
Abstract
Losing an only child affects the mental health of many older adults in China, placing them at a higher risk of loneliness. However, few studies explore the long-term effects of losing an only child on loneliness trajectories among older Chinese bereaved parents. Adopting a qualitative, grounded theory approach, this study investigates how experiences of loneliness among bereaved parents evolve and the implications for staged intervention. Twenty-seven in-depth interviews were conducted with people who lost their only child in Shanghai and Wuhan. A multistep data analysis technique was used to analyze the data. The findings indicate that trajectories of perceived loneliness have three distinct stages and follow a U-shape in their frequency and intensity. Interventions of psychological consultation, social network restoration, and improved old-age support should be emphasized at each stage.
The implementation of the one-child policy between 1979 and 2015 resulted in many one-child families in China. Couples who have experienced the death of their only child after the wife has been through menopause and did not have another child are known as Shidu parents or Shiduer (N. Wang & Hu, 2019). The number of Shidu families in China was around one million in 2012, and increases by approximately 76,000 households per year (Wu, 2013). With the first generation of one-child parents entering old age, their vulnerability and specific support needs have attracted scholarly attention (L. Chen, Song, & You, 2019).
Among many issues, considerable research has identified loneliness as a mental health problem, but few studies have explored the specific nature and development of loneliness among this group. This study adopts a qualitative approach, using retrospective interview data to explore the experience of loneliness among Chinese Shiduer. We focus on how loneliness is perceived among Shidu parents and how this feeling evolved. Importantly, this investigation provides evidence for targeted interventions at different stages of grief to improve the quality of life of Shidu parents.
Loneliness and Parental Bereavement
Loneliness is defined as an experience associated with a discrepancy between one’s perceived and ideal relationships (Sermat, 1978) or an unpleasant experience arising from deficiencies in social relations (Peplau & Perlman, 1982). Weiss (1973) distinguishes between emotional loneliness and social loneliness. The former reflects an individual’s perceived lack of intimate attachment, while the latter is associated with a lack of social engagement in the community or larger society (Dykstra & Fokkema, 2007). Within emotional loneliness, detachment from family relations and a lack of romantic relations are identified as family and romantic loneliness, respectively (Cramer et al., 2000). Existing studies recognize that loneliness is influenced by sociodemographic factors like being female, widowed, in poor health, childless, aged 75 and above, or living alone (Grenade & Boldy, 2008; Victor et al., 2005). In addition, loneliness is related to the absence of social relationships, dissatisfaction in relationships, or low levels of social engagement (Victor et al., 2005).
Losing a loved one is conceptualized as “intimate loneliness” (Riches & Dawson, 2000). Indeed, literature shows that bereaved parents are more prone to loneliness compared with other parents in China and internationally (Arnold & Gemma, 2008; Davies, 2004; Hu et al., 2014). Among bereaved parents, those without living children experience the most severe loneliness (Ren & Ye, 2017). Evidence suggests that the experience of loneliness among bereaved parents could decline over time if mediated by available emotional resources, living children, good family function, and counseling services (Hang et al., 2015; Hu et al., 2014). However, loneliness cannot be alleviated by increased income or financial support (Ren & Ye, 2017).
Loneliness Among Shidu Parents
Although very few studies have focused on loneliness among Chinese Shiduer, we can anticipate that this group faces risks of both emotional and social loneliness. On one hand, losing an only child renders the meaningful parent–child relationship unavailable. On the other, the quality and number of other important social relations change due to cultural stigma and self-isolation (Masi et al., 2011). Using the UCLA Loneliness Scale, scholars found that Chinese Shidu parents experienced significantly greater loneliness compared with their nonbereaved counterparts (Y. Chen & Hang, 2016).
The social and emotional loneliness among Chinese Shidu parents is deeply rooted in their cultural context. Chinese society is underpinned by a strong Confucian ideology and familism culture, advocating filial piety and continuity of the family line as a life mission (Zhang & Jia, 2018). People who fail to meet society’s expectations face significant social stigma (Zheng & Lawson, 2015). Thus, becoming childless later in life can be stigmatized as receiving divine retribution for familial evil in one’s previous life (N. Wang & Hu, 2019). This severe cultural stigma not only leads to social discrimination for Shiduer, but also causes a psychological burden, lowering their self-esteem (Zhang & Jia, 2018; Zheng et al., 2017). Consequentially, Shiduer become isolated in Chinese society, developing significant social loneliness.
