
Abstract
Based on information 11,408 university students provided on perpetration of physical assault in a romantic relationship, they were classified into three Dyadic Concordance Types (DCTs). We then examined six risk factors drawn from previous literature of partner violence: physical abuse as a child, antisocial personality characteristics, alcohol abuse, coercive control, chronic denigration in a relationship, and patriarchy at the societal level. We hypothesized that some risk factors for assault are different dependent on the DCT. Using multinomial logistic regression, we found that some risk factors were associated with an increase in the risk of a couple being in the Male Only assaulted DCT more than the other two DCTs (e.g., men who were high in antisocial personality characteristics). Other risk factors were found to be associated with a greater increase in the risk a couple being in the Both assaulted DCTs (e.g., chronic denigration). These results suggest that theories about the etiology of partner violence should take into account whether the couple is Male Only, Female Only, and Both assaulted. Identification of the DCTs of cases can be helpful in focusing research, treatment, and prevention of partner violence in a way that better reflects the actual situation.
Studies of the etiology of partner violence (PV) have almost always focused on assault by one of the partners, either the male or the female partner, although some now investigate bidirectional assault. Attention to bidirectional assault is a major step forward because a review of 48 studies found that it is characteristic of the majority of PV cases (Langhinrichsen-Rohling, Selwyn, & Rohling, 2012) and that this applies regardless of whether the data were provided by the male or female partner, or by children reporting violence between their parents (Straus, 2015; Straus & Michel-Smith, 2014). As important as it is to distinguish bidirectional assault from sole-perpetrator assault, an additional specification is needed to categorize PV in heterosexual relationships. Studies that distinguish between Perpetrator-Only, Victim-Only, and Perpetrator-Victim, such as Dixon, Edwards, and Gidycz (2016) and Melander, Noel, and Tyler (2010), ignore an important aspect of a relationship which is central to almost all theories and treatment of PV: the gender of the actors.
The research reported in this article provides the necessary gender specification by the use of Dyadic Concordance Types (DCTs; Straus, 2015). DCTs classify couples in which violence has occurred into three categories: Male Only, Female Only, and Both assaulted. DCTs therefore identify both (a) the cases to theorists and clinicians whose primary concern is violence against women and also identify (b) cases to theorists and clinicians whose primary concern is understanding and treating PV as a dyadic problem. DCTs are both a mode of conceptualizing PV at the dyadic level, and a typology or measure to operationalize that conceptualization. Further information on the both the conceptual and measurement aspects of DCTs can be found in other articles on this typology (Rodriguez & Straus, 2016; Straus, 2015).
Basing the conceptualization and analysis on DCTs rather than on individual perpetrators is consistent with one of the general objectives of the study, which is to add to the understanding of PV as a couple-level phenomenon. A second and more specific objective is to present results of the net effect of six indicators of the most widely discussed theories of PV. This is in contrast to studies that tested each of them separately. The third objective is to present results which examined gender as an empirically measured variable. This is in contrast to most of the research on risk factors for PV which often investigated risk factors for perpetration by men but not by women. The common failure to take gender into account is indicated by the meta-analysis of 25 risk factors by Stith, Smith, Penn, Ward, and Tritt (2004), which only found sufficient empirical studies to compare men and women on only a single risk factor.
Literature Review
Diversity of PV
It is increasingly recognized that PV is not a unitary phenomenon. This diversity needs to be taken into account to formulate more adequate theories about the causes of PV. Several modes of differentiating between types of PV have contributed to this end. One of the earliest differentiates between less severe attacks (e.g., slapping and throwing things at a partner) and severe assaults (e.g., choking, and attacks with objects that could injure a partner; Straus, 1979). This important difference parallels the legal distinction between simple and aggravated assault. Another typology distinguishes between Generally Violent/Antisocial, Dysphoric/Borderline, and Family-Only perpetrators (Holtzworth-Munroe, Meehan, Herron, Rehman, & Stuart, 2000). A typology of much current interest distinguishes between Common Couple violence and Intimate Terrorist relationships (Johnson, 2008).
Each of these typologies has important limitations. For example, the Intimate Terrorist type, despite what the name suggests, does not classify cases on the basis of the severity, chronicity, or injury. Johnson (2008) explicitly argues “ . . . the frequency and severity of the violence has no bearing whatsoever on whether the violence is classified as IT” (p. 94). Rather, it is based entirely on whether one partner tries to exercise a high level of coercive control. Given the limitations of existing typologies, there is a need for additional ways to distinguish between the many ways in which PV occurs: one of which may be the DCTs identified previously, and in more detail below.
DCTs
DCTs are both a conceptual framework and a measurement method. The three DCT categories of Male Only, Female Only, and Both assaulted measure a key characteristic of couples: concordance in perpetration of a behavior of interest, in this case assault. DCTs are an emergent characteristic of a relationship because it is a characteristic that does not exist until the partners interact. It is unknown to the researcher or practitioner unless steps are taken to identify this emergent characteristic of a couple. Fortunately, the first step in research is very simple in a heterosexual relationship: cross-tabulate assault by the male partner with assault by the female partner. Three of the resulting four cells identify the Male Only, Female Only, and Both assaulted DCTs, and the fourth is the reference category of Neither. DCTs do not replace the basic data on assaults by a male partner and by a female partner.
In clinical work, if the presenting offender or the presenting victim is asked about violence by both his or her own violence and that of his or her partner, it almost automatically provides an initial identification of which of the three DCTs applies. This permits a clinician to take this into account in developing a treatment plan. Thus, in addition to dealing with the behavior of each partner as individuals, DCT provide a practical way for both practitioners and researchers to address PV as a couple-level problem.
DCTs are also a conceptual methodological advancement over measuring gender “symmetry” in perpetration. It is advancement over symmetry because approximately equal rates of perpetration by males and females can exist simultaneously with 0% in the Both DCT. This could occur if a study found 12% of men and 12% of women assaulted their partner, but in each case their partner was not violent. In this situation, there would be no cases in which both partners assaulted despite the gender symmetry in PV perpetration of the overall sample. A key point is that DCTs identify perpetration by partners in the same relationship.
