
Abstract
BACKGROUND:
Musculoskeletal disorders are prevalent among physiotherapists. They perform many repetitive tasks in awkward postures that require a high muscle load. This issue was often addressed through subjective analysis (questionnaire) but rarely using postural evaluation combined with an ergonomic assessment.
OBJECTIVE:
The aim of this article was to decompose draining lymphatic massage performed by physiotherapists in generic postures (GP) to quickly assess the musculoskeletal disorder risk.
METHODS:
Based on numeric video recorded in frontal and sagittal planes, 3360 postures were defined from 20-minutes lymphatic drainage massage performed by 7 physiotherapists over a period of 6 months. A hierarchical cluster analysis was applied to define the GP.
RESULTS:
Seven GP were identified, which were described by their average joint angles, variability and relative frequency. GP6, GP4 and GP2 had the highest frequencies (17.6%, 16.9% and 16.8% respectively). Trunk and neck were essentially flexed (neck: 17.0±10.0° for GP1; trunk: 20.4±8.7° for GP4). Shoulder flexion and abduction ranged from 15° (GP7) to 60° (GP4). Mean and variability of RULA score completed the analysis. The highest scores were computed for GP2 and GP3 (respectively 5.5±1.3 and 5.8±1.2, p < 0.05). GP4 had the lowest (4.0±1.1, p < 0.05). The results suggest that massages have to be monitored. Attention should be paid to the postures used to prevent the occurrence of MSDs.
CONCLUSION:
The massages could be described as a combination of generic posture for a rapid ergonomic assessment.
Introduction
Physiotherapists (P) and Physical Therapists (PT) are exposed to musculoskeletal disorders (MSDs) during their work. Numerous works have reported that these work-related musculoskeletal disorders (WMSDs) are the result of repetitive task, labour intensive and performed in awkward postures for long periods of time [1–3]. The overall prevalence of WMSDs among physiotherapists has been evaluated to be over 80% [4, 5]. Many studies have investigated the prevalence, characteristics and causes of WMSDs mainly through subjective analysis. First, researchers investigated the prevalence of body parts associated with WMSDs. Albert et al. [6] and Chung et al. [2] reported that the body areas with significant prevalence were the lower back (65.3% and 53.5% respectively) and shoulders (62.2% and 45.2% respectively). Other studies have focused on the risk factors responsible for the appearance of MSDs [5, 8]. Holder et al. [1] and Al-Eisa et al. [9] also investigated factors that exacerbated symptoms associated with these WMSDs. Among the criteria highlighted, some refer directly to uncomfortable postures such as “bending or twisting forward”, “working in awkward/cramped position” or “working at/or near physical limits”. Finally, some authors have analysed how WMSDs altered the work habits [1, 10] and responses to reduce their effects [1, 5].
The information reported through these different criteria highlighted that the adopted postures were directly related to the presence of MSDs. However, in these studies, no joint data were measured. These subjective studies could be completed by quantitative data on posture to better understand the MSDs and the feelings mentioned in the previous studies. Kang et al. [11] quantified kinematics of the lumbar, pelvis, and hips in physical therapists to prevent chronic low back pain. Albert et al. [12] studied neck, trunk, and shoulder flexion during massage activities. In this work, the authors studied the time spent in different joint sectors defined for these 3 joints (i.e. neutral, mild and severe). This approach is interesting because it shows the evolution of the posture over time. However, these different works reported biomechanical data relative to certain parts of the skeleton. These works did not propose a global evaluation of the working postures in the different planes. A complete analysis of the posture enables to identify the joints at risk and to use ergonomic indicators to quantify the MSD risk associated with the posture adopted. The Rapid Upper Limb Assessment (RULA) [13] is one of the most widely used ergonomic tools in occupational activities [14]. It indicates through a score the risk of MSDs related to a posture.
In this framework, the aim of this work was to quantify the postures adopted by physiotherapists during a massage activity and to assess the risk of MSDs using the RULA. The underlying hypothesis was that there would be generic postures (GP) that would be repeated and could be used to more simply describe long-duration complex activities.
