
Abstract
BACKGROUND:
Preoperative prediction of cervical lymph node metastasis (CLNM) in patients with papillary thyroid carcinoma (PTC) is significant for surgical decision-making.
OBJECTIVE:
This study aims to develop a dual-modal radiomics (DMR) model based on grayscale ultrasound (GSUS) and dual-energy computed tomography (DECT) for non-invasive CLNM in PTC.
METHODS:
In this study, 348 patients with pathologically confirmed PTC at Jiangsu University Affiliated People’s Hospital who completed preoperative ultrasound (US) and DECT examinations were enrolled and randomly assigned to training (n = 261) and test (n = 87) cohorts. The enrolled patients were divided into two groups based on pathology findings namely, CLNM (n = 179) and CLNM-Free (n = 169). Radiomics features were extracted from GSUS images (464 features) and DECT images (960 features), respectively. Pearson correlation coefficient (PCC) and the least absolute shrinkage and selection operator (LASSO) regression with 10-fold cross-validation were then used to select CLNM-related features. Based on the selected features, GSUS, DECT, and GSUS combined DECT radiomics models were constructed by using a Support Vector Machine (SVM) classifier.
RESULTS:
Three predictive models based on GSUS, DECT, and a combination of GSUS and DECT, yielded performance of areas under the curve (AUC) = 0.700 [95% confidence interval (CI), 0.662–0.706], 0.721 [95% CI, 0.683–0.727], and 0.760 [95% CI, 0.728–0.762] in the training dataset, and AUC = 0.643 [95% CI, 0.582–0.734], 0.680 [95% CI, 0.623–0.772], and 0.744 [95% CI, 0.686–0.784] in the test dataset, respectively. It shows that the predictive model combined GSUS and DECT outperforms both models using GSUS and DECT only.
CONCLUSIONS:
The newly developed combined radiomics model could more accurately predict CLNM in PTC patients and aid in better surgical planning.
Keywords
Introduction
Thyroid carcinoma (TC) has been on the rise in recent years, making it the most frequent malignant endocrine tumor in the world [1]. PTC is the most common pathologic type of thyroid cancer, accounting for 80 to 90% of all cases [2]. The majority of PTC are low-grade malignant tumors with a slow progression and a favorable prognosis. Some PTCs demonstrate aggressive behavior and recurrence with extrathyroidal extension (ETE) and CLNM [3–6]. Although the death rate of PTC remains low, CLNM usually occurs when the early characteristics of thyroid cancer nodules are not obvious, and 30–80% of PTC patients may have CLNM [7, 8]. Predicting CLNM using imaging modalities prior to PTC surgery is critical for surgical method selection.
Several imaging modalities including US, CT, MRI, PET, and scintigraphy are all traditional imaging modalities for the diagnosis of thyroid nodules [9]. Due to its excellent superficial resolution and real-time dynamic exploration of the internal structure and adjacent regions of the lesion without radiation, high frequency US examination is the first line commonly used imaging modality for assessing PTC and CLNM. However, some diagnostic limitations in the US examination of PTC CLNM are unavoidable. US diagnosis relies heavily on the operator’s experience and subjective judgment. On the other hand, the sensitivity of US in detecting CLNM needs to be improved, and 20–80% of clinically negative PTC patients have microscopic lymph node metastasis [10, 11]. Besides, significant acoustic shadowing is generated by normal anatomic structures, such as larynx, trachea, areas deep in the clavicles, jaw and sternum [12]. This limited US detection of the mediastinum and retropharyngeal area, which seriously affects the accuracy of diagnosis.
In comparison to the US, CT is a standardized, objective imaging technique that is less reliant on the operator. The American Thyroid Association (ATA) statement on preoperative imaging for TC surgery emphasizes that contrast CT can be used to fully evaluate lymph node lesions when physical examination and/or US suggest that lymph node metastasis of volume or extent cannot be fully evaluated by US. In addition, the Chinese Society of Clinical Oncology (CSCO) pointed out in the ‘Guidelines for the Diagnosis and Treatment of Persistent/Recurrent and Metastatic Differentiated Thyroid Cancer (2018 Edition)’ that when local lesions are suspected, Neck US, enhanced CT or MRI are also recommended as Level I-2A, the highest recommendation level [13]. Furthermore, DECT is superior to traditional single-energy computed tomography (SECT), which can reduce radiation dose compared to SECT while maintaining excellent image quality [14]. Multiple metastases are common when PTC metastasizes through lymphatic vessels to lymph nodes in the neck, due to the number of lymphatic vessels and lymph nodes in the head and neck. On imaging, it is difficult to detect all metastatic lymph nodes [15]. Radiomics is a new technology that can extract hundreds of quantitative features from medical images and combine them into a radiomics signature, which is an image-based biomarker that can be used to build a radiomics model to identify diseases. Although ultrasound radiomics (USR) and DECT radiomics have been used to predict CLNM in order to perform noninvasive assessments prior to surgery [16–18], there is no literature on the preoperative evaluation of CLNM in PTC using GSUS combined with DECT radiomics, so the purpose of this study is to develop a joint predictive model incorporating radiomics features of GSUS combined with DECT for preoperatively predicting PTC with CLNM, not just central or lateral lymph node metastases.