Identification and Analysis of DCTs
Any existing measure of PV that a research finds appropriate for study can be used to identify DCTs. If the instrument asks only about the behavior of one partner, dyadic data can be obtained by reusing the same instrument with the referent person as the other partner. Two widely used measures of PV, the Conflict in Adolescent Dating Relationships Inventory (Wolfe et al., 2001) and the Revised Conflict Tactics Scales or CTS2 (Straus, Hamby, Boney-McCoy, & Sugarman, 1996; Straus, Hamby, Finkelhor, Moore, & Runyan, 1998), are inherently dyadic because they ask the respondents about both their own behavior and that of their partner. The short form of the CTS2 (Straus & Douglas, 2004) takes only 3 to 5 min to administer and also provides the data necessary to identify DCTs for assault and four other abusive behaviors: injury, intransigence, denigration of a partner, and sexual coercion.
Risk Factors Investigated
The six risk factors were selected because each has been included in previous theories about the etiology of PV: physical abuse as a child, antisocial personality characteristics, alcohol abuse, coercive control, chronic denigration in a relationship, and patriarchy at the societal level. Although previous research has shown the relation of these risk factors to PV (Charles, Whitaker, Le, Swahn, & DiClemente, 2011; Medeiros & Straus, 2006), there is a need for information on whether each risk factor applies to the Female Only, Male Only, and Both DCTs.
For example, most research on the relation of coercive control to PV examined the extent to which the male partner was controlling and violent. However, studies which measured coercive control for both partners have found a similar level of coercive behaviors by female and male partners. In addition, the relation of coercive control to physical assault is also similar for both men and women (Bates, Graham-Kevan, & Archer, 2014; Black et al., 2011; Felson & Outlaw, 2007; Karakurt & Cumbie, 2012; Laroche, 2005; Straus, 2008). Based on these studies, our hypothesis is that coercive control is related not only to couple being in the Male Only assaulted DCT, but to Female Only, and Both assaulted couples, although not necessarily to the same extent. By extension, such may also be the case for the other risk factors included in this study as well, where a particular risk factor may have different relations to the different DCTs.
Theoretical Basis of DCTs
The theoretical basis of DCTs is general systems theory (Buckley, 1967; Von Bertalanffy, 1967) and more specifically family systems theory (Broderick, 1993). A basic assumption is that the whole is more than the sum of the parts. More specifically, families as social systems have distinctive characteristics that need to be measured and examined in addition to the characteristics of the individual members. The same applies to family subsystems, such as husband–wife, parent–child, and sibling dyads. As indicated above, DCTs for married and dating couples are a measure of the couple per se that is in addition to the characteristics of the partners used to measure the categories making up the DCT. Couples, like individuals, have distinctive characteristics and ongoing behavioral patterns that need to be taken into account.
The measurement benefit of also using a couple-level measure, such as the DCTs, is illustrated by comparing hypothetical two couples. In both, the husband often loses his tempter and hits his wife. In one couple, however, the wife also often loses her temper and hits her husband. The characteristic of the male partner in both of these couples is the same, but the nature of their relationships is likely to be very different. For example, research shows that when both partners assault each other, the probability of injury is much higher than if only the male partner assaults or only the female partner assaults (Straus & Gozjolko, 2014; Whitaker, Haileyesus, Swahn, & Saltzman, 2007). Similarly, examining the effect of low self-control by men and low self-control by women may miss this couple-effect because they are not likely to look at the interaction of the two that is identified by DCTs.
These unique couple effects are shown by studies that found that each DCT category has different consequences. These include studies of depression by each partner (Straus & Winstok, 2013) and of criminal behavior by adults who were exposed to each dyadic type of violence between their parents as children (Straus & Michel-Smith, 2012). Studies that have measured sexual coercion by both partners have found only slightly higher perpetration by male than female partners (Turchik, Hebenstreit, & Judson, 2016). For example, Straus and Kemmerer (2015) found that verbal sexual coercion was perpetrated by 29% of men and by 21% of women in the previous 12 months, and physical sexual coercion by 2.4% of men and 1.8% of women. They also found that the relation of sexual coercion to relationship distress depended on whether the coercion was Male Only, Female Only, or by Both.
Independent Effects of Each Risk Factor
Not only is PV diverse in the way it takes place, research has suggested a diversity of causes of PV. This etiological diversity is illustrated by the 18 empirically established risk factors listed by the World Health Organization (Krug, Dahlberg, Mercy, Zwi, & Lozano, 2002) and the 31 risk factors listed by the U.S. Centers for Disease Control and Prevention (Centers for Disease Control and Prevention & National Center for Injury Prevention and Control, 2006). The six risk factors examined by the current study are in one or both of those lists. However, the empirical evidence used to compile the two lists rarely took into account whether each risk factor applied to perpetration by women as well as men, or the extent to which the risk factors co-occur. The current study took both those issues into account by including gender and all six risk factors in the same model.
Gender Differences in Risk Factors
As indicated previously, only a few studies have examined the extent to which each risk factor applies to assaults by women as well as men. The available research that compared gender differences tended to find parallel gender effects for most risk factors. For example, the National Family Violence Survey found that 16 of the 17 risk factors investigated were associated with assaults by female as well as by male partners (Straus, Gelles, & Steinmetz, 1980/2006). A study of 36,861 U.S. Air Force (USAF) members and their civilian partners investigated 26 risk factors and found that 22 of the 26 were significant for both men and women. Two of the six risk factors in the current study were also examined by those two studies (coercive control and alcohol abuse; Slep, Foran, Heyman, Snarr, & USAF Family Advocacy Research Program, 2014). This provides a basis for hypothesizing that the six in the current study will be risk factors for perpetration by both men and women.
