
Abstract
Background:
Present study aims to examine the socioeconomic and demographic factors that affect health care utilization, health care expenditure and financing strategies for delivery care in India.
Methods:
The study uses data from National Family Health Survey (NFHS-4), 2015-2016. Descriptive, bivariate and multivariate regression analysis were carried out to examine health care utilization, out of pocket expenditure and financing strategies for delivery care in India. We used hardship financing as when people resort to borrowings, or sale of property/jewelry to pay for healthcare expenditure
Results:
Overall, Janani Suraksha Yojana (JSY) could cover less than 40% of the delivery care expenditure across all states. One-third of the households borrowed money or sold property/jewelry for delivery care expenditure. Highest exposure to hardship financing was observed in utilisation of private healthcare facilities for delivery. Women from the higher income quintiles are less likely to experience hardship financing as compared to women from the poorest wealth quintile.
Conclusions:
The study results will be useful for government to ensure that financing policies for delivery such as JSY are effective to provide availability and affordability of delivery healthcare in India.
Introduction
Health status of the population is perhaps the most crucial factor that contributes to the development of any country. Despite of achieving considerable success in the reduction of maternal mortality rates over the last decade in India, from 560 per 100,000 live births in 1990 to 167 per 100,000 live births in 2011–2013, the country still tops on a global level in terms of absolute numbers of female deaths due to pregnancy-related causes. It is interesting to note that our country along with Nigeria accounted for about 33% of all global maternal deaths in 2014, with 17% (50,000) in India and 14% (40,000) in Nigeria (Ministry of Statistics and Programme Implementation [MoSPI], 2015; Office of Registrar General of India, 2013; World Health Organization & UNICEF, 2014). It is now globally recognised that healthy living is a necessity and thus should not be a privilege of few; hence, countries world over seek to achieve Universal Health Coverage (UHC). Nonetheless, in a developing country like India, out-of-pocket expenditure (OOPE) is a major hurdle in achieving universal health coverage. Thus, significant sections of the population suffer due to limited public funding, high cost of hospitalisation, cost of drugs and lack of insurance and dominance of private health service providers. Therefore, OOPE further worsens the financial conditions by making the poor even poorer. Interestingly, it is the financial hardship that is the prime reason for meagre utilisation of maternal health services in India (International Institute for Population Sciences, ORC Macro, 2000).
It is sad to note that even though India has made significant economic progress, the public expenditure on health care in the country has not improved since the early 1990s. In fact, our Government expenditure on health care is appreciably low even when compared with countries with similar levels of per-capita income, inequality and poverty (International Institute for Population Sciences and Macro International, 2007; MoSPI, 2015). India has a huge share of maternal and child health problems at the global level due to the fact that financial incapacity prevents the uptake of maternal and child health care services in the country. This sets up a vicious cycle, where poverty leads to ill health and ill health further leads to poverty, hence a huge hurdle in the path of our country’s progress. Moreover, there is a huge problem of informal payments for antenatal, delivery and postnatal services in the Indian public health sector, primarily due to service bias, social discrimination and poverty (Drèze & Sen, 2015). To meet the various challenges in the path of health care access to the community, several schemes have been launched in the country. These include Janani Suraksha Yojana (JSY) launched in 2005 and Janani Shishu Suraksha Yojana launched in 2011. Such schemes aim at reducing the OOPE not only for the expecting mothers, but also for the neonates.
Need for the Study
A few studies have assessed the basic questions associated with health care expenditure and financing strategies for delivery care in India (Bonu et.al., 2009; Leone et.al., 2013; Mohanty & Srivastava, 2012; Sahu & Bharti, 2017; Yadav & Yadav, 2017). However, there is a need to study; what is condition of health care seeking behaviour, health care expenditure and financing strategies for delivery health care services in India. Do health care seeking behaviour, health care expenditure and financing strategies for delivery health care services in India vary by socioeconomic backgrounds of women? If yes, what are the main socio-economic predictors? To answer these questions, it is important to examine the socioeconomic and demographic factors that affect healthcare-seeking behaviour, health care expenditure and source of financing strategies for delivery care in India. The purpose of the study is to identify the predictors that affect healthcare-seeking behaviour and inform policy makers on improving the health systems and carrying the idea of financing strategies for delivery health care services in India.
Study Setting, Data and Methods
Data, Sampling Techniques and Sample Size
The study uses data from the fourth round of the National Family Health Survey (NFHS-4), the Indian version of the Demographic and Health Survey. The NFHS-4 sample is a stratified two-stage sample. The 2011 Census served as the sampling frame for the selection of PSUs. PSUs were villages in rural areas and Census Enumeration Blocks in urban areas. PSUs with fewer than 40 households were linked to the nearest PSU. Within each rural stratum, villages were selected from the sampling frame with probability proportional to size. In each stratum, six approximately equal substrata were created by crossing three substrata, each created based on the estimated number of households in each village, with two substrata, each created based on the percentage of the population belonging to Scheduled Castes (SCs) and Scheduled Tribes (STs) (International Institute for Population Sciences (IIPS) and ICF, 2017). For this study, analysis considered 149,770 most recent live births among women of age 15–49 years who had a live birth in the five years preceding the survey and that was delivered in a health facility.
Outcome Measurements
This study examines the three main outcomes namely healthcare-seeking behaviour, health care expenditure and financing strategies for delivery care. For healthcare-seeking behaviour, this study used the information on type of health facility used by women for delivery care. Based on the availability of data, the type of health facility is divided into two categories: public hospital and private hospital. For health care expenditure, this study used expenses incurred for delivery health care in terms of; direct medical costs (hospital stay, consultation, treatment medicines and procedures, laboratory and other investigation charges), direct non-medical costs (transportation, meals, lodging (for patients and attendants)), and indirect costs (loss of wages for patient and care giver, days of schooling loss for children). This study used population exposed to hardship financing who were forced to borrow from friends, and/or sold property/jewellery (John & Kumar, 2017).
