affected body part while ankle and neck regions were involved among nurses and technicians, respectively. This is mostly in line with the results already available that report the knee region to be commonly affected among 19.8% physicians followed by the low back region. However, the frequency of the complaints seems to be quite low [22]. A systematic review reported the prevalence among the surgeons to be 73% to 88%. The wide variability might be due to low response rates by the respondents and inconsistent methodologies [23]. On the other hand, literature has reported that neck and knee regions are commonly affected among this population [24–26].
This study found that sedentary life is associated with WRMDS. One study reported that regular exercise and physical activity was linked to a lower risk of musculoskeletal pain in the working population [27]. The findings of this study reported that physiotherapists were at more risk of MSDs as compared to other health workers. The incidence of WRMSDs reported by Neeti in physiotherapists in various anatomical locations was low back (35%), neck (25%), shoulders and upper back (15%) and wrist / hands (5%) [28]. According to the literature, the work-related activities that most commonly cause WRMSDs among healthcare professionals are manual therapy practices, which involve transferring and lifting patients, maintaining posture for a long period of time and responding to sudden and repetitive movements by the patient [15, 29–32]. A systematic review examined the association between sedentary lifestyle and LBP using a comprehensive definition of sedentary behaviour including prolonged sitting both at work and during leisure time. In this review, one high-quality cohort study reported a positive association, between LBP and sitting at work only; all other studies reported no significant associations. According to the study, there was limited evidence to demonstrate that sedentary behaviour alone is a risk factor for developing LBP. Sedentary behaviour at home and during leisure time coupled with work-related activities and occupationally demanding tasks are more significant contributor of low back pain [33]. Being physically active during leisure time is associated with a decreased risk of upper-body occupational repetitive strain injuries, adding another potential health benefit to participation in leisure-time physical activity [34].
Working in the same position for long periods, working in awkward or cramped positions and handling an excessive number of patients or samples in one day were found to be the most commonly reported job risk factors that contributed to the development of WMSDs among healthcare professionals. In this study, about half (50.7%) of the participants reported symptoms in at least one part of their bodies, over the past 12 months. Among all the symptoms, low back pain was the highest (45.7%), followed by neck pain (28.5%) and shoulder pain (23.5%), whereas hip/thigh pain (7.1%) and elbow pain (5%) were the least reported. Irrespective of regions, body pain during the last 12 months was complained by 56% of nurses, 55% of physiotherapists, 54% of dentists, 39% of lab technicians and 38% of physicians. Overall, musculoskeletal pain complained by all participants was 50.7%, and among that, 26.4% was found to be of work-related origin. Work-related pain was found to be high in nurses, dentists, and physiotherapists, whereas non-work-related pain was found to be predominant in physicians and lab technicians [35].
A systematic analysis of literature determined prevalence and risk factors for WMSDs in AHP. A 1-year prevalence rate of between 28% and 96% indicates AHPs are at high risk of developing a WMSD. The lower back was the most commonly affected body part. Factors identified were predominately physical in nature and included working in awkward positions, working in the same position, bending or twisting, transferring patients, lifting, performing tasks monotonously, performing repetitive tasks, a high number of patients, and a lack of rest breaks. Relevant factors identified with the development of WMSDs included inexperience in the role and area of employment. High risk factors associated with the development of a WMSD include being a younger therapist, having fewer years of experience, and being exposed to higher levels of manual and repetitive tasks [36].
The majority of the study participants considered the factor “Unanticipated sudden movement or fall by patient” as no pain-causing factor. A vast majority of the HCWs 66% (974), considered factors “Performing the same task over and over” and “Working near or at your physical limits” as minimal to moderate pain-causing factors, while a major problem-causing factor was considered to be “Treating an excessive number of patients in one day” by 65% of the enrolled personnel. A study conducted among nurses mentioned the high working demands to be an important factor responsible for causing musculoskeletal complaints [18]. Most commonly reported causative factors among nursing population came out to be the lifting of patients in the bed or from the floor, such activities create excessive stressors on body biomechanics [37]. Similarly, back trauma, long working hours and physical demands imposed by the job are also mentioned to be responsible [38, 39].
In this study, the most common coping strategies to avoid musculoskeletal discomfort were getting someone else to help in handling a heavy patient, followed by using a different part of the body in administering different procedures, and selecting techniques/procedures that will not aggravate or provoke any discomfort. Literature has reported similar strategies used by HCWs to deal with physical demands. These strategies have been known to be used due to repetitive nature of the job demands that are established factors for causing WMSDs [40, 41].
Conclusion
This study found that the highest prevalence of WMSDs was the lower back pain among HCWs. In addition, the main risk factor identified was the treatment of too many patients, possibly due to a lack of healthcare workers. In the meantime, the most commonly used coping strategy for overcoming risk factors of WMSDs was to get someone else to help treat a heavy patient. The probability of developing WRMSDs was higher among physiotherapists working in Faisalabad City.
Limitations
This study was not without limitations. Because the study was limited to a single location, the findings cannot be generalised. A larger sample size, including other cities, may be necessary to provide more comprehensive findings. This study did not investigate all risk variables and made no clinical evaluation of discomfort. Since this study focused only on active duty HCWs, individuals who quit work owing to MSDs or other reasons were excluded from the analysis, as were the quantitative interactions between demographic, occupational, and psychosocial characteristics.
Funding
None to declare.
Conflict of interest
The authors declare no conflict of interest.
Footnotes
Acknowledgments
The authors thank the Chief Executive Officer of the District Health Authority for permission to collect data from HCWs working in hospitals in the Faisalabad District, Pakistan.