Method
The data for this study were obtained as part of the International Parenting Study (IPS). They were gathered by a consortium of researchers located in 15 nations between October 2007 and March 2010. Each IPS consortium member used the same core questionnaire, except for the final section, which was reserved for each member to add questions about issues of specific local or theoretical interest. A description of the study, including the questionnaire and all other key documents, can be downloaded from http://pubpages.unh.edu/~mas2.
The procedures for the IPS were reviewed and approved by the University of New Hampshire Institutional Review Board and by the equivalent board or administrator at each of the 31 participating universities. Collectively, the sites represent four regions of the world: Asia, Europe, North America, and Israel. Participation was restricted to students age 18 or older. Potential participants read a consent form that stressed that participation was entirely voluntary and that they were free to not answer any question they chose to omit. Steps were taken to ensure the privacy and anonymity of the data. The recruitment strategy and questionnaire format varied by site, but the majority of students were recruited in class (71%) and completed a paper version of the questionnaire (75%). After completing the questionnaire, participants received a debriefing form explaining the purpose of the study and a list of mental health referrals.
Participants
The sample consists of 11,408 students in 15 nations, but subsequent analyses have fewer cases because of missing data (n = 8,649). A total of 2,117 students reported never being part of a romantic relationship during the reference period, which excluded them from our analysis. The remaining small proportions of dropped cases result from skipping one or more questions used to construct our variables in the multivariate analysis.
Seventy percent of the total sample were women, which may be reflective of the general gender composition of the psychology, sociology, nursing, education, family studies, and social work courses from which most of the participants were recruited. The age of the total sample ranged from 18 to 40 (M = 21, SD = 3.93). Despite the skewed distribution of age, 89% of the sample was under the age of 25 which corresponds with college student population. The overwhelming majority were undergraduate students as only three universities also surveyed graduate students. Ninety percent of the sample reported being born in the country of data collection, and 80% self-identified as belonging to the majority racial or ethnic group.
Ninety-six percent of the students reported on both biological parents. Their parent’s educational attainment level tended to be high: 43% of fathers and 41% of mothers completed a college degree. Employment status was 93% of fathers worked full time, but only 55% of mothers worked full time outside the home. A table giving these and other characteristics of the sample for each of the 15 nations is in Straus and Michel-Smith (2014). This article focuses on the overall pattern found for the issues investigated. National context differences were not addressed because of sample size problems when the analysis is on the subgroup in each nation who assaulted and on categories within that subgroup, and because of the limited length permitted for a journal article. An example of results by nation for this sample is Straus and Michel-Smith (2014).
Measure of Physical Assault
Violence in the dating relationship of the student during the preceding 12 months was measured by the short form of the CTS2 (Straus & Douglas, 2004). In the past 40 years, the CTS has been used in more than 500 studies in more than 50 other countries. The CTS has demonstrated cross-cultural reliability and validity (Archer, 1999; Straus, 1990, 2004, 2012; Straus & Mickey, 2012). The items and psychometric data are available in Straus et al. (1996). The short form has been shown to have high validity but tends to underestimate prevalence (Straus & Douglas, 2004). Thus, the rates to be presented are lower bound estimates.
The physical assault scale has one item to measure “minor” violence (“pushed, shoved, or slapped partner”) and one to measure more “severe” violence (“punched or kicked or beat-up partner”). If a participant reported having done one of these behaviors in the past 12 months, they were classified as having assaulted, irrespective of the frequency or the severity of their assault. The alpha coefficient of internal consistency for data provided by men = .81, by women = .76, and by total sample = .81.
DCTs for physical assault
The CTS can be used to identify DCTs because it asks study participants about both their own behavior and that of their partner. By cross-classify assault by the respondent with assault by the partner, the resulting four cells identify the three DCTs, Male Only, Female Only, Both, and the reference category, Neither.
However, using data on both partners provided by one of them means that the degree of agreement between partners could not be investigated. A few studies have compared data from each partner. They found that strong agreement on prevalence (whether violence occurred) but little agreement on chronicity (how often) it occurred (Fritz, Slep, & O’Leary, 2012). They do not provide empirical evidence or conclusions about which is better, except to recommend using the data provided by the partner who disclosed more.
Risk Factor Measures
Physical abuse as a child
This was measured using the severe assault scale of the Parent–Child Conflict Tactics Scales or CTSPC (Straus et al., 1998). Respondents were asked about their childhood experiences retrospectively using age 10 as a reference age. Although each question was asked separately for mothers and fathers, the mother and father behaviors were combined for purposes of this study. Age 10 was chosen because corporal punishment is still prevalent and it is also an age when children are old enough to remember and describe incidents.
The five CTSPC items asked how often each parent (a) “hit you with a fist or kicked you hard”; (b) “grabbed you around the neck and choked you”; (c) “beat you up, that is, hit you over and over as hard as they could”; (d) “hit you on some other part of the body besides the bottom with something like a belt, hairbrush, a stick, or some other hard object”; and (e) “threw or knocked you down.” The response categories for this scale are as follows: N = this never happened; 0 = not in that year, but it happened before or after; 1 = once in that year; 2 = twice in that year; 3 = 3 to 5 times in that year; 4 = 6 to 10 times in that year; 5 = 11 to 20 times in that year; and 6 = more than 20 times in that year. Despite the measurement of frequency, this study used a dummy indicator of if the respondents have ever experienced one of the five child abuse items by one or both of their parents. The alpha coefficients of internal consistency for this sample are as follows: men = .90, women = .83, and total = .87.
Measures from the Personal and Relationships Profile (PRP)
The PRP measures 25 risk factors for PV. Information on the instrument as a whole and the development of each scale is in the test manual (Straus, Hamby, Boney-McCoy, & Sugarman, 2010) and other publications (Medeiros & Straus, 2006; Straus & Mouradian, 1999). This section therefore presents only a brief description of the scales used for this study. The PRP scales are typically eight items. However, because of space limitation in the IPS questionnaire, versions using fewer items were used.