Defining Predictor Variables
Important socioeconomic and demographic predictors such as age, education, sex, marital status, religion, social group, wealth quintile, sanitation facilities, drinking water facilities, cooking facilities, place of residence and regions of residence were included as predictor variables in the present study based on the previous studies (John & Kumar, 2017; Leone et al., 2013; Sahu & Bharati, 2017; Yadav & Yadav, 2017).
Analytical Approach
To meet the objective, this study used bivariate, multivariate and binary logistic regression models. In the first step of analysis the multivariate analysis was used to understand the condition and variation of women seeking delivery care in government and private health facilities. Second, the mean health care expenditure (medical cost, non-medical cost, transportations cost and OOPE) for the utilisation of delivery health care services was presented by selected background characteristics of women. In the third part of analysis, the multivariable regression analysis was carried out to estimate the adjusted effects of selected covariates on OOPE and hardship financing.
Results
Health Facility Utilisation
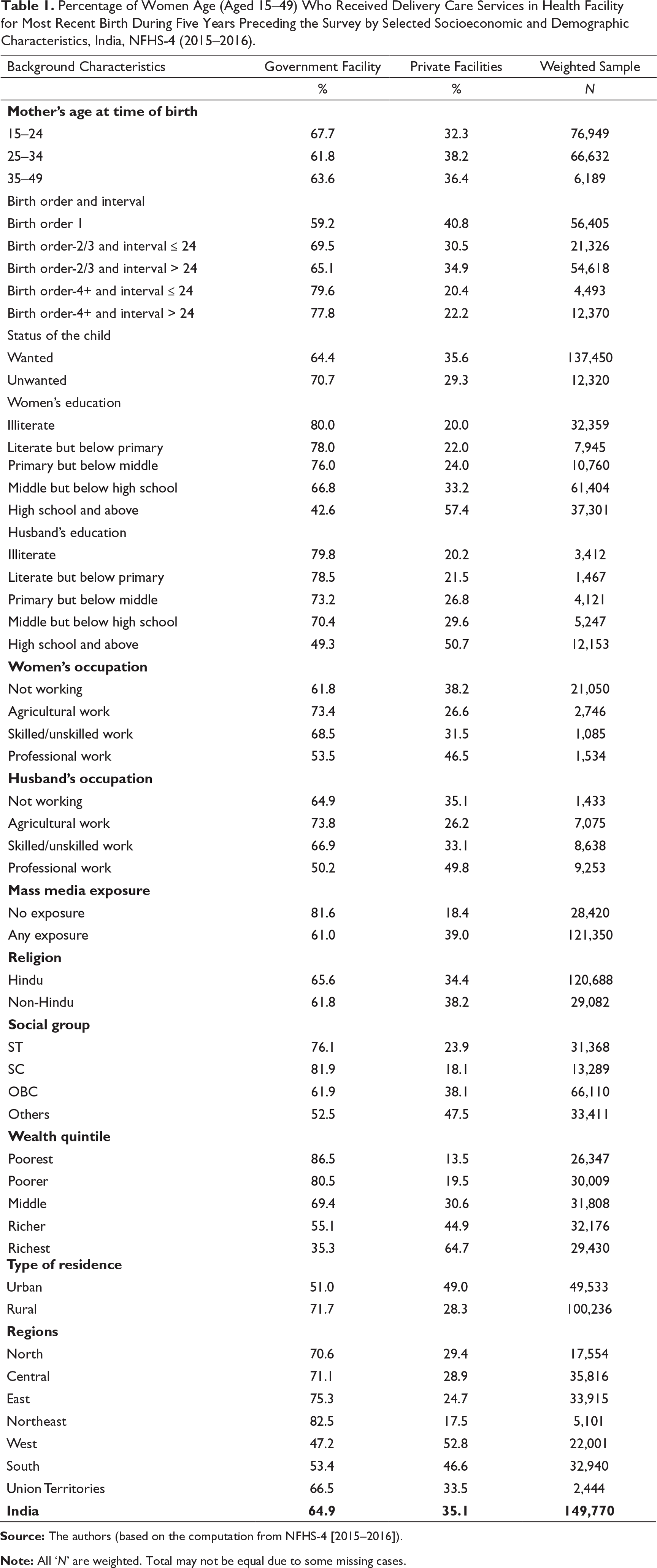
To examine the health facility utilisation for delivery care, this study examines selected socioeconomic and demographic characteristics. Table 1 shows the weighted percentage of women who utilised delivery health care services by selected background characteristics. Findings from analysis show that 65% of women seek government health care facilities for delivery while 35% sought private hospitals for delivery. There is greater utilization of government health services with increasing birth order; it was seen that 59% people prefer government hospital in their first child delivery, while almost 80% go to these hospitals with birth order 4 or more. Only 35% of people with richest wealth quintile use government health services for delivery while 87% poorest people go to government hospital for childbirth. When we see the urban−rural difference, 72% rural population prefers government hospital for deliveries while only 51% of deliveries in urban areas take place in government hospitals. Further, our study also explores the utilisation of health facility by states of India. The results showed variation in the choice of health facilities utilisation for delivery care in India. States such as Telangana (64%), Kerala (60%), Gujarat (61%) and Andhra Pradesh (58%) reported more public health facilities for delivery care. More than two-third of the deliveries were conducted in public health facilities (71%) as compared to only (29%) in private health facilities (Figure 1).

Source: Authors’ calculations based on the computation from NFHS-4 [2015–2016].
Percentage of Women Age (Aged 15–49) Who Received Delivery Care Services in Health Facility for Most Recent Birth During Five Years Preceding the Survey by Selected Socioeconomic and Demographic Characteristics, India, NFHS-4 (2015–2016).