Materials and methods
Patients
The Jiangsu University Affiliated People’s Hospital’s local ethics committee approved this retrospective study, and the informed consent requirement was waived due to its retrospective nature. Between January 2021 and February 2022, 348 patients of our hospital (269 female, mean age, 47.57±11.65 [range, 18–76] years) and 79 male, mean age, 45.32±10.96 [range, 27–75] years) who underwent US examination and DECT scanning of the neck region before thyroidectomy were retrospectively selected. Figures 1 and 2 show the working procedure.
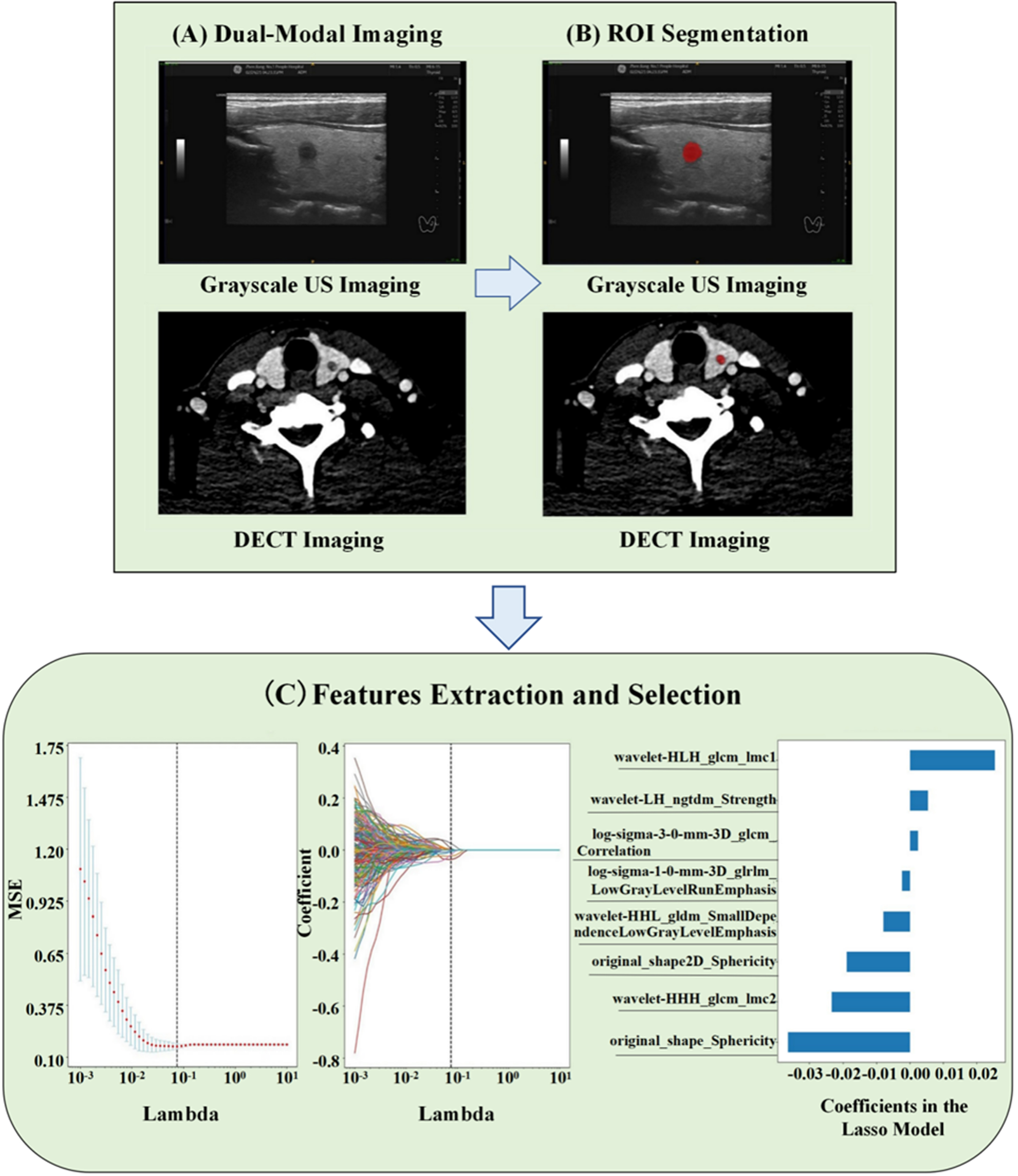
Radiomics workflow for the CLNM prediction in patients with PTC based on dual-modal imaging. US, ultrasound; DECT, dual-energy computed tomography; ROI, region of interest, CLNM, cervical lymph node metastasis; PTC, papillary thyroid carcinoma.

Study flowchart of radiomics modeling for the CLNM prediction in PTC. US, ultrasound; DECT, dual-Energy computed tomography; CLNM, cervical lymph node metastasis; PTC, papillary thyroid carcinoma.
The inclusion criteria were detailed as follows: (1) >18 years old; (2) having thyroid US within one month before surgery, with relevant US image data, and a preoperative PTC basic diagnosis; (3) undergoing preoperative DECT scanning of the neck region within a week, with complete nodule characteristics; (4) and the PTC diagnosis conformed by the postoperative pathology.
Exclusion criteria included: (1) accepting relevant therapies of the neck; (2) the maximum diameter of the primary lesion was <3 mm; (3) incomplete available data of US, DECT, and pathology results; (4) images of US and DECT were not unequivocally identifiable; (5) patients with a history of neck carcinoma except PTC (i.e., nasopharyngeal carcinoma, pharyngeal carcinoma, and neck squamous cell carcinoma).
