
Abstract
School psychology in Singapore gained greater prominence with the development of the National Mental Health Blueprint in 2007 that included a focus on children and adolescents. A partnership between the Ministry of Health and the Ministry of Education was formed to develop a community mental health pilot program called ‘Response, Early Intervention and Assessment in Community Mental Health for Students’ (REACH). Disruptive behavior disorders (DBD) are among the most common disorders seen in schools and child psychiatric clinics in Singapore. Children with disruptive behavior disorders (DBD) often exhibit deficits in social cognition and behavior, thereby influencing their cognitive appraisal processes and interpersonal problem-solving skills. This in turn affects their processing and interpretation of social cues in ambiguous situations, and mars subsequent production of socially competent behavior. This article describes a potential framework based on the cognitive-behavioral approach for working with children with disruptive behaviors and aggression in the school system. By combining REACH, a national collaborative framework, and evidence-based treatment programs, we provide a promising model of care to support children and their families in Singapore.
Keywords
Child psychiatrists, paediatricians, school and educational psychologists, school counsellors, and other mental health professionals often provide psychological services to children and adolescents in Singapore. The effort to promote psychological services for Singaporean children and adolescents in schools is faced with great challenges—such as the lack of qualified mental health professionals and a current 1:14,000 ratio of school psychologist to students (Yeo & Choi, 2011), the social stigma associated with seeking professional help (Ang, Lau, Tan, & Lim, 2007; Kee, 2004; Van Schalkwyk, 2011), and the absence of a mandate for special education services, amongst others. A recent review by Jimerson, Skokut, Cardenas, Malone, and Stewart (2008) indicated the lack of indicators of school psychology’s presence in Singapore. Despite this, one needs to be mindful that the development and practice of school psychology differs in each country and region (e.g. Ding, Kuo, & Van Dyke, 2008; Zhou, Bray, Kehle, & Xin, 2001).
School psychology is not new in Singapore; we have long had the provision of services such as school counselling and guidance services, academic and behavioral assessments, and intervention (Ministry of Education, 2012a, 2012b). Although school psychology is not a new discipline, due to the challenges outlined earlier, school psychology practice has not been very systematic and the pace of development has only been gradual. School psychology gained more prominence with the development of the National Mental Health Blueprint in 2007 that further developed mental health services in Singapore. The focus of the Blueprint for children and adolescents is in the school system, as primary school education is mandatory and schools form the most appropriate avenue for prevention and intervention efforts. This led to a partnership between the Ministry of Health and the Ministry of Education to form a community mental health pilot program called ‘Response, Early Intervention and Assessment in Community Mental Health for Students’ (REACH).
The primary aims of the REACH program are to train and support school counsellors in the early identification and management of children with behavioral and emotional difficulties. The REACH program comprises a multidisciplinary team of psychiatric residents (also known as medical officers in the Singapore context), psychologists, medical social workers, nurses, and occupational therapists. The REACH team works closely with each school to identify children at risk for behavioral and emotional disturbance, including violence, and engages these children and their families into services before the emerging problems become severe. A network of family doctors and social service agencies within the school’s vicinity are also engaged to provide support for these children and their families. The REACH program helps to reduce the stigma associated with seeking mental health services. Previous studies on help-seeking behavior indicated that reluctance to seek professional help is more salient in Asian countries because seeking help from non-family members is considered a ‘loss of face’ (Leong, 1999). As a result, many Asian families tend to avoid seeking treatment until a crisis develops (Berg & Jaya, 1993). The REACH program supports the school counsellor, teachers, and other staff, who may have developed trust and rapport with the parents and the child to help them ‘save face’ by assuring them of their good intentions (Berg & Jaya, 1993; Van Schalkwyk, 2011).
In line with the Ministry of Education’s (MOE) classification of mainstream schools into clusters (Ministry of Education, 2011), four REACH teams were formed to support these four school clusters of North, South, East, and West Singapore, advised by staff psychiatrists from three hospitals with child psychiatry services.
Child and adolescent mental health in Singapore
Child and adolescent mental issues in Singapore are increasingly gaining attention. Using the World Health Organization (WHO) concept of Disability Adjusted Life Years (DALYs), findings from a Singapore burden disease study showed that mental health disorders in youths from birth to 14 years (e.g. Attention Deficit Hyperactivity Disorder, Autism Spectrum Disorders) contributed to three of the five most common conditions (Phua, Chua, Ma, Heng, & Chew, 2009). In addition, a recent survey of about 2,400 youths revealed that 5% of children (6–12 years old) in Singapore schools exhibit evidence of externalizing problems (non-normative aggression, hostility, antisocial behavior toward others) (Woo et al., 2007). Within the clinical setting, disruptive behavior disorders (DBD) such as ADHD, Oppositional Defiant Disorder (ODD), and Conduct Disorder (CD) are the most common diagnostic referral issues to child mental health centres from schools, with referrals continuing to show a rising trend (Lee, Fung, Cai, & Teo, 2003).