Out-of-Pocket Expenditure for Delivery Care
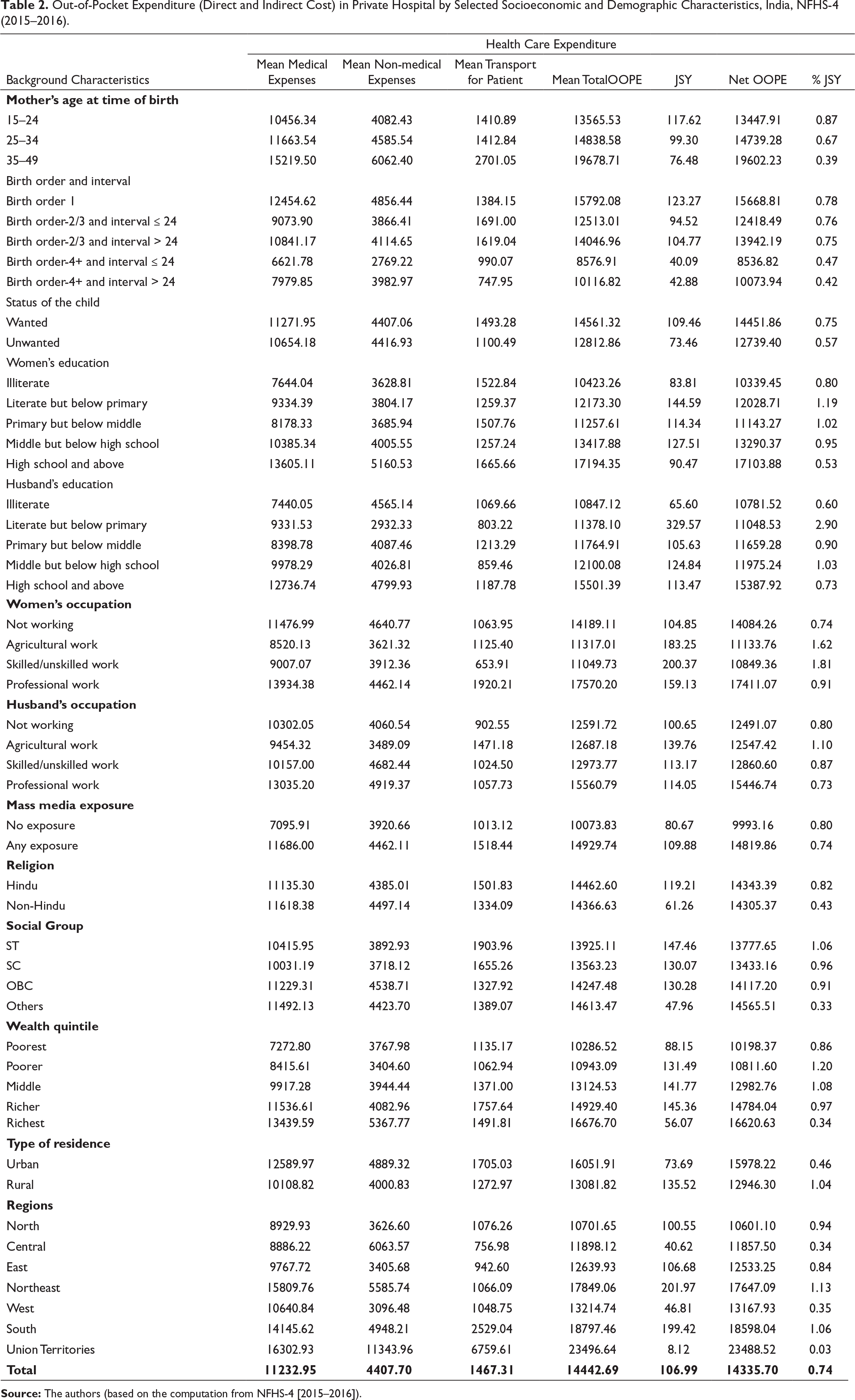
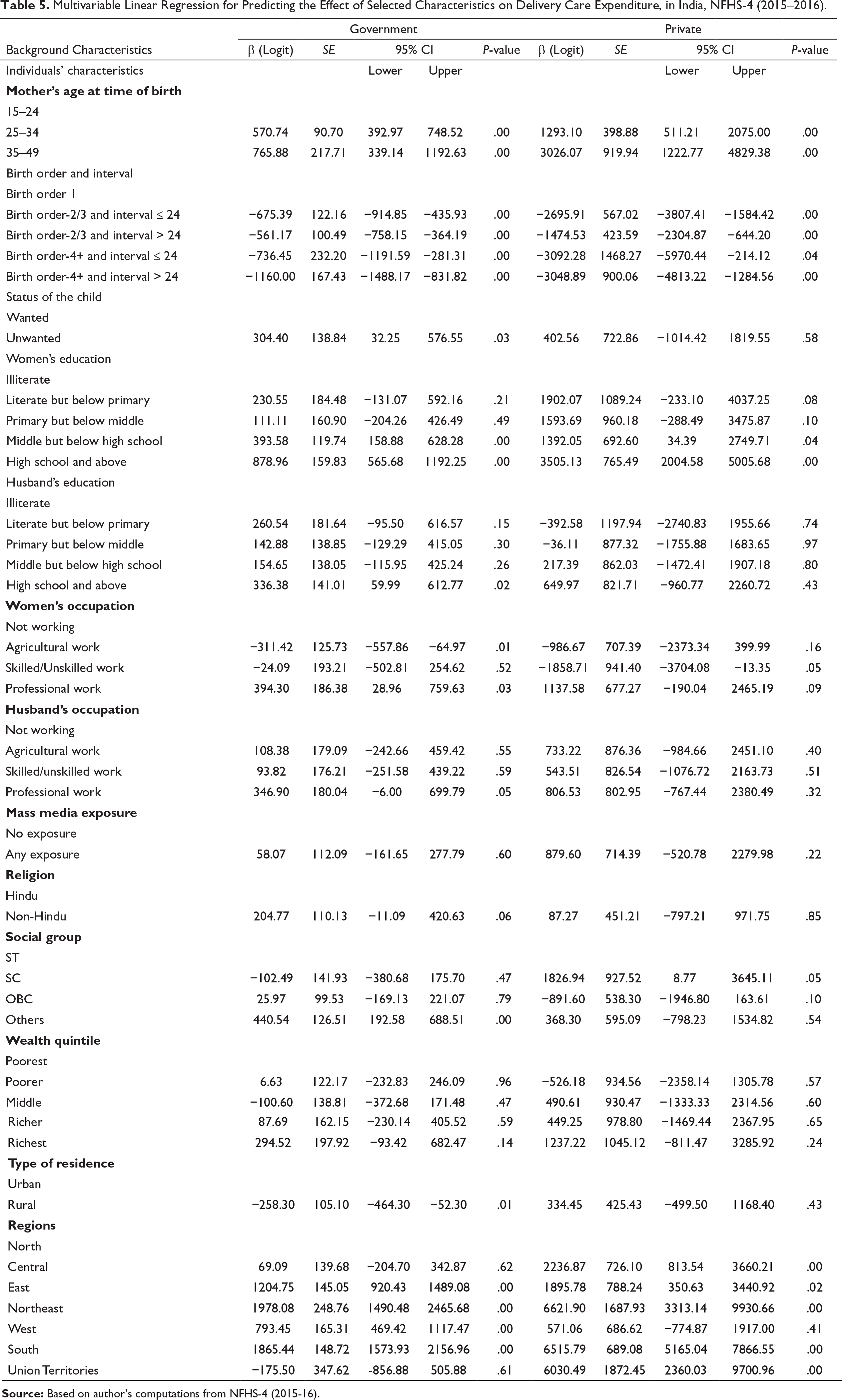
Furthermore, with increasing birth order there appears to be a somewhat increasing trend in utilisation of JSY with a decline in both medical (barring birth order 2/3 with a gap of more than two years) and non-medical expenses (Tables 2 & 3). An interesting finding is that there are higher expenditures (medical, non-medical as well as OOPE) and lower extent of JSY utilisation in unwanted as compared to wanted child births. If we compare our findings in the private health care facilities, the expenditure is almost ten times that in public sector. Higher educated and those living in urban area have higher expenditure for delivery health care compared to their rural counterparts. Amongst the different social groups, the scheduled tribe (ST) people are observed to spend the least on delivery healthcare. This is further supported by the fact that the average delivery healthcare expenditure is very high among richest women compared to poorest women (Tables 3 & 4).
