
Abstract
This article uses nationally representative household survey data between June 2019 and 2020 from India to examine changes in household consumption expenditure following the first wave of the COVID-19 pandemic. We find that across rural and urban households, there was a strong reduction in overall expenditures, in particular, related to food and health. This corroborates findings from existing literature on food insecurity during the first lockdown in India (March–April 2020) and provides the first set of estimates on changes in health expenditure for this period. Although there were expansions to health insurance and subsidized COVID-related healthcare costs in India, our findings likely do not reflect this. We discuss implications for policy and outline future work.
Introduction
The coronavirus pandemic has created a large hole in the pocket of a majority of the Indian population. In general, total expenses per household (in the urban areas) declined by 34% in April 2020 (Bhardwaj, 2021) when the first wave of the pandemic was raging strong, and the pan-India lockdown was enforced. One of the significant reasons behind declining spending is the massive reduction in incomes; owing to the lockdown, a staggering 84% of households witnessed a drop in incomes which coincided with a spike in unemployment rates to 25.5% as of 5 May 2020 (Bertrand et al., 2020). Furthermore, according to the Consumer Pyramids database of the Centre for Monitoring the Indian Economy (CMIE), households spent only about 3% of total expenditures on healthcare and related items as of June 2020, a 1% reduction since the same month the previous year (Tagat, 2021). As per the Ipsos Cost of Living Survey, since COVID-19 entered India, urban households have spent 49% of their earnings compared to a global spending figure of 27% for healthcare products (Bhatia, 2020).
Out-of-Pocket (OOP) Spending
High out-of-pocket (OOP) spending on healthcare products and services has been an incessant problem in India even before the coronavirus came into being. In a 2019 report by the World Health Organization (WHO, 2019), Indians were spending 80% of their total healthcare OOP expenditure on medicines alone. Second, based on the National Health Accounts estimates, household expenditures on health (per capita at current prices) rose from ₹875 in 2004–2005 to ₹2,465 in 2013–2014 (Dilip & Nandraj, 2017). Third, according to the Ministry of Health and Family Welfare, Government of India, the government’s public expenditure (GPE) on healthcare as a proportion of the aggregate government revenue stood at a mere 1.28% which suggests that OOP expenses and private expenses on health is extremely high (Siddiqui et al., 2020). In a 2013 study, it was found that at the country level, 10.1% of rural households were rendered poor or more impoverished as a consequence of OOP payments in healthcare-related domains compared to 6.2% of urban households (Ladusingh & Pandey, 2013). As per the World Health Statistics, 2020, India fares the poorly with regard to OOP payments for healthcare as approximately 17% of the population spends more than 10% of their incomes on health (as cited in the Economic Survey, 2020–2021, 2021).
As OOP expenses on healthcare have been continuously rising, it presents itself as a considerable bottleneck during the pandemic since people on the lower rungs of the income spectrum might have to spend exorbitantly to access health-related goods and services. High OOP spending might become the primary reason behind the unaffordability of healthcare services during the menacing COVID-19 pandemic, jeopardising household welfare and well-being.
Changes in Household Expenditure Patterns due to COVID-19
Panic buying was widely prevalent during and before the national lockdown (Janata Curfew) was set to be enforced in India from 22 March 2020 (Kumar & Abdin, 2021). People began stocking up on household essentials and curtailed spending on electronic appliances, beauty and tobacco products and luxury items (Ernst & Young [EY], 2020). For instance, concerning household essentials, those who usually purchased around 1–2 kgs of rice were seen buying around 5 kgs of rice in bulk once the date of the nationwide lockdown commencement was announced (Kharat, 2020).
According to Chauhan and Shah (2020), the pandemic has instilled heightened awareness about health and hygiene items, medical requirements, and healthy and nutritious food; additionally, the authors present that the change in consumption and expenditure behaviour due to the pandemic and lockdown is expected to continue and remain permanent even after the pandemic’s intensity reduces in the near future (as cited in De & Pradhan, 2020, p. 89). In March 2020, there was a 350%-rise (approximate figure) in demand for hand sanitisers and a 60% escalation in demand for handwash. Immunity boosters also encountered soaring demand as Chyawanprash, turmeric and packaged health foods witnessed a demand boost of approximately 80%, 40% and 35%, respectively. On the other hand, confectionery goods, alcohol and consumer durables experienced steep declines in demand by more than 20% (EY, 2020).