A child has great value to their parents under the one-child policy and families without children are seen as incomplete (Chow & Zhao, 1996). Therefore, couples whose only child dies may find their family structure and intergenerational relationships deficient, leading to specific family loneliness (Chou & Chi, 2004). In addition, research has suggested that many Shidu couples experience marital trouble (N. Wang & Hu, 2019; Zheng et al., 2017). Eventually, some Shidu parents divorce, while others face communication difficulties after losing their child (Riches & Dawson, 1996). This uneasy couple relationship may further aggravate Shiduer’s feelings of emotional loneliness.
Although some studies have identified vulnerable mental health status and loneliness among Shiduer (E. Wang et al., 2019; Wei et al., 2016; Yin et al., 2018), few focus on their loneliness experiences and trajectories over time. As existing studies found a strong relationship between loneliness and higher risks of morbidity and mortality (Hawkley & Cacioppo, 2010; Luo et al., 2012), it is crucial to investigate loneliness experiences and their characteristics over time among Chinese Shidu parents (an increasingly at risk subpopulation) to provide timely and targeted interventions.
Materials and Methods
A grounded theory (GT) approach was adopted in this study. In GT, data collection and analysis happen simultaneously in an iterative process to develop a theory (Charmaz, 1996). This method could generate basic social processes by theoretical coding (Glaser & Holton, 2005; Glaser & Strauss, 2017) and was adopted here to understand how loneliness is perceived and handled by Shidu parents at different stages after their child’s death.
Sampling and Data Collection
We implemented a combination of purposive and theoretical sampling to recruit participants following GT methodology (Glaser, 1978, 1992). Initially, purposive sampling was adopted to access Shidu parents who had experienced loneliness (Strauss & Corbin, 1998). Considering accessing Shidu parents is difficult and loneliness is a sensitive topic to discuss (Rokach & Brock, 1997), our initial participants were sampled from our previous research networks in urban Shanghai and Wuhan where we had already established mutual trust (Pettigrew & Roberts, 2008). The recruitment criteria were Shidu parents who (1) were aged 49 and over; (2) did not give birth or adopt after their child’s death; and (3) reported feeling lonely in our previous research.
Eighteen potential participants from communities in Wuhan and Shanghai were contacted through Wechat App or telephone. Fifteen gave written consent to participate while three opted not to participate due to health and time issues. The first stage of data collection occurred between March and May 2019. Semistructured, in-depth interviews were conducted at participants’ homes or quiet restaurants. We designed broad questions to capture participants’ perceptions and experiences relating to loneliness in everyday life after losing their only child. The first stage interview schedule covered the experience of this loss, subsequent life changes and restoration, intimate relationships, social networks, social participation, and health issues. Demographic and socioeconomic information was also collected. Interviews lasted from 60 to 125 min, averaging 73 min.
During analysis, we found that the perception of loneliness among participants was related to the duration of bereavement and their own life stages. As 73% of the first stage participants had been grieving for less than 10 years, and 67% of them were aged below 65, we aimed, in the second stage, to recruit more participants who had been grieving for more than 10 years, and were aged 65 and over to expand our research scope. We contacted potential participants living in Wuhan and Shanghai from our previous research networks. Data collection adopted a similar interview protocol to Stage 1 but focused more on the staged characteristics of loneliness perception and experience and changes in participants’ perceptions over time. After 12 interviews, data saturation was reached (Charmaz, 1996). Interviews were conducted between June and August 2019, ranging from 55 to 120 min, averaging 80 min.
This study received ethical approval (PAS1901-05). We acknowledged that our interview might cause distress, and therefore, made it clear that participants could withdraw at any time or opt to not answer any questions. We assigned numbers to participants and kept research materials in a locked drawer and password-protected disk to ensure anonymity and confidentiality.