In summary, the enrolled patients were divided into the CLNM-Free group (n = 169) and the CLNM group (n = 179) based on postoperative pathologic results. The clinical information of patients, such as age, gender, characteristics of US and DECT were also collected.
The enrolled patients had a routine US examination performed by experienced US radiologists using a Philips iU22, Philips Q5 (both Healthcare, Eindhoven, the Netherlands) or a LOGIQ E9, GE LOGIQ s8, LOGIQ E20 (GE Medical Systems, American General) US system with a 5–12 MHz linear array transducer. Then, the machine was operated using a specialized ‘Thyroid’ program.
The patients were positioned supine, with the pillow removed and the head slightly tilted. The neck was thus exposed to the greatest extent possible, and a US examination of the thyroid and neck area was performed using longitudinal and transverse continuous scanning. The main US characteristics included tumor diameter (maximum long axis of the primary lesion), tumor border (clear, less clear, fuzzy), tumor shape (irregular, oval, circle), tumor vascularization (without, rare, abundant), internal echo pattern (uniform, owe uniform, nonuniform), tumor location (left lobe, isthmus, right lobe), tumor position (upper pole, middle pole, inferior pole), multifocality (singleness, multifocality), bilateral (unilateral, bilateral), Aspect Ratio (height divided by width on transverse views, A/T), calcification (no calcification, microcalcification, macrocalcification), elastic classification (0 points: tumor tissue color-coded red, 1 point: between red and green,2 points: uniform green tumor; 3 points: tumor mainly between green and blue-green; 4 points: tumor mainly between blue-green and blue; 5 points: homogeneous blue tumor) were observed.
DECT Examination
The patients were subjected to dual-energy scanning for the venous phase. Imaging acquisition of PTC patients was undergone by using a third generation DECT scanner (Somatom Force; Siemens Healthcare). The range of DECT scans were from the bottom of the skull to the upper margin of the aortic arch. The technician encouraged the patients to hold their breath during eupnea prior to the horizontal scan in the recumbent position. Identical acquisition protocol as follows: detector configuration, 192×0.6 mm; gantry rotation, 0.25 s; pitch factor, 0.6; field of view, 150×150 mm. Tube A was operated at a peak voltage of 80kVp and a reference tube current of 118mAs. Tube B was used at Sn150kVp and a reference tube current of 59mAs. For contrast-enhanced scanning, 80 mL of an iodinated non-ionic contrast agent (Iohexol,300 mg/dL iodine, Yangzijiang Pharmaceutical Company or Iodixanol, 320 mg/dL iodine, Yangzijiang Pharmaceutical Company) was injected through cubital vein at a flow rate of 3.5 mL/s using an automated high-pressure syringe. The scan delay times for the venous phases were the 50 s. The achieved venous phase CT images under voltage of 80kVp were reconstructed to 1 mm layer thickness and exported in DICOM format for further analysis. Some characteristics of DECT observed included lesion shape (regular, irregular), edge of lesions after enhancement (clear, blurred), thyroid contour (continuity, interruption), marginal contact range (MCR, non-contact, <1/4, 1/4-1/2, >1/2), calcification (no calcification, microcalcification, macrocalcification), cystic degeneration (negative, positive).
Region of Interest (ROI) Segmentation
Two blinded radiologists with 10 and 15 years of experience in thyroid radiological imaging independently interpreted all GSUS images and manually determined the ROI by delineating the margin of thyroid carcinoma using ITK-SNAP software (https://www.itksnap.org), focusing on the solid part of the carcinoma and avoiding cystic, hemorrhagic, and necrotic areas.
The tumor regions in the DECT images of 80kVp were delineated by two radiologists with 8 years and 13 years of experience in neck diseases. To ensure clear images, the layer with the most axial lesions was chosen as the ROI. ROI was placed in the largest solid part of the tumor as far as possible to avoid cystic degeneration, necrosis, or calcification, and no adjacent blood vessels were involved. The two radiologists need to reach a consensus on the selection of slices and the marking of the ROI. If their selections differ, they need to discuss and resolve the discrepancies. If the two radiologists cannot reach a consensus, a third expert can be asked to decide. Any objections to the segmentation were resolved by consensus.
Radiomics feature extraction
Total 1424 radiomics features (GSUS: 464 radiomics features, DECT: 960 radiomics features) were extracted from these ROIs on dual-modal medical image data using PyRadiomics (version 2.2.0, https://github.com/Radiomics/pyradiomics). These features included first-order features, shape features, grey-level run length matrix (GLRLM) features, grey-level size zone matrix (GLSZM) features, grey-level dependence matrix (GLDM) features, neighborhood grey-tone dependency matrix (NGTDM) features, grey-level co-occurrence matrix (GLCM) features, and features derived from wavelet filter images containing first-order GLCM, GLRLM, GLSZM, GLDM, and NGTDM features.
Features reproducibility evaluation and selection
Intraclass correlation coefficients (ICC) were used to evaluate the agreement and robustness of extracted features from the different ROIs in the same images between two observers. The reproducibility of radiomics features were evaluated by computing ICC prior to feature selection. An ICC value greater than 0.8 was believed to reflect good consistency. Because the ideal characterization condition frequently means the smallest prediction error, feature selection as an important aspect for pattern classification plays an important role in the processing of high-dimensional radiomics information. In this study, PCC was utilized in the training group to reduce redundant and irrelevant features, and LASSO algorithm with 10-fold cross-validation was used for features selection.