Individuals were also seen to indulge heavily in health insurance expenses as the premia paid on individual health insurance policies shot up by 34% in the April-to-September period in 2020 (Srinivas, 2020). Another survey carried out by Max Bupa found that before the coronavirus outbreak, a mere 10% of Indians were keen on signing up for health insurance but, post the pandemic outbreak, 71% of respondents expressed the need for taking up health insurance during these uncertain times (as cited in Puttaiah et al., 2020) thus highlighting their preference for the same.
Class-wise Medical Expenses due to the Virus Outbreak
Class-wise medical spending assumes importance since the socioeconomic class of a person has a significant impact on health. Donkin (2014) showed that those lower in socioeconomic position had poor health and a shorter lifespan relative to higher socioeconomic group individuals. The researcher illustrated the ‘Whitehall study of British civil servants’ to portray the negative link between societal class and health and also observed a ‘social gradient’ in health status whereby the following progression is evident: those in the highest social rank live longer and healthier than those just below them who in turn live healthier than those below them and the pattern continues.
In 2020, the Indian middle class has diminished by 32 million due to the virus outbreak, whereas the number of Indian poor has shot up by 75 million, which constitutes roughly 60% of the worldwide rise in poverty (Kochhar, 2021). This result is problematic because of two reasons: first, as an increasing number of people find themselves among the Indian poor, the ‘social gradient’ concept assumes relevance since the poor might become more vulnerable to the infection compared to other social strata due to the unaffordability of medications, drugs and other requirements to counter the virus. Second, people belonging to the middle-income are predominantly salaried employees (Aslany, 2019) and, due to job losses and rising poverty levels, they face significant hurdles with regard to affording medical expenses related to COVID-19. This claim is backed by a study conducted by Gupta and Khapre (2020), which lists the multiple high costs incurred by an average middle-class person at various stages of hospitalisation due to the coronavirus infection.
Health-Income Gradient
As explained by Dr Kathleen Brown, the health-income gradient is a concept that connects one’s income (or wealth) and health such that as income increases, the health of an individual is enhanced. This idea can also explain the relationship between the health and wealth of an entire community (Nelson, 2019). Deaton (2002), using data from 1980, found that people whose family incomes constituted the top 5% in the income distribution had the chance of living roughly 25% longer compared to those whose family incomes fell in the bottom 5%. Next, a study used the National Health Interview Survey (2001–2003) of the National Center for Health Statistics (NCHS) of the United States of America (USA) found that across three health measures (fair or poor health, the number of bad mental health days in the past month and the number of poor physical health days in the past month), those people with higher incomes reported enhanced health conditions across all three health measures compared to people whose incomes were lower (Evans et al., n.d.).
A study conducted by Asaria et al. (2019) highlights the evidence of the health-income gradient in India. Through the usage of data from the National Family Health Survey’s (NFHS) fourth round (2015–2016), it suggested that one-fifth of the poorest Indian households had a life expectancy at birth of 65.1 years while one-fifth of the wealthiest households had a life expectancy of 72.7 years.
As more Indians are pushed into poverty with the growing pandemic growing, the health-income gradient becomes more relevant than ever. Thus, it becomes important to examine the changes in household expenditure related to health in the face of an income shock in the form of the COVID-19 pandemic and associated lockdowns. This paper examines this from an empirical perspective using household-level panel data from India before and immediately after the COVID-19 pandemic struck India.
The remainder of the article is structured as follows. Section 2 contains the data used in this paper. Section 3 outlines the empirical framework used to examine the impact of COVID-19 on health expenditures. Section 4 describes the key results and findings. Section 5 concludes with implications for health policy and limitations of the current work.
Data
The data used in this article come from the Centre for Monitoring the Indian Economy (CMIE) Consumer Pyramids Household Survey (CPHS), which contains detailed data on consumption expenditures at monthly and annual frequencies for urban and rural India since 2014 (Vyas, 2020). The CPHS is a commonly used dataset that researchers in India have previously used to study labour market participation, and changes in food consumption patterns, among various others in the context of COVID-19 (Abraham et al., 2021). Thus, the CPHS typically surveys a ‘panel’ of households, which are surveyed three times a year. As Abraham et al. (2021) note, due to the COVID-19 pandemic, CPHS was administered using telephonic methods, resulting in large sample attrition.