Out-of-Pocket Expenditure (Direct and Indirect Cost) in Private Hospital by Selected Socioeconomic and Demographic Characteristics, India, NFHS-4 (2015–2016).
Out-of-Pocket Expenditure (Direct and Indirect Cost) in Government Hospital by Selected Socioeconomic and Demographic Characteristics, India, NFHS-4 (2015–16).
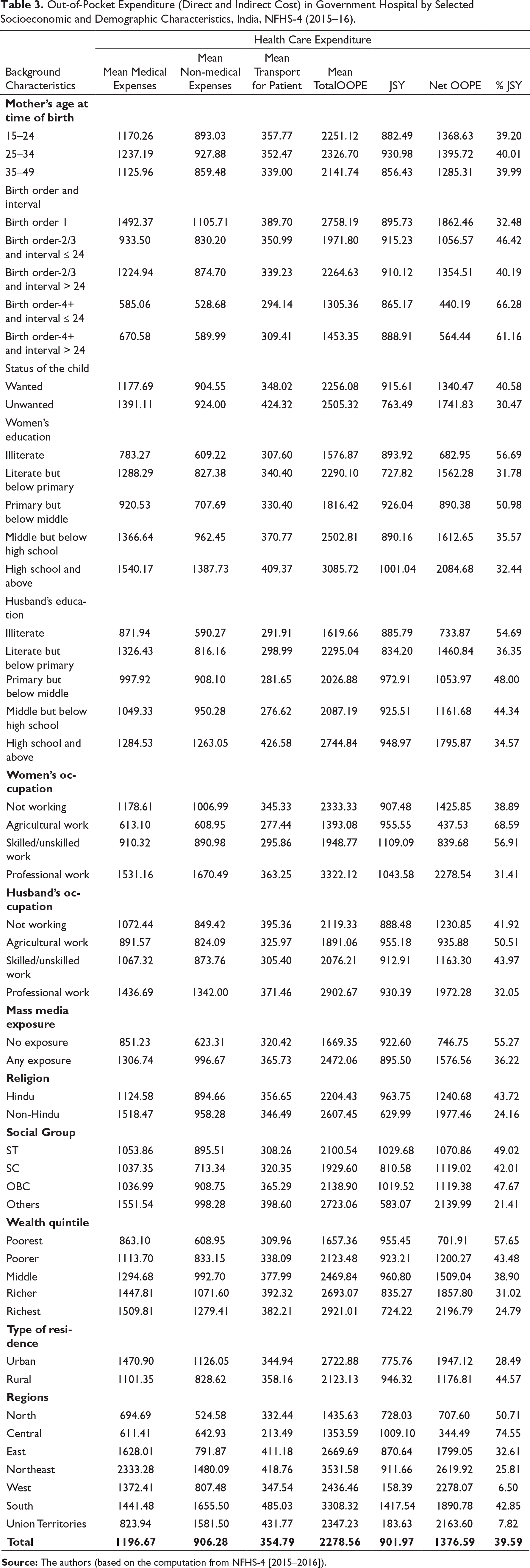
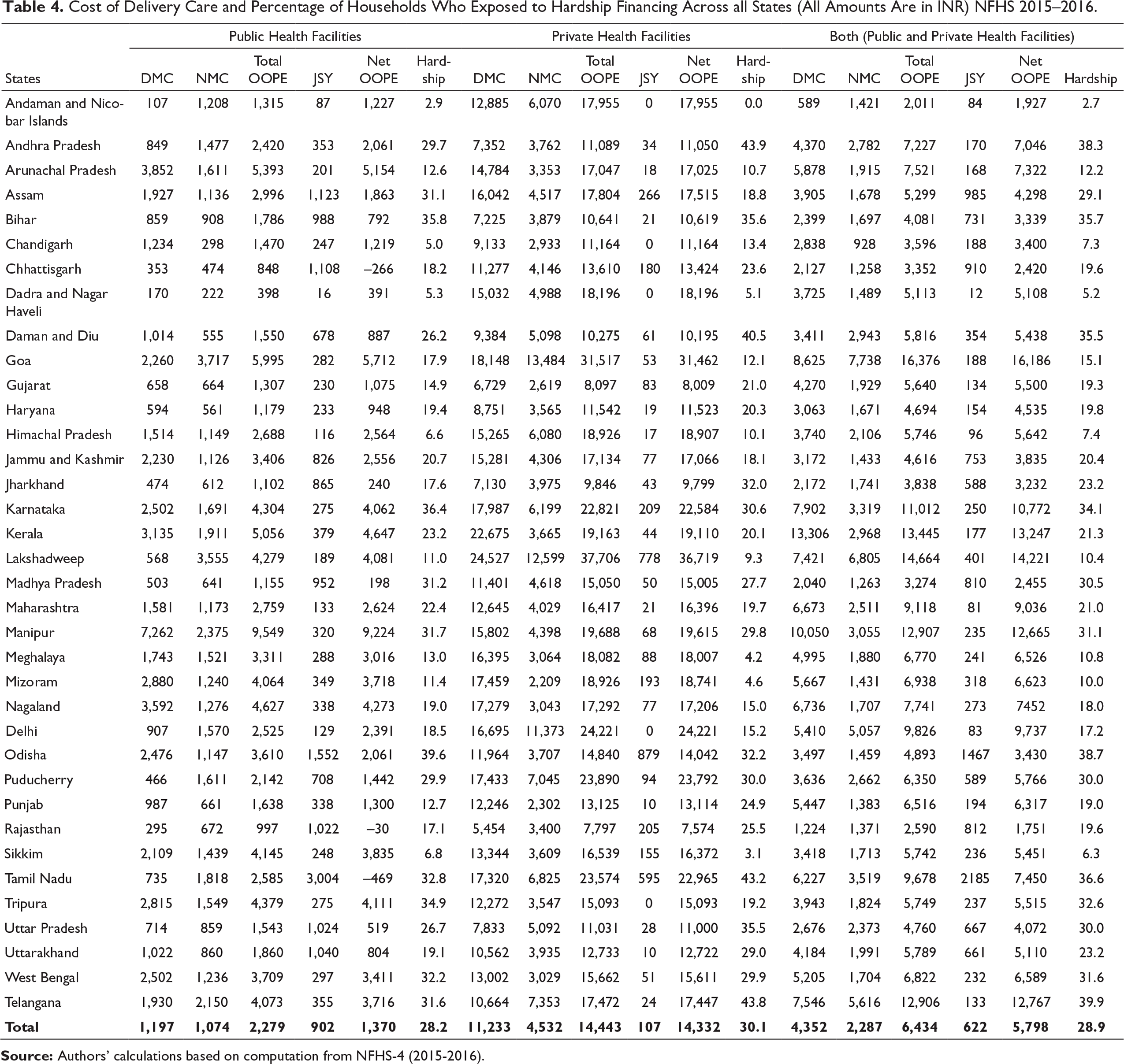
Delivery care cost is observed to be high among all the Union Territories and South region of India as compared to Central and East regions of India. Next, we present the choice of health facility utilization for delivery care in India and its states and impact of health care expenditure on households in terms of hardship financing due to health care expenditure for delivery care (Table 4). Our study indicates large variations in the health care expenditure (including hardship financing) across public and private health facilities (Table 5). Amongst the difference social groups, the ST people are observed to spend the least on delivery health care, possibly because they tend to be earning least amongst various social groups. This is further supported by the fact that the average delivery health care expenditure is very high among richest women compared to poorest women. Delivery care cost is high among all the union territories and South region of India as compared to Central and East regions of India. Next, we present the choice of health facility utilisation for delivery care in India and its states and impact of health care expenditure on households in term of hardship financing due to health care expenditure for delivery care. Our study indicated large variations in the health care expenditure and hardship financing in various types of health facilities (Table 2 & 4).
Cost of Delivery Care and Percentage of Households Who Exposed to Hardship Financing Across all States (All Amounts Are in INR) NFHS 2015–2016.
Multivariable Linear Regression for Predicting the Effect of Selected Characteristics on Delivery Care Expenditure, in India, NFHS-4 (2015–2016).