Children and adolescents with DBD are more likely than their typically developing peers to exhibit aggressive behaviors (Moffitt, 1993; Patterson, Reid, & Dishion, 1992). Aggression is a salient problem in children and adolescents with DBD that serves as a predictor for various negative outcomes including delinquency and criminality, and substance abuse (Fite, Colder, Lochman, & Wells, 2007; Loeber & Farrington, 2000; Piquero & Chung, 2001). Children and adolescents with DBD are included in mainstream schools, together with other typically developing children. Given the symptoms exhibited by children and adolescents with DBD, it is not surprising they experience difficulties in school. Teachers are also likely to experience frustration managing these children while fulfilling their primary responsibility of teaching. Hence, evidence-based treatments that prevent the developmental trajectory towards more serious outcomes are needed.
Many researchers have suggested that intervention programs that are comprehensive, integrated, and directed toward the salient features of DBD are most effective (Kazdin, 2002). Cognitive Behavioral Therapy (CBT) based programs have gained popularity due to their effectiveness and generalizability (Dunn, Lochman, & Colder, 1997; Prinz, Blechman, & Dumas, 1994). Effectiveness of CBT based programs [e.g. Social Problem-Solving Skills Training (SPSST)] in children and adolescents who are severely aggressive and disruptive has been demonstrated in several studies using Singapore samples (e.g. Ang, 2003; Ooi, Ang, Fung, Wong, & Cai, 2007; Yeo & Choi, 2011). For instance, Ang (2003) found that juveniles in the SPSST intervention condition improved significantly on aggressive behavior from pre-intervention to post-intervention compared with juveniles in the wait-list control condition. Similarly, Ooi et al. (2007) demonstrated that children with DBD in the SPSST + Treatment-As-Usual (TAU) group showed significantly lower levels of aggression and significantly lower levels of parental stress at post-treatment and at three-month follow-up in comparison to the TAU group, who received medication treatment and individual supportive therapy and parent training using behavioral techniques.
A framework based on social problem solving skills training
Findings from various clinical studies have contributed to the knowledge of effective intervention for children and adolescents with DBD (e.g. Greenberg et al., 2003; Ooi et al., 2007). The REACH program adopts a variety of tools and resources that were originally designed for use in tertiary child psychiatric settings and then modifies (if necessary) these tools for use in the community. One of these examples is the SPSST program (i.e. Ang & Ooi 2003a, 2003b) described in this article, which has been validated in the Singapore setting. The SPSST program also provides a useful framework for working with children and adolescents with DBD and those without serious aggression problems and without diagnosable conditions, in the school system.
The 12 lessons of the SPSST program, a revised version from the nine-lesson program (e.g. Ang & Ooi, 2003a; 2003b; Ooi & Ang, 2004) involves teaching of various core behavioral and social-cognitive skills such as: (a) identification of feelings; (b) anger coping skills; (c) social-cognitive skills; and (d) pro-social skills. These skills have been identified as factors that buffer students from behavioral problems (Walker et al., 1996). The SPSST program is based on our understanding of the social-cognitive difficulties of children with DBD (Crick & Dodge, 1994; Crozier et al., 2008; Dodge, Lochman, Harnish, Bates, & Petit, 1997). The main aim of the SPSST program is to alter children’s distorted thoughts and beliefs (e.g. attributions of intent and beliefs about the legitimacy of aggression) to produce changes in thinking, feeling, behavior, and to build more effective coping strategies, which can then be applied and generalized to everyday life. The SPSST program also draws from Social Learning Theory, which emphasizes the importance of observational learning, self-reflection, and reinforcement in the acquisition and maintenance of behavioral repertoires (Bandura, 1986).
While the SPSST program is based on a Western understanding of the CBT approach, the language, analogies, and scenarios/examples that are relevant to Singaporean children’s cultural context are used. In addition, the therapist needs to be mindful of certain cultural sensitivities such as the importance of developing trust and rapport with the children to help them ‘save face’ (Berg & Jaya, 1993; Kee, 2004; Van Schalkwyk, 2011). Also, as Asians are less direct in expressing their experiences and feelings (Kaneshige, 1973; Kee, 2004), the therapist may need to spend more time on rapport building or find other ways of eliciting this information (e.g. writing a journal). The 12-lesson SPSST program can be delivered as an individual therapy, a group-based treatment, or a combination of both treatment modalities. Based on our clinical experience, two therapists are required for a group of six to eight children. Each treatment session last approximately 75–90 minutes, and each is devoted to one lesson. Empirically supported strategies for teaching appropriate skills (e.g. modelling, feedback, social reinforcement, role-play practice) are used. Homework assignments are provided at the end of each lesson and will be reviewed during the following session. The 12-lesson SPSST program is currently being evaluated in an on-going randomized controlled trial (RCT) involving children and adolescents with DBD (between 9- and 16-years-old) to examine the efficacy of omega-3 fatty acids and SPSST in reducing aggression.