Radiomics model construction and validation
Three predictive models were built in this study: (1) First, the SVM classifier was utilized to create a GSUS radiomics model and a DECT radiomics predictive model utilizing only the selected features. (2) By integrating the GSUS and DECT radiomics features, a new feature set was formed. SVM with kernel = ’linear’ was used to generate a radiomics model based on the combination of GSUS and DECT radiomics features. In the training and test cohorts, the performance of the joint model in predicting CLNM was examined and validated using receiver operating characteristic curve (ROC) analysis. The AUC, sensitivity (SEN), specificity (SPE), accuracy (ACC), positive predictive value (PPV) and negative predictive value (NPV) were computed. Decision curve analysis (DCA) is applied to determine the clinical usefulness of radiomics models by counting the net benefit of different thresholds in joint training and validation groups [19–21].
Statistical analysis
Statistical analyses were processed using Python software (version 3.7) and SPSS 25.0 software (SPSS, Inc., Chicago, IL). Pearson’s chi-square or Fisher’s exact test was used to compare differences for categorical characteristics. The independent sample t-test was calculated for continuous factors with normal distribution, whereas the Mann-Whitney U test was used for continuous factors without normal distribution. A two-sided P < 0.05 demonstrated statistically significant differences. To evaluate the best predictive models, AUCs in the ROC analysis were calculated.
Results
Clinical characteristics
A total of 348 PTC patients, including 269 women (mean age, 47.57±11.65 [range, 18–76] years) and 79 men (mean age, 45.32±10.96 [range, 27–75] years) were enrolled in this study. All patients were randomly divided into either the training group (n = 261) or the test group (n = 87) adopting a stratified sampling method, and the CLNM and CLNM-Free groups were randomly divided at 3:1, respectively. A comparison of the clinical data and dual-modal imaging characteristics of the 348 patients between the training and test groups is shown in Table 1. There was no significant difference between the two groups in clinical-pathological information and dual-radiological image characteristics (all P > 0.05) besides tumor diameter (p = 0.029) and US elastic classification (p = 0.03).
Clinical data and dual-modal imaging characteristics of patients with papillary thyroid carcinoma in the training and test cohorts
Clinical data and dual-modal imaging characteristics of patients with papillary thyroid carcinoma in the training and test cohorts
The relation between the CLMN and dual-modal imaging characteristics is shown in Table 2. 179 (51.4%) patients developed CLNM, and 169 (48.6%) patients had free-CLNM. There were significant differences in the gender, tumor diameter, multifocality, bilateral, (GSUS) tumor shape, (GSUS) tumor border, (GSUS) internal echo pattern, (GSUS) calcification, (GSUS) aspect radio, (GSUS) tumor vascularization, (DECT) tumor shape, (DECT) thyroid contour, (DECT) MCR, (DECT) cystic degeneration.
Relationship between the cervical lymph node metastasis and dual-modal imaging characteristics through visual assessment of papillary thyroid carcinoma
Based on the training cohort, extracted features were reduced to 10, 7 and 8 potential predictors in GSUS, DECT and GSUS combined DECT respectively, using the PCC and LASSO regression with 10-fold cross-validation (Fig. 3).

Dual-modal radiomics features selection using the least absolute shrinkage and selection operator (LASSO) logistic regression model in the training cohort.The 10-fold cross-validation and the minimal criteria process generated the optimal penalization coefficient lambda in the LASSO model and LASSO coefficient profiles of dual-modal radiomics features. (a) The selected process of GSUS radiomics features; (b) The selected process of DECT radiomics features; (c)The selected process of dual-modal joint radiomics features.
GSUS decision function is given as follows.
S G = 0.018329×original_firstorder_Kurtosis
-0.052421×original_shape2D_Sphericity
+0.003840×original_glcm_Contrast
-0.003237×wavelet-LH_firstorder_Minimum
+0.005974×wavelet-LH_glcm_Imc2
-0.022181×wavelet-LH_glcm_InverseVariance
+0.010663×wavelet-LH_glszm_LargeAreaEmphasis
+0.004850×wavelet-LH_ngtdm_Strength
+0.027259×wavelet-HL_glszm_ZoneEntropy
+0.016326×wavelet-HH_ngtdm_Busyness
+0.4980842911877396.
DECT decision function is given as follows.
S D = 0.001452×log-sigma-3-0-mm-3D_glcm_Correlation
-0.035197×original_shape_Sphericity
-0.003807×log-sigma-1-0-mm-3D_glrlm_LowGrayLevelRunEmphasis
+0.025072×wavelet-HLH_glcm_Imc1
-0.007081×wavelet-HHL_gldm_SmallDependenceLowGrayLevelEmphasis
-0.025946×wavelet-HHH_glcm_Imc2
+0.000198×wavelet-HHH_glszm_ZoneEntropy
+0.49808429118773945.
DECT + GSUS decision function is given as follows.