Data Analysis
Interviews were conducted in Chinese and transcribed verbatim to Chinese text. Data analysis was an iterative process along with data collection; memos were kept throughout the research process, exploring theoretical possibilities through analytic, conceptual, and theoretical notes (Thornberg & Charmaz, 2014). We followed a multistep data analysis technique including initial coding, focused coding, and theoretical coding outlined by Thornberg and Charmaz (2014).
Initial line-by-line coding was conducted independently by both authors. Constant comparative methods were used to compare data with data, data with code, and code with code, to sort and cluster codes. Codes of similar meanings were merged for higher-level codes. After completing the initial coding, we discussed the final coding structure and selected one core category (loneliness trajectories) which we believed made the most analytic sense and established a set of focused codes around this category. These codes guided our second-stage theoretical sampling to collect more appropriate cases for further exploration. After focused coding with all transcripts, we explored possible relationships between categories and developed theoretical codes such as causes, stages, and consequences to summarize participants’ staged development of loneliness trajectories.
We adhered to rigorous research methods by coding independently, constantly reviewing our methods and data, seeking coding advice from other researchers who had research experience in GT, and sending preliminary results to six participants for member-check (Lincoln & Guba, 1985). Significant feedback was considered and integrated into the subsequent analysis. Final themes were confirmed by consensus between the researchers and six research participants.
Results
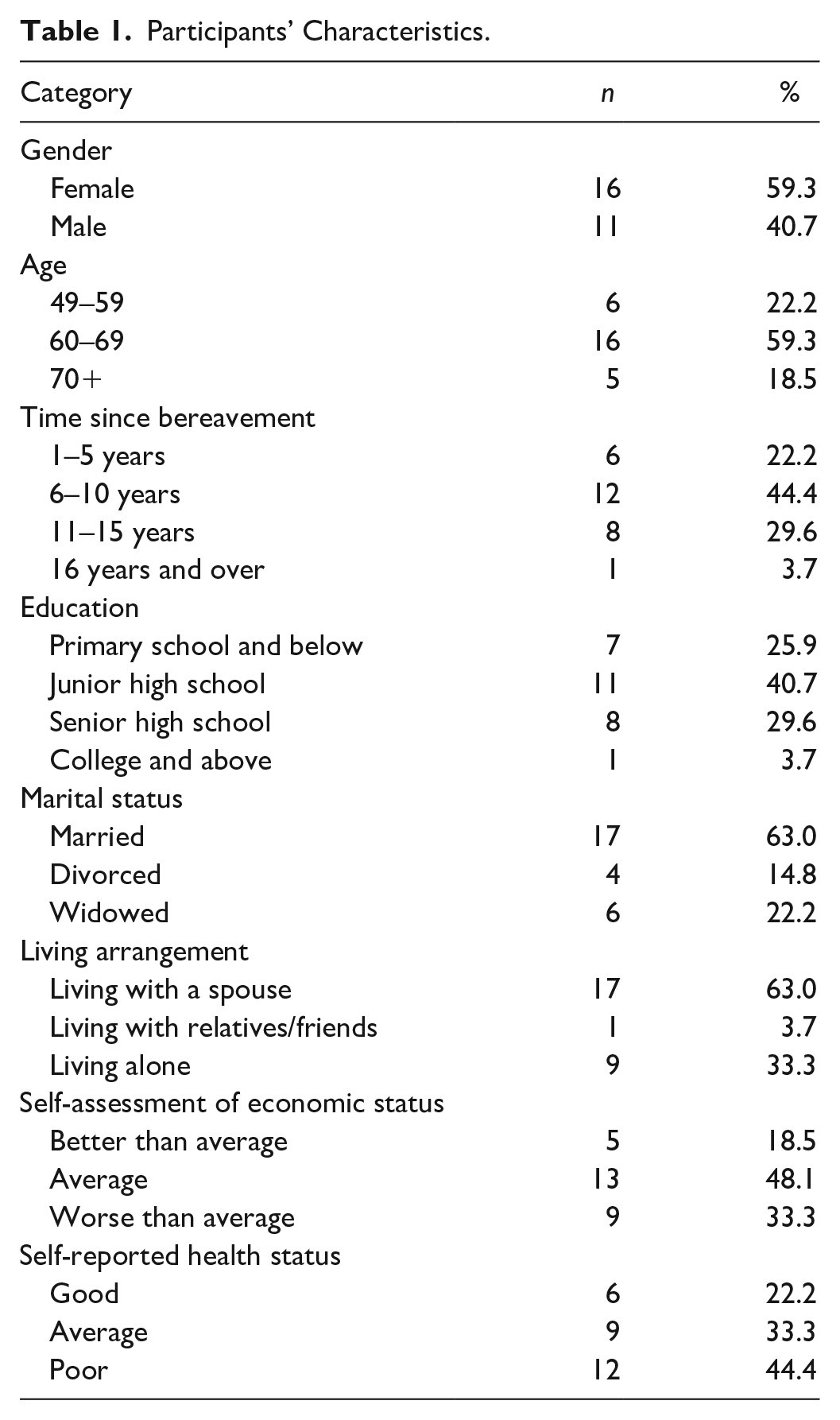
Among the 27 participants, 11 were men and 16 were women. Their ages ranged from 49 to 76 years, averaging 65 years. Most participants had junior (40.7%) or senior (29.6%) high school education. More than half (63.0%) were married, while 22.2% and 14.8% were widowed and divorced, respectively. The average time since losing their only child was 9 years. Of the participants, 63.0% lived with a spouse, 33.3% lived alone, and 3.7% lived with others. Most participants rated their economic status as average (48.1%) or below (33.3%) and their general health as average (33.3%) and poor (44.4%) (see Table 1; for participants’ information, see Supplemental Material).
Participants’ Characteristics.
Overall, the experience of loneliness among the participants followed a three-stage path; the intensity and frequency of feelings of loneliness formed a U-shape.
Stage 1: Intense Emotional and Social Aspects of Loneliness