SPSST program components and program content.

Note: SPSST = Social problem-solving skills training.
Lesson 1 of the SPSST program focuses on the identification of feelings in children and begins with children identifying and discussing a wide range of feelings including pleasant (e.g. calm, joyful, hopeful) and unpleasant (e.g. sad, angry, lonely, guilty) feelings they have experienced. Children are taught to identify clues that could help them to understand feelings such as words (what people say), tone of voice, body language, and the situation. Lesson 2 targets and teaches specifically feelings underlying anger and associated with anger. It teaches strategies to help children recognize anger triggers in their physical bodies (e.g. feeling tensed or relaxed), thoughts (e.g. I want to hit him), and actions (e.g. punch). Children are taught to understand that anger feelings can range from mild (e.g. irritable), to moderate (e.g. frustrated), or severe (e.g. enraged) and help them articulate what makes them angry or calm. Following that, children are guided to understand the distinction between feelings and behavior and that feelings influence but do not dictate their behaviors. While children are taught to normalize and accept their angry feelings, they are also reminded the three Anger Rules: (1) It is not okay to hurt myself when I am angry; (2) It is not okay to hurt/hit others (including animals) when I am angry; and (3) It is not okay to destroy things when I am angry.
Lessons 3 and 4 are designed to teach children various anger coping techniques such as deep breathing, visualization, muscle relaxation, leisure activities, positive self-talk, asking for help, and assertive management of intense emotions and difficult situations. The therapist can choose to teach three to four anger coping techniques that are most appropriate for their group of children. In these lessons, children are asked to identify situations that typically arouse their intense, angry feelings and practice anger coping strategies to inhibit automatic and impulsive responses. Children are encouraged to use these anger coping techniques when they encounter angry situations as part of their homework. Lessons 5 and 6 are designed to teach children empathy and perspective-taking skills. Through these lessons and activities, children are guided to recognize other people’s feelings (empathy), see things from other people’s point of view, and pay attention to social cues inconsistent with attribution of hostile intent (perspective-taking). To practice empathy skills, children will participate in a discussion of social encounters that involve identifying other people’s feelings and the impact of their behaviors towards them. To practice perspective-taking skills, children will participate in a discussion of social encounters that involve discriminating between accidental and intentional actions, and share experiences and reactions to hypothetical situations. This enables the child to gradually recognize the possibility that negative social encounters could be the result of an accident and may not always be intentional.
Lesson 7 focuses on Fighting Fair, another method of resolving frustration and conflict by building rather than tearing down relationships, and it allows anger to be expressed in a healthy way (Shapiro & Cole, 1994). In Fighting Fair, children are taught five rules: (1) Attack the problem, not the person; (2) Listen to the other person, and allow for disagreement; (3) Respect the other person’s feelings; (4) Take responsibility for your own actions; and (5) Avoid ‘fouls’. Children apply this strategy to simple hypothetical problem situations and to real life problems. They practice using verbal mediation or ‘self-talk’ (Meichenbaum, 1977) as a strategy to remind them to control impulses, think about consequences of actions, and reinforce their own behaviors. Lesson 8 teaches children pro-social skills such as sharing, cooperation, helping, making friends, and keeping out of fights. Many children who display behavioral difficulties have developed such a repertoire of unacceptable behaviors over many years such that these negative behaviors become almost part of these children’s personality and self-image. The homework exercise based on ‘Random Acts of Kindness’ helps to gradually reverse this negative downward spiral by deliberately putting children in situations where they will behave well and even in altruistic ways.
ANGER Plan.