Financing Strategies to Meet the Health Care Expenditure
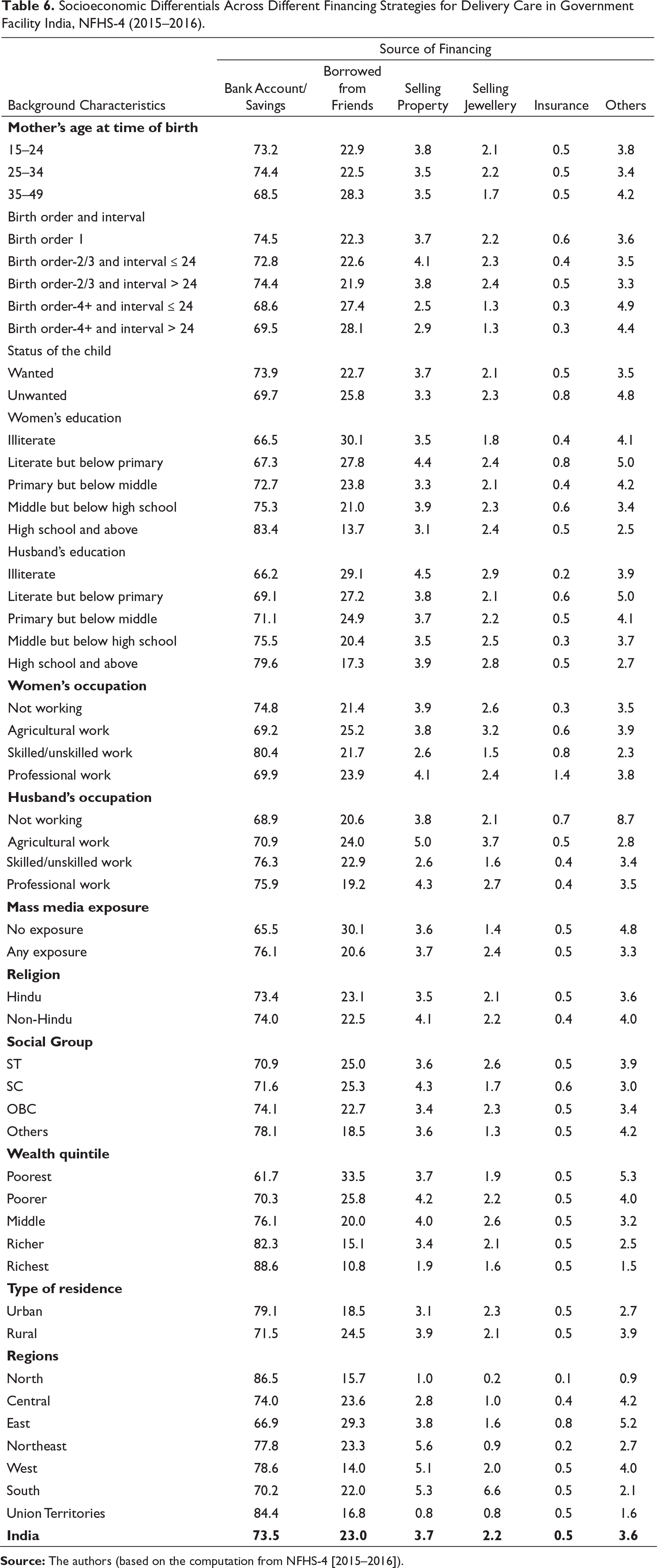
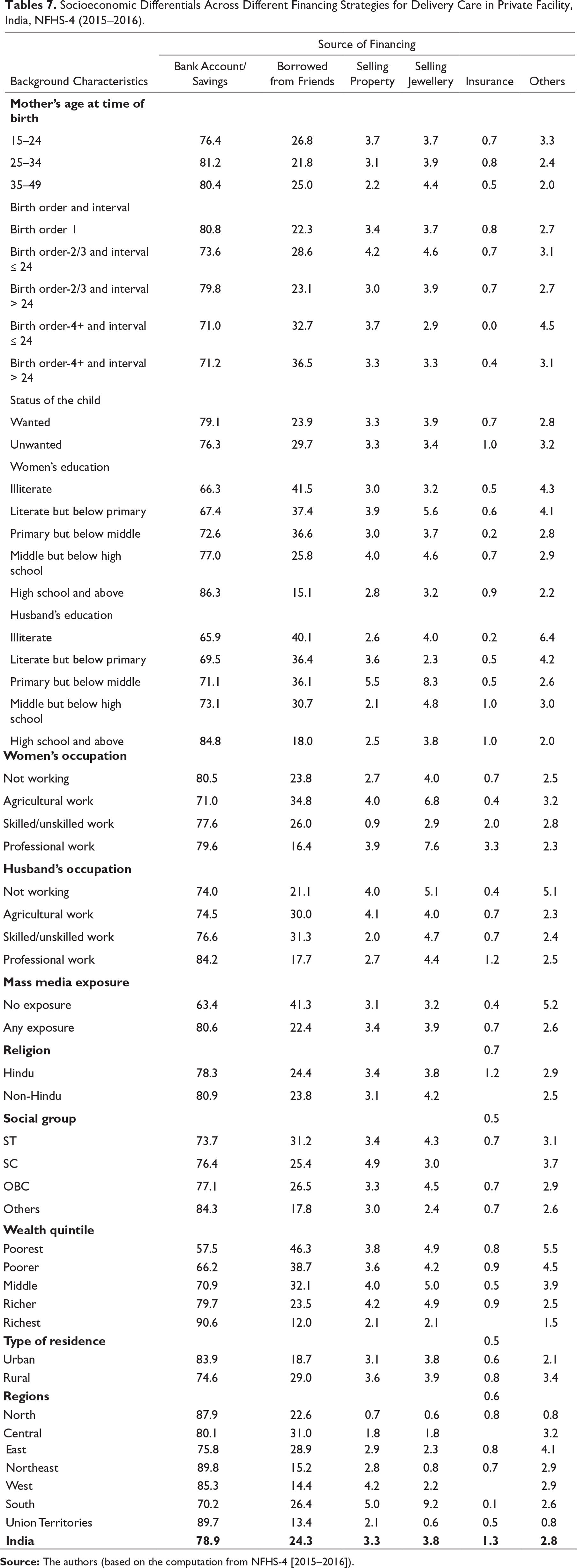
All the socio-demographic differentials showed higher percentage of women resorting to sale of property or jewellery to pay for delivery expenditure in private health facilities compared to government health facilities (Tables 6 & 7). Majority (around 80%) of the financing is through bank accounts/savings followed by borrowings from friends for financing delivery care in both public and private health facilities.