Methods
Task
The task was to perform a 20-minute lymphatic drainage massage of an upper or lower limb using 20 mmHg pressure with hands. Fourteen massage performed by 7 physiotherapists were analyzed. The subject characteristics were presented in Table 1. All physiotherapists came from the neurology department of the Léon Bérard hospital. The massage analysis was carried out on the basis of the availability of the physiotherapists in the department according to their schedule and the admissions of the patients in the hospital.
Characteristics of the physiotherapist population
Characteristics of the physiotherapist population
The physiotherapists’ postures were recorded by two numeric cameras (Samsung galaxy S20) fixed at 90° to each other in order to capture movements in the frontal and sagittal planes. From the video recordings, two experts defined the postures (measurements of joint angles) adopted by the physiotherapists every 5 seconds, i.e. 3360 postures, using Dartfish application to quickly measure the angles in each plane. The data were then integrated into a model developed in Matlab (Mathworks Inc., Natick, MA, USA) to verify the measured posture by comparing to the observed one. Each posture was determined by ten joint angles relative to neck, trunk, shoulders, elbows, hips and knees flexion/extension and abduction/adduction or inclination following the International Society of Biomechanics recommendations [15, 16]. Flexions/extensions correspond to movements in the sagittal plane around the mediolateral axis. Abduction and tilting correspond to movements in the frontal plane around the anteroposterior axis of the body. The different segmental rotations were defined by presence (1) or absence (0). These data were used to perform the RULA analysis of each posture. The RULA technique is used to obtain a score from the joint values and correspondence tables for the upper and lower limbs of each posture. This score indicates the level of risk for MSDs: 1-2 acceptable, no action required; 3-4 low risk, change may be needed; 5-6 medium risk, further investigation and change soon; 6+ very high risk, implement change now [13].
In order to describe the adopted posture during massage, a hierarchical cluster analysis (HCA) was applied using Statistica software (Statistica 7.1, Statsoft, Tulsa, OK, USA). The ten joint angles defining each of the 3360 measured postures were used as input data. The software automatically matched the postures based on distances between joint angles using Ward’s linkage method [17] and delivered a dendrogram. The identification