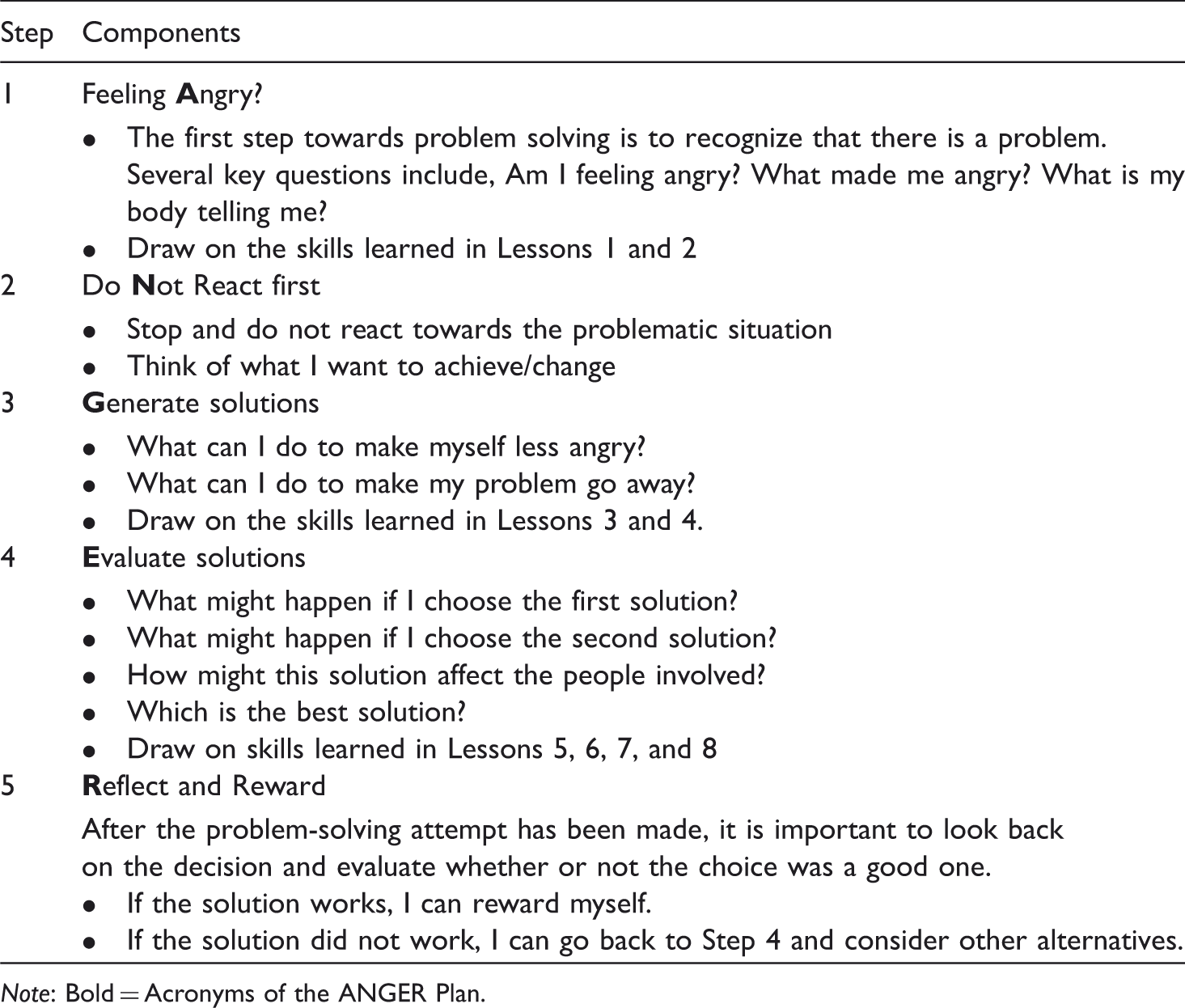
Note: Bold = Acronyms of the ANGER Plan.
Lesson 12 serves as the summary and integrative review session. This lesson requires children to demonstrate what they have learned from previous lessons. Another critical component of the final intervention session is empowerment. Therapists need to empower children by encouraging and believing that they have the capacity to overcome these various behavioral difficulties on their own gradually and to continue to apply what they have learned in their daily interactions with other people. In addition, therapists need to emphasize to children that improvement in behavior can be a long, slow, and tedious process. Thus, it is crucial for children to set realistic and manageable goals for themselves as they strive to improve their behavior. Booster sessions should be considered to support generalization to natural social settings as well as for the maintenance of skills. Parent training supplemented with child focused CBT-based programs have been found to be more effective than child focused CBT-based programs alone (e.g. Kazdin, 1996, 2001). Because the REACH team works closely with the school and families, combining child focused CBT-based programs and parent training is feasible and has the potential to enhance treatment effects. At present, the REACH program is adopting the SPSST program but it has not been formally evaluated in the school setting in Singapore. Such an effort is critical to further validate the effectiveness of the SPSST program.
Conclusion
This article provides information about the continuing development and evolvement of school psychology in Singapore. We describe the development of the National Mental Health Blueprint promoting child and adolescent mental health services in Singapore. We also describe a potential framework based on the CBT approach in addressing disruptive behaviors and aggression in the school system. By incorporating a national collaborative framework (i.e. REACH program) and evidence-based treatment programs, we can develop a promising model of care to support children and their families.