The response categories for all scales are as follows: 1 = strongly disagree, 2 = disagree, 3 = agree, and 4 = strongly agree. If an item is reverse scored, an (R) is shown. Given somewhat lower levels of alpha coefficient for some of our subscales, we used confirmatory factor analysis and used the factor scores for all of the following subscales. From those factor scores, we created a dummy variable for the highest quintile within our sample for ease of interpretation. The only exception is the following measure for coercive control, which we took the highest decile of the factor score.
Antisocial personality characteristics
This is a five-item scale with the following items: “I feel sorry when I hurt someone (R),” “I often do things that other people think are dangerous,” “I don’t think about how what I do will affect other people,” “I often lie to get what I want,” and “I have trouble following the rules at work.” The alpha coefficients of reliability for this sample are as follows: men = .61, women = .58, and total = .62.
Alcohol abuse
This was measured using the following three items: “I worry that I have an alcohol problem”; “When I am drinking, I usually have five or more drinks at a time”; and “Sometimes I can’t remember what happened the night before because of drinking.” The alpha coefficients of reliability for this sample are as follows: men = .71, women = .74, and total = .74.
Coercive control
This measure of coercive control of one’s partner in the relationship was measured using two items from the Hamby Dominance Scale (Hamby, 1996): “My partner needs to remember that I am in charge” and “I generally have the final say when my partner and I disagree.” Consistent with research on Cronbach’s alpha with few items (Cortina, 1993), the alpha coefficients of reliability for this scale are low: men = .47, women = .43, and total = .44. Despite the low alpha coefficients, we found that these two items loaded well on a single factor, similar to the other scales.
Chronic denigration in a relationship
This was measured by the Psychological Aggression scale of the CTS short form (Straus & Douglas, 2004). Study participants were asked how often during the past year they had insulted or swore or shouted or yelled at their partner, and how often they had destroyed something belonging to their partner or threatened to hit their partner. These two questions were repeated for the behavior of the partner. The midpoint of each response category was used to calculate the frequency of psychological aggression. The scores ranged from 0 to 50 (M = 2.52, SD = 5.45). Because denigration is so prevalent, we used chronic denigration as the risk factor to investigate, as measured by the participant with scores at or above the 80th percentile. The alpha coefficient of internal consistency for data provided by men = .71, by women = .69, and by total sample = .70.
Gender Inequality Index (GII)
This scale indicates the degrees of male dominance in the nation where the study was conducted. The scale was developed by the United Nations as part of the Human Development Reports (Gaye, Klugman, Kovacevic, Twigg, & Zambrano, 2010). The GII ranges from 0 to 1, with 1 being the highest level of inequality. For the following analysis, a dummy variable was constructed to indicate five of the 15 participating nations of the IPS with the highest level of gender inequality: Greece (.14), Israel (.14), Poland (.14), the United States (.26), and Russia (.31).
Control Variables
Socially desirable responding
This was measured by a six-item version of the Reynolds Social Desirability Scale (Reynolds, 1982). The six items were chosen to represent diverse behaviors: “I sometimes try to get even rather than forgive and forget (R),” “No matter who I am talking to I am always a good listener,” “I sometimes feel resentful when I don’t get my way (R),” “I’m always willing to admit it when I make a mistake,” “There have been times when I was quite jealous of the good fortune of others (R),” and “I am always courteous, even to people who are disagreeable.” R indicates reversed scoring. The response categories are as follows: 1 = strongly disagree, 2 = disagree, 3 = agree, and 4 = strongly agree. The alpha coefficients of reliability for this sample are as follows: men = .50, women = .58, and total = .56. Although these low coefficients are expected given the diverse set of behaviors of this scale, they nonetheless loaded on a single factor reliably. We have decided to use the raw factor score as our control.
Nation
This is a variable that coded all 15 participating nations of the IPS: Belgium, Canada, Greece, Hong Kong, Italy, Israel, Norway, Poland, Russia, Scotland, Slovenia, Spain, Switzerland, Taiwan, and the United States. The sample size greatly varies from nation to nation (see table in Straus & Michel-Smith, 2014). We controlled for the nation of the participant so that nations with large sample size do not have undue influence in the model.
Participant age and paternal education
These were controlled in our model because they both have been shown by previous studies to be related to both the risk factors and PV and therefore could result in spurious relationships (Suitor, Pillemer, & Straus, 1990). Participant age is a continuous variable. Paternal education, on the contrary, is a dummy variable indicating whether the participant’s father received college-level education.
Data Analysis
Multinomial logistic regression was used to estimate the degree to which each of the risk factors was associated with a different DCT. Multinomial logistic regression is designed for a categorical dependent variable to compare the effects of the independent variables favoring a particular outcome, in this case, Male Only, Female Only, or Both assaulted, compared against the reference base category, Neither assaulted. In multinomial logistic regression, the relationship is presented as a relative risk ratio (RRR). It is mathematically similar to an odds ratio (OR), except an OR is only calculated for one outcome against one reference category. RRR, on the contrary, is calculated for each outcome against the same reference category. All analyses were conducted using STATA 14.1.
Results
Individual and Couple Rates of Partner Assault
Among male students, 14% had physically assaulted their partner during the year covered by this study, compared with 18% of women, F(2701, 6755) = 0.58, p < .001. The similar rates of perpetration by men and women are consistent with more than 200 other studies (Desmarais, Reeves, Nicholls, Telford, & Fiebert, 2012). The past-year prevalence rate of any physical assault reported at the couple-level was 17%. This is much lower than the sum of the male and female rates because of the high rate of bidirectional assault in a given couple. It is important to note that these percentages are prevalence rates of the overall sample and are not the proportion of each DCT.
Figure 1 shows the percentage in each DCT. It can be seen that, according to both the men and the women in this study, about half of couples who had experienced violence were in the Both assaulted DCT. This result is consistent with a review of 48 studies of PV (Langhinrichsen-Rohling et al., 2012). Figure 1 is also consistent with studies that reported results on the percentage in each DCT separately for male and female study participants such as the U.S. National Comorbidity Survey (Kessler, Molnar, Feurer, & Appelbaum, 2001) and the World Mental Health Survey (Miller et al., 2011). See Straus (2015) for the percentages found by these other studies.