SD+G= 0.002407×log-sigma-3-0-mm-3D_glcm_Correlation
-0.036400×original_shape_Sphericity
-0.002365×log-sigma-1-0-mm-3D_glrlm_LowGrayLevelRunEmphasis
+0.025443×wavelet-HLH_glcm_Imc1
-0.007943×wavelet-HHL_gldm_SmallDependenceLowGrayLevelEmphasis
-0.023442×wavelet-HHH_glcm_Imc2
-0.018951×original_shape2D_Sphericity
+0.005373×wavelet-LH_ngtdm_Strength
+0.4980842911877395.
On the training cohort containing 261 patients, the classifier correctly classified 94 (true positive) out of 142 without CLNM, and correctly classified 83 (true negative) out of 119 patients having CLNM (Fig. 4A). In the test cohort containing 87 patients, the dual-modal prediction model correctly classified 37 (true positive) out of 54 patients with no CLNM, and correctly classified 21 (true negative) out of 33 patients having CLNM (Fig. 4B).
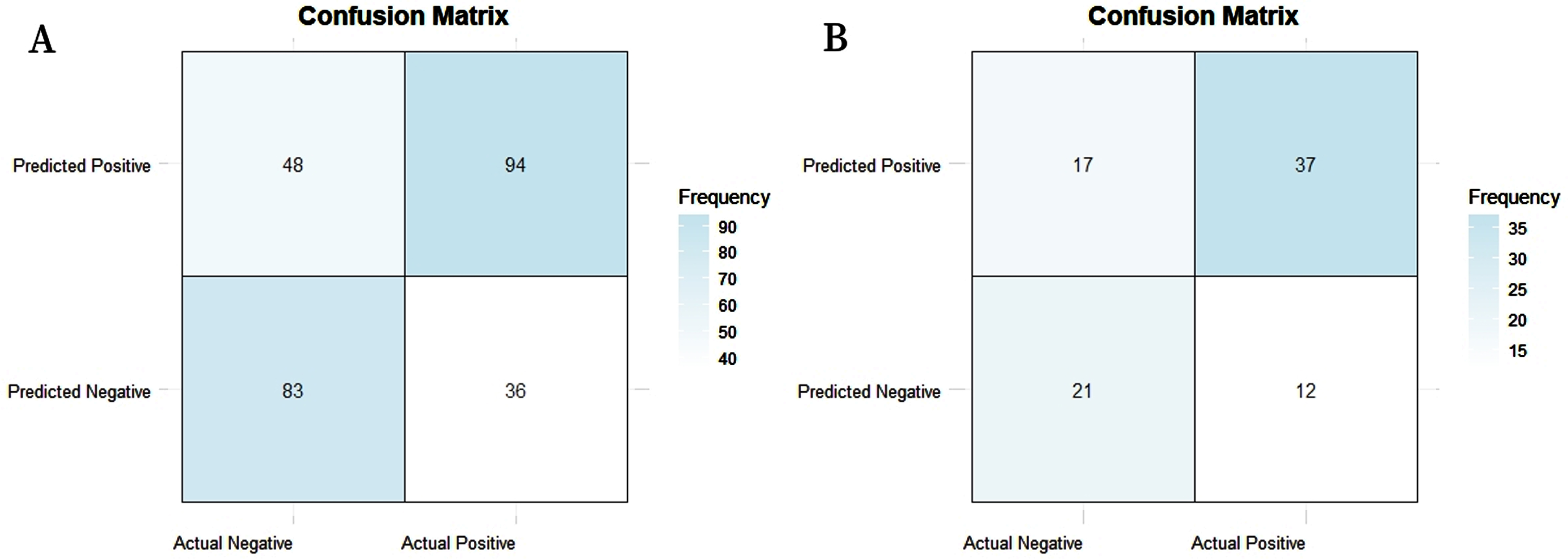
Confusion matrix. The 2×2 contingency table reports the number of true negatives, true positives, false negatives, and false positives. (A) Training cohort; (B) Test cohort.
The AUCs of the GSUS, DECT, GSUS combined DECT joint predictive model in the training dataset was 0.700 (95% CI, 0.662–0.706), 0.721 (95% CI, 0.683–0.727), and 0.760 (95% CI, 0.728–0.762), respectively. In the test dataset, the AUCs were 0.643 (95% CI, 0.582–0.734), 0.680 (95% CI, 0.623–0.772), and 0.744 (95% CI, 0.686–0.784), respectively. Detailed information about the predictive performance of the models is shown in Table 3. The joint model performed satisfactorily in both the training and test dataset, with AUCs of 0.760 and 0.744, respectively. The combined model performed better than the GSUS and DECT models independently. The ROC curves of the three models are shown in Fig. 5.
Performance of the constructed radiomics models
Performance of the constructed radiomics models
aAUC, area under the curve. bSEN, sensitivity. cSPE, specificity. dPPV, positive predictive value. eNPV, negative predictive value. fACC, balanced accuracy.
