
Abstract
OBJECTIVE:
To evaluate the diagnostic value of ultrasonography and mammography for plasma cell mastitis.
METHODS:
The ultrasonographic and mammographic images of 111 women with histopathologically confirmed plasma cell mastitis were retrospectively analyzed. The diagnostic accuracy of the two imaging methods was compared.
RESULTS:
Ultrasonography identified 91 out of 111 (82.0%) patients with plasma cell mastitis, while the other twenty (18.0%) patients were misdiagnosed. Mammography identified 83 (74.8%) out of 111 patients with plasma cell mastitis. Nineteen (17.1%) patients were misdiagnosed. There was no significant difference between the diagnostic accuracy of using two imaging tests (P = 0.127). Mammography clouds identified 11 out of 20 patients who were not diagnosed by ultrasonography. Meanwhile, 19 of the 28 cases misdiagnosed with mammography were correctly identified by ultrasonography. Overall, 91.9% (102/111) of the patients were identified by the combination of ultrasonography and mammography, which yielded statistically significant higher accuracy than using each single test only (P < 0.05).
CONCLUSIONS:
In diagnosis of plasma cell mastitis, high-frequency ultrasonography and mammography should be combined to improve the diagnostic accuracy.
Introduction
Plasma cell mastitis (PCM) is a rare disease of the breast that usually occurs in middle-aged women at nonpregnancy or nonlactation stages [1, 2]. The etiology of PCM remains unclear, but may be due to many factors, such as congenital nipple malformation or dysplasia, mammary gland impairment, inflammation, endocrine disorders, mammary gland degeneration, and autoimmune disorders [2, 3]. PCM is a nonbacterial inflammatory breast disease that develops when epithelial cell debris and secretion are overly accumulated in the obstructed mammary duct, causing ductal ectasia and a periductal phlogistic reaction characterized by a large amount of plasma cell infiltration [4–6].
Preoperative diagnosis of PCM is very difficult. The main clinical manifestations, including acute or chronic breast pain, mass, nipple discharge, nipple deformation, etc., are not specific [7–9]. Moreover, some patients have no obvious symptoms. Hence, PCM is difficult to identify from breast carcinoma, intraductal papilloma and other breast inflammatory diseases [10, 11]. Although CT perfusion imaging and MR perfusion imaging can be used to exclude breast carcinoma, it is too expensive and time consuming to be a routine examination for the diagnosis of breast diseases [12, 13]. Ultrasonography and mammography are the first choice for breast diseases because these methods are simple, safe and inexpensive [14–17]. Ultrasonographic and mammographic images of PCM have been widely studied [18, 19]. However, few publications specifically compare the diagnostic accuracy of ultrasonography and mammography for PCM.
In the present study, the ultrasonographic and mammographic images of 111 women with histopathologically confirmed PCM were retrospectively analyzed. The image features and diagnostic accuracy of the two imaging methods were compared to evaluate the diagnostic value of ultrasonography and mammography for PCM.
Patients and methods
This study was approved and supervised by the ethics committee of the First Hospital of Chongqing Medical University. In all, 111 women aged 15–71 years with histopathologically confirmed PCM who were treated from January 2008 to May 2017 were included in this study. All patients underwent ultrasonographic and mammographic examination followed by surgical excision and pathological examination.
Ultrasonography was performed by using a Toshiba 790A (Tokyo, Japan) equipped with a variable frequency probe possessing a frequency of 5 mHz in the central area. The patients were in the supine position, and scanning was performed in both radial and antiradial directions starting from the nipple. The lesions were characterized according to location, amount, size in diameter, shape, margin, echogenicity and sound attenuation. The vascularity in and around the lesions was further evaluated by using the same equipment, and the peak systolic velocity (PSV), end diastolic velocity (EDV) and resistance index (RI) for each lesion were recorded. The bilateral axillary lymph nodes were also evaluated. The examinations were conducted by radiologists with more than 5 years of experience in breast ultrasonography. The ultrasonographic images were evaluated by the operating doctor and another doctor who also had more than 5 years of experience in breast imaging. If any disagreement occurred, a senior doctor with more than 10 years of experience in breast ultrasonography was consulted.