All participants reported a period of severe distress immediately after the death of their child and unmanageable levels of emotional and social loneliness which were “difficult to escape,” “constant,” and “everywhere.” This stage lasted 6 months to 2 years, depending on individuals’ characteristics and available support. We generally found that married participants and those with support networks recovered sooner than unmarried and isolated participants. Our analysis showed three triggers for intensive and frequent feelings of loneliness.
Interrupted bonds and emotional loneliness
Recalling life before their child’s death, most participants communicated that their child was their life focus, whom they devoted endless time and effort to. The child’s death severed their most valued bond and destroyed life’s meaning, resulting in severe family loneliness. F1 confided, In the first year after my child’s death, I was drowning in feelings of loneliness all the time. I could not accept the reality of my daughter’s passing and life became meaningless. Every day, I could do nothing but look at photos of my daughter. I tried to talk to her but never ever got a response. . . It was like being abandoned by the whole world. No one could really understand me at that moment.
Overpowering emotional loneliness emerged when Shidu parents realized that they had lost their only child, unbearable for someone in a society with such a strong familial culture.
Impaired romantic relationships and intimate loneliness
For some, the child’s death destroyed the very existence of their family and endangered their marriage. Fifteen participants confessed that their marriages were impacted to various degrees and four participants got divorced within 2 years of their child’s death. F11 confided, Our life was focused on our child before, but after his passing, we saw each other as different people and argued constantly. Communication with my husband was not possible, as any words relating to our child could trigger grief and arguments. . . I felt extremely lonely and suffered every moment in that period; who could you talk to when the most intimate person even abandoned you?
Difficult spousal relationships further aggravated feelings of emotional loneliness at this stage.
Social disconnection, self-alienation, and social loneliness
We found many Shidu parents experienced social exclusion at Stage 1 because of external social stigma and self-alienation. Nineteen participants said they were regarded as the “unlucky” person who brings “bad fortune.” To avoid such stigma, most participants stopped socializing altogether; four participants even moved homes.
Eighteen participants clearly stated that they did not have a confidant to share their feelings of grief with during that first year. They described this period as “desperate” and “isolating.” M6 shared, I stopped contact with relatives, friends, and colleagues during the first year of bereavement although, before, I was an extrovert. I was afraid of being scorned, despised, or irritating. Most of the time I just stayed at home and recalled memories of my deceased child. Life was about loneliness and despair.
Most participants reduced socializing due to perceived stigma and self-isolation, amplifying their feelings of social loneliness.