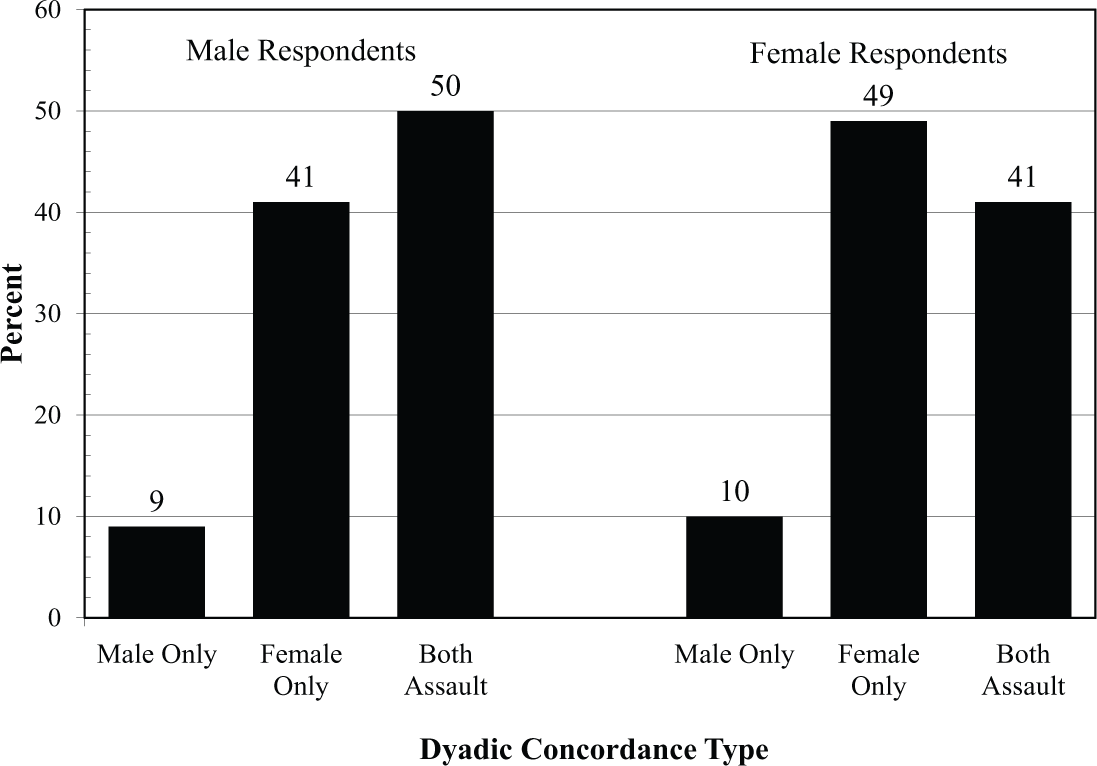
Concordance between partners in physical assault as reported by men and women.
Gender Differences in Risk Factors for Partner Assault
Table 1 shows both similarities and differences between men and women in the extent to which they are characterized by the six risk factors examined in this study. Compared with women, the percentage of men in our sample were more likely to be physically abused by one or more of their parents at age 10, F(3426, 7928) = 1.33, p < .001; more likely to exhibit antisocial personality characteristics, F(3426, 7928) = 1.83, p < .001; more likely to abuse alcohol, F(3426, 7928) = 1.44, p < .001; more likely to be controlling, F(3268, 7601) = 1.64, p < .001; and more likely to reside in nations characterized by a higher level of gender inequality, F(3426, 7928) = 0.94, p < .05. However, there was no significant difference between men and women who were in a relationship characterized by a high level of chronic denigration, F(3426, 7928) = 0.99, p = .80.
Gender Differences in Risk Factor Prevalence.
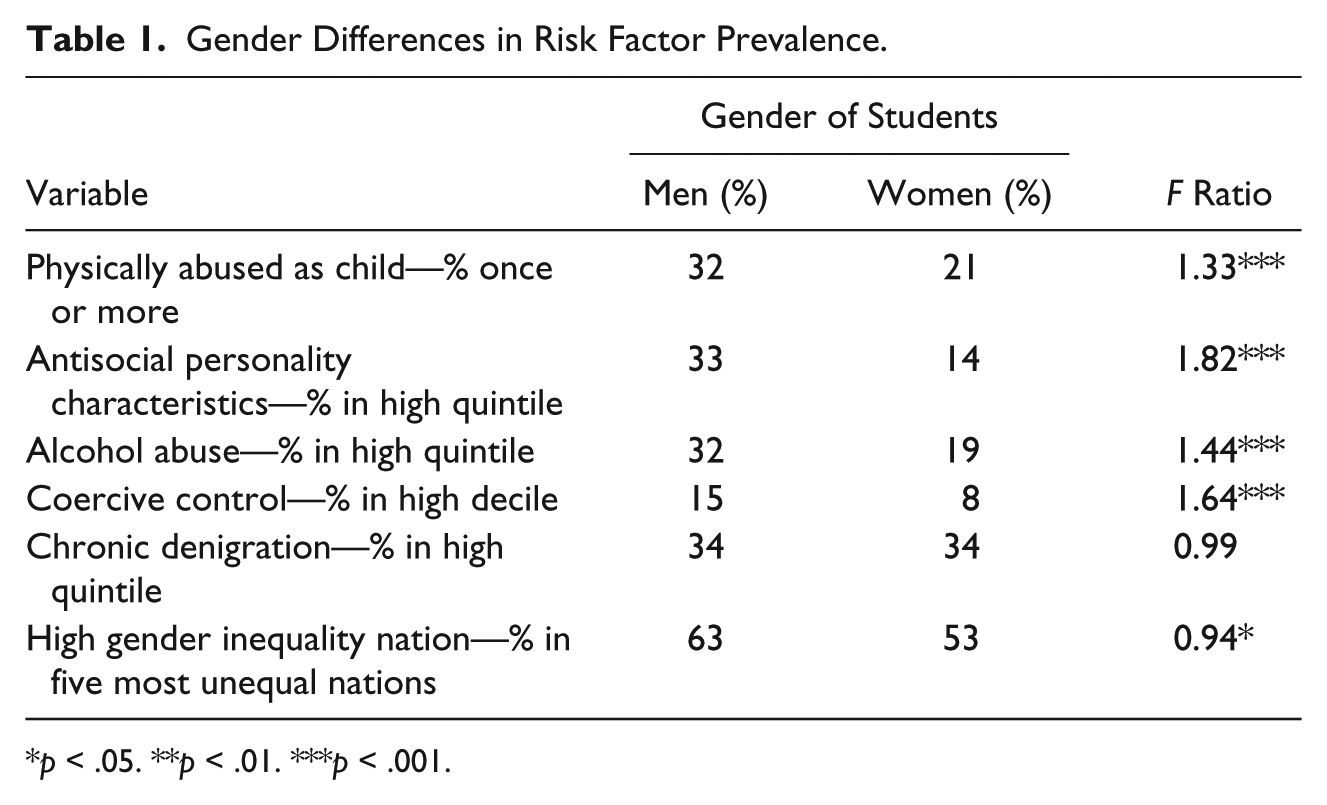
p < .05. **p < .01. ***p < .001.