Mammography was performed using a dedicated breast unit (Senographe DMR, General Electrics, USA). Craniocaudal and mediolateral oblique projections of the breast were observed routinely. Features of breast lesions were evaluated, including location, amount, size, margins, shape, density, microcalcifications and bilateral axillary lymph nodes. The mammographic images were evaluated following the same process as that of ultrasonographic image reading.
Statistical analysis was performed with the SPSS 19.0 statistical software package (SPSS Inc, Chicago, IL, USA). A one-way analysis of variance test was used to compare the ratios of the Breast Imaging Reporting and Data System (BI-RADS) categories among the sonographic, mammographic and combined methods. P < 0.05 was considered statistically significant.
Results
The patients were aged between 15 and 61 years (median, 30.9), and the majority (92/111, 82%) of them were of reproductive age. No patient had a family history of breast cancer. Patients’ complaints varied between mass, mastalgia, nipple retraction, discharge, skin sinus, and skin resembling orange peel. A palpable mass was present in all patients except one who presented with pruritus of the breast. Seventy-two (64.9%) patients had mastalgia, 30 (27.0%) patients had nipple retraction, and 9 (8.1%) patients had discharge. The remaining clinical symptoms were skin sinus in 7 (6.3%) patients and skin resembling an orange peel in 1 (0.9%) patient. Meanwhile, axillary lymph adenopathy was found in 65 (58.6%) patients by clinical examination.
As seen in Table 1, one hundred (90.1%) patients had identifiable lesions, nine (8.1%) had tubular extensions, and two (1.8%) had ambiguous lesions with disorganized glands. Five of the 100 patients had multiple lesions, and only the largest lesions were recorded and analyzed. Six of the one hundred lesions were too large to be accurately measured, and the other 94 lesions ranged from 0.5 to 9.0 cm (median, 3.1 cm). Fifty-eight percent (58/100) of the lesions locate in the subareolar area. The majority (67/100) of the lesions were solid masses, 22 lesions were cystic-solid masses, and only 11 lesions were cystic. Sixty-six patients had ill-demarcated lesions. Prominent posterior acoustic shadowing was observed in 9 patients, while weakened posterior acoustic shadowing was observed in 13 patients. In 105 patients, only 3 calcifications and 17 mammary duct ectasia were observed. Fifty-seven patients (51.4%) had markedly axillary enlarged lymph nodes. Color Doppler blood flow signals were detected in 82 patients, and increased vascularization was evident in 51 of the 82 lesions. The hemodynamic parameters in color Doppler flow images were measured. The PSV ranged from 6.4 to 59.8 cm/s (median, 23.3), EDV ranged from 2.3 to 21.8 cm/s (median, 8.5), and RI ranged from 0.5 to 0.9 cm/s (median, 0.7).
Ultrasonographic findings of 111 patients with plasma cell mastitis
Ultrasonographic findings of 111 patients with plasma cell mastitis
The mammographic findings are shown in Table 2. Distinct lesions were observed on mammograms in 105 of 111 patients; 67 (63.8%) lesions were located in the subareolar area, 20 (19.1%) in the lateral upper quadrant, 6 (5.7%) in the lateral lower quadrant, 5 (4.8%) in the inner upper quadrant, and 7 (6.7%) in the inner lower quadrant. The mammographic manifestations of lesions varied. Poorly defined borders were observed in 80 of 105 patients. Lesions with irregular forms were noted most frequently (92/105). Twenty-three pathological calcifications were observed, including 14 macrocalcifications and 9 microcalcifications. In the remaining 6 patients, mammography showed no obvious localized breast lesions; 4 patients had mammary gland structure abnormalities, and 2 patients were normal. Forty-seven patients (42.3%) had markedly axillary enlarged lymph nodes.