Stage 2: Life Restoration and Lessened Loneliness
Participants’ feelings of loneliness generally lessened after 2 years. Most participants gradually accepted their child’s death and tried to restore their lives, reconstruct their social network, and seek new meanings. This stage can last for a long time. Their feelings of loneliness were described as occasional, temporary, and contextual. For example, participants said, “On ordinary days I am fine, but I feel particularly lonely on special days or festivals, when I see other families together”; “Daytime is OK, but I often feel lonely late at night”; and “I do not allow myself too much free time as I will feel lonely if I am not occupied.” They identified several factors that reduce loneliness: having a positive outlook, a support network, better socioeconomic status, good health, and mutual support between couples. Three key strategies were found among the participants for life restoration and loneliness mitigation.
Reconstructing support networks
The first strategy was to build or repair support networks in three different ways. Twelve participants built up quasi-kinships, mainly interacting with other Shidu parents who shared similar experiences of loss. Five participants mainly repaired their relationships with relatives and previous friends. Eight participants adopted a more open strategy by both establishing new relationships with other Shidu parents and repairing previous social networks. Among these three subgroups, although the loneliness of participants from the first group initially lessened, they fell into another kind of social isolation. M22 confided, I felt inferior to others after my child’s death, and stopped speaking to friends and relatives. I joined an online group of Shiduer and have been interacting with them as we have similar sad memories and can understand each other. Indeed, initially, I felt relieved to share similar sad stories and travel together. It was good to have someone to talk to, someone that understands you. . . However, gradually, I felt people in this group were passive and paralyzed, and they never really recovered from grief and returned to normal life.
It is noteworthy that although most participants mentioned increasing social interaction at this stage, many kept a “safe distance,” finding it difficult to develop friends. Because of the stigma surrounding Shiduer, they still felt isolated from others. In addition, special family days (e.g., The Spring Festival, Mid-Autumn Day, the deceased child’s birthday and death day) triggered feelings of loneliness.
Seeking new meanings in life
The second strategy was to adjust social cognition by seeking new meanings in life. Seven participants had good relationship with their living parents and they refocused themselves to “live for their parents.” Other life purposes were described as “live for the deceased child” and “live for myself.” These brought Shidu parents a sense of self-efficacy and self-worth. New life meanings and endeavors distracted Shiduer from feelings of loneliness. F1 shared, Our generation generally had one child per family and that child is all our hope and life meaning. My life collapsed after my child’s death and I lost the point of living. Three years later, my mother was ill, and I had to look after her. I suddenly realized that I already have no hope or caregiver in my life, how could I bring the same suffering to my own mother? From then on, being a filial daughter and a good caregiver is my new life meaning. We moved in together and I have not been too lonely since then.
Enriching daily life
Third, participants distracted themselves from thoughts of loss by busying their schedules. Some participants developed interests or returned to old hobbies. Others, who had not yet retired, returned to work. Some, with better economic status, traveled to refresh their minds and find peace in nature. Such activities helped to distract Shidu parents’ from endless grief, leaving the space of loneliness. F16 confided, I tried to distract my grief by making a busy schedule. I entered the Senior’s college, learned dancing, and handcraft. And I did a lot of volunteering. My feelings of loneliness reduced with an increasing sense of life fulfillment. However, late at night, I still sometimes thought of my child and felt lonely every now and then. But comparatively, my mental status was much better than before.
In Stage 2, participants gradually restored their lives. Although participants still reported occasional, temporary, and contextual loneliness, the frequency and intensity of this loneliness were largely alleviated due to increased social connection, newly built life meaning, and enriched schedules.
Stage 3: Aging-Related Events/Issues and Renewed Loneliness
Stage 3 generally started when participants passed their mid-sixties. We found that loneliness at this stage increased with age. Three key factors could account for such changes.
Additional bereavement and reduced emotional support
Relationships were found to be crucial support resources for life restoration and loneliness relief among Shidu parents. With aging, however, chances of losing such bonds were higher. The loss of a spouse and other family members brings additional grief and results in reduced emotional ties. M17 described, This year, my child has left me for a whole decade. I spent three years getting used to the loss and restoring my life. There are a few years that I felt recovered from the distress and did not feel so lonely. But good times did not last long. My wife passed away last year and left me alone. I felt totally abandoned, and again started drowning in the feelings of loneliness.