of the clusters was quantitatively determined by the agglomeration coefficient and this decision was verified by a visual inspection of the dendrogram. Each cluster represents a Generic Posture (GP). Each GP was defined by the ten mean joint angles with standard deviation. Two complementary parameters were used to qualify each identified GP: the ergonomic risk level of MSD occurrence calculated by the RULA [13] and the time spent in each GP in relation to the total massage duration (frequency of use). Mean joint angles and RULA scores computed for each GP were compared using Kruskal Wallis test. The level of significance was set to 5%.
Results
The hierarchical cluster analysis identified seven GP from all measured joint angles (Fig. 1, coefficient set at 40% of the data variance). Each GP was defined by mean values and standard deviation of 10 joints angles. Data were completed with use rate (frequency in %) and RULA ergonomic score. Table 2 summarizes all these data.
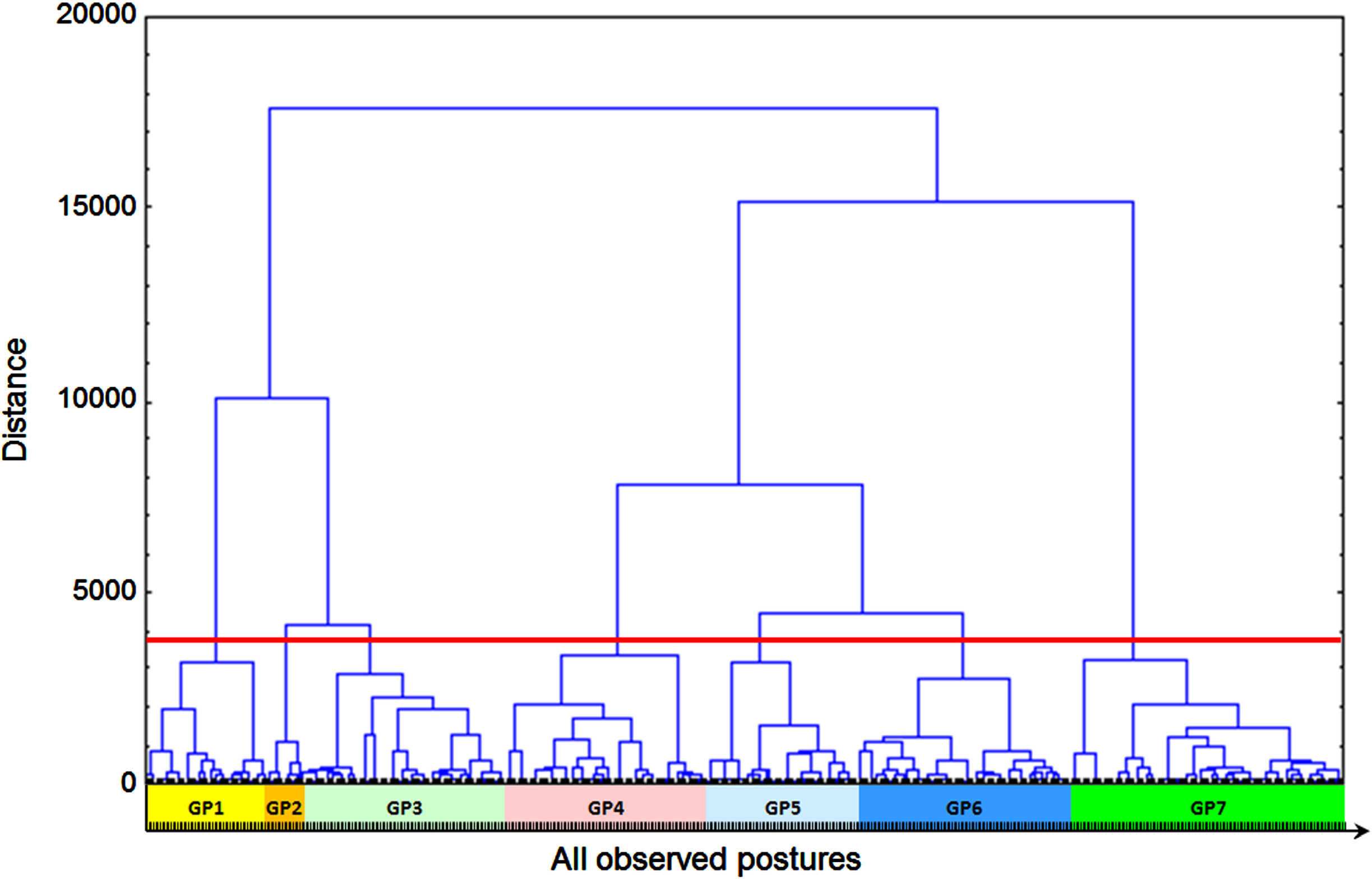
Ward’s minimum variance linkage dendrogram of the hierarchical cluster analysis of observed postures during massage representing the seven-cluster solution. The seven groups are highlighted by color rectangles.
Frequency, mean joint angles and mean RULA score (STD) of each generic posture (GP)







*RULA scores take into account the presence of rotations at the head, trunk, shoulder, and forearm joints. The two grey lines represent complementary parameters.
Ergonomic analysis highlighted that all GP had a RULA score greater than 4, indicating at least a moderate risk of MSD occurrence with a requirement to monitor activity [13]. The GP with the lowest risk of MSDs were GP4 and GP6 (RULA score of 4.3±1.3 and 4.0±1.1 respectively, p < 0.05, Table 2). The GP with the highest risk were GP2 and GP3 with RULA scores of 5.5±1.3 and 5.8±1.2 respectively (p < 0.05). The latter were characterized by high shoulder flexion (64.7±16.4° for GP2 and 50.3±28.3° for GP3) and low elbow flexion (36.0±20.1° for GP2 and 34.5±25.9° for GP3), both of which contribute to an increased risk of MSDs. Trunk flexion also contributed to this high risk with flexion (14.5±8.1° for GP2 and 16.8±7.7° for GP3) as well as neck flexion, that was more pronounced for GP3. For all the GP, some joints should be monitored because they may present risky values such as trunk flexion greater than 15° for GP1 to GP5, trunk inclination for all the GP except GP4, and neck flexion for GP1 and GP3. GP4 and GP6 have suitable angular values, although shoulder flexion needs to be checked.