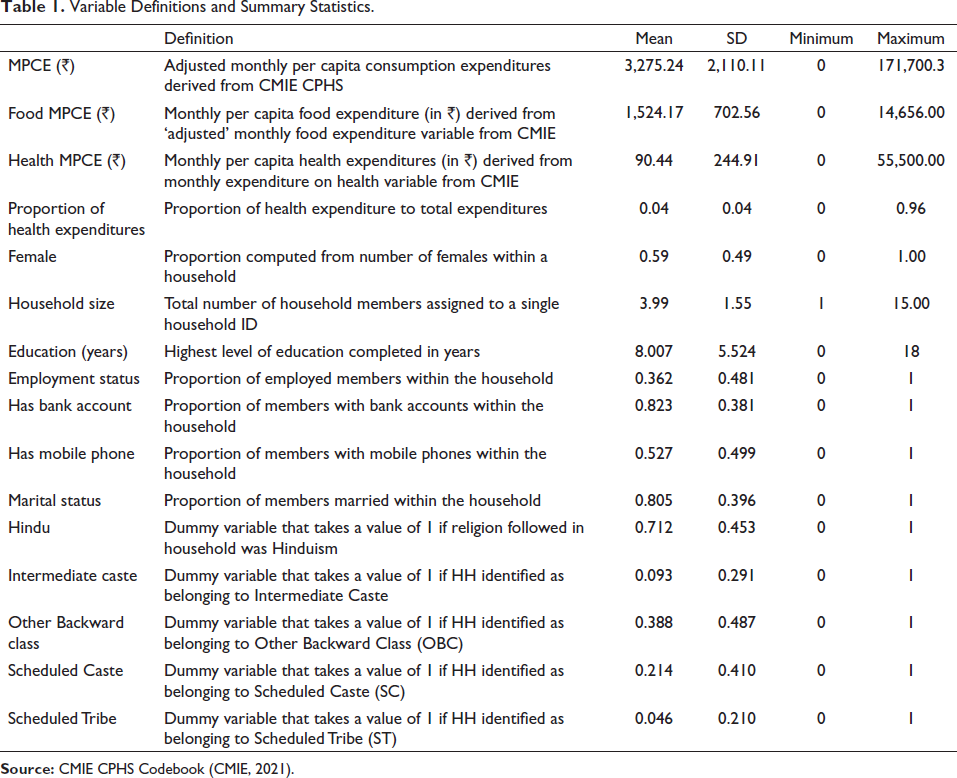
CPHS also provides sample weights, the details of which can be found in Vyas (2020). To model the impacts of the COVID-19 pandemic on health expenditures in India, we formed a panel between June 2019 and June 2020, as this constituted the first wave of the pandemic in India, which was accompanied by the strongest restrictions in place (Hale et al., 2021). We use data from CPHS between June 2019 and June 2020 on household characteristics (employment status, mobile phone ownership, religion, caste group, rural/urban residence, among others), health status, and consumption expenditures (monthly recall, related to health and food). These are summarised alongside the variable definitions provided in Table 1.
Variable Definitions and Summary Statistics.