In this study, six participants lost their spouses while nine experienced the death of a parent or close sibling. This additional bereavement rendered the already limited emotional support unavailable, restoring Shiduer’s loneliness.
Decreased self-efficacy and reduced social interaction
Self-efficacy is the belief that one can organize and execute certain actions toward a desired goal (Blazer, 2002). Along with aging, many participants reported decreased self-efficacy, saying “I am not able to do [something] after I entered old age” or “I cannot do [something] any longer because of aging.” They had to reduce socializing due to deterioration of physical health and memory loss. M22 described,
I am 70 this year. Before 65, I always traveled around with other Shidu parents . . .We spent months traveling, to escape distress and loneliness. Now I seldom do that, as I am older and have health problems. Last year I fell while getting off the bus and was hospitalized for half a month. Since then, I have minimized my outings.
For many participants aged 65 and over, daily activities were restricted to their homes, and their social networks, once again, shrunk, deepening their feelings of social loneliness. Loneliness was worse for participants who lived alone.
Deteriorated health, unmet care needs, and uncertain long-term care arrangements
In later life, participants were sick more frequently, experienced chronic illness, or often needed to visit a doctor or hospital. Their care-needs, while increasing, go untended because they have no children. Loneliness combined with helplessness emerged in this situation.
When talking about hospitalization, 11 participants sobbed. They described feeling “fearful,” “lonely,” and “helpless.” F21 said, My health is deteriorating, and I have to visit the hospital regularly. Most people my age have their children around to support. I feel extremely lonely and helpless every time I go to hospital and have no company. How I wish my child were by my side when I need her!
Those who were widowed, of low socioeconomic status, in poor health, lived alone, or experienced adverse life events reported more intense and frequent loneliness at this stage compared with their counterparts.
Discussion
This study investigated the loneliness trajectories among parents who have lost their only child in China. Overall, we found that participants’ perception of the frequency and intensity of loneliness observed three different stages of bereavement following a U-shape where loneliness declined from a peak level and then re-increased over time. Our results support existing findings about Shiduer’s vulnerable mental health (Wei et al., 2016; Yin et al., 2018; Zheng et al., 2017) and enrich this research by illustrating the staged development of loneliness with corresponding influencing factors for each stage.
In the first stage of severe grief, a good spousal relationship was a protective factor for intensive loneliness. Couples’ dyadic coping (constructive communication, emotion sharing, and joint problem-solving) was critical when they felt stigmatized and reluctant to socialize or receive external support (Bergstraesser et al., 2015; L. Chen, Fu, et al., 2019). Consistent with existing literature, we found that many Shiduer experience marital strain after child loss (N. Wang & Hu, 2019; Zheng et al., 2017), thus increasing their mental health vulnerability and need for support.
In the second stage, participants gradually start to restore their lives. With constant cognitive adjustment and increasing social interaction, most participants perceived loneliness at this stage as occasional, temporary, and contextual. Following previous research (Warner et al., 2019), kinship networks and self-support groups help alleviate loneliness. Notably, building a relationship with a Shidu self-support group only may not be the ultimate long-term solution for social isolation and loneliness. While Shidu self-support groups provide emotional support, they also constantly trigger grief in Shidu parents (N. Wang & Hu, 2019). This study found that a robust social network for Shiduer should include a self-support group and other kinship and friends (Stemen, 2020).
Stage 3 generally started when participants encountered aspects of vulnerability due to aging. It is well-recognized that loneliness increases with older age, due to deteriorating health, shrinking social network, and loss of contacts (Blazer, 2002; Cohen-Mansfield et al., 2009; Victor & Bowling, 2012). This is consistent with the social loneliness experienced by our older Shiduer participants caused by decreased self-efficacy and reduced social interaction. However, emotional loneliness among older Shiduer was specifically related to their child’s death. Experiencing additional bereavement and struggling with old age care constantly reminded them of their deceased child, triggering feelings of familial deficiency. Thus, emotional loneliness was awakened and reinforced at this stage. Here, it seems that older Shidu parents may be more vulnerable to loneliness than older adults generally. Socioeconomic status was also found to be an important insulating factor allowing some participants to access additional resources as they age. Therefore, older Shiduer with lower socioeconomic status may be particularly vulnerable at this stage.