Relation of Each Risk Factor to Dyadic Concordance in Assault
Table 2 and Figure 2 summarize the results of the multinomial logistic regression analysis. Table 2 provides RRRs with the 95% confidence interval (CI), and Figure 2 provides adjusted marginal plots created with STATA. For each risk factor, the results show the RRR net of the other five risk factors and the covariates used as controls.
Relation of Six Variables to a Couple Being in Each Dyadic Concordance Type of Physical Assault.

Note. Controls in the model (i.e., the nation, father’s education, age, social desirability scale) are not shown but included. RRR = relative risk ratio; CI = confidence interval.
p < .05. **p < .01. ***p < .001.

Relations of dyadic concordance in six risk factors to partner assault.
Child abuse
Experiencing physical abuse as a child was associated with a greater risk of all three DCTs of assault for both men and women, which indicates that they are likely to be in a relationship in which one or both partners had engaged in PV. The greatest risk for DCT due to child abuse was Both DCT for both men, RRR = 4.5, 95% CI = [3.1, 6.5], p < .001, and women, RRR = 2.1, 95% CI = [1.6, 2.6], p < .001.
Antisocial personality characteristics
Antisocial personality characteristics were associated with a higher risk for DCTs for men than women. For men who exhibited high levels of antisocial personality characteristics, this increased the risk of PV. This increase in risk is reflected by the Male Only DCT, RRR = 2.4, 95% CI = [1.1, 5.3], p < .05, and Both DCT, RRR = 2.0, 95% CI = [1.4, 3.0], p < .001. For women with higher levels of antisocial personality characteristics, they were only more likely to be Both DCT, RRR = 1.7, 95% CI = [1.3, 2.2], p < .001, where both partners engaged in PV.
Alcohol abuse
Alcohol abuse was only associated with an increased risk of being in a couple characterized by PV for women. Women who reported high levels of alcohol abuse were more likely to be Female Only DCT, where they are the sole perpetrators, RRR = 1.7, 95% CI = [1.3, 2.1], p < .001, and Both DCT, where they and their partner both engaged in PV, RRR = 1.8, 95% CI = [1.4, 2.3], p < .001.
Coercive control
Men who exhibited high levels of controlling characteristics were more likely to be in a relationship characterized by PV, as they were at higher risk for all three DCTs. Coercive men were most at risk for being the sole perpetrator of PV in the relationship, reflected by the Male Only DCT, RRR = 2.8, 95% CI = [1.3, 6.3], p < .05. Controlling characteristics in women, on the contrary, were only associated with DCTs, where they perpetrated PV, Female Only DCT, RRR = 1.7, 95% CI = [1.3, 2.3], p < .001, or Both DCT, RRR = 1.9, 95% CI = [1.4, 2.6], p < .001.
Chronic denigration
Respondents whose relationship was characterized by high levels of chronic denigration were at significant risk for all three DCTs. The greatest increases were in the risks for Both DCTs, where both partners would perpetrate PV. This was true for both men, RRR = 16.2, 95% CI = [11.2, 23.4], p < .001, and women, RRR = 16.6, 95% CI = [13.1, 21.0], p < .001.
National context of gender inequality
Compared with men who did not live in nations which had higher levels of gender inequality, men who lived in a more male-dominant society were only at a higher risk of Both DCT, where both partners engaged in PV, RRR = 1.8, 95% CI = [1.1, 2.9], p < .05. On the contrary, women who lived in a more male-dominant society were at risk for being in a relationship characterized by PV for all three forms of DCTs: Male Only DCT, RRR = 1.6, 95% CI = [1.0, 2.5], p < .05; Female Only DCT, RRR = 1.4, 95% CI = [1.1, 1.7], p < .01; and Both DCT, RRR = 1.5, 95% CI = [1.1, 1.9], p < .01.
Discussion
The hypothesis that each of the six risk factors for violence is associated with a greater risk of some DCTs of assault than others was found for all six risk factors. Although the size of the relationship differed, we found that two of the six risk factors (physically abused as a child and being in a relationship characterized by chronic denigration) were related to all three DCTs. Therefore, according to the results of this study, these risk factors apply for both men and women. Thus, if either partner had been abused as a child or were in a relationship characterized by chronic denigration, it was associated with an increased probability of all three DCTs. This result is consistent with studies, including longitudinal studies, which found that denigration of a partner (usually called psychological abuse) is an important risk factor for physical assault (Murphy & O’Leary, 1989; O’Leary & Woodin, 2009; Salis, Kliem, & O’Leary, 2014).