The 7 GP identified allow to describe in a simplified way all the postures used during a massage (i.e. 240 postures per massage or 3360 in total). Table 3 illustrates the composition of each massage by specifying the rate of use (frequency in %) of each GP as well as the RULA ergonomic analysis. The latter was carried out in two parts: the first based on RULA scores computed by posture for each GP; the second based on average RULA scores for each GP to estimate the risk of MSDs on the basisof GP.
Frequency and mean RULA score of generic postures observed for each massage
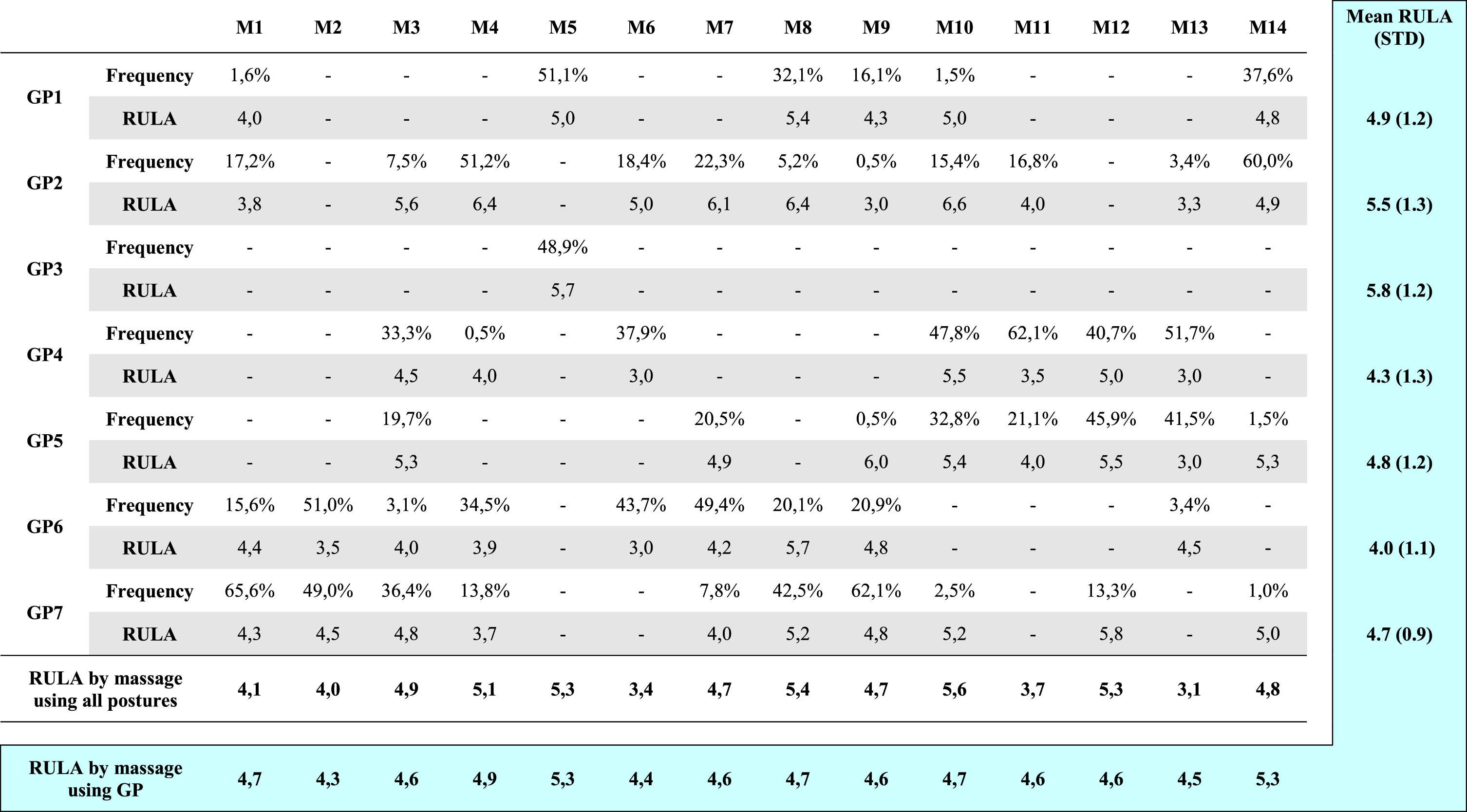
*M = massage; GP = Generic Posture; RULA = Rapid Upper Limb Assessment [13]. The grey values represent the mean RULA scores obtained from all the postures of each GP for each massage. In the blue part, the mean RULA scores of each GP are presented vertically (all massage combined) and the RULA score of each massage obtained from the average RULA scores of the GP are presented horizontally.