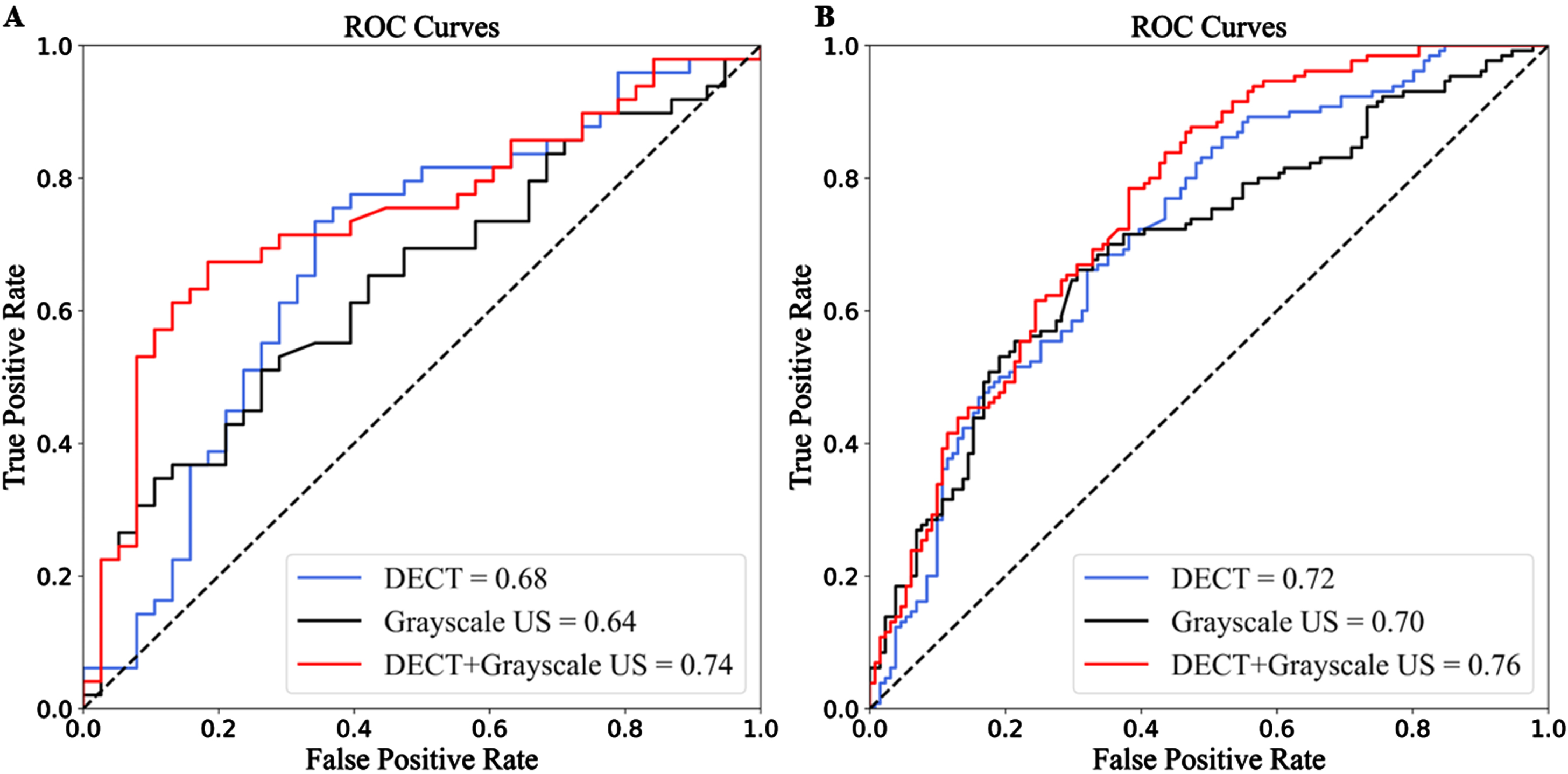
The ROC curves of the three models. (A) Test cohort; (B) Training cohort. US, ultrasound; DECT, dual-energy computed tomography; ROI, region of interest; ROC, receiver operating characteristic curve.
DCA was used to determine the clinical significance of radiomics models. The DCA also indicated that the GSUS and DECT combination predictive model functioned effectively (Fig. 6). It demonstrated that utilizing the combined radiomics model to predict CLNM adds more net benefit than either the ‘treat-all-patients’ or ‘treat-none’ techniques and unitary radiomics models.