For three risk factors, the relationships were different for men and women. One of these, antisocial personality characteristics of male respondents, was related to an increased risk of a couple being in the Male Only or Both assaulted DCTs. However, antisocial personality characteristics of female respondents were only associated with an increased risk of Both assaulted DCT. Another gendered pattern is the risk of PV for students who reside in a nation characterized by higher level of gender inequality. For women, we found a small but nonetheless statistically significant increase in their risk of all three DCTs of assault. This was not true for men in the sample, as they were only likely to be part of the Both assaulted DCT. Finally, the multivariate analysis found no relation of alcohol abuse to partner assault by men. This is in contrast to the repeated finding of alcohol abuse being associated with an increased probability of men assaulting a partner (Foran & O’Leary, 2008; Kaufman Kantor & Straus, 1987). Bivariate correlation in Table 3 also found no statistically significant relationship between alcohol abuse and PV for the male students in our sample either. In a follow-up analysis not shown, higher level of alcohol abuse for the male respondents in our sample was correlated to never being in a relationship during the reference period. Therefore, it may be that the male students who drank heavily were excluded from our analysis for this reason.
Correlation of All Study Variables.
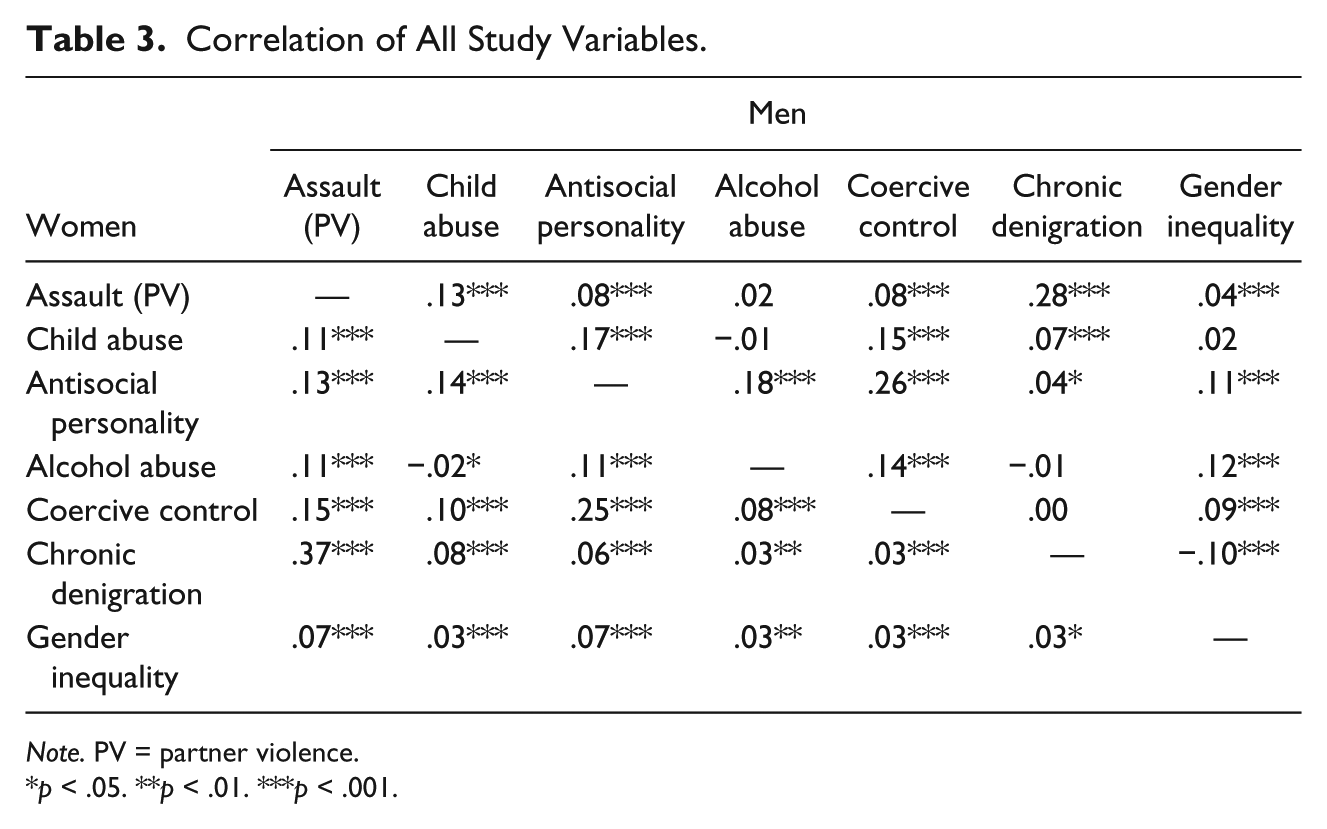
Note. PV = partner violence.
p < .05. **p < .01. ***p < .001.
Diversity
Previous research found that Both assaulted is the most prevalent DCT worldwide (Michel-Smith & Straus, 2014; Straus, 2015) and in the United States among all racial and ethnic groups for which DCTs have been identified (Charles et al., 2011; Field & Caetano, 2005). DCTs are also applicable to same-sex couples because the requirement that DCTs identify the role of each partner in the relationship is met using a role that is appropriate for the population or theory, such as older and younger partner. If no specific role is appropriate, same-sex couples can be classified as Partner A and B. Examples of DCTs among same-sex couples are in Langhinrichsen-Rohling et al. (2012) and Turchik et al. (2016). The large number of studies reviewed in these studies cited above and in Straus (2015) suggest that DCTs are applicable to our understanding and treatment of PV in diverse contexts such as socioeconomic status, race, ethnicity, language, nationality, sex, gender identity, sexual orientation, religion, geography, ability, and age.