Socioeconomic Differentials Across Different Financing Strategies for Delivery Care in Government Facility India, NFHS-4 (2015–2016).
Socioeconomic Differentials Across Different Financing Strategies for Delivery Care in Private Facility, India, NFHS-4 (2015–2016).
Determinants of Hardship Financing
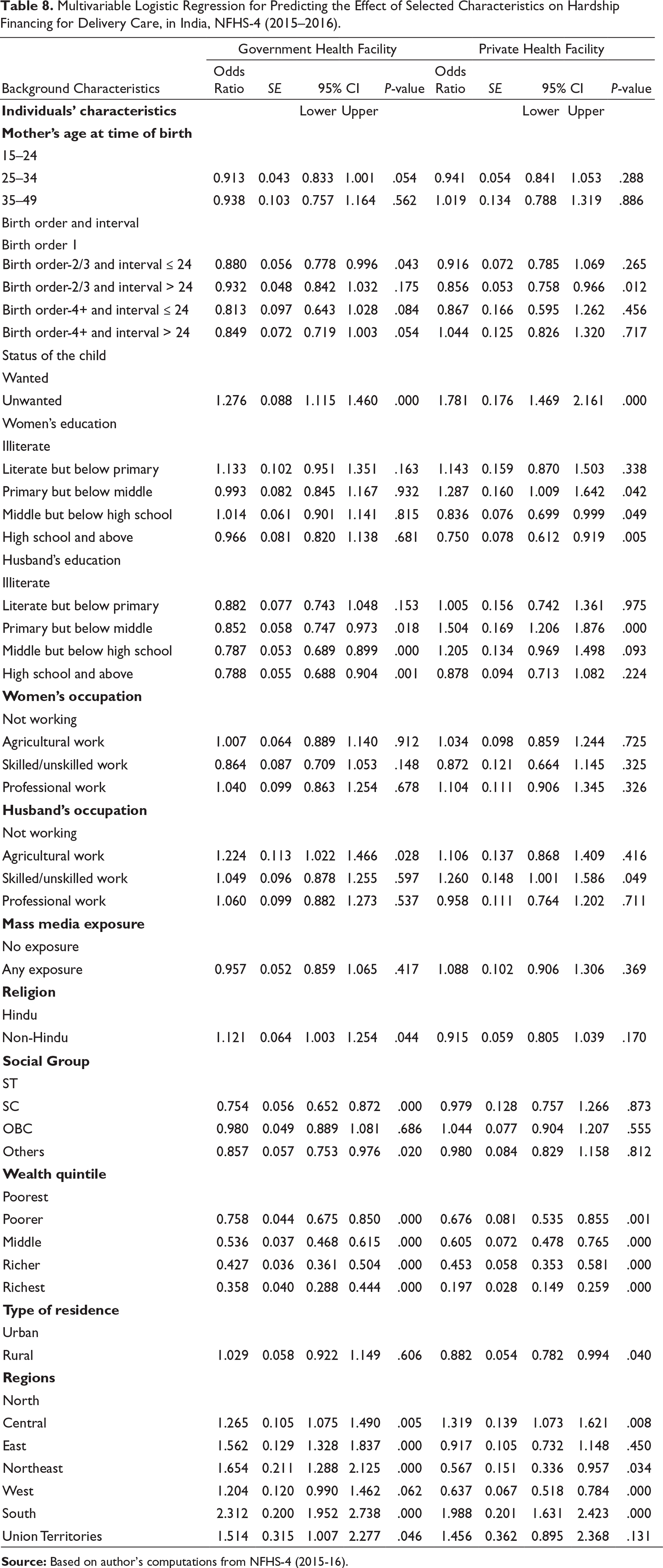
Table 8 provides the factors associated with hardship financing for managing expenditure related to delivery care. Middle age women (25-34 years) were less likely to have hardship financing than the younger women (15-24years) (Table 8). The likelihood risk of seeking hardship financing for delivery care expenditure are found to be less likely among women who had more than one child than among women who experienced their first childbirth. If the child was not planned there is a significant (OR=1.42, CI =1.27-1.59) higher likelihood to have hardship financing than when the child is planned or wanted. Education of women has a significant negative association with hardship financing. In fact, women with Middle but below high school education (OR=0.879, CI=0.79-0.97) are less likely to experience hardship financing as compared to uneducated women. Odds of being exposed to hardship financing among women who had high school and above education level (OR=0.84, CI=0.73-0.95) were less compared to uneducated women. Women from the richer (OR=0.32, CI =0.27-0.37), richest (OR=0.54, CI=0.47-0.62), middle (OR=0.61, CI=0.54-0.69) and poorer (OR=0.79, CI=0.72-0.88) wealth quintiles are less likely to experience hardship financing as compared to women from the poorest wealth quintile. Mass media exposure, Religion and place of residence are not significantly related with hardship financing.
Multivariable Logistic Regression for Predicting the Effect of Selected Characteristics on Hardship Financing for Delivery Care, in India, NFHS-4 (2015–2016).