Our findings support many existing studies on bereavement, aging, and loneliness (Fried et al., 2015; Grenade & Boldy, 2008; Hazer & Boylu, 2010; Utz et al., 2014; Victor et al., 2005). However, we have investigated the staged characteristics of loneliness in Chinese Shiduer, distinct manifestations and triggers of loneliness, and the need for staged support. Our results indicate that policymakers and practitioners should consider specific loneliness characteristics at different stages and design tailored and effective interventions.
Policy and Clinical Implications
Although experiences of loneliness are distinctly heterogeneous among Shidu parents, our sample reflects clear staged characteristics of loneliness trajectories. Based on our findings, we suggest that the assessment of loneliness stages should be conducted before specific interventions. Attention should be given to clients’ primary needs and preferences when designing staged interventions.
First-stage interventions should focus on treatment that helps Shiduer adjust to grief and improves communication skills between spouses and family members (Biegel, 1985; Riches & Dawson, 1996). Free psychological counseling services should be available for Shiduer to help them cope with potential mental crises and enhance communication with family members. Special attention should be paid to those without partners or who are living alone.
In Stage 2, effort should be focused on helping them reconstruct their wider social network, improving their social skills, rebuilding life’s meaning, and improving community engagement (Biegel, 1985; Riches & Dawson, 1996). Social workers could lead groups to help Shidu parents reconstruct varied social connections and the community should provide amenities that promote social interactions among Shiduer. Consultation services should be considered to help prepare Shiduer for old age. Furthermore, community social workers should consider visiting Shidu parents on festival days.
Interventions for the third stage should focus on age-related issues (e.g., medication, hospitalization, daily care, bereavement support, help moving into care homes) and provide more social support (L. Chen, Song, & You, 2019; G. Wang et al., 2011). Special attention should be paid to those who are widowed or divorced, have bad health, low income, or a weak support network. Measures such as special assistance for hospital visits and general volunteer programs should be introduced and the most vulnerable Shiduer individuals identified.
Limitations
There are several limitations to this study. First, we only interviewed urban participants who did not have subsequent children or any grandchildren. Therefore, our results may not apply to rural Shiduer, or those who gave birth to/adopted another child or had grandchildren. Second, participants were recruited based on reporting loneliness previously, thus we did not cover Shiduer experiencing less loneliness or who may have developed resilience. This group needs attention in future investigations. Third, we studied loneliness trajectories through retrospective in-depth interviews, rather than following each participant at different stages of their bereavement. Some participants might forget or hide distressing experiences to avoid additional pain, causing potential research bias (Rokach & Brock, 1997). Future studies should consider extending their research focus and including a wider range of participants. Longitudinal studies could track Chinese Shidu parents’ mental health over time.
Conclusion
This study is among the first to focus on loneliness trajectories, giving suggestions for staged interventions for Chinese Shiduer, an aging social group that desperately needs support. It provides insight into different stages of loneliness experienced by Shiduer, and their specific staged needs. These have important policy and practical implications. Our findings may also be relevant in social contexts for long-term intervention in other groups who experience loneliness.
Supplemental Material
sj-pdf-1-jag-10.1177_0733464820978808 – Supplemental material for Loneliness Trajectories: Evidence for Staged Intervention Among Chinese Bereaved Parents
Supplemental material, sj-pdf-1-jag-10.1177_0733464820978808 for Loneliness Trajectories: Evidence for Staged Intervention Among Chinese Bereaved Parents by Ning Wang and Qian Hu in Journal of Applied Gerontology
Footnotes
Acknowledgements
The authors acknowledge all research participants for their contribution to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Social Science Foundation Youth Project under Grant 18CSH037, Shanghai Pujiang Program under Grant 2020PJC023, and Guangzhou University Talents Cultivation Funding (RP2020009).
Ethics Approval
The study design was approved by the ethics review board of School of Public Administration at Guangzhou University. Ethics Approval Number PAS1901-05.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.