Limitations
Cross-sectional
We believe that the results are consistent with causal relationships, but because the data are cross-sectional, they only show that the independent and dependent variables of this specific sample are related. To reflect that limitation, we used noncausal terminology such as “associated with” to describe the results. Nevertheless, some results are consistent with existing longitudinal studies, which is often used as a basis to argue causal pathways (Murphy & O’Leary, 1989; Salis, Salwen, & O’Leary, 2014).
Convenience samples of student couples
Although dating couples are a minority of all couples, studies of risk factors for PV conducted with student couples and with general population household samples tend to find similar results. The main difference seems to be the much higher prevalence rates of PV among student couples.
Validity of the data
The measure of PV used for this study is correlated .68 with the measure used by the European Union’s study of violence against women (Fundamental Rights Agency, 2014). However, because most of the nations in the current sample were not in Europe, only six overlapped. With only six nations, even a correlation as high as .68 only approached significance, p = .07. However, there is evidence from another multination study using samples of university students which suggests that such studies can provide valid cross-national comparisons because a “national context effect” tends to affect most segments of the population (Straus, 2009). This study of student samples from 32 nations found correlations from .43 to a high of .69,with a median r of .51 between the rank of a nation based on the student data and the rank based on nationally representative data. The .69 is particularly relevant because it is the correlation (using nations as the unit of analysis) between the measures of coercive control used for the current study with the United Nations’s GII (Gaye et al., 2010).
Nation-to-nation differences
These are not addressed in our study because presenting and explaining national differences would require more pages than is permitted. In addition, considerable information on national differences in DCTs is presented in other articles in the Concordance Analysis Research Program (Michel-Smith & Straus, 2014, 2015; Straus & Michel-Smith, 2014).
Conclusions and Implications for Future Research
The results of this study suggest that revising the way PV is conceptualized, measured, and treated by augmenting the current focus on individual offenders and individual victims to an approach based on recognizing that PV is also a dyadic phenomenon can enhance these efforts. Moreover, because almost all methods used to obtain data on PV can be used to identify the three DCTs, this important aspect of PV can be identified in almost all research studies and clinical diagnoses. Thus, DCTs are a practical way for both researchers and clinicians to identify a key aspect of violent relationships. Because of the important additional information they provided, identifying the DCT of each case should be a default early step in research and practice.
Implications for Theories of PV
Theories of PV need to be improved to recognize the dyadic nature of PV specifically that this study and others cited found that approximately half of cases of PV are bidirectional and that there are substantial percentage of Female Only assaulted couples (Langhinrichsen-Rohling et al., 2012; Straus, 2015).
Implications for Research
In research, it is clearly important to examine the separate effects of the behavior of each partner, but the results in this article suggest that may not adequately depict the situation. Characteristics of the couple such as their DCT also should be a unit of study. This has also been a conclusion from studies of the effects on individuals and the relationship of being in different DCTs (Fehringer & Hindin, 2009; Graham, Bernards, Flynn, Tremblay, & Wells, 2012; Rodriguez & Neighbors, 2015; Straus & Winstok, 2013). Those studies have found effects that are in addition to the effect of the characteristics of each partner.
Implications for Prevention and Treatment
Gender similarities in risk factors
Consistent with other studies, we found that risk factors for PV by men and women tended to be parallel. The similar risk factors and the similar rates of perpetration found by more than 200 studies (see Desmarais et al., 2012) make it important to replace prevention programs solely directed to men and boys with programs that are applicable and explicitly mention examples of assaults by women and girls as well by men and boys.
Chronic denigration
The finding that a relationship that is characterized by chronic denigration of a partner (usually labeled as psychological aggression) was related to all three DCTs is consistent with 40 years of previous research that found denigration to be one of the most important risk factors for PV, including longitudinal research (Murphy & O’Leary, 1989; Salis, Salwen, & O’Leary, 2014; Straus, 1974). Moreover, denigration may be a risk factor that is more amenable to modification than other risk factors, such as personality disorders and drinking problems. Helping both partners reduce denigration can be conceptualized as part of a prevention and treatment approach that attends to enhancing overall relationship skills.
Victim services
Although studies, including our own, suggest that women perpetrate PV at similar levels to men, studies have consistently shown that women are injured more, physically, psychologically, and economically (Archer, 2000; Michel-Smith & Straus, 2014; Stets & Straus, 1990). Consequently, part of the explanation for the resistance to addressing perpetration of PV by women as well as by men is fear that recognizing perpetration by women will detract from the effort to aid female victims. We believe that PV perpetration by women can be addressed sensibly by helping them with difficulties they face that are captured by the risk factors for PV found to be significant in this study, such as experiencing child abuse and struggling with drinking problems.
A dyadic approach to treatment of PV can accomplish this. It takes into account the problems of both partners, many of which existed before the relationship (McCauley, Breslau, Saito, & Miller, 2015), and acknowledges the wide prevalence bidirectional PV (or Both DCT), which was the most common type of PV found in numerous other studies (Langhinrichsen-Rohling et al., 2012; Straus, 2015; Straus & Michel-Smith, 2014). Moreover, when both partners assault, PV tends to result in the highest probability of injury and is most resistant to cessation (Charles et al., 2011; Feld & Straus, 1989; Whitaker et al., 2007). Combined with the similarity in factors associated with perpetration with PV, our findings suggest that a dyadic approach to research and treatment of PV may be more effective than the current primary attention of PV by male partners.
Dyadic treatment does not necessarily mean couple therapy. It means addressing the problems and needs of both partners, not just those of the presenting offender. We believe that replacing the current “batterer intervention programs” with programs that identify and address the problems and needs of both partners, such as those investigated in the current study and many others identified in checklists of empirically demonstrated risk factors (Centers for Disease Control and Prevention & National Center For Injury Prevention and Control, 2006; Krug et al., 2002), is more likely to be successful. Moreover, we believe it is a more humane approach in reducing all aspects of partner abuse.
Footnotes
Authors’ Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Earlier phases of the study were supported by the National Institute of Mental Health Grant T32MH1516.
Author Biographies
![]() .
.
![]() .
.