Mammographic findings of 111 patients with plasma cell mastitis
The ultrasonographic and mammographic diagnoses of the 111 patients with PCM are shown in Table 3. Ultrasonography identified 91 out of 111 (82.0%) patients with PCM, while the other twenty (18.0%) patients were misdiagnosed, including 2 patients with mammary duct ectasia, 6 with galactoma, 7 with breast carcinoma, 2 with mastopathy, 1 with abscess, 1 with intraductal papilloma, and 1 with mammary fibroadenoma. Mammography identified 83 (74.8%) out of 111 patients with PCM. Nineteen (17.1%) cases were misdiagnosed as breast carcinoma, 3 (2.7%) as fibroadenoma, 2 (1.8%) as cyclomastopathy, 2 (1.8%) as galactoma, 1 as galactocele, and 1 as abscess. Mammography clouds identified 11 out of 20 patients who were not diagnosed by ultrasonography. Meanwhile, 19 of the 28 cases misdiagnosed by mammography were correctly identified by ultrasonography. Overall, 102 out of the 111 patients were identified by the combination of ultrasonography and mammography, but 9 patients were still misdiagnosed. The accuracy rate and misdiagnosis rate of ultrasonography and mammography are shown in Table 4. In addition, the ultrasonographic and mammographic images of a 35-year-old patient are shown and compared in Fig. 1.
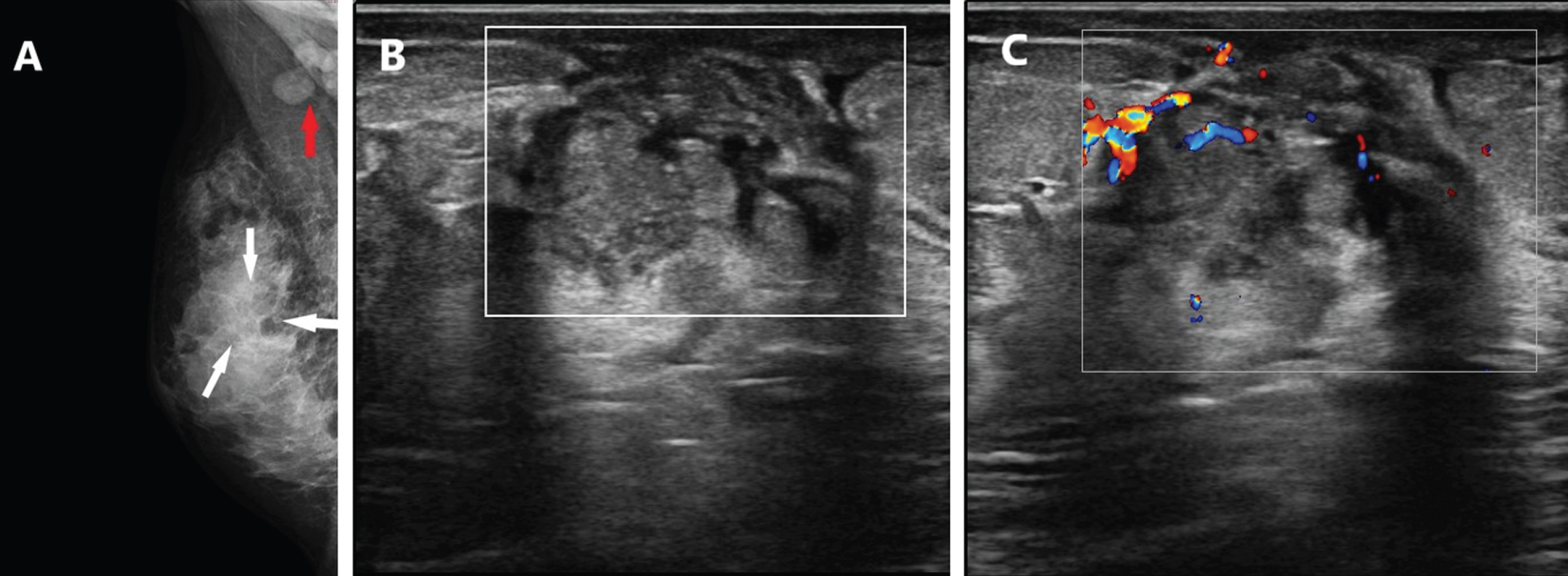
A 35-year-old patient presented with a mass in her right breast. A, Mammography showed no obvious localized breast lesion, but the density of the mammary gland parenchyma in the central region was patchy increased, and the mammary gland structure was abnormal (white arrow), accompanied by markedly enlarged ipsilateral axillary lymph nodes (red arrow). B, Ultrasound showed a cystic-solid lesion (white rectangle) that was mainly hypoechoic with small patchy anechoic areas. C, Color Doppler blood flow signals were detected, and increased vascularization was evident in and around the hypoechoic region.