For the first part of the analysis, the overall RULA scores for each massage ranged from 3.1 (M13) to 5.6 (M10). M13 was defined by the presence of GP4, GP5, and GP6. These GP were associated with the lowest RULA scores. On the contrary, M10 was composed mainly of GP1, GP2, and GP5, which were associated with high RULA scores. This explains the high RULA score (5.6) for this massage. For the second part of the analysis (Table 3 in blue), the overall RULA were higher than 4 for all massages (4.3 for M2 to 5.3 for M5 and M14).
On the 14 massages studied, the data set could be summarized as follows: GP1 was observed in 6 of 14 massages, percentage of time spent ranging from 1.6 to 51.1% of the total massage duration with RULA score of 4.9 (±1.2); (> 4: medium risk, further investigation and change soon); GP2 was observed in 11 of 14 massages, percentage of time spent ranging from 0.5 to 60% of the total massage duration with RULA score of 5.5 (±1.3); (> 4: medium risk, further investigation and change soon); GP3 was observed in 1 of 14 massages, percentage of time spent of 48.9% of the total massage duration with RULA score of 5.8 (±1.2); (> 4: medium risk, further investigation and change soon); GP4 was observed in 7 of 14 massages, percentage of time spent ranging from 0.5 to 62.1% of the total massage duration with RULA score of 4.3 (±1.3); (> 4: medium risk, further investigation and change soon); GP5 was observed in 8 of 14 massages, percentage of time spent ranging from 0.5 to 45.9% of the total massage duration with RULA score of 4.8 (±1.2); (> 4: medium risk, further investigation and change soon); (> 4: medium risk, further investigation and change soon); GP6 was observed in 9 of 14 massages, percentage of time spent ranging from 3.1 to 51.0% of the total massage duration with RULA score of 4.0 (±1.1); (> 4: medium risk, further investigation and change soon); GP7 was observed in 10 of 14 massages, percentage of time spent ranging from 1.0 to 65.6% of the total massage duration with RULA score of 4.7 (±0.9); (> 4: medium risk, further investigation and change soon).
An important variability was observed for the percentage of time spent in each GP relative to total massage time and for RULA scores. The use of GP mean RULA scores to characterize each massage reduced the variability.
The aim of this work was to determine whether the lymphatic drainage massage performed by physiotherapists could be decomposed into GP. A hierarchical cluster analysis was applied on the 3360 postures extracted from 14 massages of 20 minutes performed by 7 different physiotherapists. Seven GP were evidenced on the base of an agglomeration coefficient of 40%. This coefficient was set to obtain the best compromise between the number of GP and the percentage of variance explained. The objective was to describe simply the massage throughout GP. Each GP was defined by ten mean joint angles. The risk level of MSD occurrence (RULA score) and the use rate of each GP were considered to enhance the GP study.
Ergonomic RULA scores provided an objective quantification of the MSD risk for each massage (Table 3). Each massage was composed of several GP. The RULA scores computed for each massage ranged from 4.3 to 5.3 using the GP mean RULA scores. These values were smoothed out compared to those obtained from all the postures (RULA score between 3.1 and 5.6). The latter presented a postural variability during the massages performed by the physiotherapists. However, the estimation of MSD risk using GP remains acceptable for the rapid assessment of MSDs. To our knowledge, no such classification has been proposed for healthcare professionals. According to the RULA interpretation grid, these results suggest that massage is medium risk activity (score of 4+). In addition, massage activities are among the manual therapies that are frequently reported as MSD risk factors [18, 19]. As shown by the presence of GP, lymphatic drainage is an activity that involves the repetition of movements with the application of force. It has been widely shown that repetition and force are two biomechanical parameters involved in the development of MSDs [20]. Massage is therefore an activity that should be monitored and for which changes should be made to the work environment and the postures adopted by physiotherapists to reduce their exposure to MSDs.