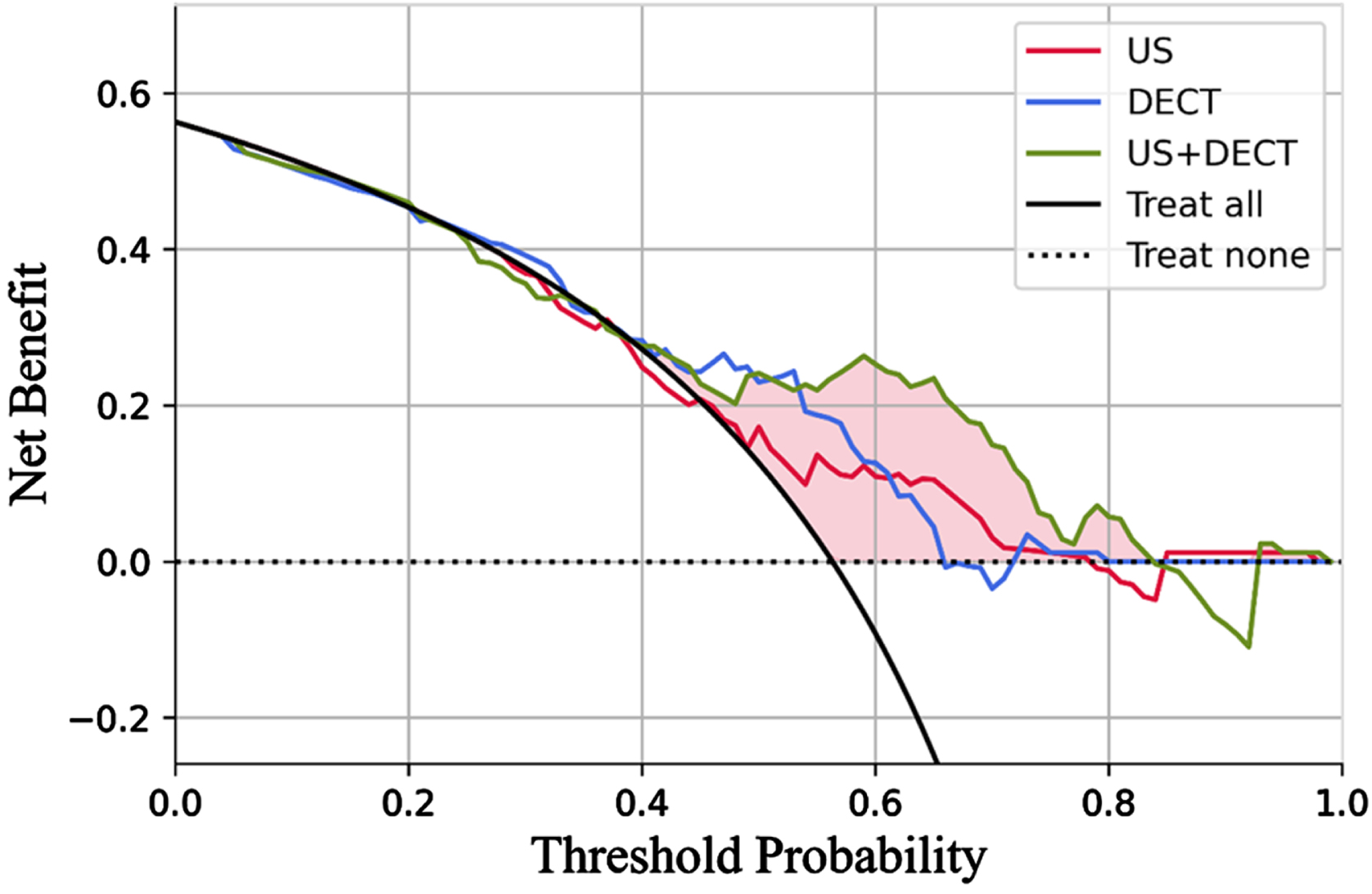
DCA of each model in predicting CLNM for PTC. The vertical axis demonstrated standardized net benfit. The horizontal axis measures the corresponding risk threshold. The DCA showed that if the threshold probability is between 0.55 and 0.85, adopting the dual-modal joint radiomics model (green curve) derived in the present study to predict CLNM is more beneficial than the US radiomics model (red curve) and the DECT radiomics model (blue curve). DCA, decision curve analysis; US, ultrasound; DECT, dual-energy computed tomography; CLNM, cervical lymph node metastasis; PTC, papillary thyroid carcinoma.
Most PTCs progress slowly and do not threaten the patient’s life. However, some PTC subtypes (high cell count, diffuse sclerosing type, infiltrative type) exhibit aggressive behaviours and recurrence with ETE, vascular invasion, and CLNM. CLNM is an important indicator for evaluating the progression of PTC, and it is also a predictor of poor prognosis determined by multiple variables. An important measure to avoid the rapid progression of PTC is early identification of tumors with potential for CLNM. Surgical resection is the primary therapeutic option for clinically diagnosed PTC patients now. Patients with suspected thyroid tumors must undergo fine needle aspiration biopsy and prophylactic lymph node dissection (PLND) to detect CLNM. However, both procedures are invasive and unnecessary for most patients without CLNM. The benefits of PLND are debatable, because the possibility of increased risk of postoperative complications, hypoparathyroidism must be considered when performing prophylactic lymphadenectomy and total thyroidectomy. Henry et al. [22] reported that central neck lymph node dissection would increase the risk of permanent hypoparathyroidism from 0% to 4%. Therefore, preoperative early identification of CLNM of PTC is not only conducive to clinical selection of appropriate surgical plan and scope, reducing the occurrence of postoperative complications, but also reduce the risk of recurrence, avoid second surgery, and positively improves prognosis.
It is required to investigate a more objective and reliable approach of accurately predicting CLNM prior to invasive and surgery. In this study, the clinical data of the 348 patients between the CLNM and CLNM-Free groups showed that the male, the node diameter≥1 cm, multifocality and bilateral were conformed associated with CLNM, which was consistent with other relevant reports [23–26]. For GSUS imaging characteristics, we found that the internal echo pattern, calcification, vascularization of lesions between two have the otherness, which are related with CLNM and this corresponds with previous studies [27–29]. Some characteristics of DECT, including irregular tumor shape, interrupted thyroid contour, with marginal contact, without cystic degeneration of PTCs prefer to have CLNM. Interrupted thyroid contour and marginal contact of tumors were significant CT images characteristics which having high relation to ETE of PTC [30]. And ETE is corrected with CLNM, because thyroid contour interrupting and dissemination in the glandular lobes leading expansion by surrounding lymphatic capillaries [7, 31].