The ultrasonographic and mammographic diagnosis of the 111 patients with plasma cell mastitis
Accuracy rate and misdiagnosis rate of ultrasonography and mammography in the 111 patients with plasma cell mastitis
aCompared with Ultrasonography, F = 1.7, p = 0.127; bcompared with Ultrasonography, F = 4.8, p = 0.022; ccompared with Mammography, F = 11.7, p = 0.001.
At present, due to their advantages of economy, convenience and noninvasiveness, high-frequency ultrasonography and mammography examinations have become the initial assessments of young females with palpable breast lesions [14–17]. The imaging mechanisms of high-frequency ultrasonography and mammography are very different, and the tissue structures of the lesions in the image are different. High-frequency ultrasonography can clearly display the anatomical structure of the breast, showing the skin, fat, glands and lesions layer by layer and identifying breast duct and cystic structures. It can be used to dynamically observe the expanded catheter and the characteristics of retention substances. Color Doppler ultrasound can display the blood flow distribution of the lesion and axillary lymph nodes and calculate the hemodynamic parameters. Mammography can sensitively display the type and size of calcification foci in the lesion, especially microcalcification, which might be easily overlooked by ultrasonography [20, 21].
In recent years, the imaging performance of high-frequency ultrasonography and mammography for PCM has been widely studied [18, 19]. The ultrasonographic and mammographic images of PCM are very complicated and are closely related to the disease course and pathological changes that occur. In the acute phase, the breast ducts expand due to secretion blockage, mammographic features are abnormal expansion of the breast duct, and thick secretions can form ductal slaggy or earthworm dense shadows. Ultrasonographic images often show simple catheter dilatation, fine echogenicity can be seen in the lumen, and lumen content flow can be seen under pressure. As the disease progresses, the ducts are further dilated due to their thickened wall, and a mass is formed with the secretions in the duct and the granulation tissue surrounding the duct. Mammographic signs are often characterized by limited infiltrating-type lesions that are ill-defined cystic or mixed cystic-solid lesions in the ultrasonographic images. During the chronic phase, PCM lesions often present as nodular masses with dense mass shadows in mammography, solid masses with enhanced echo of peripheral tissues and no echo of the capsule in high-frequency ultrasonography. Guo diagnosed 25 out of 30 patients (83.3%) with PCM by using ultrasonography and 17 out of 30 patients (56.7%) by using mammography [20]. According to Xu et al., the diagnostic compliance rates of ultrasonography for the diagnosis of PCM varied with the pathological type and were 79.7% for ductal dilatation types, 72.7% for cyst types, 93.1% for abscess types and 79.4% for solid mass types [21]. Zhu et al found that the sensitivity, specificity and accuracy rate of conventional ultrasound in differentiating PCM were 78.21%, 64.71% and 75.59%, respectively [22]. Zhang Mei et al. reported that the sensitivity, specificity and accuracy rate of mammography in differentiating PCM were 51.9%, 61.5% and 55.9%, respectively [23]. Among the 111 cases in this study, the diagnostic accuracy of high-frequency ultrasonography was 82.0% and that of mammography was 74.8%, which was consistent with the literature.
PCM is difficult to diagnose by relying solely on high-frequency ultrasonography or mammography because of the complex pathophysiological changes and clinical manifestations of PCM [18, 19]. In this study, the diagnostic accuracy of high-frequency ultrasonography and mammography was 82.0% and 74.8%, respectively, and there were no significant differences between the two methods (P = 0.127). Ultrasonography can be used to dynamically observe the breast and detect the blood supply of lesions without radiation, but it is difficult to display the fine structure due to its poor resolution, and the diagnostic accuracy is greatly affected by the professional expertise and experience of the ultrasound physician. Mammography can be used to provide clinicians with objective images of the breast and lesions and has more advantages in the detection of calcification foci than ultrasound, but masses in dense glands are easy to miss by mammography [24–26].
However, the combined diagnostic accuracy of high-frequency ultrasonography and mammography was 91.9%, which was statistically significant when compared with each single test (P < 0.05). The combination of high-frequency ultrasonography and mammography could make up for the deficiencies in each method, thereby providing clinicians with more information about lesions and helping them to more accurately diagnose PCM. Therefore, to improve the accuracy of diagnosing PCM, high-frequency ultrasonography and mammography should be combined.