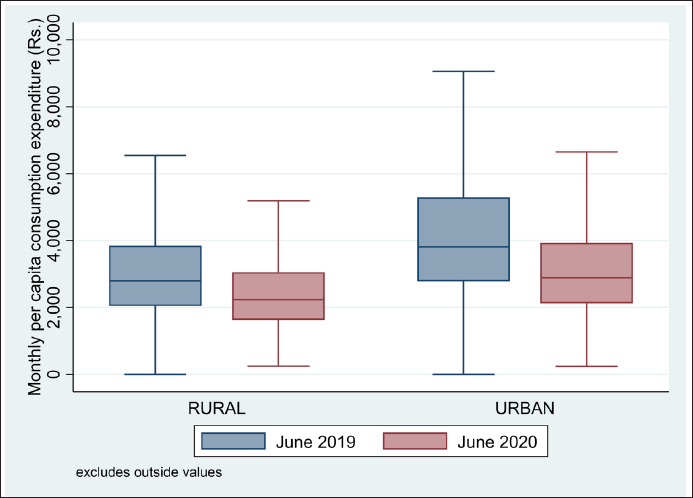
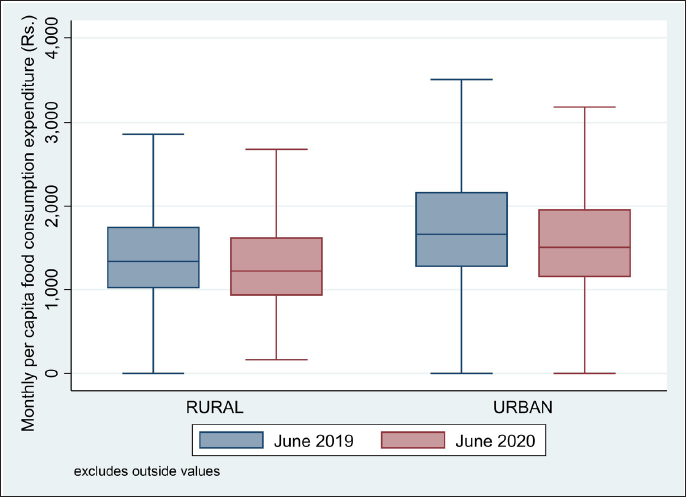
Figures 1–4 below show changes in the key variables of interest between 2019 and 2020 to motivate our key research question.


Methodology
This article focuses on measuring changes in household expenditure due to the coronavirus pandemic. The following is the reduced-form regression equation.

where
Results
The results from the panel OLS estimations on Equation (1) are presented in Table 2.
Regression Results.

Food Expenditure (Rural and Urban)
First, among the rural sample, the food MPCE was lower by about ₹90.37 in the June wave of 2020 relative to the June wave of 2019. Similarly, in the urban sample, the MPCE towards food was lower by about ₹185 in the June 2020 wave compared to the June 2019 wave. Second, the MPCE towards food of an employed person within the rural sample was higher by about ₹74.75 compared to that of an unemployed person. However, this variable had no statistically significant impact in the urban sample. For every unit increase in household size, there is a reduction of around ₹242.2 in the MPCE towards the food in the rural areas and a decline of around ₹293.9 in the MPCE towards food in the urban areas. Both bank account ownership and mobile phone ownership within the household appeared to have no statistically significant impact in the rural and urban samples on food MPCE.
These findings appear to be corroborated by other large-scale survey evidence from telephonic interviews in Delhi (Desai, 2020). They found that many households reported experiencing a sharp increase in food prices (38%) and went hungry (14%). Similarly, Niyati and Vijayamba (2021) found that 45% of their sample of 164 rural households in 26 villages across 13 states reported a drop in food consumption, which varied by socio-economic groups. As other surveys conducted around this time suggested, there was a change in the pattern and composition of food consumption—away from nutritious food like fruits and vegetables and to more affordable staples like rice and wheat in the northern state of Uttarakhand (KISLAY Social Research Collective, 2021) especially, for children in rural Karnataka (Centre for Child and the Law, 2020). This was also likely on account of poor access to ration shops, the designated point of public distribution of foodgrains at subsidized prices (or for free) as well as additional evidence of supply chain bottlenecks during the COVID-19 crisis (Afridi et al., 2020; Mahajan & Tomar, 2021). Heightened food insecurity (Fitzpatrick et al., 2021) arising out of this reduction in food expenditures (especially in urban areas) has been cited to be a critical threat for recovering from the economic productivity shock arising from the pandemic (World Bank, 2021).