Discussion
The present study has analysed the socioeconomic disparities in burden of delivery health care expenditure in India using the secondary data like many others previous studies (Modugu et al., 2012; Mohanty & Srivastava, 2012; Ved et al., 2012). Findings from this study show that more than one third of the women seek private health facilities and almost two third women seek treatment in government health facility for delivery healthcare. The results indicate that there exists various socioeconomic disparities in the utilization of health services for delivery in India. Women from richest wealth quintile, higher education, low birth order and women from urban area prefer seeking treatment in private health facility. With increasing birth order, the utilization of government health facility also increases for delivery services. This could be likely to be the result of declining financial resources with increasing number of births in the family. Furthermore, it can be noted that the more literate the woman is, lesser is her preference to visit a government hospital. This is because literate women are more likely to earn and spend on costlier private health sector compared to illiterate females who have not much choice and knowledge but to seek more affordable government health facilities. Women who are exposed to any mass media prefer private health facility for delivery healthcare. Private hospitals lately have been using media advertising such as hoardings, newspaper ads etc. which provides information and media influence for usage of these facilities for delivery services.
As the services and comforts of private hospitals come with higher costs, only 35% of people with richest wealth quintile use government health services for delivery while 87% of the poorest people visit a government hospital for childbirth. With regards to urban-rural difference, 72% of the rural population prefers government hospital for deliveries while only 51% of deliveries in urban areas take place in government hospitals. This can be attributed to the higher spending ability, greater awareness band better accessibility to private health care in urban areas. The present study has also analysed the socioeconomic disparities in burden of delivery health care expenditure in India. Results from the multivariate analysis reveal that the birth order and interval, education of women and husband’s education, mass media exposure, economic status, place of residence and region are associated with the delivery healthcare expenditure; these findings are similar to previous studies (Sahu & Bharti, 2017).
Several programmes have been offered by government and non-government organisations for free delivery healthcare but still significant portion of population is utilising private health facilities and spend considerable amount of household expenditure on delivery expenditure. Results from this study clearly indicate that the expenditure of delivery care in private healthcare facilities is more than 5 times higher than public healthcare facilities as suggested in previous studies as well (Bonu et.al., 2009; Goldie et. al., 2010; Peters et.al., 2002). It was seen that in comparison to urban households, rural households spend a considerable proportion of household expenditure on delivery expenditure.
In order to afford expenditure on delivery related health services, several sources of financing have been availed in our sample population (e.g. savings, borrowing money from friends and others, sale of jewellery/property, insurance and others). These borrowings come with markedly different interest rates and may further add up to the economic burden on the households. In some cases, this can lead to depletion of present fixed assets or future income, e.g. sale of jewellery/property. This study used hardship financing to assess the impact of healthcare expenditure (John & Kumar, 2017). Across both private and public health facilities, the major sources are bank accounts/savings, and borrowings from friends. It was also found that with increasing birth order there is greater exposure to hardship financing; mainly due to increasing financial burden with increasing family size. Hardship financing is observed to be higher in unwanted birth than wanted child, probably as the family is financially better prepared before the birth of wanted child. Media, called as the eyes and ears of the people, also plays an important part; those who are exposed to media are more aware of the various aspects like family planning as well as affordable healthcare facilities and schemes, and thus are less likely to need financing, and this is observed in our study as well. SC, ST and OBC classes have higher exposure to hardship financing for delivery expenditure compared to the general category.
Furthermore, due to lesser means of earnings in rural areas, the rural people have a greater share of being exposed to hardship financing than those in urban areas. Ironically, the poorest, who spend the least in absolute terms, are the ones who bear the highest expenditure burden in relative terms, and consequently they are the most disadvantaged ones. As seen in use of general health services, the poorest are at a high risk of falling into the vicious cycle of debt trap if they use maternal health care services (Krishna, 2006).
The poorer the person, more is his/her exposure to hardship financing to manage delivery care expenditure. Furthermore, due to lesser means of earnings in rural areas, the rural people take greater share of hardship financing than those in urban areas. Ironically, the poorest, who spend the least in absolute terms, are the ones who bear the highest load in relative terms, and consequently they are the most disadvantaged ones. Hence, it suggests that the poorest are at a high risk of falling into the vicious cycle of debt trap if they use maternal health care services, and a similar case has been found with the use of general health services (Krishna, 2006).
Conclusion
The present study provides significant insights into the variations in the health care seeking behavior, health care expenditure and hardship financing for delivery health care services in India. Health is the one of the prime pillars on which the development of any country rests. Hence, government policies should be implemented earnestly for bridging the gaps of the deprived masses with regards to availability and affordability delivery health care services in the country. Media can spread awareness about these government schemes besides sensitizing the masses for family planning. This will undoubtedly contribute manifold to the country’s progress by ensuring healthy, safe and lower financial burden on households for deliver episodes..
Strengths and Limitations of the Study
The strength of this study derives from its use of national representative data from National Family Health Survey, the Indian version of Demographic health Survey. The sample is very large which offers the generalisability to the study results. The findings of this study may help to find appropriate population policy for delivery care in India. While this study has numerous strengths, there are some limitations as well. Our study did not calculate the indirect costs due to loss of wage of patient and caregivers due to unavailability of data in data set, and both the variable outcome and predictors are self-reported and hence subject to recall bias.
Footnotes
Acknowledgements
An earlier version of this paper was presented in National Seminar on the Poverty and Social Exclusion: A Life Course Perspective” during 12-13 April, 2018, Dr. Ambedkar Chair in Social Justice, Indian Institute of Public Administration, New Delhi, India with collaboration with Lokashraya Foundation, New Delhi TERI School of Advanced Studies, New Delhi. Author is grateful to session chairpersons and participants for comments and constructive suggestions facilitating improvement in the paper.
Author’s Contributions
JY led the analysis and organised the draft of manuscript. JY contributed to the analysis. JY and SA did the interpretation and manuscript writing. DJ contributed to the design, interpretation and manuscript writing. DJ and GRM conceived this study, led the design, analysis and interpretation, and drafted the final manuscript. All authors approved the final version of the manuscript.
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship and/or publication of this article.