In the dual-modal radiomics prediction model radiomics signatures constructed based on GSUS and DECT, including GLCM, shape features, GLRLM, GLDZM and NGTDM. These invisible radiomics features provide more information about the vascular microenvironment of PTC associated with invasive bio-behavior [32, 33], which is to some extent correlated with CLNM. In this study, we innovatively used SVM machine learning classier with kernel = ’linear’ to create the DMR model. The linear-SVM classifier is usually applied specifically for massive levels of high-dimensional data and features, this increases its training and classification speed [34]. The AUC of the predictive model constructed from the radiomics features of single-modal GSUS was 0.700 in the training cohort and 0.643 in the test cohort, the AUC of single-modal DECT was 0.721 in the training cohort and 0.680 in the test cohort. The AUC value of the GSUS model in this study was lower than that of the DECT model in the test cohort, which could be attributed to the fact that the DECT image contains more texture features.
Furthermore, the final AUC value of the GSUS combined DECT model (AUC = 0.774) was higher than that of the GSUS and DECT models separately. In the current study, we used stratified 10-fold cross-validation, which held out 10% of the test data, and then randomly divided all the data into ten parts and repeated ten times. Vivian Y. Park et al. [35] developed a USR model to predict lateral lymph node metastasis in PTCs and the AUC of its performance in discriminating metastatic and non-metastatic lateral lymph node metastasis was 0.710 (95% CI: 0.649–0.770) in the training cohort and was 0.621 (95% CI: 0.560–0.682) in the validation cohort. The AUC of their model for the diagnosis of lateral CLN metastasis was lower in the validation cohort compared with the dual-modal predictive model in our current study (0.621 vs 0.744). In another research, Zou et al. [36] used different kinds of machine learning models based on US images achieved by six different Doppler ultrasonic diagnostic apparatuses to determine the probability of CLNM. The AUC value of their model for the diagnosis of CLNM was slightly lower in the validation cohort compared with our study (0.731 vs 0.744). The higher AUC value in this current study could be attributed to the better images used in this study and we also constructed DMR model using radiomics features extracted by GSUS and DECT images.
Zhou and colleagues [16] created and validated two iodine maps of DECT-based radiomics nomograms for preoperatively predicting CLNM and central lymph node metastasis of PTC. The AUC of their model predicting CLNM was 0.807 which is higher than ours (AUC = 0.744). They used arterial and venous phase iodine maps and as well included more information of ROIs, but the relatively higher radiation exposure during dual-phase contrast-enhanced DECT scan should not be ignored and the PTC patients in our hospital only undergo dual-energy scanning for the venous phase, this benefits to patients are obvious. And their nomogram prediction model they constructed incorporated clinical risk factors, not just radiomics signatures.
New imaging technology and good quality images improve predictive model performance in machine learning. A good tumor risk predictive model is more than just a basic mathematical combination of dependent variables and independent variables, it must also have real therapeutic significance [37]. As a result, we used the clinical DCA to further assess the model’s real benefit; the results confirm the model’s good feasibility in the actual clinical application (Fig. 6). On the other hand, the efficiency of the dual-modal joint prediction model constructed by us is higher than that of any single-modal prediction model, which also supports some studies reported that combined CT/US may become a supportive role, especially for preoperative surgical planning in patients with suspected CLNM or a high-risk of CLNM [38, 39].
The limitations of this study include the following aspects. Firstly, this is a retrospective study, so it may be inevitable that there are some selection biases and data imbalances that affect our results. Secondly, among the selected cases, it is difficult to determine which lesion causes CLNM in patients with multifocal and bilateral PTC, and we do not have specific subtypes of PTC. Thirdly, the use of iodized contrast media may delay radioiodine therapy in patients with PTC. However, radioactive iodine therapy is usually performed at least 2 months after surgery in our facility and previous studies have reported that uptake of iodine-131 is normal at this time interval [40]. Fourthly, we just use a single classifier and no external test set. Fifthly, since the data in our research are from a single center, the prediction model will have some robust problems.
In summary, we presented a non-invasive predictive tool based on GSUS and DECT radiomics features. The DMR model could provide useful information for the preoperative assessment of CLNM in patients with PTC and guide a more appropriate surgical planning.
Abbreviations
Accuracy American Thyroid Association Areas under the curve Confidence interval Cervical lymph node Cervical lymph node metastasis Chinese Society of Clinical Oncology Computed tomography Decision curve analysis Dual-energy computed tomography Dual-modal radiomics Extrathyroidal extension Grey-level co-occurrence matrix Grey-level dependence matrix Grey-level run length matrix Grey-level size zone matrix Grayscale ultrasound Intraclass correlation coefficients Least absolute shrinkage and selection operator Marginal contact range Magnetic resonance imaging Neighborhood grey-tone dependency matrix Negative predictive value Pearson correlation coefficient Positron emission tomography Prophylactic lymph node dissection Positive predictive value Papillary thyroid carcinoma Receiver operating characteristic curve Region of Interest Single-energy computed tomography Sensitivity Specificity Support Vector Machine Thyroid carcinoma Ultrasound Ultrasound radiomics
Funding
This research was financially supported by National Natural Science Foundation of China (Project No. 81971629), Science and Technology Bureau of Zhenjiang (Project No. SH2020046), Postgraduate Research & Practice Innovation Program of Jiangsu Province (Project No. SJCX21_1728) and National Natural Science Foundation of Jiangsu Province (Project No. BK20211122).