Health Expenditure (Rural and Urban)
In terms of health expenditures between 2019 and 2020, in the rural sample, the MPCE towards health was lower by about ₹36.55 in the June wave of 2020 relative to the June wave of 2019. In the urban sample, the MPCE towards health was lower by about ₹45.80 in the June 2020 wave in comparison to the June 2019 wave. Employment status had no statistically significant impact in the rural and urban samples on MPCE towards health. Next, for every unit increase in the household size, the MPCE towards health in the rural areas is lower by around ₹9.720 and for the urban sample, the MPCE towards health is lower by about ₹13.74 for every unit increase in household size. The MPCE towards the health of a person holding a bank account is lower by around ₹20 compared to a person not having a bank account in the urban areas whereas, this variable had no statistically significant impact in the rural sample. Finally, the MPCE towards the health of a person owning a mobile phone in rural areas is lower by about ₹16.93 than a person who does not possess a mobile phone. In contrast, in the urban sample for the same variable, the coefficient is higher by around ₹19.26 compared to one that does not own a mobile phone.
There is not much evidence specifically on changes in health expenditures related to the pandemic in India. Garg et al. (2022) found in a sample from the state of Chhattisgarh that there were ‘catastrophic’ health expenditures due to the hospitalisation of COVID-19 patients. However, it is not likely to reflect in a broader sample such as the CMIE, given that COVID-related testing and treatment were largely subsidised and regulated by the Government of India (Garg et al., 2022). A change in health expenditures observed here could be on account of lower visits to health facilities or putting off medical procedures due to the threat of the pandemic, although there is no empirical evidence that suggests this (but see Barbieri et al., 2021; Hebbar et al., 2020).
Total Expenditure (Rural and Urban)
In terms of total expenditures, we find that total MPCE was lower in the rural sample by about ₹684.9 in 2020 relative to 2019. In the urban sample, the total MPCE was lower by about ₹1,061 in the June 2020 wave in comparison to the June 2019 wave. For every unit increase in household size, there is a reduction of around ₹540.8 in the total MPCE in the rural areas and a decline of around ₹645 in the total MPCE in urban areas. Employment status, ownership of a bank account or mobile phone ownership had no statistically significant impact in the rural and urban samples on the total MPCE.
The results obtained echo the existing literature regards the reduction in household consumption expenditure in 2020 relative to the pre-COVID-19 period. Upon analysing the CMIE CPdx data, found that the per capita expenditure on eggs, milk, fish and meat declined by 23% in August 2020 compared to August 2019. They also found that the per capita spending on other food products such as fruits, vegetables and spices slipped by around 20% during the first lockdown imposed in India in March 2020. Next, according to the Reserve Bank of India’s Report on Currency and Finance, the growth in private consumption painted a worrisome picture: it contracted 16.6% for durable goods and 9.3% for services in 2020–2021 . This is broadly in line with early simulation studies that predicted a contraction in economic activity in specific sectors following the COVID-19 outbreak (Chaudhary et al., 2020). In studies by the World Bank, Data Development Lab, and ID Insight, nearly half of all households reported a drop in consumption expenditures (weekly). However, they suggested that between July and September 2020 (the months following the CMIE data considered in this article), there was some improvement in consumption expenditures.
Concluding Remarks
Our findings indicate that the onset of the COVID-19 pandemic in India resulted in a general reduction in food, health, and overall expenditures in both rural as well as urban areas between 2019 and 2020. The findings are particularly driven by urban households as well as those with greater household size. These results are in line with earlier survey evidence on changes in household consumption expenditures as well as patterns in rural and urban India. Our study contributes to understanding the extent to which consumption expenditures have changed during the first few months of the pandemic as well as following a national-level lockdown in March 2020. In finding that health expenditures reduced in both urban as well as rural areas, there are implications for health policy given that many households may have foregone regular health expenditures on account of the threat of COVID-19 infection at health centres or other medical facilities.
Although there was an increase in coverage under health insurance promulgated by the Government of India, our findings are not able to distinguish between households that were affected by COVID-19 infection and those that were not. To some extent, our findings suggest that these large-scale changes in household consumption expenditures do not necessarily reflect access to health insurance or healthcare facilities, but rather an adjustment in household consumption budgets following the COVID-19 pandemic and subsequent losses due to lockdown restrictions. Future work can use subsequent rounds of the CMIE dataset to map these trends into the longer-term impact of COVID-19 on household health and food expenditures. A major shortcoming of the study is that we are not able to pinpoint the channels or pathways through which these changes in household consumption expenditures have taken place, which would require more expansive data on access to public welfare schemes and social capital, among other insurance mechanisms.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.