The assessment of the work-related musculoskeletal disorders using ergonomic tools has already been widely proposed in the literature [14, 21]. However, MSDs in physiotherapists was most often carried out through subjective cross-sectional survey, addressing various problems such as discomfort, pain or prevalence of MSDs by body part area [1, 22]. It is interesting to note that some of the MSD risk factors reported by physiotherapists correspond to items in ergonomic tools such as RULA. These include “performing the same task over and over” [2, 4], and “working in a same/awkward/cramped position for a long time” [7, 23]. Furthermore, the subjective identification of affected body part areas [7, 9] and the posture assessment in the RULA are complementary. Indeed, they make it possible to link the origins and consequences of the MSD appearance. GP introduced in this work is one way to describe accurately lymphatic drainage massage. In other words, they allow a quantified schematic description of a massage, i.e. a combination of GP for which the angular (joint angles) and ergonomic (RULA score) characteristics are known. The results showed that all the GP have a RULA value greater than 4. Two GP (GP2 and GP3) had values greater than 5 (5.5±1.3 and 5.8±1.2 respectively). The lowest value was obtained for GP6 (4.0±1.1). Although the latter is the least likely to be at risk, GP6 is classified in level 2 according to the RULA classification remains a posture to be monitored.
Considering the joint values (Table 2), the different GP would lead to the development of MSDs in specific joint, i.e. neck flexion for GP1, shoulder and elbow flexion for GP2, neck, shoulder and elbow flexion for GP3, trunk flexion and shoulder flexion/abduction for GP4, trunk flexion and shoulder abduction for GP5, shoulder flexion/abduction for GP6, trunk flexion and inclination for GP7. These results are in agreement with studies dealing with WMSD prevalence by body part. Cromie et al. [24], Albert et al. [6], Chung et al. [2] and Khairy et al. [5] reported that the neck, lower back and shoulder were the areas most affected byWMSDs.
Since GP would constitute the elementary postures and have be qualified with an averaged RULA score with its standard deviation, a rapid MSD evaluation can be conducted for a massage performed by a new physiotherapist. Moreover, some recommendations could be addressed regarding the postures adopted by physiotherapists during massages in order to reduce the risk of MSDs. For example, in our sample, GP2 and GP3 (RULA scores of 5.5±1.3 and 5.8±1.2) should be avoided to perform massage. Furthermore, it was observed that the most experienced physiotherapists preferred to use GP with lower ergonomic scores, i.e. GP4 and GP6.
Some limitations could be addressed to this work. First, hierarchical cluster analysis identified seven GP. Each of them was defined by mean joint angles and RULA score. Due to the large number of postures included, each GP showed a variability of joint angles around these averages. As a result, two postures belonging to the same GP can have a different RULA score, and therefore a different level of risk. Future work could investigate the effect of RULA values on postures at the boundaries of the GP variability domain. This would allow a more accurate analysis of the risk of MSDs in massage activities. The experience and health status of the physiotherapists were not taken into account in this study. As shown in Table 3, not all massages are performed in the same way, i.e. with different combinations of GP. It might be interesting to consider these aspects in future work.
Conclusion
The present work showed that a 20-minute lymphatic massage can be decomposed into a limited number of GP. These GP are characterized by a mean value and standard deviation of joint angles and an ergonomic RULA score. As a result, a massage can now be defined a few number of GP and their percentage of occurrence over the total duration. From these data, MSD risk level could be assessed. The most experienced physiotherapists used GP with moderate RULA scores, i.e. GP4 and GP6. This result could be reinforced with a larger massage sample. It was also found that when massages were repeated, the physiotherapists did not always reproduce the same GP sequence. The repetition of the acts over time is also an aspect that could be further investigated.
Footnotes
Acknowledgments
The authors thank the director of the Léon Bérard Hospital and the physiotherapist team: Christine, Maria, Karine, Edith, Claudia, Emeline, and Clothilde. This study also received partial financial and technical support from ErBio-Connect and Léon Bérard Hospital.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
None to report.
Informed consent
All subjects were informed of the entire protocol and gave their consent.
Ethical approval
The experimental protocol was approved by the local ethics committees of the Léon Bérard Hospital and the University of Toulon.